
Tangram Puzzles in Patients with Neurocognitive Disorders: A Pilot Study
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Protocol
2.3. MMSE
2.4. MoCA-J
2.5. TMT
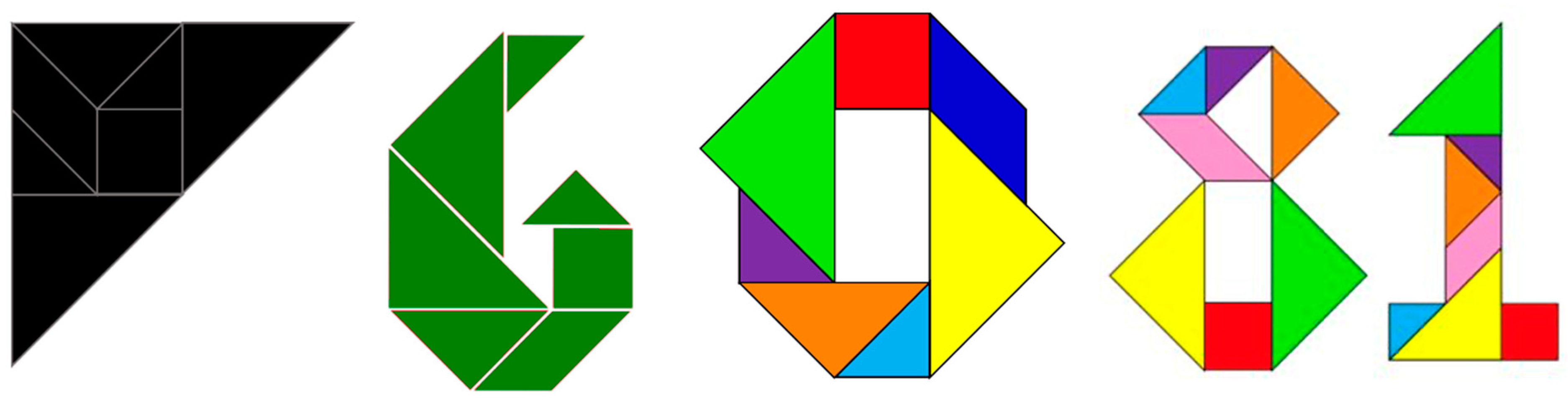
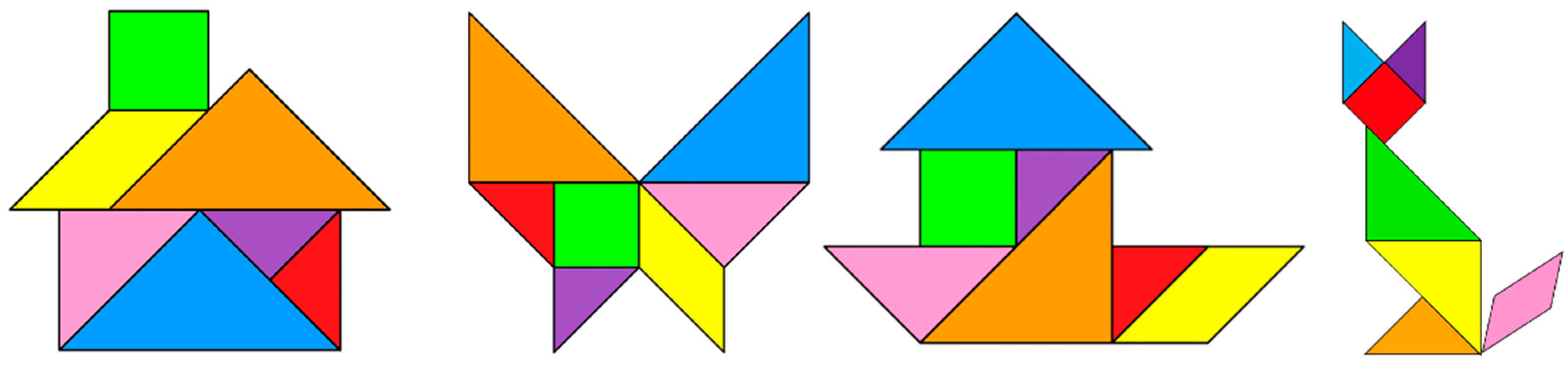
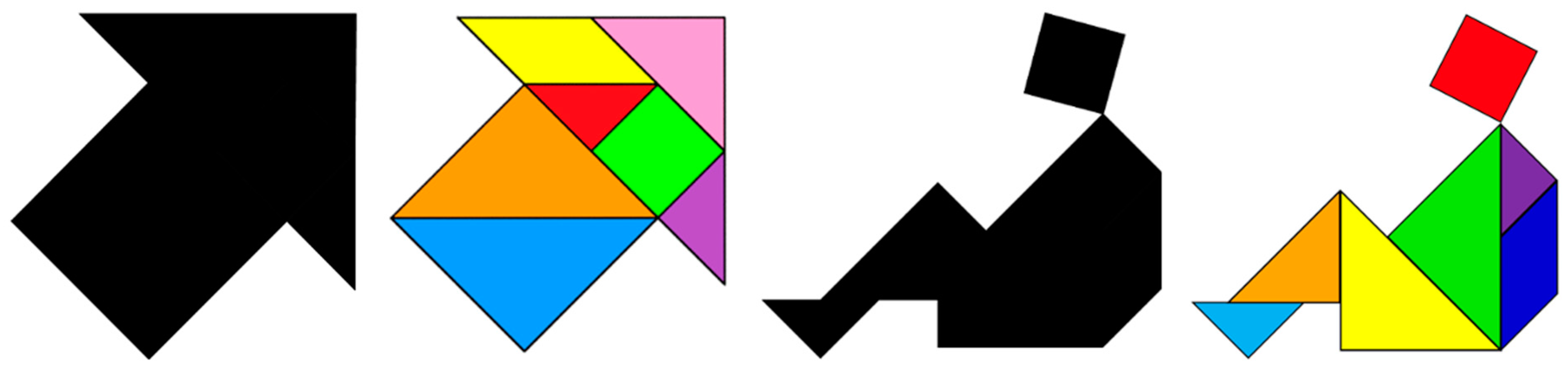
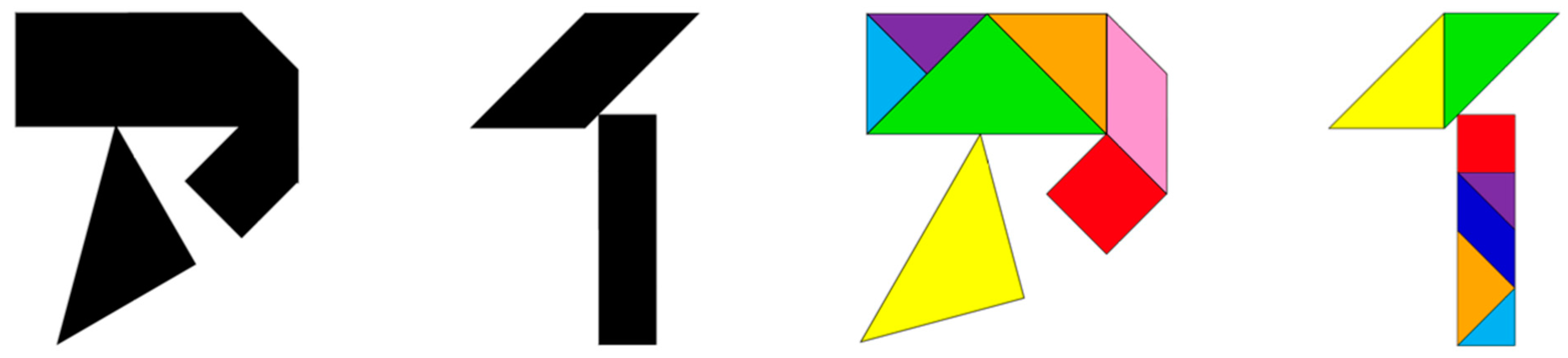
2.6. Tangram Task
2.7. Demonstration
2.8. Overall Procedure
2.9. Statistical Analysis
3. Results
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Portal Site of Official Statistics of Japan. Current Population Estimates as of October 1, 2022. Available online: https://www.stat.go.jp/english/data/jinsui/2022np/index.html#a15k01-a (accessed on 20 March 2023).
- Ninomiya, T. A Study on Future Estimates of the Elderly Population with Dementia in Japan. Research Report for 2014. Grant-in-Aid for Scientific Research on Health, Labor and Welfare. Special Research Project on Health, Labor and Welfare Science Ministry of Health, Labor and Welfare (Japan). 2015. Available online: https://mhlw-grants.niph.go.jp/system/files/2014/141031/201405037A/201405037A0001.pdf (accessed on 1 March 2015).
- Nakahori, N.; Sekine, M.; Yamada, M.; Tatsuse, T.; Kido, H.; Suzuki, M. Future projections of the prevalence of dementia in Japan: Results from the Toyama Dementia Survey. BMC Geriatr. 2021, 21, 602. [Google Scholar] [CrossRef] [PubMed]
- Sado, M.; Ninomiya, A.; Shikimoto, R.; Ikeda, B.; Baba, T.; Yoshimura, K.; Mimura, M. The estimated cost of dementia in Japan, the most aged society in the world. PLoS ONE 2018, 13, e0206508. [Google Scholar] [CrossRef] [PubMed]
- Sheehan, B. Assessment scales in dementia. Ther. Adv. Neurol. Disord. 2012, 5, 349–358. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.T.; Chang, C.C.; Chang, W.N.; Tsai, N.W.; Huang, C.C.; Chang, Y.T.; Wang, H.C.; Kung, C.T.; Su, Y.J.; Lin, W.C.; et al. Neuropsychiatric symptoms in Alzheimer’s disease: Associations with caregiver burden and treatment outcomes. QJM 2017, 110, 565–570. [Google Scholar] [CrossRef] [PubMed]
- Arevalo-Rodriguez, I.; Smailagic, N.; Roqué-Figuls, M.; Ciapponi, A.; Sanchez-Perez, E.; Giannakou, A.; Pedraza, O.L.; Bonfill Cosp, X.; Cullum, S. Mini-Mental State Examination (MMSE) for the early detection of dementia in people with mild cognitive impairment (MCI). Cochrane Database Syst. Rev. 2021, 7, CD010783. [Google Scholar] [CrossRef] [PubMed]
- Wong, S.H.; Rajikan, R.; Das, S.; Yusoff, N.A.M.; Lee, L.K. Antioxidant Intake and Mild Cognitive Impairment Among Elderly People in Klang Valley: A Pilot Study. Sains Malays. 2010, 39, 689–696. [Google Scholar]
- Eshkoor, S.A.; Hamid, T.A.; Mun, C.Y.; Ng, C.K. Mild cognitive impairment and its management in older people. Clin. Interv. Aging 2015, 10, 687–693. [Google Scholar] [CrossRef] [PubMed]
- Mendez, M.F. Early-Onset Alzheimer Disease. Neurol. Clin. 2017, 35, 263–281. [Google Scholar] [CrossRef]
- Cummings, J.L.; Tong, G.; Ballard, C. Treatment Combinations for Alzheimer’s Disease: Current and Future Pharmacotherapy Options. J. Alzheimers Dis. 2019, 67, 779–794. [Google Scholar] [CrossRef]
- van Dyck, C.H.; Swanson, C.J.; Aisen, P.; Bateman, R.J.; Chen, C.; Gee, M.; Kanekiyo, M.; Li, D.; Reyderman, L.; Cohen, S.; et al. Lecanemab in Early Alzheimer’s Disease. N. Engl. J. Med. 2023, 388, 9–21. [Google Scholar] [CrossRef]
- Risk Reduction of Cognitive Decline and Dementia: WHO Guidelines. 2019. Available online: https://www.who.int/publications/i/item/9789241550543 (accessed on 1 January 2019).
- Stern, C.; Munn, Z. Cognitive leisure activities and their role in preventing dementia: A systematic review. Int. J. Evid. Based Healthc. 2010, 8, 2–17. [Google Scholar] [CrossRef]
- Tsai, Y.-R. The Effects of the Physical and Virtual Tangram on Preschool Children’s Creativity, Spatial Ability, Achievement, and Learning Interest–A Case Study of an Interactive e-Storybook; National Taiwan University of Science and Technology: Taipei, China, 2016. [Google Scholar]
- Ayaz, H.; Shewokis, P.A.; Izzetoğlu, M.; Çakır, M.P.; Onaral, B. Tangram solved? Prefrontal cortex activation analysis during geometric problem solving. In Proceedings of the 2012 Annual International Conference of the IEEE Engineering in Medicine and Biology Society, San Diego, CA, USA, 28 August–1 September 2012; pp. 4724–4727. [Google Scholar] [CrossRef]
- Leijenaar, J.F.; van Maurik, I.S.; Kuijer, J.P.A.; van der Flier, W.M.; Scheltens, P.; Barkhof, F.; Prins, N.D. Lower cerebral blood flow in subjects with Alzheimer’s dementia, mild cognitive impairment, and subjective cognitive decline using two-dimensional phase-contrast magnetic resonance imaging. Alzheimer’s Dement. Diagn. Assess. Dis. Monit. 2017, 9, 76–83. [Google Scholar] [CrossRef]
- Monroe, T.; Carter, M. Using the Folstein Mini Mental State Exam (MMSE) to explore methodological issues in cognitive aging research. Eur. J. Ageing 2012, 9, 265–274. [Google Scholar] [CrossRef]
- Davis, D.H.; Creavin, S.T.; Yip, J.L.; Noel-Storr, A.H.; Brayne, C.; Cullum, S. Montreal Cognitive Assessment for the detection of dementia. Cochrane Database Syst. Rev. 2021, 7, CD010775. [Google Scholar] [CrossRef]
- Ashendorf, L.; Jefferson, A.L.; O’Connor, M.K.; Chaisson, C.; Green, R.C.; Stern, R.A. Trail Making Test errors in normal aging, mild cognitive impairment, and dementia. Arch. Clin. Neuropsychol. 2008, 23, 129–137. [Google Scholar] [CrossRef] [PubMed]
- Lin, R.; Chen, H.Y.; Li, H.; Li, J. Effects of creative expression therapy on Chinese elderly patients with dementia: An exploratory randomized controlled trial. Neuropsychiatr. Dis. Treat. 2019, 15, 2171–2180. [Google Scholar] [CrossRef] [PubMed]
- Gross, A.L.; Chu, N.; Anderson, L.; Glymour, M.M.; Jones, R.N.; Diseases, C.A.M. Do people with Alzheimer’s disease improve with repeated testing? Unpacking the role of content and context in retest effects. Age Ageing 2018, 47, 866–871. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.C.; Lee, S.C.; Chiu, E.C. Practice effect and test-retest reliability of the Mini-Mental State Examination-2 in people with dementia. BMC Geriatr. 2022, 22, 67. [Google Scholar] [CrossRef] [PubMed]
- Fonte, C.; Smania, N.; Pedrinolla, A.; Munari, D.; Gandolfi, M.; Picelli, A.; Varalta, V.; Benetti, M.V.; Brugnera, A.; Federico, A.; et al. Comparison between physical and cognitive treatment in patients with MCI and Alzheimer’s disease. Aging 2019, 11, 3138–3155. [Google Scholar] [CrossRef] [PubMed]
- Panza, G.A.; Taylor, B.A.; MacDonald, H.V.; Johnson, B.T.; Zaleski, A.L.; Livingston, J.; Thompson, P.D.; Pescatello, L.S. Can Exercise Improve Cognitive Symptoms of Alzheimer’s Disease? J. Am. Geriatr. Soc. 2018, 66, 487–495. [Google Scholar] [CrossRef]
- Cota, T.T.; Ishitani, L. Motivation and benefits of digital games for the elderly: A systematic literature review. Rev. Bras. Comput. Apl. 2015, 7, 2–16. [Google Scholar] [CrossRef]
- Chesham, A.; Wyss, P.; Müri, R.M.; Mosimann, U.P.; Nef, T. What Older People Like to Play: Genre Preferences and Acceptance of Casual Games. JMIR Serious Games 2017, 5, e8. [Google Scholar] [CrossRef] [PubMed]
- Seydell-Greenwald, A.; Ferrara, K.; Chambers, C.E.; Newport, E.L.; Landau, B. Bilateral parietal activations for complex visual-spatial functions: Evidence from a visual-spatial construction task. Neuropsychologia 2017, 106, 194–206. [Google Scholar] [CrossRef] [PubMed]
- Martin, L.R.; Williams, S.L.; Haskard, K.B.; Dimatteo, M.R. The challenge of patient adherence. Ther. Clin. Risk Manag. 2005, 1, 189–199. [Google Scholar] [PubMed]
- Jimmy, B.; Jose, J. Patient medication adherence: Measures in daily practice. Oman Med. J. 2011, 26, 155–159. [Google Scholar] [CrossRef] [PubMed]
- Canevelli, M.; Valletta, M.; Toccaceli Blasi, M.; Remoli, G.; Sarti, G.; Nuti, F.; Sciancalepore, F.; Ruberti, E.; Cesari, M.; Bruno, G. Facing Dementia During the COVID-19 Outbreak. J. Am. Geriatr. Soc. 2020, 68, 1673–1676. [Google Scholar] [CrossRef]
- Thyrian, J.R.; Kracht, F.; Nikelski, A.; Boekholt, M.; Schumacher-Schönert, F.; Rädke, A.; Michalowsky, B.; Vollmar, H.C.; Hoffmann, W.; Rodriguez, F.S.; et al. The situation of elderly with cognitive impairment living at home during lockdown in the Corona-pandemic in Germany. BMC Geriatr. 2020, 20, 540. [Google Scholar] [CrossRef]
- van Maurik, I.S.; Bakker, E.D.; van den Buuse, S.; Gillissen, F.; van de Beek, M.; Lemstra, E.; Mank, A.; van den Bosch, K.A.; van Leeuwenstijn, M.; Bouwman, F.H.; et al. Psychosocial Effects of Corona Measures on Patients With Dementia, Mild Cognitive Impairment and Subjective Cognitive Decline. Front. Psychiatry 2020, 11, 585686. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Participants (n = 8) |
|---|---|
| Sex, M/F | 7/1 |
| Age, mean ± SD, years | 66.0 ± 12.3 (50–78) |
| Age of onset of AD (range), years | 63.3 ± 11.7 (49–77) |
| Duration of AD (range), years | 2.8 ± 1.8 (1–6) |
| Education (range), years | 14 ± 2.1 (12–16) |
| No. | 2 | 4 | 5 | 6 | 7 | 8 | 9 | 10 |
|---|---|---|---|---|---|---|---|---|
| Sex | M | M | M | M | M | M | M | F |
| Age (y) | 76 | 50 | 62 | 76 | 52 | 78 | 56 | 78 |
| Onset (y) | 73 | 49 | 61 | 72 | 49 | 77 | 53 | 72 |
| Dur (y) | 3 | 1 | 1 | 4 | 3 | 1 | 3 | 6 |
| Edu (y) | 12 | 16 | 16 | 12 | 16 | 12 | 16 | 12 |
| Medication | Donepezil hydrochloride | Donepezil hydrochloride | Memantine hydrochloride | Rivastigmine | Donepezil hydrochloride | Donepezil hydrochloride | Donepezil hydrochloride | Memantine hydrochloride |
| Dosage | 5 mg/QD | 5 mg/QD | 10 mg/QD | 9 mg/QD | 5 mg/QD | 3 mg/QD * | 5 mg/QD | 20 mg/QD |
| Living with | Spouse | Spouse | Spouse | Spouse | Spouse | Spouse | Spouse | Daughter |
| Plays Tangram Puzzles with | Self | Self | Self | Self | Self | Self | Self | Self |
| Entertainment | No hobby | No hobby | Walking | No hobby | Gym, climbing | Golf | Aerobic exercise | No hobby |
| Alcohol Intake | No | No | No | No | No | No | 500 mL/day ** | No |
| Tobacco Use | No | No | No | No | No | No | No | No |
| Previous/ Present Career | Unemployed | Engineer (still working) | Apartment supervisor | Chef | Mechanical design | Service industry | Office staff | Housewife |
| Retirement (y) | - | 63 | 72 | 50 | 61 | 56 | - |
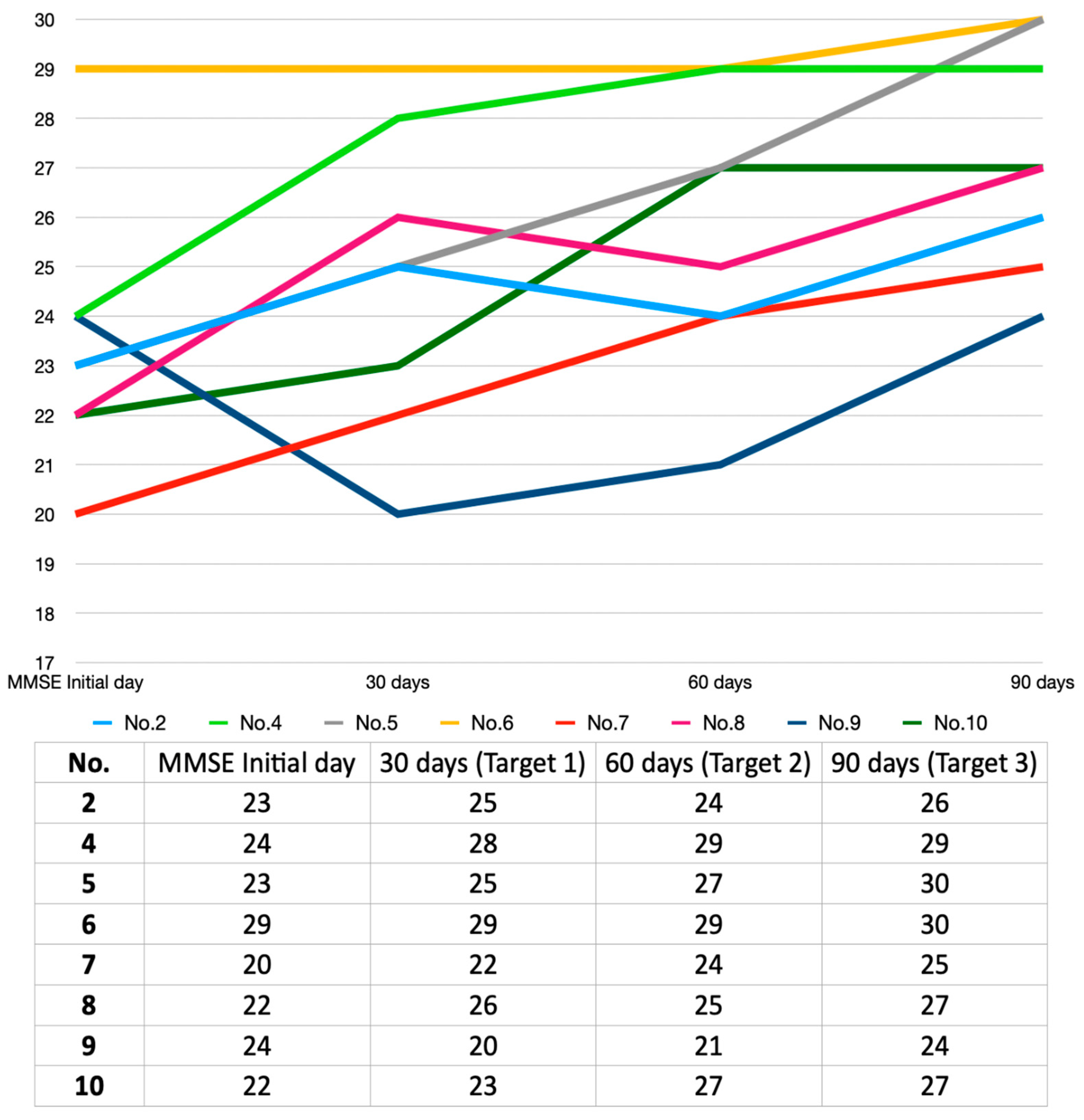
| MMSE Score | Initial Day | Final Day | Z | p |
|---|---|---|---|---|
| Total | 23.4 ± 2.6 (20–29) | 27.3 ± 2.3 (24–30) | 2.4 | 0.016 |
| Orientation | 7.9 ± 1.6 (5–10) | 9.3 ± 1.4 (6–10) | 2.2 | 0.026 |
| Registration | 3.0 ± 0.0 (3) | 3.0 ± 0.0 (3) | 0 | 1.000 |
| Attention and calculation | 2.6 ± 1.5 (0–5) | 3.9 ± 1.5 (1–5) | 1.8 | 0.066 |
| Recall | 1.3 ± 1.2 (0–3) | 2.1 ± 1.1 (0–3) | 1.5 | 0.140 |
| Language and praxis | 8.5 ± 0.8 (7–9) | 9.0 ± 0.0 (9) | 1.6 | 0.102 |
| Variable | Patients (n = 9) |
|---|---|
| Sex, M/F | 2/7 |
| Age, mean ± SD, years | 79.2 ± 3.1 (75–83) |
| Age of onset of AD (range), years | 75.4 ± 3.7 (70–80) |
| Duration of AD (range), years | 3.9 ± 2.7 (1–9) |
| Education (range), years | 13.1 ± 2.8 (9–16) |
| No. | 1 | 2 | 4 | 5 | 6 | 7 | 8 | 9 | 10 |
|---|---|---|---|---|---|---|---|---|---|
| Sex | F | M | F | M | F | F | F | F | F |
| Age (y) | 79 | 75 | 82 | 76 | 80 | 81 | 82 | 83 | 75 |
| Diagnosis | AD | AD | AD | MCI | MCI | AD | AD | AD | AD |
| Onset (y) | 70 | 73 | 75 | 74 | 78 | 80 | 79 | 79 | 71 |
| Dur (y) | 9 | 2 | 7 | 2 | 2 | 1 | 3 | 4 | 5 |
| Edu (y) | 12 | 16 | 16 | 9 | 14 | 12 | 14 | 9 | 16 |
| Medication | Donepezil hydrochloride | Donepezil hydrochloride | Donepezil hydrochloride | Donepezil hydrochloride | Donepezil hydrochloride | Donepezil hydrochloride | Galantamine hydrobromide | Donepezil hydrochloride | Memantine hydrochloride |
| Dosage | 5 mg/QD | 5 mg/QD | 5 mg/QD | 10 mg/QD | 5 mg/QD | 5 mg/QD | 8 mg/BID | 5 mg/QD | 5 mg/BID |
| Living with | Daughter | Spouse | Spouse | Spouse | Spouse & Daughter | Spouse | Spouse | Daughters | Spouse |
| Plays Tangram Puzzles with | Daughter/Grandson | Self | Self | Self | Self | Self | Self | Daughter/Grandson | Self |
| Entertainment | Television | Walking | Television | Daily shopping, walking | Ballet | Walking/Housework | Singing | Daily shopping/walking/housework | Taichi/Daily shopping/Housework |
| Alcohol Intake | No | 360 mL/day * | No | No | No | No | No | No | 180 mL/day * |
| Tobacco Use | No | No | No | 10 cigarettes/day | No | No | No | No | No |
| Previous Career | Office staff | Sales staff | Music teacher | Office staff | Office staff | Office staff | Housewife | Housewife | Housewife |
| Retirement (y) | - | 68 | 70 | 63 | 60 | 60 | - | - | - |
| No. | Moca-J (S) | Moca-J (E) | MMSE (S) | MMSE (E) | TMT-B/A (S) | TMT-B/A (E) |
|---|---|---|---|---|---|---|
| 1 | 15 | 15 | 17 | 19 | 3.9 | 5.5 |
| 2 | 18 | 21 | 22 | 22 | 2.6 | 1.4 |
| 4 | 21 | 18 | 26 | 19 | 1.9 | 5 |
| 5 | 25 | 23 | 23 | 22 | 2.7 | 1.9 |
| 6 | 18 | 14 | 22 | 20 | 5.3 | 3.1 |
| 7 | 19 | 15 | 19 | 18 | 1.7 | 2.2 |
| 8 | 18 | 20 | 23 | 24 | 2.2 | 1.9 |
| 9 | 17 | 17 | 17 | 21 | 4.0 | 3.3 |
| 10 | 18 | 19 | 22 | 22 | 2.9 | 2.1 |
| Total Score | Initial Day | Final Day | Z | p |
|---|---|---|---|---|
| MMSE | 21.2 ± 3.0 (17–26) | 20.8 ± 1.9 (18–24) | 0.300 | 0.764 |
| MoCA-J | 18.7 ± 2.8 (15–25) | 18.0 ± 3.0 (14–23) | 0.839 | 0.401 |
| TMT-B/A | 3.0 ± 1.6 (1.7–5.3) | 2.9 ± 1.4 (1.4–5.5) | 0.533 | 0.594 |
| MMSE Score | Initial Day | Final Day | Z | p |
|---|---|---|---|---|
| Total | 21.2 ± 3.0 (17–26) | 20.8 ± 1.9 (18–24) | 0.300 | 0.764 |
| Orientation | 6.2 ± 1.9 (4–9) | 5.7 ± 1.6 (4–9) | 0.549 | 0.583 |
| Registration | 3.0 ± 0.0 (3) | 3.0 ± 0.0 (3) | 0.000 | 1.000 |
| Attention and calculation | 2.7 ± 1.9 (0–5) | 2.8 ± 1.8 (1–5) | 0.503 | 0.615 |
| Recall | 0.6 ± 0.7 (0–2) | 0.4 ± 0.5 (0–1) | 0.186 | 0.853 |
| Language and praxis | 8.8 ± 0.4 (8–9) | 8.9 ± 0.3 (8–9) | 1.000 | 0.317 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhang, J.; Katsuta, N.; Takayama, T.; Orimo, N.; Shibata, N.; Kato, T. Tangram Puzzles in Patients with Neurocognitive Disorders: A Pilot Study. Psychiatry Int. 2023, 4, 404-415. https://doi.org/10.3390/psychiatryint4040036
Zhang J, Katsuta N, Takayama T, Orimo N, Shibata N, Kato T. Tangram Puzzles in Patients with Neurocognitive Disorders: A Pilot Study. Psychiatry International. 2023; 4(4):404-415. https://doi.org/10.3390/psychiatryint4040036
Chicago/Turabian StyleZhang, Jian, Narimasa Katsuta, Toshiki Takayama, Narihiro Orimo, Nobuto Shibata, and Tadafumi Kato. 2023. "Tangram Puzzles in Patients with Neurocognitive Disorders: A Pilot Study" Psychiatry International 4, no. 4: 404-415. https://doi.org/10.3390/psychiatryint4040036