
Mental Health Biobanks—A Systematic Review on the Prevalence, Creation, and Implementation of Mental Health Biobanks Globally

Abstract
:1. Background
2. Psychiatric Illness and Biochemical Markers
3. Biobank
4. Materials and Methods
4.1. Aims
4.2. Study Design
4.3. Search Strategy
4.4. Inclusion and Exclusion
4.5. Search Procedure and Outcomes
4.6. Strength of Evidence
4.7. Data Extraction and Synthesis
5. Results
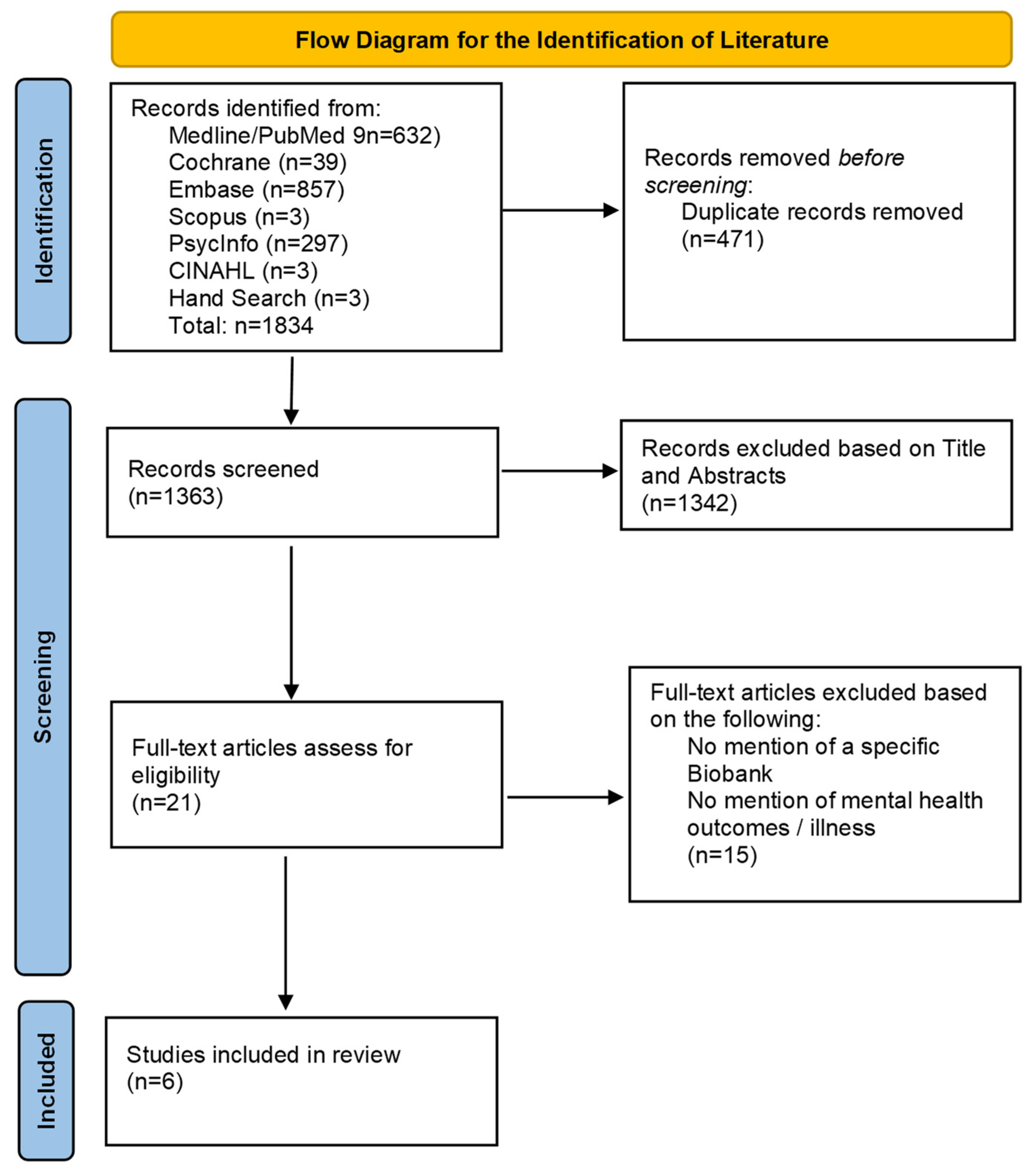
5.1. Search Results
5.2. Quality Assessment
6. Summary of Evidence
6.1. Type of Paper
6.2. Country
6.3. Setting
6.4. Recruitment
6.5. Sample Size
6.6. Ethical Considerations
6.7. Psychiatric Illness
6.8. Biological Samples
6.9. Constructs Evaluated in Clinical Outcome Measures
7. Discussion
7.1. Country
7.2. Recruitment
7.3. Sample Size
7.4. Psychiatric Illness
7.5. Biomarker
8. Limitations
9. Clinical Implications
10. Future Recommendations
11. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
| Author (Year) | Anxiety | Bipolar Disorder | Depression | Personality Disorders | Post-Traumatic Stress Disorder | Schizophrenia | Self-Harm | Substance Abuse |
|---|---|---|---|---|---|---|---|---|
| Molnar and Bencsik (2006) [17] | √ | √ | ||||||
| Frye et al. (2015) [18] | √ | |||||||
| Witt et al. (2016) [19] | √ | √ | √ | √ | √ | |||
| Davis and Hotopf, (2019) [6] | √ | √ | √ | √ | √ | |||
| Jeppesen et al. (2021) [20] | √ | √ | √ | √ | ||||
| Tigchelaar et al. (2021) [21] | √ |
| Study | Blood | Body Fluids (Amniotic Fluid, Cells, and Urine) | Cerebral Spinal Fluid | Faecal Sample | Hair | Saliva | Tissue (Placenta, Muscle/Nerve/Kidney Biopsy) |
|---|---|---|---|---|---|---|---|
| Molnar and Bencsik, 2006 [17] | √ | √ | √ | ||||
| Frye et al., 2015 [18] | √ | ||||||
| Witt et al., 2016 [19] | √ | √ | √ | √ | √ | ||
| Davis and Hotopf, 2019 [6] | |||||||
| Jeppesen et al., 2021 [20] | √ | √ | √ | ||||
| Tigchelaar et al., 2021 [21] | √ | √ |
| Author (Year) | Anxiety | Bipolar | Cognition | Depression | Diagnostic | Personality | Post-Traumatic Stress Disorder | Schizophrenia | Other |
|---|---|---|---|---|---|---|---|---|---|
| Molnar and Becsik (2006) [17] | - | - | - | - | - | - | - | - | - |
| Frye et al. (2015) [18] | - | Structured Clinical Interview for DSM-IV | - | - | - | - | - | - | Cumulative Illness Rating Scale |
| Witt et al. (2016) [19] | - | - | - | - | - | - | - | - | - |
| Davis and Hotopf (2019) [6] | Generalised Anxiety Disorder 7-item scale | - | - | - | Composite International Diagnostic Interview Short Form | Eysenck Personality Inventory | Childhood trauma screen, post-traumatic stress disorder checklist-5 | - | Addiction (Self-report), Alcohol Use Disorder Identification Tool |
| Jeppesen et al. (2021) [20] | Hamilton Anxiety Rating Scale | Young Mania Rating Scale | Montreal Cognitive Assessment, Mini-mental state examination | Hamilton Depression Rating Scale, Montgomery-Asberg Depression Rating Scale | - | - | - | Positive and Negative Symptom Scale, Scale for Assessment of Positive/Negative Symptoms | Trail Making Test |
| Tigchelaar et al. (2021) [21] | Generalised Anxiety Disorder 7-item scale | - | Montreal Cognitive Assessment | Patient Health Questionnaire for depression, 16-item Quick Inventory of Depressive Symptomatology–Self-report | - | - | - | - | Patient Health Questionnaire for somatisation |
References
- Tripathi, A.; Das, A.; Kar, S.K. Biopsychosocial Model in Contemporary Psychiatry: Current Validity and Future Prospects. Indian. J. Psychol. Med. 2019, 41, 582–585. [Google Scholar] [CrossRef]
- Jurgen Rehm, K.D.S. Global Burden of Disease and the Impact if Mental and Addictive Disorders. Curr. Psychiatry Rep. 2019, 21, 10. [Google Scholar] [CrossRef]
- Bandelow, B.; Michaelis, S. Epidemiology of anxiety disorders in the 21st century. Dialogues Clin. Neurosci. 2015, 17, 327–335. [Google Scholar] [CrossRef]
- Evans-Lacko, S.; Aguilar-Gaxiola, S.; Al-Hamzawi, A.; Alonso, J.; Benjet, C.; Bruffaerts, R.; Chiu, W.T.; Florescu, S.; de Girolamo, G.; Gureje, O.; et al. Socio-economic variations in the mental health treatment gap for people with anxiety, mood, and substance use disorders: Results from the WHO World Mental Health (WMH) surveys. Psychol. Med. 2018, 48, 1560–1571. [Google Scholar] [CrossRef]
- Liu, N.H.; Daumit, G.L.; Dua, T.; Aquila, R.; Charlson, F.; Cuijpers, P.; Druss, B.; Dudek, K.; Freeman, M.; Fujii, C.; et al. Excess mortality in persons with severe mental disorders: A multilevel intervention framework and priorities for clinical practice, policy and research agendas. World Psychiatry. 2017, 16, 30–40. [Google Scholar] [CrossRef]
- Davis, K.; Hotopf, M. Mental health phenotyping in UK Biobank. Prog. Neurol. Psychiatry 2019, 23, 4–7. [Google Scholar] [CrossRef]
- Brand, S.J.; Moller, M.; Harvey, B.H. A Review of Biomarkers in Mood and Psychotic Disorders: A Dissection of Clinical vs. Preclinical Correlates. Curr. Neuropharmacol. 2015, 13, 324–368. [Google Scholar] [CrossRef]
- Boksa, P. A way forward for research on biomarkers for psychiatric disorders. J. Psychiatry Neurosci. 2013, 38, 75–77. [Google Scholar] [CrossRef]
- Strawbridge, R.; Young, A.H.; Cleare, A.J. Biomarkers for depression: Recent insights, current challenges and future prospects. Neuropsychiatr. Dis. Treat. 2017, 13, 1245–1262. [Google Scholar] [CrossRef]
- Otlowski, M.; Nicol, D.; Stranger, M. Biobanks information paper 2010. J. Law Inf. Sci. 2010, 20, 87. [Google Scholar]
- Akervall, J.; Pruetz, B.L.; Geddes, T.J.; Larson, D.; Felten, D.J.; Wilson, G.D. Beaumont health system biobank: A multidisciplinary biorepository and translational research facility. Biopreserv. Biobank 2013, 11, 221–228. [Google Scholar] [CrossRef] [PubMed]
- Muka, T.; Glisic, M.; Milic, J.; Verhoog, S.; Bohlius, J.; Bramer, W.; Chowdhury, R.; Franco, O.H. A 24-step guide on how to design, conduct, and successfully publish a systematic review and meta-analysis in medical research. Eur. J. Epidemiol. 2020, 35, 49–60. [Google Scholar] [CrossRef] [PubMed]
- da Costa, B.R.; Cevallos, M.; Altman, D.G.; Rutjes, A.W.; Egger, M. Uses and misuses of the STROBE statement: Bibliographic study. BMJ Open 2011, 1, e000048. [Google Scholar] [CrossRef]
- McArthur, A.; Klugárová, J.; Yan, H.; Florescu, S. Innovations in the systematic review of text and opinion. JBI Evid. Imp. 2015, 13, 188–195. [Google Scholar] [CrossRef] [PubMed]
- Chan, A.-W.; Tetzlaff, J.M.; Altman, D.G.; Laupacis, A.; Gøtzsche, P.C.; Krleža-Jerić, K.; Hróbjartsson, A.; Mann, H.; Dickersin, K.; Berlin, J.A.; et al. SPIRIT 2013 statement: Defining standard protocol items for clinical trials. Ann. Intern. Med. 2013, 158, 200–207. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; A Akl, E.; E Brennan, S.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Molnar, M.J.; Bencsik, P. Establishing a Neurological-Psychiatric Biobank: Banking, informatics, ethics. Cell Immunol. 2006, 244, 101–104. [Google Scholar] [CrossRef]
- Frye, M.A.; McElroy, S.L.; Fuentes, M.; Sutor, B.; Schak, K.M.; Galardy, C.W.; A Palmer, B.; Prieto, M.L.; Kung, S.; Sola, C.L.; et al. Development of a bipolar disorder biobank: Differential phenotyping for subsequent biomarker analyses. Int. J. Bipolar Disord. 2015, 3, 14. [Google Scholar] [CrossRef]
- Witt, S.; Dukal, H.; Hohmeyer, C.; Radosavljevic-Bjelic, S.; Schendel, D.; Frank, J.; Lang, M.; Streit, F.; Strohmaier, J.; Treutlein, J.; et al. Biobank of Psychiatric Diseases Mannheim. BioPsy. Open J. Bioresour. 2016, 3, e2. [Google Scholar]
- Jeppesen, R.; Orlovska-Waast, S.; Sørensen, N.V.; Christensen, R.H.B.; Benros, M.E. Immunological investigations of the cerebrospinal fluid in patients with recent onset psychotic disorders: A study protocol. PLoS ONE 2021, 16, e0257946. [Google Scholar] [CrossRef]
- Tigchelaar, C.; Atmosoerodjo, S.D.; van Faassen, M.; Wardenaar, K.J.; de Deyn, P.P.; Schoevers, R.A.; Kema, I.P.; Absalom, A.R. The Anaesthetic Biobank of Cerebrospinal fluid: A unique repository for neuroscientific biomarker research. Ann. Trans. Med. 2021, 9, 455. [Google Scholar] [CrossRef] [PubMed]
- Cuschieri, S. The STROBE guidelines. Saudi J. Anaesth. 2019, 13, S31–S34. [Google Scholar] [CrossRef] [PubMed]
- Patel, V. Mental health in low- and middle-income countries. Br. Med. Bull. 2007, 81–82, 81–96. [Google Scholar] [CrossRef] [PubMed]
- Mascayano, F.; Armijo, J.E.; Yang, L.H. Addressing stigma relating to mental illness in low- and middle-income countries. Front. Psychiatry 2015, 6, 38. [Google Scholar] [CrossRef]
- Amarasinghe, M.; Tan, H.; Larkin, S.; Ruggeri, B.; Lobo, S.; Brittain, P.; Broadbent, M.; Baggaley, M.; Schumann, G. Banking the brain. Addressing the ethical challenges of a mental-health biobank. EMBO Rep. 2013, 14, 400–404. [Google Scholar] [CrossRef]
- Altman, D.G. Practical Statistics for Medical Research, 1st ed.; CRC Press: New York, NY, USA, 1990. [Google Scholar]
- World Health Organisation. Depression. Available online: https://www.who.int/news-room/fact-sheets/detail/depression (accessed on 3 July 2023).
- Davis, K.A.S.; Cullen, B.; Adams, M.; Brailean, A.; Breen, G.; Coleman, J.R.I.; Dregan, A.; Gaspar, H.A.; Hübel, C.; Lee, W.; et al. Indicators of mental disorders in UK Biobank-A comparison of approaches. Int. J. Methods Psychiatr. Res. 2019, 28, e1796. [Google Scholar] [CrossRef]
- Vaught, J.B.; Henderson, M.K. Biological sample collection, processing, storage and information management. IARC Sci. Publ. 2011, 163, 23–42. [Google Scholar]
- Jeppesen, R.; Christensen, R.H.B.; Pedersen, E.M.J.; Nordentoft, M.; Hjorthøj, C.; Köhler-Forsberg, O.; Benros, M.E. Efficacy and safety of anti-inflammatory agents in treatment of psychotic disorders—A comprehensive systematic review and meta-analysis. Brain Behav. Immun. 2020, 90, 364–380. [Google Scholar] [CrossRef]
- Toben, C.; Arnet, V.K.; Lo, A.; Saunders, P.H.; Baune, B.T. Standardized biomarker and biobanking requirements for personalized psychiatry. In Personalized Psychiatry, 1st ed.; Baune, B.T., Ed.; Elsevier Academic Press: San Diego, CA, USA, 2019; pp. 537–547. [Google Scholar]
- Clark, L.A.; Cuthbert, B.; Lewis-Fernández, R.; Narrow, W.E.; Reed, G.M. Three Approaches to Understanding and Classifying Mental Disorder: ICD-11, DSM-5, and the National Institute of Mental Health’s Research Domain Criteria (RDoC). Psychol. Sci. Public Interest 2017, 18, 72–145. [Google Scholar] [CrossRef]
- Stapelberg, N.J.C.; Branjerdporn, G.; Adhikary, S.; Johnson, S.; Ashton, K.; Headrick, J. Environmental Stressors and the PINE Network: Can Physical Environmental Stressors Drive Long-Term Physical and Mental Health Risks? Int. J. Environ. Res. Public Health 2022, 19, 13226. [Google Scholar] [CrossRef]
- Sudlow, C.; Gallacher, J.; Allen, N.; Beral, V.; Burton, P.; Danesh, J.; Downey, P.; Elliott, P.; Green, J.; Landray, M.; et al. UK biobank: An open access resource for identifying the causes of a wide range of complex diseases of middle and old age. PLoS Med. 2015, 12, e1001779. [Google Scholar] [CrossRef] [PubMed]

| Author (Year) | Type of Paper | Country | Setting/Clinic/Hospital | Recruitment | Sample Size | Limitations |
|---|---|---|---|---|---|---|
| Molnar and Bencsik (2006) [17] | Study Protocol | Hungary | four sites—Department of Neurology and Psychiatry from four Medical Universities (Budapest, Debrecen, Pecs, Szeged) | - | - | - |
| Frye et al. (2015) [18] | Cohort Study | United States of America | two sites—(1) Mayo Clinic, Rochester, Minnesota, (2) Linder centre for HOPE, Cincinnati, Ohio. | Clinical population | 1363 a | Little racial variation-90% Caucasian, unable to measure severity of illness |
| Witt et al. (2016) [19] | Study Protocol | Germany | three sites—(1) Department of Genetic Epidemiology in Psychiatry, (2) Molecular Genetic Laboratory, (3) Central Institute of Mental Health (CIMH) | Clinical population | 78,000 b | - |
| Davis and Hotopf (2019) [6] | Commentary Paper | United Kingdom | four sites—(1) UK Biobank, (2) Hospital Episodes Statistics for England (3) Scottish Morbidity Record (4) Patient Episode Database for Wales | Voluntary participation of general population | 150,000 c | Large sample size to conduct interview, mental disorders under-reported in routine health care, self-report bias |
| Jeppesen et al. (2021) [20] | Study Protocol | Denmark | Mental Health Centre, Copenhagen | Clinical population | 200 d | Selection bias, Confounders such as smoking, alcohol use and eating habits, possible adverse effects following collection of biospecimens |
| Tigchelaar et al. (2021) [21] | Cohort Study | The Netherlands | University Medical Centre Groningen | Clinical population | 450 e | Selective sample of patients, nil healthy controls. CSF was collected at only one time point subjected to biochemical changes in circadian rhythm, Self-report questionnaires bias |
| Molnar and Bencsik (2006) [17] | Jeppesen et al. (2021) [20] | Witt et al. (2016) [19] | ||
|---|---|---|---|---|
| Administrative Information | ||||
| Title | 1 | 1 | 1 | |
| Title registration | 1 | 1 | 4 | |
| Protocol Version | 1 | 2 | 5 | |
| Funding | NR | 10 | 1 | |
| Introduction | ||||
| Background and Rationale | 1 | 2 | 1 | |
| Objectives | 2 | 3 | 1 | |
| Trial Design | NR | 3 | NR | |
| Methods: Participants, Interventions, Outcomes | ||||
| Study Setting | 2 | 3 | 4 | |
| Eligibility Criteria | NR | 3 | NR | |
| Interventions | 2 | 4 | NR | |
| Outcomes | NR | 4 | NR | |
| Participant timeline | NR | 5 | 3 | |
| Sample size | NR | 5 | 4 | |
| Recruitment | 2 | 3 | NR | |
| Methods: Data collection, management, and analysis | ||||
| Data collection methods | 2 | 4 | 2 | |
| Data management | 2 | 4 | 3 | |
| Statistical methods | NR | 5 | NR | |
| Methods: Monitoring | ||||
| Data monitoring | 3 | NR | NR | |
| Harms | 3 | 6–7 | 3 | |
| Auditing | NR | NR | NR | |
| Ethics and Dissemination | ||||
| Research ethics approval | 3 | 3 | 3 | |
| Protocol Amendments | NR | NR | NR | |
| Consent or assent | 3 | 3 | 3 | |
| Confidentiality | 3 | 4 | 3 | |
| Declaration of interests | NR | 10 | 5 | |
| Access to data | 3 | 10 | 5 | |
| Ancillary and post-trial care | NR | NR | NR | |
| Dissemination policy | 3 | 10 | 5 | |
| Appendices | ||||
| Informed consent materials | 3 | NR | NR | |
| Biological specimens | 2 | 7 | 3 | |
| Tigchelaar et al. (2021) [21] | Frye et al. (2015) [18] | ||
|---|---|---|---|
| Title and Abstract | 1 | 1 | |
| Introduction | |||
| Background/rationale | 2 | 2 | |
| Objectives | 2 | 2 | |
| Methods | |||
| Study Design | 2 | 1 | |
| Setting | 2 | 2 | |
| Participants | 1 | 2 | |
| Variables | 2 | 1 | |
| Data sources/measurement | 2 | 2 | |
| Bias | 0 | 0 | |
| Study size | 2 | 1 | |
| Quantitative variables | 2 | 2 | |
| Statistical methods | 1 | 1 | |
| Results | |||
| Participants | 2 | 1 | |
| Descriptive Data | 2 | 1 | |
| Outcome Data | 2 | 2 | |
| Main Results | 1 | 1 | |
| Other analyses | 0 | 0 | |
| Discussion | |||
| Key results | 2 | 2 | |
| Limitations | 2 | 2 | |
| Interpretation | 2 | 2 | |
| Generalisability | 0 | 2 | |
| Other information | |||
| Funding | 2 | 2 | |
| Total: | 34/44 | 32/44 | |
| Total percentage score: | 77.3% | 72.8% |
| Author (Year) | 1. Is the Source Completed Identified? | 2. Does the Source of the Opinion Have Standing Field of Expertise? | 3. Are the Interests of the Population in the Central Focus of This Opinion? | 4. Is the Stated Position the Result of an Analytic Process, and Is There Logic in the Opinion Expressed? | 5. Is There Reference to Existing Literature? | 6. Is Any Incongruence with Literature/Sources Logically Defended? |
|---|---|---|---|---|---|---|
| Davis and Hotopf (2019) [5] | Yes | Yes | Unsure | Yes | Yes | Yes |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Govind, N.S.; Gillespie, K.M.; Branjerdporn, G. Mental Health Biobanks—A Systematic Review on the Prevalence, Creation, and Implementation of Mental Health Biobanks Globally. Psychiatry Int. 2024, 5, 1-14. https://doi.org/10.3390/psychiatryint5010001
Govind NS, Gillespie KM, Branjerdporn G. Mental Health Biobanks—A Systematic Review on the Prevalence, Creation, and Implementation of Mental Health Biobanks Globally. Psychiatry International. 2024; 5(1):1-14. https://doi.org/10.3390/psychiatryint5010001
Chicago/Turabian StyleGovind, Nitika S., Kerri M. Gillespie, and Grace Branjerdporn. 2024. "Mental Health Biobanks—A Systematic Review on the Prevalence, Creation, and Implementation of Mental Health Biobanks Globally" Psychiatry International 5, no. 1: 1-14. https://doi.org/10.3390/psychiatryint5010001