

Stereotactic Radiotherapy for Critically Located Pancreatic and Biliary Targets: A Review on Simultaneous Integrated Protection and Other Dose-Painting Strategies to Minimize Dose to Critical Organs at Risk
 ,
,  , and
, and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Material and Methods
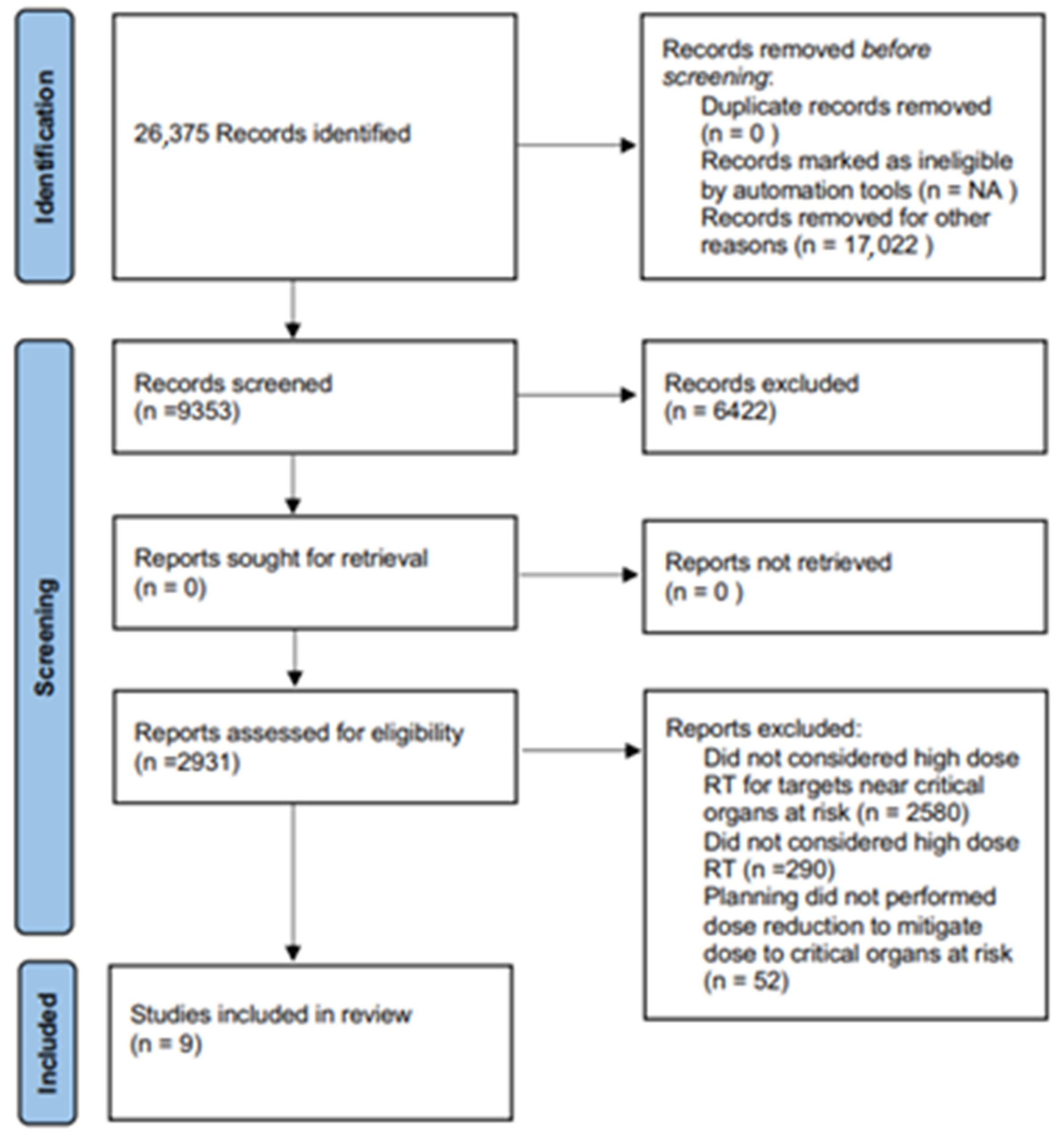
2.1. Search Strategy
2.2. Study Selection
- -
- Patients > 18 years old;
- -
- Studies from 2010 to 2023 that performed SRT in patients with target lesions near critical OARs. Suitable SRT criteria consisted of prescription doses of at least 35 Gy in five fractions, delivered with volumetric-modulated arc therapy (V-MAT), IMRT, Helical IMRT or Robotic IMRT;
- -
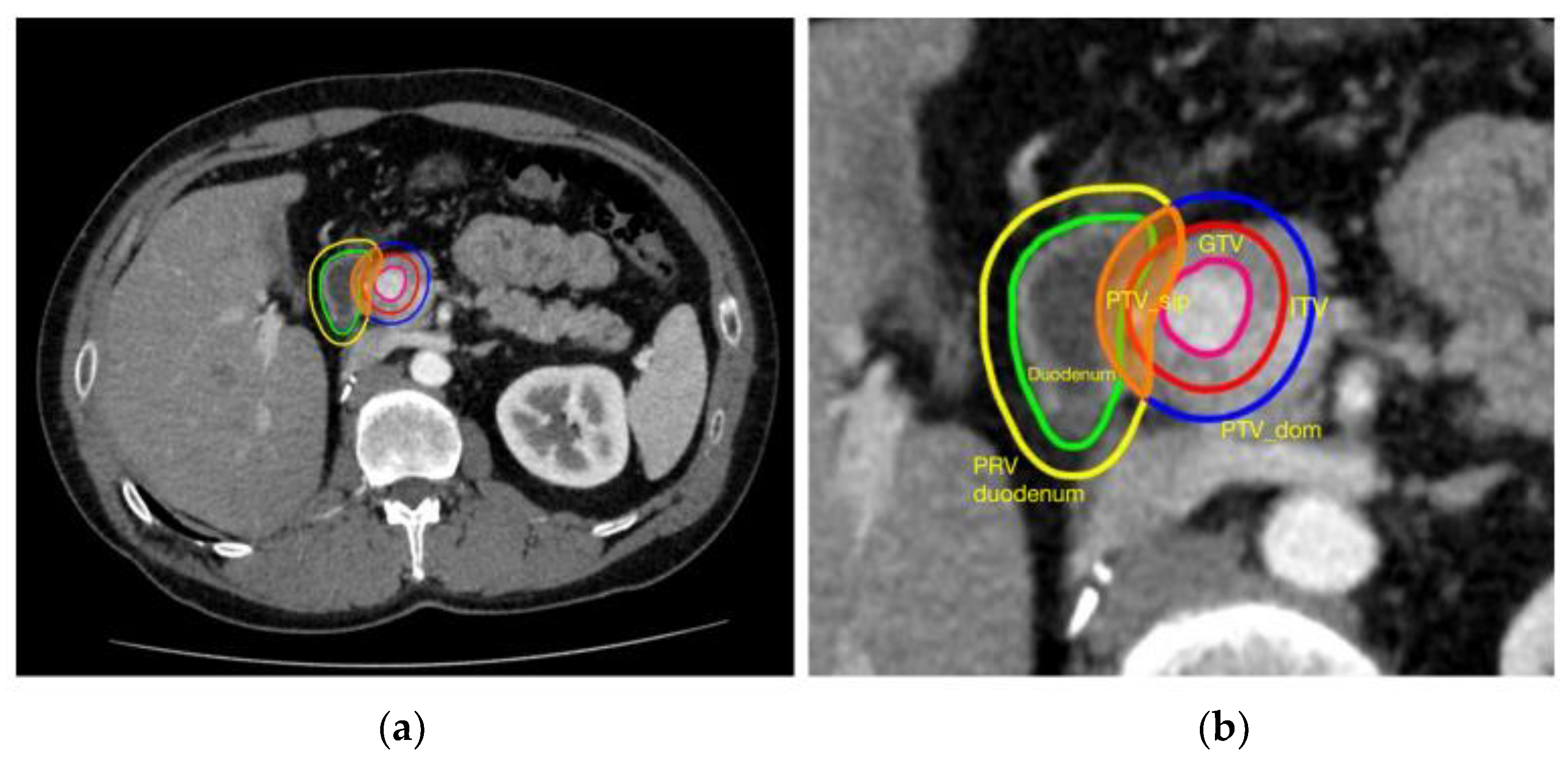
- For use of SIP as planning strategy, the planning process had to be clearly described in material and methods sections; the keyword “SIP” was not necessary, but dose prescription had to be decreased in the area of overlap between PTV and OAR as in the SIP process;
- -
- A report about target coverage (at least PTV and GTV) and dose constraints for critical OARs;
- -
- Selected studies had to include clinical and radiological information about follow-up for toxicity assessment, as well as information concerning local control.
2.3. Study Endpoints
3. Results
4. Discussion
- -
- Is there a loss of tumor control probably due to these approaches? If yes, is it related to the volume of PTV_SIP (i.e., greater area of overlap = greater area of dose reduction) or related to other clinical-dosimetric factors?
- -
- If relapse occurs, is it in SIP/dose reduction area?
- -
- If relapse is not in SIP area or does not occur, which biologic mechanism could also explain the tumor control in case of non-ablative doses delivered?
- -
- Is it safe and useful compared to the ICRU 91 and SIP approach prescribing extremely high doses in the area of PTV relatively far from critical OARs, as suggested by some authors? (The so-called “combined SIB/SIP approach”)?
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Wilke, L.; Andratschke, N.; Blanck, O.; Brunner, T.B.; Combs, S.E.; Grosu, A.L.; Moustakis, C.; Schmitt, D.; Baus, W.W.; Guckenberger, M. Icru report 91 on prescribing, recording, and reporting of stereotactic treatments with small photon beams: Statement from the degro/dgmp working group stereotactic radiotherapy and radiosurgery. Strahlenther. Onkol. 2019, 195, 193–198. [Google Scholar] [CrossRef] [PubMed]
- Lebredonchel, S.; Lacornerie, T.; Rault, E.; Wagner, A.; Reynaert, N.; Crop, F. About the non-consistency of ptv-based prescription in lung. Phys. Med. 2017, 44, 177–187. [Google Scholar] [CrossRef] [PubMed]
- Moustakis, C.; Blanck, O.; Ebrahimi, F.; Ka Heng Chan, M.; Ernst, I.; Krieger, T.; Duma, M.N.; Oechsner, M.; Ganswindt, U.; Heinz, C.; et al. Time for standardization of sbrt planning through large scale clinical data and guideline-based approaches. Strahlenther. Onkol. 2017, 193, 1068–1069. [Google Scholar] [CrossRef] [PubMed]
- Moustakis, C.; Blanck, O.; Ebrahimi Tazehmahalleh, F.; Ka Heng Chan, M.; Ernst, I.; Krieger, T.; Duma, M.N.; Oechsner, M.; Ganswindt, U.; Heinz, C.; et al. Planning benchmark study for sbrt of early stage nsclc: Results of the degro working group stereotactic radiotherapy. Strahlenther. Onkol. 2017, 193, 780–790. [Google Scholar] [CrossRef] [PubMed]
- Andratschke, N.; Parys, A.; Stadtfeld, S.; Wurster, S.; Huttenlocher, S.; Imhoff, D.; Yildirim, M.; Rades, D.; Rödel, C.M.; Dunst, J.; et al. Clinical results of mean gtv dose optimized robotic guided sbrt for liver metastases. Radiat. Oncol. 2016, 11, 74. [Google Scholar] [CrossRef]
- Baumann, R.; Chan, M.K.H.; Pyschny, F.; Stera, S.; Malzkuhn, B.; Wurster, S.; Huttenlocher, S.; Szücs, M.; Imhoff, D.; Keller, C.; et al. Clinical results of mean gtv dose optimized robotic-guided stereotactic body radiation therapy for lung tumors. Front. Oncol. 2018, 8, 171. [Google Scholar] [CrossRef]
- Brunner, T.B.; Nestle, U.; Adebahr, S.; Gkika, E.; Wiehle, R.; Baltas, D.; Grosu, A.L. Simultaneous integrated protection: A new concept for high-precision radiation therapy. Strahlenther. Onkol. 2016, 192, 886–894. [Google Scholar] [CrossRef]
- Koay, E.J.; Hanania, A.N.; Hall, W.A.; Taniguchi, C.M.; Rebueno, N.; Myrehaug, S.; Aitken, K.L.; Dawson, L.A.; Crane, C.H.; Herman, J.M.; et al. Dose-escalated radiation therapy for pancreatic cancer: A simultaneous integrated boost approach. Pract. Radiat. Oncol. 2020, 10, e495–e507. [Google Scholar] [CrossRef]
- Tao, R.; Krishnan, S.; Bhosale, P.R.; Javle, M.M.; Aloia, T.A.; Shroff, R.T.; Kaseb, A.O.; Bishop, A.J.; Swanick, C.W.; Koay, E.J.; et al. Ablative radiotherapy doses lead to a substantial prolongation of survival in patients with inoperable intrahepatic cholangiocarcinoma: A retrospective dose response analysis. J. Clin. Oncol. 2016, 34, 219–226. [Google Scholar] [CrossRef]
- Tsurugai, Y.; Takeda, A.; Eriguchi, T.; Sanuki, N.; Aoki, Y. Hypofractionated radiotherapy for hepatocellular carcinomas adjacent to the gastrointestinal tract. Hepatol. Res. 2021, 51, 294–302. [Google Scholar] [CrossRef]
- Crane, C.H. Hypofractionated ablative radiotherapy for locally advanced pancreatic cancer. J. Radiat. Res. 2016, 57 (Suppl. S1), i53–i57. [Google Scholar] [CrossRef] [PubMed]
- Bonù, M.L.; Mataj, E.; Balduzzi, J.; Cefaratti, M.T.; Pedersoli, G.; Cossali, G.; Triggiani, L.; Tomasini, D.; Buglione, M.; Magrini, S.M. Stereotactic radiotherapy with simultaneous integrated protection planning technique for synovial sarcoma with stomach abutment: A case report of a complete response. Tumor Discov. 2023, 2, 356. [Google Scholar]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The prisma 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, 71. [Google Scholar] [CrossRef]
- Eisenhauer, E.A.; Therasse, P.; Bogaerts, J.; Schwartz, L.H.; Sargent, D.; Ford, R.; Dancey, J.; Arbuck, S.; Gwyther, S.; Mooney, M.; et al. New response evaluation criteria in solid tumours: Revised recist guideline (version 1.1). Eur. J. Cancer 2009, 45, 228–247. [Google Scholar] [CrossRef] [PubMed]
- Gkika, E.; Adebahr, S.; Kirste, S.; Schimek-Jasch, T.; Wiehle, R.; Claus, R.; Wittel, U.; Nestle, U.; Baltas, D.; Grosu, A.L.; et al. Stereotactic body radiotherapy (sbrt) in recurrent or oligometastatic pancreatic cancer: A toxicity review of simultaneous integrated protection (sip) versus conventional sbrt. Strahlenther. Onkol. 2017, 193, 433–443. [Google Scholar] [CrossRef] [PubMed]
- Comito, T.; Cozzi, L.; Clerici, E.; Franzese, C.; Tozzi, A.; Iftode, C.; Navarria, P.; D’Agostino, G.; Rimassa, L.; Carnaghi, C.; et al. Can stereotactic body radiation therapy be a viable and efficient therapeutic option for unresectable locally advanced pancreatic adenocarcinoma? Results of a phase 2 study. Technol. Cancer Res. Treat 2017, 16, 295–301. [Google Scholar] [CrossRef]
- Simoni, N.; Micera, R.; Paiella, S.; Guariglia, S.; Zivelonghi, E.; Malleo, G.; Rossi, G.; Addari, L.; Giuliani, T.; Pollini, T.; et al. Hypofractionated stereotactic body radiation therapy with simultaneous integrated boost and simultaneous integrated protection in pancreatic ductal adenocarcinoma. Clin. Oncol. 2021, 33, e31–e38. [Google Scholar] [CrossRef]
- Suker, M.; Nuyttens, J.J.; Eskens, F.; Haberkorn, B.C.M.; Coene, P.L.O.; van der Harst, E.; Bonsing, B.A.; Vahrmeijer, A.L.; Mieog, J.S.D.; Jan Swijnenburg, R.; et al. Efficacy and feasibility of stereotactic radiotherapy after folfirinox in patients with locally advanced pancreatic cancer (lapc-1 trial). eClinicalMedicine 2019, 17, 100200. [Google Scholar] [CrossRef]
- Tozzi, A.; Comito, T.; Alongi, F.; Navarria, P.; Iftode, C.; Mancosu, P.; Reggiori, G.; Clerici, E.; Rimassa, L.; Zerbi, A.; et al. Sbrt in unresectable advanced pancreatic cancer: Preliminary results of a mono-institutional experience. Radiat. Oncol. 2013, 8, 148. [Google Scholar] [CrossRef]
- Chuong, M.D.; Springett, G.M.; Freilich, J.M.; Park, C.K.; Weber, J.M.; Mellon, E.A.; Hodul, P.J.; Malafa, M.P.; Meredith, K.L.; Hoffe, S.E.; et al. Stereotactic body radiation therapy for locally advanced and borderline resectable pancreatic cancer is effective and well tolerated. Int. J. Radiat. Oncol. Biol. Phys. 2013, 86, 516–522. [Google Scholar] [CrossRef]
- Chuong, M.D.; Bryant, J.; Mittauer, K.E.; Hall, M.; Kotecha, R.; Alvarez, D.; Romaguera, T.; Rubens, M.; Adamson, S.; Godley, A.; et al. Ablative 5-fraction stereotactic magnetic resonance-guided radiation therapy with on-table adaptive replanning and elective nodal irradiation for inoperable pancreas cancer. Pract. Radiat. Oncol. 2021, 11, 134–147. [Google Scholar] [CrossRef]
- Chuong, M.D.; Herrera, R.; Kaiser, A.; Rubens, M.; Romaguera, T.; Alvarez, D.; Kotecha, R.; Hall, M.D.; McCulloch, J.; Ucar, A.; et al. Induction chemotherapy and ablative stereotactic magnetic resonance image-guided adaptive radiation therapy for inoperable pancreas cancer. Front. Oncol. 2022, 12, 888462. [Google Scholar] [CrossRef] [PubMed]
- Franzese, C.; Bonu, M.L.; Comito, T.; Clerici, E.; Loi, M.; Navarria, P.; Franceschini, D.; Pressiani, T.; Rimassa, L.; Scorsetti, M. Stereotactic body radiotherapy in the management of oligometastatic and recurrent biliary tract cancer: Single-institution analysis of outcome and toxicity. J. Cancer Res. Clin. Oncol. 2020, 146, 2289–2297. [Google Scholar] [CrossRef] [PubMed]
- Hoyer, M.; Roed, H.; Sengelov, L.; Traberg, A.; Ohlhuis, L.; Pedersen, J.; Nellemann, H.; Kiil Berthelsen, A.; Eberholst, F.; Engelholm, S.A.; et al. Phase-ii study on stereotactic radiotherapy of locally advanced pancreatic carcinoma. Radiother. Oncol. 2005, 76, 48–53. [Google Scholar] [CrossRef] [PubMed]
- Schellenberg, D.; Goodman, K.A.; Lee, F.; Chang, S.; Kuo, T.; Ford, J.M.; Fisher, G.A.; Quon, A.; Desser, T.S.; Norton, J.; et al. Gemcitabine chemotherapy and single-fraction stereotactic body radiotherapy for locally advanced pancreatic cancer. Int. J. Radiat. Oncol. Biol. Phys. 2008, 72, 678–686. [Google Scholar] [CrossRef]
- Koong, A.C.; Christofferson, E.; Le, Q.T.; Goodman, K.A.; Ho, A.; Kuo, T.; Ford, J.M.; Fisher, G.A.; Greco, R.; Norton, J.; et al. Phase ii study to assess the efficacy of conventionally fractionated radiotherapy followed by a stereotactic radiosurgery boost in patients with locally advanced pancreatic cancer. Int. J. Radiat. Oncol. Biol. Phys. 2005, 63, 320–323. [Google Scholar] [CrossRef]
- Koong, A.C.; Le, Q.T.; Ho, A.; Fong, B.; Fisher, G.; Cho, C.; Ford, J.; Poen, J.; Gibbs, I.C.; Mehta, V.K.; et al. Phase i study of stereotactic radiosurgery in patients with locally advanced pancreatic cancer. Int. J. Radiat. Oncol. Biol. Phys. 2004, 58, 1017–1021. [Google Scholar] [CrossRef]
- Chang, D.T.; Schellenberg, D.; Shen, J.; Kim, J.; Goodman, K.A.; Fisher, G.A.; Ford, J.M.; Desser, T.; Quon, A.; Koong, A.C. Stereotactic radiotherapy for unresectable adenocarcinoma of the pancreas. Cancer 2009, 115, 665–672. [Google Scholar] [CrossRef]
- Courtney, P.T.; Paravati, A.J.; Atwood, T.F.; Raja, N.; Zimmerman, C.T.; Fanta, P.T.; Lowy, A.M.; Simpson, D.R.; Xu, R.; Murphy, J.D. Phase i trial of stereotactic body radiation therapy dose escalation in pancreatic cancer. Int. J. Radiat. Oncol. Biol. Phys. 2021, 110, 1003–1012. [Google Scholar] [CrossRef]
- Pollom, E.L.; Alagappan, M.; von Eyben, R.; Kunz, P.L.; Fisher, G.A.; Ford, J.A.; Poultsides, G.A.; Visser, B.C.; Norton, J.A.; Kamaya, A.; et al. Single- versus multifraction stereotactic body radiation therapy for pancreatic adenocarcinoma: Outcomes and toxicity. Int. J. Radiat. Oncol. Biol. Phys. 2014, 90, 918–925. [Google Scholar] [CrossRef]
- Herman, J.M.; Chang, D.T.; Goodman, K.A.; Dholakia, A.S.; Raman, S.P.; Hacker-Prietz, A.; Iacobuzio-Donahue, C.A.; Griffith, M.E.; Pawlik, T.M.; Pai, J.S.; et al. Phase 2 multi-institutional trial evaluating gemcitabine and stereotactic body radiotherapy for patients with locally advanced unresectable pancreatic adenocarcinoma. Cancer 2015, 121, 1128–1137. [Google Scholar] [CrossRef] [PubMed]
- Loi, M.; Magallon-Baro, A.; Suker, M.; van Eijck, C.; Sharma, A.; Hoogeman, M.; Nuyttens, J. Pancreatic cancer treated with sbrt: Effect of anatomical interfraction variations on dose to organs at risk. Radiother. Oncol. 2019, 134, 67–73. [Google Scholar] [CrossRef] [PubMed]
- Alam, S.; Veeraraghavan, H.; Tringale, K.; Amoateng, E.; Subashi, E.; Wu, A.J.; Crane, C.H.; Tyagi, N. Inter- and intrafraction motion assessment and accumulated dose quantification of upper gastrointestinal organs during magnetic resonance-guided ablative radiation therapy of pancreas patients. Phys. Imaging Radiat. Oncol. 2022, 21, 54–61. [Google Scholar] [CrossRef]
- Murphy, J.D.; Christman-Skieller, C.; Kim, J.; Dieterich, S.; Chang, D.T.; Koong, A.C. A dosimetric model of duodenal toxicity after stereotactic body radiotherapy for pancreatic cancer. Int. J. Radiat. Oncol. Biol. Phys. 2010, 78, 1420–1426. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Study | Year | Target Site | N° pts | Methodology | Acute ≥ G3 (n°—(Grade) | Late G2 | Late G3 | Late G4 | Late G5 | FFLR (L.C.) |
|---|---|---|---|---|---|---|---|---|---|---|
| Brunner et al. [7] | 2016 | Pancreas | 2 | SIP | N.R. | 0 | 0 | 0 | 100% at 8.6 months | |
| Gkika et al. [15]. | 2017 | Pancreas | 9 | SIP (SIP and without-SIP group) | 2—G3 | N.R. | 0 | 0 | 0 | 67% at 1-year |
| Comito et al. [16] | 2016 | Pancreas | 45 | Priority to OARs | 0 | 2 | 0 | 0 | 0 | 90% at 2-year |
| Simoni et al. [17] | 2020 | Pancreas | 59 | SIB/SIP | 0 | N.R. | 0 | 0 | 0 | 79.7% at 1-year (unresected pts) |
| Suker et al. [18] | 2019 | Pancreas | 39 | Priority to OARs | 1—G3 1—G4 2—G5 | N.R. | 1 | 1 | 0 | Median 20 months |
| Tozzi et al. [19] | 2013 | Pancreas | 30 | Priority to OARs | 0 | 0 | 0 | 0 | 0 | 85% at 1-year |
| Choung et al. [20] | 2013 | Pancreas | 73 | Priority to OARs/SIB | 0 | 0 | 4—5.3% | 0 | 0 | 81% at 1-year (unresected pts) |
| Chuong et al. MRI-guided [21] | 2020 | Pancreas | 35 | OAR priority | 1—G3 | 1 | 1 | 0 | 0 | 87.8% at 1-year |
| Chuong et al. (update) [22] | 2022 | Pancreas | 62 | OAR priority | 3—G3 | N.R. | 2 | 0 | 1 (possible) | 98.3% at 1-year |
| Franzese et al. [23] | 2019 | Biliary tract | 14 | OAR priority | 2—G3 | 0 | 0 | 0 | 0 | 76.7% at 1-year |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bonù, M.L.; Pedersoli, G.; Balduzzi, J.; Cefaratti, M.; Mataj, E.; Cossali, G.; Granello, L.; Singh, N.; Morelli, V.; Tomasini, D.; et al. Stereotactic Radiotherapy for Critically Located Pancreatic and Biliary Targets: A Review on Simultaneous Integrated Protection and Other Dose-Painting Strategies to Minimize Dose to Critical Organs at Risk. Radiation 2023, 3, 98-109. https://doi.org/10.3390/radiation3020009
Bonù ML, Pedersoli G, Balduzzi J, Cefaratti M, Mataj E, Cossali G, Granello L, Singh N, Morelli V, Tomasini D, et al. Stereotactic Radiotherapy for Critically Located Pancreatic and Biliary Targets: A Review on Simultaneous Integrated Protection and Other Dose-Painting Strategies to Minimize Dose to Critical Organs at Risk. Radiation. 2023; 3(2):98-109. https://doi.org/10.3390/radiation3020009
Chicago/Turabian StyleBonù, Marco Lorenzo, Gloria Pedersoli, Jacopo Balduzzi, Mariateresa Cefaratti, Eneida Mataj, Gianluca Cossali, Lorenzo Granello, Navdeep Singh, Vittorio Morelli, Davide Tomasini, and et al. 2023. "Stereotactic Radiotherapy for Critically Located Pancreatic and Biliary Targets: A Review on Simultaneous Integrated Protection and Other Dose-Painting Strategies to Minimize Dose to Critical Organs at Risk" Radiation 3, no. 2: 98-109. https://doi.org/10.3390/radiation3020009