
Virtual Reality Mindfulness for Meta-Competence Training among People with Different Mental Disorders: A Systematic Review

Abstract
:1. Introduction
- Is mindfulness training an effective intervention for meta-competences development in SEND?
- Can VR-assisted mindfulness support meta-competence training in target groups, such as those with SEND?
2. Materials and Methods
2.1. Review Design
2.2. Inclusion/Exclusion Criteria
2.3. Information Sources
2.4. Search Strategy
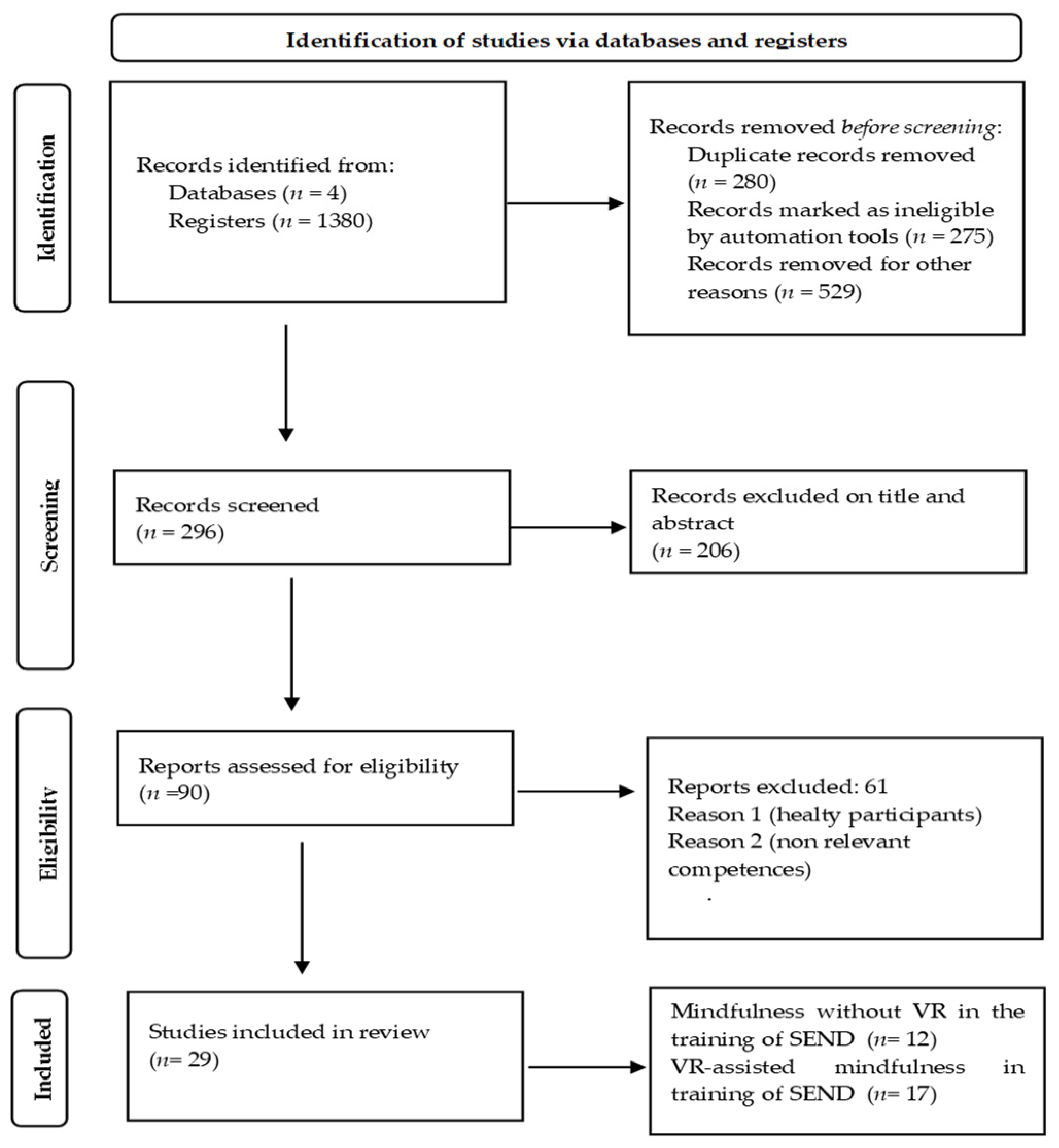
2.5. Selection Processes
2.6. Data Collection and Data Items
2.7. Critical Appraisal of Included Literature
2.8. Research Results
3. Theoretical Background
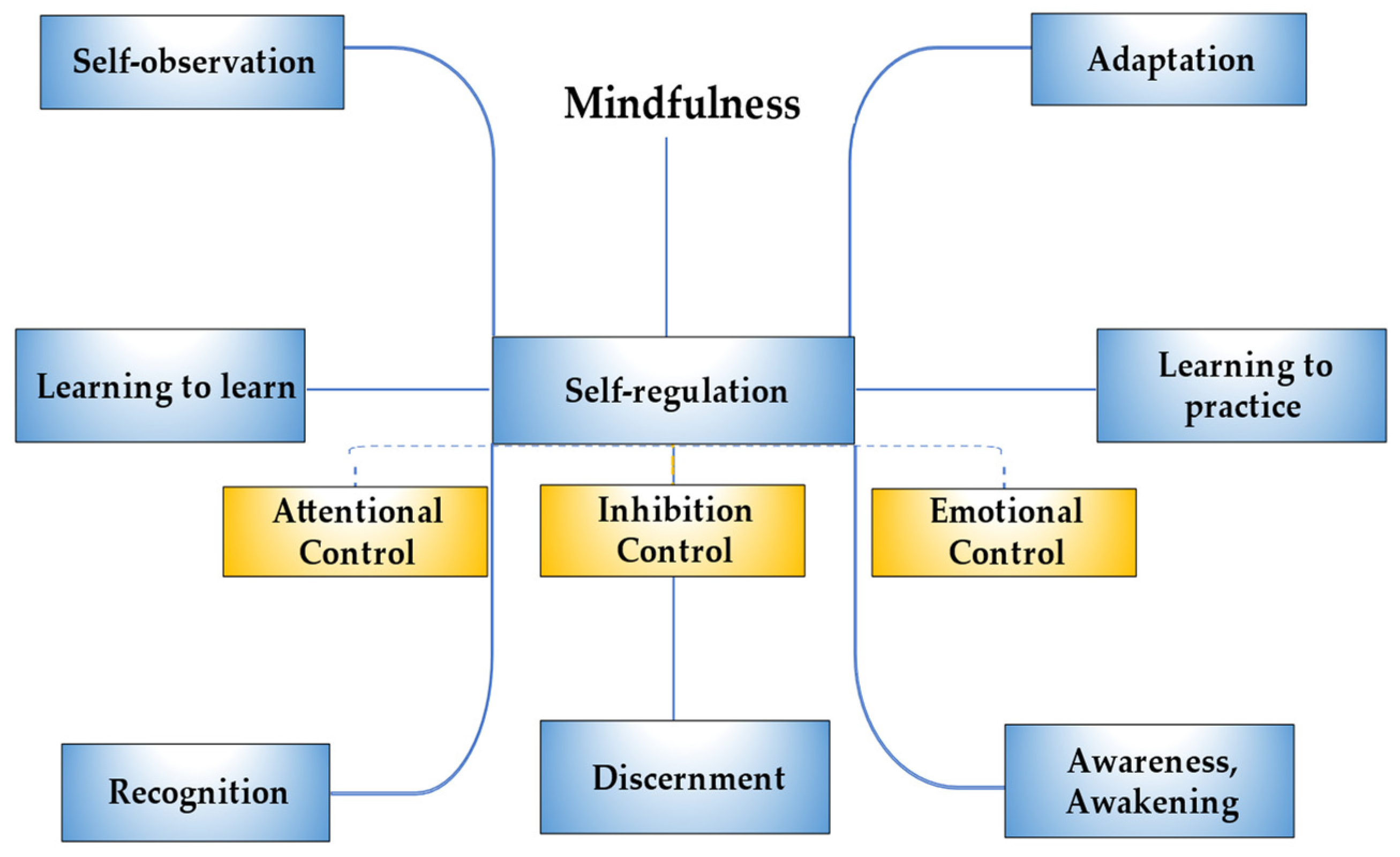
3.1. Mindfulness for Meta-Competence Training: The Mediation of Metacognition
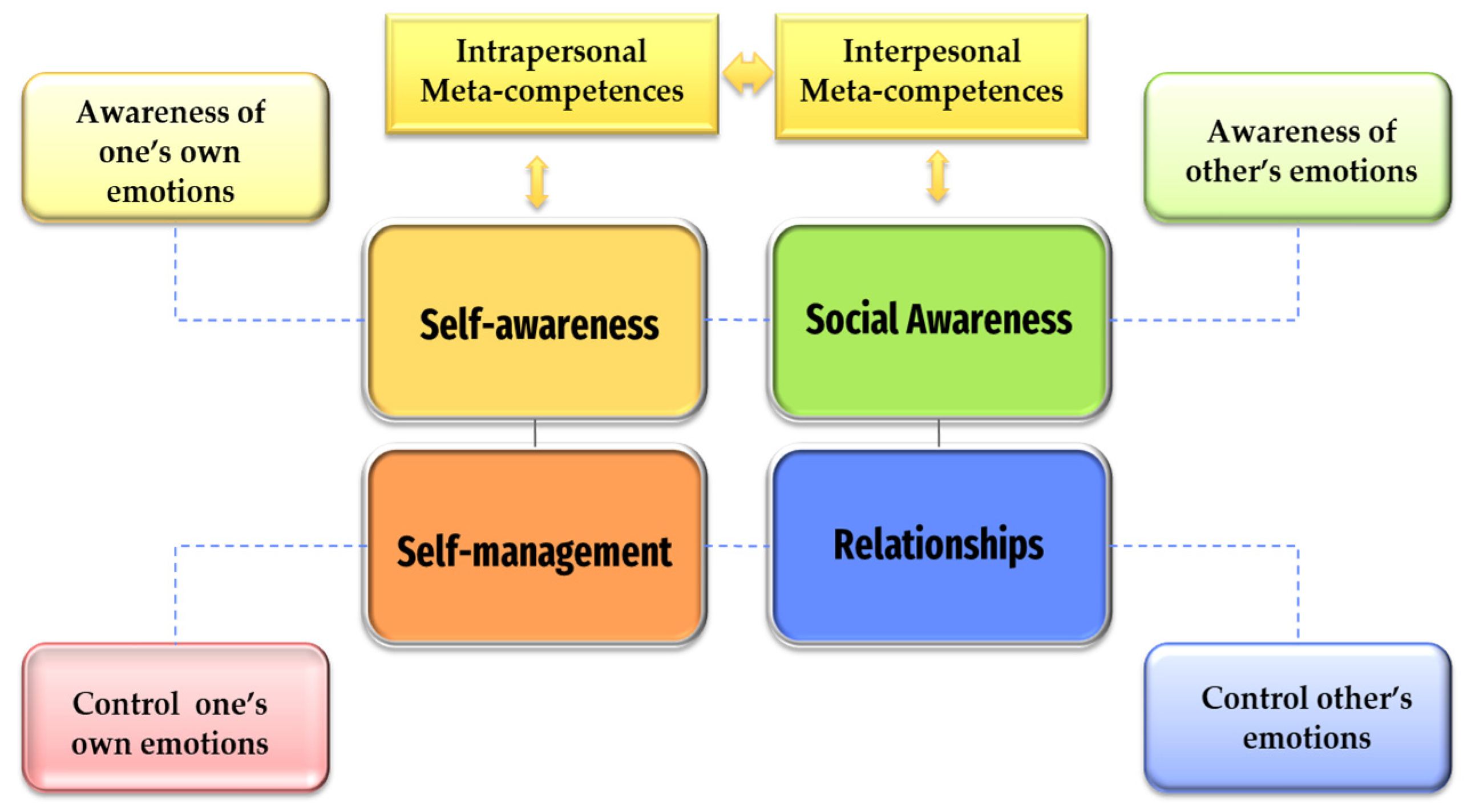
3.2. Mindfulness Training for Emotional Meta-Competences: The Mediation of Emotional Intelligence
3.3. Mindfulness Strategies for Meta-Competence Training
3.4. The Potential of VR in Assisting Mindfulness Training in SEND
4. Summary of Findings
4.1. Mindfulness Strategies for Meta-Competence Training
4.1.1. Mindfulness for Meta-Competence Training in Neurodevelopmental Disorders and Neuropsychiatric Conditions
4.1.2. Mindfulness Strategies for Meta-Competence Training in Intellectual Disabilities
4.1.3. Mindfulness Strategies for Meta-Competence Training in Learning Difficulties
4.1.4. Mindfulness Strategies for Meta-Competence Training in Giftedness
4.2. VR Mindfulness for Meta-Competence Training
4.2.1. VR Mindfulness for Meta-Competence Training in Neurodevelopmental Disorders
4.2.2. VR Mindfulness for Meta-Competence Training in Anxiety Disorders and Phobias
4.2.3. VR Mindfulness for Meta-Competence Training in Emotional and Behavioral Disorders
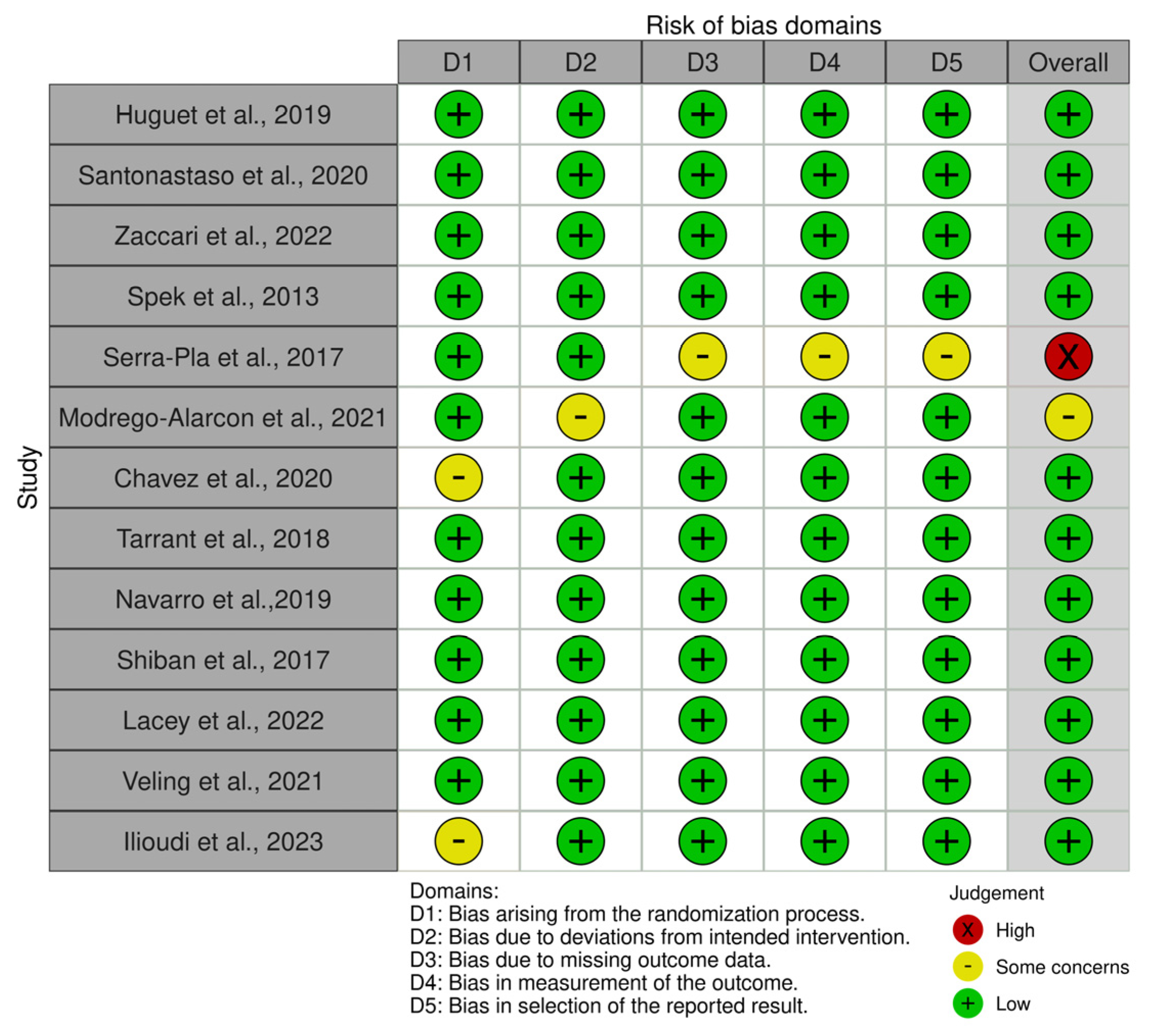
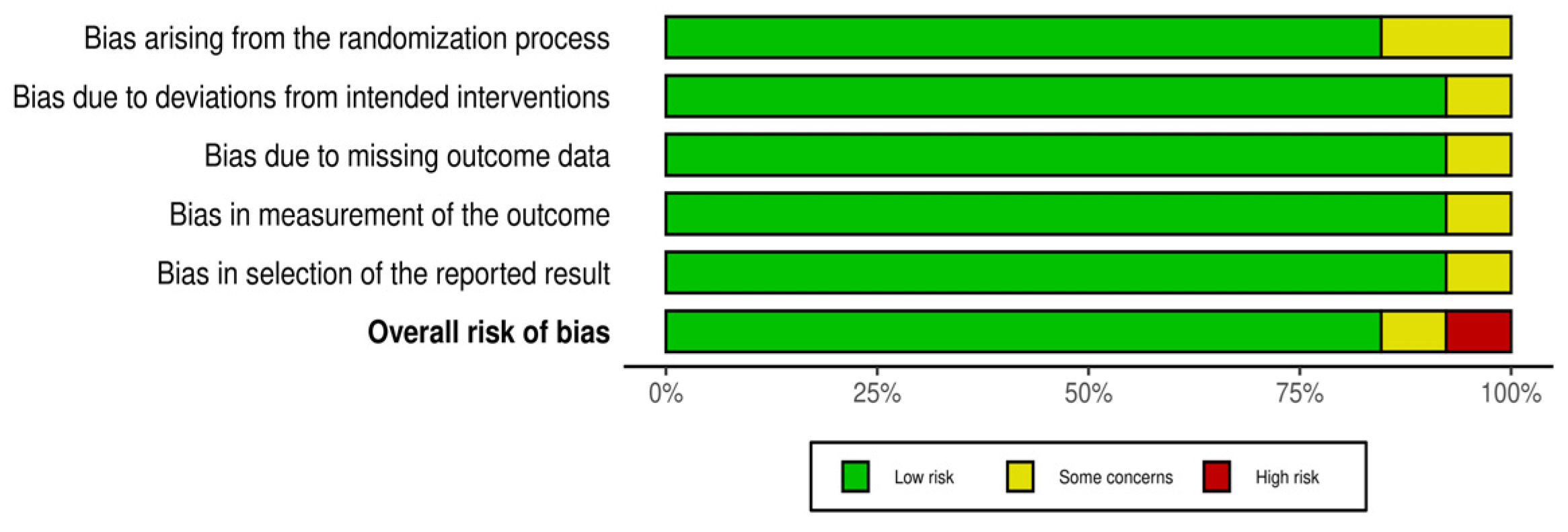
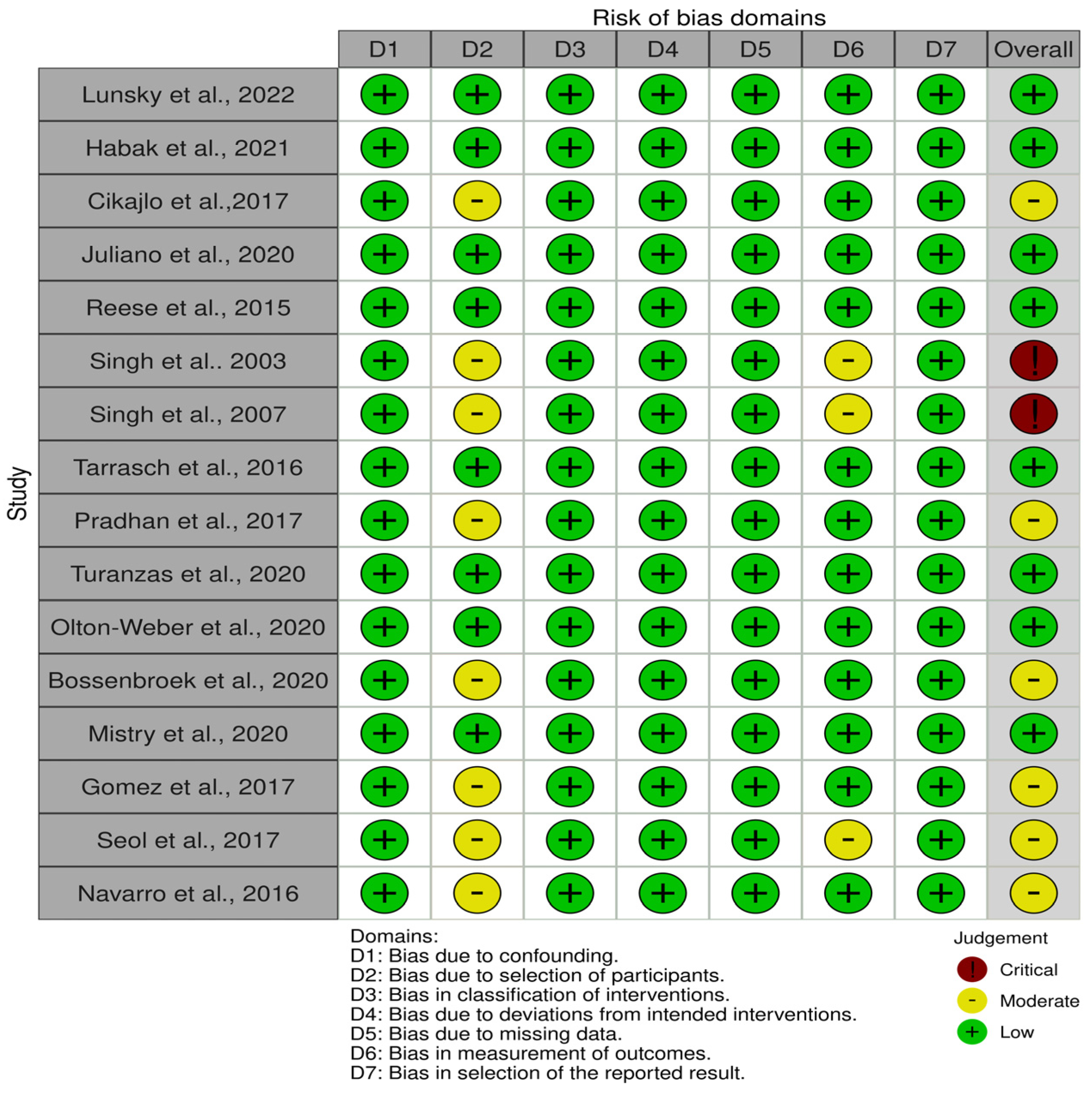
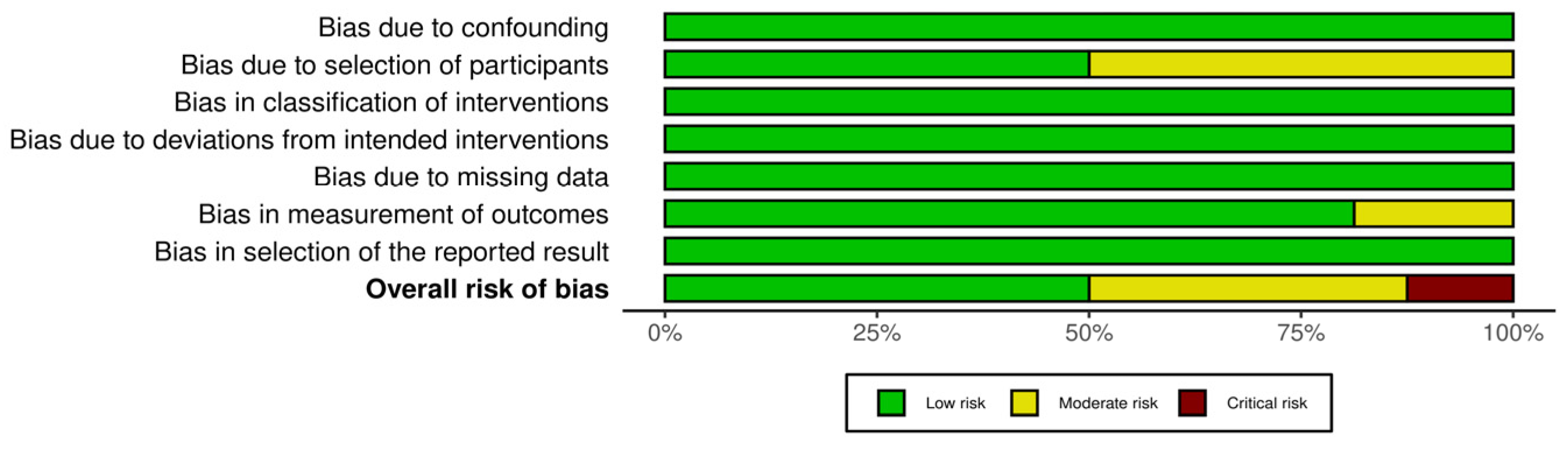
4.3. Risk of Bias Assessments
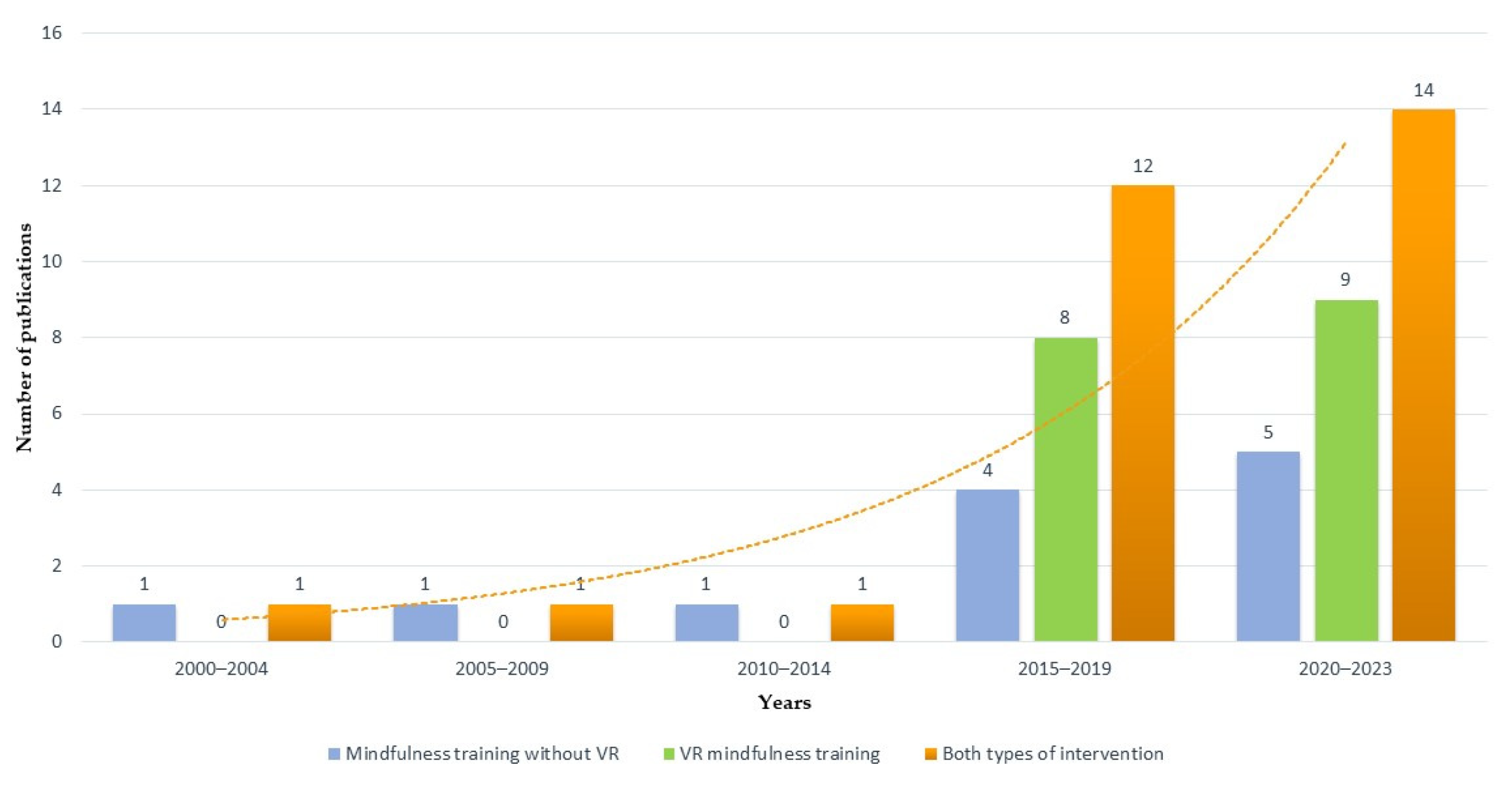
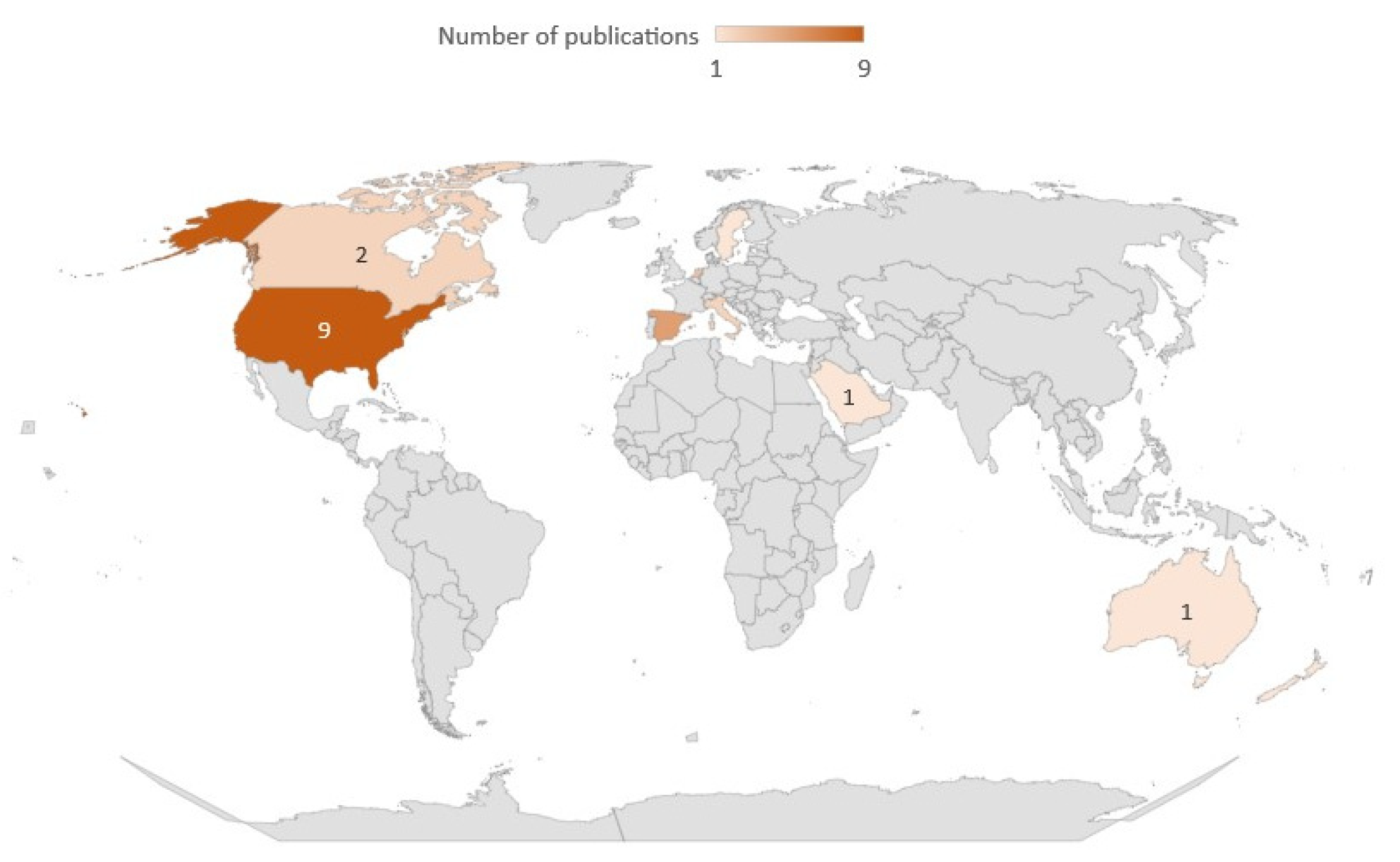
4.4. Research Impact, Authors’ Productivity, and Other Metrics
5. Discussion
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A




References
- Muktamath, V.R.; Hegde, P.; Chand, S. Types of Specific Learning Disability. In Learning Disabilities-Neurobiology, Assessment, Clinical Features and Treatments; IntechOpen: London, UK, 2022. [Google Scholar]
- Joyce-Beaulieu, D.; Sulkowski, M.L. The Diagnostic and Statistical Manual of Mental Disorders: Fifth Edition (DSM-5) Model of Impairment. In Assessing Impairment; Springer: Boston, MA, USA, 2016; pp. 167–189. [Google Scholar]
- Sisk, D. Managing the Emotional Intensities of Gifted Students with Mindfulness Practices. Educ. Sci. 2021, 11, 731. [Google Scholar] [CrossRef]
- Prasittichok, P.; Klaykaew, K.K. Meta-Skills Development Needs Assessment among Undergraduate Students. Heliyon 2022, 8, e08787. [Google Scholar] [CrossRef] [PubMed]
- Drigas, A.; Mitsea, E. 8 Pillars X 8 Layers Model of Metacognition: Educational Strategies, Exercises &Trainings. Int. J. Online Biomed. Eng. iJOE. 2021, 17, 115. [Google Scholar] [CrossRef]
- Chernyavskaya, V.S.; Malakhova, V.R. Features of Meta-Competences in Primary School Children. Procedia—Soc. Behav. Sci. 2016, 233, 352–356. [Google Scholar] [CrossRef]
- Senova, M. Meta-skills are the key to human potential. J. Behav. Econ. Soc. Syst. 2020, 2, 133–137. [Google Scholar] [CrossRef]
- Mayer, J.D.; Salovey, P. The Intelligence of Emotional Intelligence. Intelligence 1993, 17, 433–442. [Google Scholar] [CrossRef]
- D’Amico, A.; Geraci, A. Beyond Emotional Intelligence: The New Construct of Meta-Emotional Intelligence. Front. Psychol. 2023, 14, 1096663. [Google Scholar] [CrossRef]
- Kabat-Zinn, J. Mindfulness-Based Interventions in Context: Past, Present, and Future. Clin. Psychol. Sci. Pract. 2003, 10, 144–156. [Google Scholar] [CrossRef]
- Shapiro, S.L. The Integration of Mindfulness and Psychology. J. Clin. Psychol. 2009, 65, 555–560. [Google Scholar] [CrossRef]
- Malinowski, P. Mindfulness as Psychological Dimension: Concepts and Applications. Ir. J. Psychol. 2008, 29, 155–166. [Google Scholar] [CrossRef]
- Walsh, R.; Shapiro, S.L. The Meeting of Meditative Disciplines and Western Psychology: A Mutually Enriching Dialogue. Am. Psychol. 2006, 61, 227–239. [Google Scholar] [CrossRef] [PubMed]
- Creswell, J.D. Mindfulness Interventions. Annu. Rev. Psychol. 2017, 68, 491–516. [Google Scholar] [CrossRef]
- Reangsing, C.; Punsuwun, S.; Schneider, J.K. Effects of Mindfulness Interventions on Depressive Symptoms in Adolescents: A Meta-Analysis. Int. J. Nurs. Stud. 2021, 115, 103848. [Google Scholar] [CrossRef]
- Borquist-Conlon, D.S.; Maynard, B.R.; Brendel, K.E.; Farina, A.S.J. Mindfulness-Based Interventions for Youth with Anxiety: A Systematic Review and Meta-Analysis. Res. Soc. Work Pract. 2017, 29, 195–205. [Google Scholar] [CrossRef]
- Lee, Y.-C.; Chen, C.-R.; Lin, K.-C. Effects of Mindfulness-Based Interventions in Children and Adolescents with ADHD: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Int. J. Environ. Res. Public Health 2022, 19, 15198. [Google Scholar] [CrossRef] [PubMed]
- Cachia, R.L.; Anderson, A.; Moore, D.W. Mindfulness in Individuals with Autism Spectrum Disorder: A Systematic Review and Narrative Analysis. Rev. J. Autism Dev. Disord. 2016, 3, 165–178. [Google Scholar] [CrossRef]
- Linardon, J. Can Acceptance, Mindfulness, and Self-Compassion Be Learned by Smartphone Apps? A Systematic and Meta-Analytic Review of Randomized Controlled Trials. Behav. Ther. 2020, 51, 646–658. [Google Scholar] [CrossRef] [PubMed]
- Döllinger, N.; Wienrich, C.; Latoschik, M.E. Challenges and Opportunities of Immersive Technologies for Mindfulness Meditation: A Systematic Review. Front. Virtual Real. 2021, 2, 644683. [Google Scholar] [CrossRef]
- Mikropoulos, T.A. Presence: A Unique Characteristic in Educational Virtual Environments. Virtual Real. 2006, 10, 197–206. [Google Scholar] [CrossRef]
- Mesa-Gresa, P.; Gil-Gómez, H.; Lozano-Quilis, J.-A.; Gil-Gómez, J.-A. Effectiveness of Virtual Reality for Children and Adolescents with Autism Spectrum Disorder: An Evidence-Based Systematic Review. Sensors 2018, 18, 2486. [Google Scholar] [CrossRef]
- Bashiri, A.; Ghazisaeedi, M.; Shahmoradi, L. The Opportunities of Virtual Reality in the Rehabilitation of Children with Attention Deficit Hyperactivity Disorder: A Literature Review. Korean J. Pediatr. 2017, 60, 337. [Google Scholar] [CrossRef] [PubMed]
- Nabors, L.; Monnin, J.; Jimenez, S. A Scoping Review of Studies on Virtual Reality for Individuals with Intellectual Disabilities. Adv. Neurodev. Disord. 2020, 4, 344–356. [Google Scholar] [CrossRef]
- Lozano-Álvarez, M.; Rodríguez-Cano, S.; Delgado-Benito, V.; Mercado-Val, E. A Systematic Review of Literature on Emerging Technologies and Specific Learning Difficulties. Educ. Sci. 2023, 13, 298. [Google Scholar] [CrossRef]
- Chandrasiri, A.; Collett, J.; Fassbender, E.; De Foe, A. A Virtual Reality Approach to Mindfulness Skills Training. Virtual Real. 2019, 24, 143–149. [Google Scholar] [CrossRef]
- Huguet, A.; Izaguirre Eguren, J.; Miguel-Ruiz, D.; Vall Vallés, X.; Alda, J.A. Deficient Emotional Self-Regulation in Children with Attention Deficit Hyperactivity Disorder: Mindfulness as a Useful Treatment Modality. J. Dev. Behav. Pediatr. 2019, 40, 425–431. [Google Scholar] [CrossRef]
- Lunsky, Y.; Redquest, B.; Albaum, C.; Hutton, S.; Share, M.; Share-Strom, D.; Weiss, J. Virtual Group–Based Mindfulness Intervention for Autistic Adults: A Feasibility Study. Mindfulness 2022, 13, 1706–1718. [Google Scholar] [CrossRef] [PubMed]
- Arpaia, P.; D’Errico, G.; De Paolis, L.T.; Moccaldi, N.; Nuccetelli, F. A Narrative Review of Mindfulness-Based Interventions Using Virtual Reality. Mindfulness 2021, 13, 556–571. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.-Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A Revised Tool for Assessing Risk of Bias in Randomised Trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef]
- Sterne, J.A.; Hernán, M.A.; Reeves, B.C.; Savović, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I.; et al. ROBINS-I: A Tool for Assessing Risk of Bias in Non-Randomised Studies of Interventions. BMJ 2016, 366, i4919. [Google Scholar] [CrossRef]
- McGuinness, L.A.; Higgins, J.P.T. Risk-of-bias VISualization (Robvis): An R Package and Shiny Web App for Visualizing Risk-of-bias Assessments. Res. Synth. Methods 2020, 12, 55–61. [Google Scholar] [CrossRef]
- Flavell, J.H. Metacognition and Cognitive Monitoring: A New Area of Cognitive–Developmental Inquiry. Am. Psychol. 1979, 34, 906–911. [Google Scholar] [CrossRef]
- Fleur, D.S.; Bredeweg, B.; van den Bos, W. Metacognition: Ideas and Insights from Neuro- and Educational Sciences. NPJ Sci. Learn. 2021, 6, 13. [Google Scholar] [CrossRef] [PubMed]
- Drigas, A.; Mitsea, E. The 8 Pillars of Metacognition. Int. J. Emerg. Technol. Learn. (iJET) 2020, 15, 162. [Google Scholar] [CrossRef]
- Jankowski, T.; Holas, P. Metacognitive Model of Mindfulness. Conscious. Cogn. 2014, 28, 64–80. [Google Scholar] [CrossRef]
- Vickery, C.E.; Dorjee, D. Mindfulness Training in Primary Schools Decreases Negative Affect and Increases Meta-Cognition in Children. Front. Psychol. 2016, 6, 2025. [Google Scholar] [CrossRef] [PubMed]
- Vago, D.R.; David, S.A. Self-awareness, self-regulation, and self-transcendence (S-ART): A framework for understanding the neurobiological mechanisms of mindfulness. Front. Hum. Neurosci. 2012, 6, 296. [Google Scholar] [CrossRef]
- Hölzel, B.K.; Lazar, S.W.; Gard, T.; Schuman-Olivier, Z.; Vago, D.R.; Ott, U. How Does Mindfulness Meditation Work? Proposing Mechanisms of Action from a Conceptual and Neural Perspective. Perspect. Psychol. Sci. 2011, 6, 537–559. [Google Scholar] [CrossRef]
- Lutz, A.; Slagter, H.A.; Dunne, J.D.; Davidson, R.J. Attention Regulation and Monitoring in Meditation. Trends Cogn. Sci. 2008, 12, 163–169. [Google Scholar] [CrossRef]
- Soler, J.; Elices, M.; Pascual, J.C.; Martín-Blanco, A.; Feliu-Soler, A.; Carmona, C.; Portella, M.J. Effects of Mindfulness Training on Different Components of Impulsivity in Borderline Personality Disorder: Results from a Pilot Randomized Study. Borderline Personal. Disord. Emot. Dysregulation 2016, 3, 1. [Google Scholar] [CrossRef]
- Pozuelos, J.P.; Mead, B.R.; Rueda, M.R.; Malinowski, P. Short-Term Mindful Breath Awareness Training Improves Inhibitory Control and Response Monitoring. Prog. Brain Res. 2019, 244, 137–163. [Google Scholar] [CrossRef] [PubMed]
- Sanger, K.L.; Dorjee, D. Mindfulness Training with Adolescents Enhances Metacognition and the Inhibition of Irrelevant Stimuli: Evidence from Event-Related Brain Potentials. Trends Neurosci. Educ. 2016, 5, 1–11. [Google Scholar] [CrossRef]
- Tang, Y.-Y.; Hölzel, B.K.; Posner, M.I. The Neuroscience of Mindfulness Meditation. Nat. Rev. Neurosci. 2015, 16, 213–225. [Google Scholar] [CrossRef] [PubMed]
- Moore, A.; Malinowski, P. Meditation, Mindfulness and Cognitive Flexibility. Conscious. Cogn. 2009, 18, 176–186. [Google Scholar] [CrossRef] [PubMed]
- Davis, D.M.; Hayes, J.A. What Are the Benefits of Mindfulness? A Practice Review of Psychotherapy-Related Research. Psychotherapy 2011, 48, 198–208. [Google Scholar] [CrossRef] [PubMed]
- Tan, L.B.G.; Lo, B.C.Y.; Macrae, C.N. Brief Mindfulness Meditation Improves Mental State Attribution and Empathizing. PLoS ONE 2014, 9, e110510. [Google Scholar] [CrossRef]
- Drigas, A.; Mitsea, E. A Metacognition Based 8 Pillars Mindfulness Model and Training Strategies. Int. J. Recent Contrib. Eng. Sci. IT 2020, 8, 4–17. [Google Scholar] [CrossRef]
- Miao, C.; Humphrey, R.H.; Qian, S. The Relationship between Emotional Intelligence and Trait Mindfulness: A Meta-Analytic Review. Personal. Individ. Differ. 2018, 135, 101–107. [Google Scholar] [CrossRef]
- Jiménez-Picón, N.; Romero-Martín, M.; Ponce-Blandón, J.A.; Ramirez-Baena, L.; Palomo-Lara, J.C.; Gómez-Salgado, J. The Relationship between Mindfulness and Emotional Intelligence as a Protective Factor for Healthcare Professionals: Systematic Review. Int. J. Environ. Res. Public Health 2021, 18, 5491. [Google Scholar] [CrossRef]
- Schutte, N.S.; Malouff, J.M. Emotional Intelligence Mediates the Relationship between Mindfulness and Subjective Well-Being. Personal. Individ. Differ. 2011, 50, 1116–1119. [Google Scholar] [CrossRef]
- Hill, C.L.M.; Updegraff, J.A. Mindfulness and Its Relationship to Emotional Regulation. Emotion 2012, 12, 81–90. [Google Scholar] [CrossRef] [PubMed]
- Swathi, P.S.; Bhat, R.; Saoji, A.A. Effect of Trataka (Yogic Visual Concentration) on the Performance in the Corsi-Block Tapping Task: A Repeated Measures Study. Front. Psychol. 2021, 12, 773049. [Google Scholar] [CrossRef] [PubMed]
- Zaccaro, A.; Piarulli, A.; Laurino, M.; Garbella, E.; Menicucci, D.; Neri, B.; Gemignani, A. How Breath-Control Can Change Your Life: A Systematic Review on Psycho-Physiological Correlates of Slow Breathing. Front. Hum. Neurosci. 2018, 12, 353. [Google Scholar] [CrossRef] [PubMed]
- Mitsea, E.; Drigas, A.; Skianis, C. Cutting-Edge Technologies in Breathwork for Learning Disabilities in Special Education. Tech. Soc. Sci. J. 2022, 34, 136–157. [Google Scholar] [CrossRef]
- Mitsea, E.; Drigas, A.; Skianis, C. Breathing, Attention & Consciousness in Sync: The Role of Breathing Training, Metacognition & Virtual Reality. Tech. Soc. Sci. J. 2022, 29, 79–97. [Google Scholar] [CrossRef]
- Dulčić, F.J.L. La Práctica Del Silencio Como Una Herramienta Educativa: Directrices Para La Educación Basada En Competencias. Educ. E Pesqui. 2021, 47, e224651. [Google Scholar] [CrossRef]
- Wittmann, M.; Schmidt, S. Mindfulness Meditation and the Experience of Time. In Meditation—Neuroscientific Approaches and Philosophical Implications; Springer: Cham, Switzerland, 2013; pp. 199–209. [Google Scholar] [CrossRef]
- Mellenthin, C. Guided Imagery. In Play Therapy with Children: Modalities for Change Modalities for Change; American Psychological Association: Washington, DC, USA, 2021; pp. 125–139. [Google Scholar] [CrossRef]
- Toussaint, L.; Nguyen, Q.A.; Roettger, C.; Dixon, K.; Offenbächer, M.; Kohls, N.; Hirsch, J.; Sirois, F. Effectiveness of Progressive Muscle Relaxation, Deep Breathing, and Guided Imagery in Promoting Psychological and Physiological States of Relaxation. Evid. -Based Complement. Altern. Med. 2021, 2021, 5924040. [Google Scholar] [CrossRef]
- Hilert, A.J.; Tirado, C. Teaching Multicultural Counseling with Mindfulness: A Contemplative Pedagogy Approach. Int. J. Adv. Couns. 2018, 41, 469–480. [Google Scholar] [CrossRef]
- Cohen, G.L.; Sherman, D.K. The Psychology of Change: Self-Affirmation and Social Psychological Intervention. Annu. Rev. Psychol. 2014, 65, 333–371. [Google Scholar] [CrossRef]
- Schmeichel, B.J.; Vohs, K. Self-Affirmation and Self-Control: Affirming Core Values Counteracts Ego Depletion. J. Personal. Soc. Psychol. 2009, 96, 770–782. [Google Scholar] [CrossRef]
- Sansone, R.; Sansone, L. Gratitude and well being: The benefits of appreciation. Psychiatry 2010, 7, 18–22. [Google Scholar]
- Jans-Beken, L.; Jacobs, N.; Janssens, M.; Peeters, S.; Reijnders, J.; Lechner, L.; Lataster, J. Gratitude and Health: An Updated Review. J. Posit. Psychol. 2019, 15, 743–782. [Google Scholar] [CrossRef]
- Hazlett, L.I.; Moieni, M.; Irwin, M.R.; Haltom, K.E.B.; Jevtic, I.; Meyer, M.L.; Breen, E.C.; Cole, S.W.; Eisenberger, N.I. Exploring Neural Mechanisms of the Health Benefits of Gratitude in Women: A Randomized Controlled Trial. Brain Behav. Immun. 2021, 95, 444–453. [Google Scholar] [CrossRef] [PubMed]
- Gan, R.; Zhang, L.; Chen, S. The Effects of Body Scan Meditation: A Systematic Review and Meta-analysis. Appl. Psychol. Health Well-Being 2022, 14, 1062–1080. [Google Scholar] [CrossRef] [PubMed]
- Schultchen, D.; Messner, M.; Karabatsiakis, A.; Schillings, C.; Pollatos, O. Effects of an 8-Week Body Scan Intervention on Individually Perceived Psychological Stress and Related Steroid Hormones in Hair. Mindfulness 2019, 10, 2532–2543. [Google Scholar] [CrossRef]
- Penazzi, G.; De Pisapia, N. Direct Comparisons between Hypnosis and Meditation: A Mini-Review. Front. Psychol. 2022, 13, 1–7. [Google Scholar] [CrossRef]
- Drigas, A.; Mitsea, E.; Skianis, C. The Role of Clinical Hypnosis & VR in Special Education. Int. J. Recent Contrib. Eng. Sci. IT (iJES) 2021, 9, 4–18. [Google Scholar] [CrossRef]
- Olendzki, N.; Elkins, G.R.; Slonena, E.; Hung, J.; Rhodes, J.R. Mindful Hypnotherapy to Reduce Stress and Increase Mindfulness: A Randomized Controlled Pilot Study. Int. J. Clin. Exp. Hypn. 2020, 68, 151–166. [Google Scholar] [CrossRef]
- Wake, L.; Leighton, M. Pilot Study Using Neurolinguistic Programming (NLP) in Post-Combat PTSD. Ment. Health Rev. J. 2014, 19, 251–264. [Google Scholar] [CrossRef]
- Drigas, A.; Mitsea, E.; Skianis, C. Neuro-Linguistic Programming, Positive Psychology & VR in Special Education. Sci. Electron. Arch. 2021, 15, 30–39. [Google Scholar] [CrossRef]
- Allen, J.G.; Romate, J.; Rajkumar, E. Mindfulness-Based Positive Psychology Interventions: A Systematic Review. BMC Psychol. 2021, 9, 116. [Google Scholar] [CrossRef] [PubMed]
- Bolier, L.; Haverman, M.; Westerhof, G.J.; Riper, H.; Smit, F.; Bohlmeijer, E. Positive Psychology Interventions: A Meta-Analysis of Randomized Controlled Studies. BMC Public Health 2013, 13, 119. [Google Scholar] [CrossRef] [PubMed]
- Yildirim, C.; O’Grady, T. The Efficacy of a Virtual Reality-Based Mindfulness Intervention. In Proceedings of the 2020 IEEE International Conference on Artificial Intelligence and Virtual Reality (AIVR), Utrecht, The Netherlands, 14–18 December 2020. [Google Scholar] [CrossRef]
- Savickaite, S.; Husselman, T.-A.; Taylor, R.; Millington, E.; Hayashibara, E.; Arthur, T. Applications of Virtual Reality (VR) in Autism Research: Current Trends and Taxonomy of Definitions. J. Enabling Technol. 2022, 16, 147–154. [Google Scholar] [CrossRef]
- Schuemie, M.J.; van der Straaten, P.; Krijn, M.; van der Mast, C.A.P.G. Research on Presence in Virtual Reality: A Survey. CyberPsychology Behav. 2001, 4, 183–201. [Google Scholar] [CrossRef]
- Griffith, R.L.; Steelman, L.A.; Wildman, J.L.; LeNoble, C.A.; Zhou, Z.E. Guided Mindfulness: A Self-Regulatory Approach to Experiential Learning of Complex Skills. Theor. Issues Ergon. Sci. 2016, 18, 147–166. [Google Scholar] [CrossRef]
- Asad, M.M.; Naz, A.; Churi, P.; Tahanzadeh, M.M. Virtual Reality as Pedagogical Tool to Enhance Experiential Learning: A Systematic Literature Review. Educ. Res. Int. 2021, 2021, 7061623. [Google Scholar] [CrossRef]
- Hudetz, J.A.; Hudetz, A.G.; Klayman, J. Relationship between Relaxation by Guided Imagery and Performance of Working Memory. Psychol. Rep. 2000, 86, 15–20. [Google Scholar] [CrossRef]
- Habak, S.; Bennett, J.; Davies, A.; Davies, M.; Christensen, H.; Boydell, K.M. Edge of the Present: A Virtual Reality Tool to Cultivate Future Thinking, Positive Mood and Wellbeing. Int. J. Environ. Res. Public Health 2020, 18, 140. [Google Scholar] [CrossRef]
- Choo, A.; May, A. Virtual Mindfulness Meditation: Virtual Reality and Electroencephalography for Health Gamification. In Proceedings of the 2014 IEEE Games Media Entertainment, Toronto, ON, Canada, 22–24 October 2014. [Google Scholar] [CrossRef]
- Bruggeman, K.J.; Wurster, S.W. The Hiatus System. In ACM SIGGRAPH 2018 Appy Hour; Association for Computing Machinery: New York, NY, USA, 2018. [Google Scholar] [CrossRef]
- Seabrook, E.; Kelly, R.; Foley, F.; Theiler, S.; Thomas, N.; Wadley, G.; Nedeljkovic, M. Understanding How Virtual Reality Can Support Mindfulness Practice: Mixed Methods Study. J. Med. Internet Res. 2020, 22, e16106. [Google Scholar] [CrossRef]
- Cikajlo, I.; Cizman Staba, U.; Vrhovac, S.; Larkin, F.; Roddy, M. A Cloud-Based Virtual Reality App for a Novel Telemindfulness Service: Rationale, Design and Feasibility Evaluation. JMIR Res. Protoc. 2017, 6, e108. [Google Scholar] [CrossRef]
- Cruea, M.D. Gaming the Mind and Minding the Game: Mindfulness and Flow in Video Games. In Video Games and Well-Being; Palgrave Pivot: Cham, Switzerland, 2019; pp. 97–107. [Google Scholar] [CrossRef]
- Santonastaso, O.; Zaccari, V.; Crescentini, C.; Fabbro, F.; Capurso, V.; Vicari, S.; Menghini, D. Clinical Application of Mindfulness-Oriented Meditation: A Preliminary Study in Children with ADHD. Int. J. Environ. Res. Public Health 2020, 17, 6916. [Google Scholar] [CrossRef] [PubMed]
- Zaccari, V.; Santonastaso, O.; Mandolesi, L.; De Crescenzo, F.; Foti, F.; Crescentini, C.; Fabbro, F.; Vicari, S.; Curcio, G.; Menghini, D. Clinical Application of Mindfulness-Oriented Meditation in Children with ADHD: A Preliminary Study on Sleep and Behavioral Problems. Psychol. Health 2022, 37, 563–579. [Google Scholar] [CrossRef] [PubMed]
- Juliano, A.C.; Alexander, A.O.; DeLuca, J.; Genova, H. Feasibility of a School-Based Mindfulness Program for Improving Inhibitory Skills in Children with Autism Spectrum Disorder. Res. Dev. Disabil. 2020, 101, 103641. [Google Scholar] [CrossRef] [PubMed]
- Spek, A.A.; van Ham, N.C.; Nyklíček, I. Mindfulness-Based Therapy in Adults with an Autism Spectrum Disorder: A Randomized Controlled Trial. Res. Dev. Disabil. 2013, 34, 246–253. [Google Scholar] [CrossRef]
- Reese, H.E.; Vallejo, Z.; Rasmussen, J.; Crowe, K.; Rosenfield, E.; Wilhelm, S. Mindfulness-Based Stress Reduction for Tourette Syndrome and Chronic Tic Disorder: A Pilot Study. J. Psychosom. Res. 2015, 78, 293–298. [Google Scholar] [CrossRef]
- Singh, N.N.; Wahler, R.G.; Adkins, A.D.; Myers, R.E. Soles of the Feet: A Mindfulness-Based Self-Control Intervention for Aggression by an Individual with Mild Mental Retardation and Mental Illness. Res. Dev. Disabil. 2003, 24, 158–169. [Google Scholar] [CrossRef]
- Singh, N.N.; Lancioni, G.E.; Winton, A.S.W.; Adkins, A.D.; Singh, J.; Singh, A.N. Mindfulness Training Assists Individuals with Moderate Mental Retardation to Maintain Their Community Placements. Behav. Modif. 2007, 31, 800–814. [Google Scholar] [CrossRef]
- Tarrasch, R.; Berman, Z.; Friedmann, N. Mindful Reading: Mindfulness Meditation Helps Keep Readers with Dyslexia and ADHD on the Lexical Track. Front. Psychol. 2016, 7, 578. [Google Scholar] [CrossRef]
- Pradhan, B.; Parikh, T.; Sahoo, M.; Selznick, R.; Goodman, M. Current Understanding of Dyslexia and Pilot Data on Efficacy of a Mindfulness Based Psychotherapy (MBR-RAM) Model. Adolesc. Psychiatry 2017, 7, 44–55. [Google Scholar] [CrossRef]
- Turanzas, J.A.; Cordón, J.R.; Choca, J.P.; Mestre, J.M. Evaluating the APAC (Mindfulness for Giftedness) Program in a Spanish Sample of Gifted Children: A Pilot Study. Mindfulness 2018, 11, 86–98. [Google Scholar] [CrossRef]
- Olton-Weber, S.; Hess, R.; Ritchotte, J.A. Reducing Levels of Perfectionism in Gifted and Talented Youth Through a Mindfulness Intervention. Gift. Child Q. 2020, 64, 319–330. [Google Scholar] [CrossRef]
- Serra Pla, J.F.; Pozuelo, M.; Richarte, V.; Corrales, M.; Ibáñez, P.; Bellina, M.; Vidal, R.; Calvo, E.; Casas Brugué, M.; Ramos Quiroga, J.A. Treatment of attention deficit hyperactivity disorder in adults using virtual reality through a mindfulness programme. Rev. De Neurol. 2017, 64, S117. [Google Scholar] [CrossRef]
- Bossenbroek, R.; Wols, A.; Weerdmeester, J.; Lichtwarck-Aschoff, A.; Granic, I.; van Rooij, M.M.J.W. Efficacy of a Virtual Reality Biofeedback Game (DEEP) to Reduce Anxiety and Disruptive Classroom Behavior: Single-Case Study. JMIR Ment. Health 2020, 7, e16066. [Google Scholar] [CrossRef] [PubMed]
- Modrego-Alarcón, M.; López-del-Hoyo, Y.; García-Campayo, J.; Pérez-Aranda, A.; Navarro-Gil, M.; Beltrán-Ruiz, M.; Morillo, H.; Delgado-Suarez, I.; Oliván-Arévalo, R.; Montero-Marin, J. Efficacy of a Mindfulness-Based Programme with and without Virtual Reality Support to Reduce Stress in University Students: A Randomized Controlled Trial. Behav. Res. Ther. 2021, 142, 103866. [Google Scholar] [CrossRef] [PubMed]
- Chavez, L.J.; Kelleher, K.; Slesnick, N.; Holowacz, E.; Luthy, E.; Moore, L.; Ford, J. Virtual Reality Meditation Among Youth Experiencing Homelessness: Pilot Randomized Controlled Trial of Feasibility. JMIR Ment. Health 2020, 7, e18244. [Google Scholar] [CrossRef]
- Mistry, D.; Zhu, J.; Tremblay, P.; Wekerle, C.; Lanius, R.; Jetly, R.; Frewen, P. Meditating in Virtual Reality: Proof-of-Concept Intervention for Posttraumatic Stress. Psychol. Trauma Theory Res. Pract. Policy 2020, 12, 847–858. [Google Scholar] [CrossRef]
- Tarrant, J.; Viczko, J.; Cope, H. Virtual Reality for Anxiety Reduction Demonstrated by Quantitative EEG: A Pilot Study. Front. Psychol. 2018, 9, 1280. [Google Scholar] [CrossRef]
- Gomez, J.; Hoffman, H.G.; Bistricky, S.L.; Gonzalez, M.; Rosenberg, L.; Sampaio, M.; Garcia-Palacios, A.; Navarro-Haro, M.V.; Alhalabi, W.; Rosenberg, M.; et al. The Use of Virtual Reality Facilitates Dialectical Behavior Therapy® “Observing Sounds and Visuals” Mindfulness Skills Training Exercises for a Latino Patient with Severe Burns: A Case Study. Front. Psychol. 2017, 8, 1611. [Google Scholar] [CrossRef]
- Navarro-Haro, M.V.; Modrego-Alarcón, M.; Hoffman, H.G.; López-Montoyo, A.; Navarro-Gil, M.; Montero-Marin, J.; García-Palacios, A.; Borao, L.; García-Campayo, J. Evaluation of a Mindfulness-Based Intervention with and without Virtual Reality Dialectical Behavior Therapy® Mindfulness Skills Training for the Treatment of Generalized Anxiety Disorder in Primary Care: A Pilot Study. Front. Psychol. 2019, 10, 55. [Google Scholar] [CrossRef]
- Shiban, Y.; Diemer, J.; Müller, J.; Brütting-Schick, J.; Pauli, P.; Mühlberger, A. Diaphragmatic Breathing during Virtual Reality Exposure Therapy for Aviophobia: Functional Coping Strategy or Avoidance Behavior? A Pilot Study. BMC Psychiatry 2017, 17, 29. [Google Scholar] [CrossRef]
- Lacey, C.; Frampton, C.; Beaglehole, B. oVRcome—Self-Guided Virtual Reality for Specific Phobias: A Randomised Controlled Trial. Aust. New Zealand J. Psychiatry 2022, 57, 736–744. [Google Scholar] [CrossRef]
- Seol, E.; Min, S.; Seo, S.; Jung, S.; Lee, Y.; Lee, J.; Kim, G.; Cho, C.; Lee, S.; Cho, C.-H.; et al. “Drop the Beat”. In Proceedings of the 23rd ACM Symposium on Virtual Reality Software and Technology, Gothenburg, Sweden, 8–10 November 2017. [Google Scholar] [CrossRef]
- Nararro-Haro, M.V.; Hoffman, H.G.; Garcia-Palacios, A.; Sampaio, M.; Alhalabi, W.; Hall, K.; Linehan, M. The Use of Virtual Reality to Facilitate Mindfulness Skills Training in Dialectical Behavioral Therapy for Borderline Personality Disorder: A Case Study. Front. Psychol. 2016, 7, 1573. [Google Scholar] [CrossRef] [PubMed]
- Veling, W.; Lestestuiver, B.; Jongma, M.; Hoenders, H.J.R.; van Driel, C. Virtual Reality Relaxation for Patients with a Psychiatric Disorder: Crossover Randomized Controlled Trial. J. Med. Internet Res. 2021, 23, e17233. [Google Scholar] [CrossRef] [PubMed]
- Ilioudi, M.; Lindner, P.; Ali, L.; Wallström, S.; Thunström, A.O.; Ioannou, M.; Anving, N.; Johansson, V.; Hamilton, W.; Falk, Ö.; et al. Physical Versus Virtual Reality–Based Calm Rooms for Psychiatric Inpatients: Quasi-Randomized Trial. J. Med. Internet Res. 2023, 25, e42365. [Google Scholar] [CrossRef]
- Ma, J.; Zhao, D.; Xu, N.; Yang, J. The Effectiveness of Immersive Virtual Reality (VR) Based Mindfulness Training on Improvement Mental-Health in Adults: A Narrative Systematic Review. Explore 2023, 19, 310–318. [Google Scholar] [CrossRef] [PubMed]
- Simón-Vicente, L.; Rodríguez-Cano, S.; Delgado-Benito, V.; Ausín-Villaverde, V.; Cubo Delgado, E. Cybersickness. A Systematic Literature Review of Adverse Effects Related to Virtual Reality. Neurología 2022. [Google Scholar] [CrossRef]
- Baniasadi, T.; Ayyoubzadeh, S.M.; Mohammadzadeh, N. Challenges and Practical Considerations in Applying Virtual Reality in Medical Education and Treatment. Oman Med. J. 2020, 35, e125. [Google Scholar] [CrossRef]
- Russell, M.E.B.; Hoffman, B.; Stromberg, S.; Carlson, C.R. Use of Controlled Diaphragmatic Breathing for the Management of Motion Sickness in a Virtual Reality Environment. Appl. Psychophysiol. Biofeedback 2014, 39, 269–277. [Google Scholar] [CrossRef]
- Lie, S.S.; Helle, N.; Sletteland, N.V.; Vikman, M.D.; Bonsaksen, T. Implementation of Virtual Reality in Health Professions Education: Scoping Review. JMIR Med. Educ. 2023, 9, e41589. [Google Scholar] [CrossRef]
- Grossman, P.; Niemann, L.; Schmidt, S.; Walach, H. Mindfulness-Based Stress Reduction and Health Benefits. J. Psychosom. Res. 2004, 57, 35–43. [Google Scholar] [CrossRef]
- Kretschmer, C.R.; Göz Tebrizcik, B.; Dommett, E.J. Mindfulness Interventions for Attention Deficit Hyperactivity Disorder: A Systematic Review and Meta-Analysis. Psychiatry Int. 2022, 3, 363–399. [Google Scholar] [CrossRef]
- Shapero, B.G.; Greenberg, J.; Pedrelli, P.; de Jong, M.; Desbordes, G. Mindfulness-Based Interventions in Psychiatry. Focus 2018, 16, 32–39. [Google Scholar] [CrossRef]
- Groves, P. Mindfulness in Psychiatry—Where Are We Now? BJPsych Bull. 2016, 40, 289–292. [Google Scholar] [CrossRef] [PubMed]
- Zhang, S.; Chen, M.; Yang, N.; Lu, S.; Ni, S. Effectiveness of VR Based Mindfulness on Psychological and Physiological Health: A Systematic Review. Curr. Psychol. 2021, 42, 5033–5045. [Google Scholar] [CrossRef]
- Failla, C.; Marino, F.; Bernardelli, L.; Gaggioli, A.; Doria, G.; Chilà, P.; Minutoli, R.; Mangano, R.; Torrisi, R.; Tartarisco, G.; et al. Mediating Mindfulness-Based Interventions with Virtual Reality in Non-Clinical Populations: The State-of-the-Art. Healthcare 2022, 10, 1220. [Google Scholar] [CrossRef]
- Carsley, D.; Khoury, B.; Heath, N.L. Effectiveness of Mindfulness Interventions for Mental Health in Schools: A Comprehensive Meta-Analysis. Mindfulness 2017, 9, 693–707. [Google Scholar] [CrossRef]
- Kauhanen, L.; Wan Mohd Yunus, W.M.A.; Lempinen, L.; Peltonen, K.; Gyllenberg, D.; Mishina, K.; Gilbert, S.; Bastola, K.; Brown, J.S.L.; Sourander, A. A Systematic Review of the Mental Health Changes of Children and Young People before and during the COVID-19 Pandemic. Eur. Child Adolesc. Psychiatry 2022, 32, 995–1013. [Google Scholar] [CrossRef]
- Zhu, J.L.; Schülke, R.; Vatansever, D.; Xi, D.; Yan, J.; Zhao, H.; Xie, X.; Feng, J.; Chen, M.Y.; Sahakian, B.J.; et al. Mindfulness Practice for Protecting Mental Health during the COVID-19 Pandemic. Transl. Psychiatry 2021, 11, 329. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Inclusion | Exclusion |
|---|---|
|
|
| Searching String and Main Searching Terms |
|---|
| “Mindfulness” OR “Guided meditation” AND/OR “Virtual Reality” OR “VR” OR “3D” OR “Immersive technologies” AND “Attention Deficit/Hyperactivity Disorder” OR “Autism Spectrum Disorder” OR “Intellectual Disability” OR “Dyslexia” OR “Giftedness” OR “Specific Learning Difficulties” OR “Anxiety” OR “Depression” OR “Phobias” AND “Metacognitive Skills” OR “Self-regulation” OR “Emotion Regulation” OR “Self-awareness” OR “Emotional awareness” OR “Inhibition control” OR “Attention regulation” OR “Adaptability” |
| Reference | Country | Target Group | Participants | Duration | Mindfulness Program | Measurement | Research Design | Findings |
|---|---|---|---|---|---|---|---|---|
| Singh et al., 2003 [94] | USA | ID | n = 1, 27-year-old | 10 sessions, 30 mi./sessions | Soles of the Feet | Staff- and self-reported behaviors | Case study | Improved self-control |
| Singh et al., 2007 [95] | USA | ID | n = 3 27–43 years | 10 sessions, 30 mi./sessions | Soles of the Feet | Staff- and self-reported behaviors, | Multiple baseline design | Better control of aggressive behavior |
| Huguet et al., 2019 [27] | Spain | ADHD | n =70 (nexp = 34, nclt = 36 7 to 12 years, F = 51, m = 19 Mage = 9 | 8 sessions, 75 min per session | MBCT | K-SADS-PL, Wisc-IV, DSM-IV-TR, CBCL | RCT | Enhanced emotional regulation |
| Tarrasch et al., 2016 [96] | Israel | LD (ADHD, DYX) | n = 24 24–48 years Mage = 30 | 8 weekly sessions | MBSR | MAAS, PSS, RRQ, SWLS | Feasibility Study | Improved impulse and attentional regulation, better reading skills |
| Zaccari et al., 2022 [90] | Italy | ADHD | n = 25 (nexp = 15, nclt = 10) Mage = 8.9 | 24 sessions, 6 min. and rising to 30 min. | Breathing, mindfulness of body parts, mindfulness of thoughts, mindful games | CBCL, CPRS-R:L, SDSC | RCT | Sleep improvements and better behavioral regulation |
| Reese et al., 2015 [93] | USA | TS | n = 18 16–67 years | 8 weekly 2-h classes and one 4-h retreat | MBSR | SCID, YGTSS, CGI-I, ATQ, WSAS | nRCT | Better control of tic intensity |
| Spek et al., 2013 [92] | Netherlands | ASD | n = 41, (nexp = 20, nClt = 21), 18 and 65 years | 9 weeks 40–60 min daily | Mindfulness-based-therapy for autism spectrum disorders | SCL-90-R RRQ GMS VCI, WAISIII | RCT | Better self-management of anxiety, depression, and rumination |
| Pradhan et al., 2017 [97] | USA | LD | n = 3, 8–10 years | 10 sessions, 30 min | MBR-RAM | WISC-IV, WIAT-III | Case study | Improved self-regulation, self-observation, and emotional regulation |
| Juliano et al., 2020 [91] | USA | ASD | n = 27 11–16 years, F = 21, M = 6, Mage = 13.60 | 16 sessions, 30 min/session | Mindful Schools curriculum | CWIT, CN | Feasibility study | Improved inhibitory control |
| Santonastaso et al., 2020 [89] | Italy | ADHD | n = 25 (nexp = 15, nclt = 10) 7–11 years Mage = 8.9 | 3 times per week for 8 weeks | Mindful breathing, body scan, self-observation of thoughts | CPT-II, CPRS-R:L, CBCL 6–18, CBCL 6–18, CDI, PSI-SF, | RCT | Improvements in attentional control, inhibition control, and emotional regulation |
| Turanzas et al., 2020 [98] | Spain | GIFT | n = 22 8–14 years Mage = 11.36 | 8 weekly 90-min group sessions | Mindfulness for Giftedness | CAMM, AFQ-Y, CDI, STAIC, PANAS-C, ESCQ | Pilot study | Improved emotional recognition and emotional regulation |
| Olton-Weber et al., 2020 [99] | USA | GIFT | n = 42, F = 18, M = 22, NB = 2, 11 to 14 years | 6 weeks | BREATHE | CAPS, CAMM | quasi-experimental design | Better recognition and regulation of self-imposed forms of perfectionism |
| Reference | Country | Clinical Condition | Sample | VR Design | Duration | Mindfulness Program | Type of Measurement | Research Design | Main Findings |
|---|---|---|---|---|---|---|---|---|---|
| Lunsky et al., 2022 [28] | Canada | ASD | n = 37 Mage = 31, F = 14, M = 21, NB = 2 | VR meeting platform | 6 weeks, 60 min per session | MBSR | DASS-21, FFMQ-SF, SCS-SF | Feasibility study | Better regulation of stress, connectedness |
| Veling et al., 2021 [112] | Netherlands | ANX, PSY, DEP or BPD | n = 50 (nexp = 25, nClt. = 25), F = 33, M = 17, Mage = 41.6 | Samsung Galaxy S6 or S7 smartphone, connected to the Samsung Gear VR HMD, VR relaxation software | 20 (minimum of 10 min, 10 consecutive days per session) | Guided meditation and progressive relaxation techniques | BAI, GPTS, IDS, PSS-10, VAS, SSQ | RCT | Improved ability to regulate negative emotions. Enhanced positive thinking. |
| Lacey et al., 2022 [109] | New Zealand | Specific Phobias | n = 126 (nexp = 51/63 analysed, nclt: 58/63 analysed), Mage = 42.2 | Smartphone app combined with the headset that holds the smartphone and uses 360° video | 6 weeks | Meditative techniques based on acceptance and flexibility around anxiety | SMSP, PHQ9, BFNE | RCT | Flexibility to behavioral change, optimism, better self-management of negative thoughts and fears |
| Chavez et al., 2020 [103] | USA | DEP, ANX, ADHD, BPD | n = 28 (n1 =8, n2= 11, n3 = 10) M= 15, F = 14 Mage = 21.6 | Oculus Go headset | 1 session | Guided meditation | STAI-6, salivary cortisol | RCT | Anxiety regulation, no difference in cortisol levels. |
| Shiban et al., 2017 [108] | Germany | DEP, PB | n= 29, (nexp = 15, nClt.= 14), Mage = 34.3, F = 24, M = 5 | V6 Head Mounted Display | 1 session | Mindful Breathing | HR, SCL, RR, ASI, FFS, FSB | RCT | Improved ability of self-control |
| Cikajlo et al., 2017 [87] | Ireland | ANX | n = 8 24–48 years | ReCoVR System Design, 3D VR headset | 8 weeks, 30 min/per session | MBSR | SWLS, MAAS | Feasibility Study | well-being, attention regulation, and anxiety management |
| Navarro et al., 2016 [111] | USA | BPD | n = 1, 32 years, F = 1 | Kaiser Electro-OpticsVR goggles | 4 sessions | DBT Mindfulness | DBT diary card, KIMS-Short, | Case study | Improved self-regulation, observation skills, emotional regulation |
| Navarro et al., 2019 [107] | Spain | GAD | n = 39 (nexp = 19, nCtl. = 20), F = 30, M = 9, Mage = 45.23 | Oculus Rift DK2 VR goggles with head-mounted display, with head tracking | 6 sessions | DBT Mindfulness skills training | GAD-7, HADS, FFMQ, DERS, VAAS | RCT | Improved self-regulation of anxiety, depression, and emotion regulation and interoceptive awareness. |
| Gomez et al., 2017 [106] | Saudi Arabia | ANX | n = 1, 21 years old | Oculus Rift DK2 VR goggles | 4 sessions | DBT® mindfulness skills training | PCL-C | Case study | Improvements in positive thinking, emotional regulation |
| Modrego-Alarcon et al., 2021 [102] | Spain | ANX | n = 280 (nexp = 93, nClt1 = 93, nclt2 = 94), F = 59, M = 221 Mage = 22.25 years | VR goggles | 6 weeks, once a week, 90 min per session | MBSR | PSS, STAI | RCT | Better self-control, emotional balance, reduced anxiety, academic engagement |
| Tarrant et al., 2018 [105] | USA | GAD | n = 26 (nexp = 14, nCtl.= 12), F = 20, M = 6, Mage = 46.21 | Gear VR HMD powered by Samsung S7, Mindfulness in nature experience, by StoryUp VR | a brief 75 min VR meditation intervention | Participants completed VR and non-VR meditations | GAD-7, STAI EEG patterns | RCT | Improved self-regulation of anxiety. VR group showed significant electrophysiological markers indicating lower anxiety |
| Mistry et al., 2020 [104] | Canada | PTSD | n = 96 (clinical sample: n = 26), F = 54, M = 42, Mage = 24.02 96 (54 females, 42 males). | Head Mounted Display | 1 session | Guided meditation | LEC-5, LES, ACE, PCL-5, MEQ, TRASC, mDES, BASS, | Within-group mixed-methods study | Positive affect increased. Improved emotional regulation ability. Better stress management. |
| Habak et al., 2021 [83] | Australia | DEP | n = 79, F = 53, M = 23 male, NB = 3, 25–34 years | VR headset | 3 sessions | Positive Visualizations | PANAS, BHS, SWEMWBS, | Pilot study | Better regulation of negative affect |
| Serra-Pla et al., 2017 [100] | Spain | ADHD | n = 50, nexp = 25, nclt = 25 | VR goggles | Four 30-min sessions | MBSR | Pre-treatment, post-treatment, and at 3- and 12-months post-treatment. | RCT | Improved self-management skills |
| Bossenbroek et al., 2020 [101] | Nehterlands | ADHD, ASD | n = 8 (F = 1, M = 7, Mage= 14.67 | Immersive VR biofeedback game | 4 weeks, 6 sessions. 15 min. | Mindful breathing | STAI, Likert Scale to measure disruptive classroom behavior | Single-case experimental study | Improved self-regulation skills |
| Seol et al., 2017 [110] | Korea | PD | n = 5 | Head-mounted display, leap motion sensor, PSL-lecg2 and Falcon device | 2 sessions | Mindfulness scenarios, breathing regulatory guidance | DASS | Pilot Study | Improved ability to consciously stabilize their state of mind. improved self-management of anxiety, and positive feelings of peacefulness. |
| Ilioudi et al., 2023 [113] | Sweden | DEP, BPD, ANX | n = 60, nexp = 40, nClt = 20, F = 35, M = 25 Mage = 39.1 | Head-mounted display (an Oculus Go) running in a mobile app | 1 session | Βreathing exercises, Guided relaxation | MADRS-S, BAI | Quasi RCT | Improved ability to induce self-relaxation |
| Source | Journal | Publisher | Quartile Score | SJR (2022) |
|---|---|---|---|---|
| [104] | Psychological Trauma: Theory, Research, Practice, and Policy | American Psychological Association | Q1 | 2.11 |
| [112,113] | Journal of Medical Internet Research (JMIR) | JMIR Publications Inc. | Q1 | 1.99 |
| [109] | Australian and New Zealand Journal of Psychiatry | SAGE Publications Ltd. | Q1 | 1.82 |
| [102] | Behaviour Research and Therapy | Elsevier Ltd. | Q1 | 1.79 |
| [101,103] | JMIR Mental Health | JMIR Publications Inc. | Q1 | 1.41 |
| [108] | BMC Psychiatry | BioMed Central Ltd. | Q1 | 1.29 |
| [28,98] | Mindfulness | Springer Verlag | Q1 | 1.26 |
| [93] | Journal of Psychosomatic Research | Elsevier Inc. | Q1 | 1.13 |
| [90] | Psychology and Health | Routledge | Q1 | 1.03 |
| [99] | Gifted Child Quarterly | SAGE Publications Inc. | Q1 | 0.93 |
| [95] | Behavior Modification | SAGE Publications Inc. | Q1 | 0.9 |
| [27] | Journal of Developmental & Behavioral Pediatrics (JDBP) | Lippincott Williams and Wilkins Ltd. | Q1 | 0.75 |
| [96,105,106,107,111] | Frontiers in Psychology | Frontiers Media S.A. | Q2 | 0.89 |
| [83,89] | International Journal of Environmental Research and Public Health | Multidisciplinary Digital Publishing Institute (MDPI) | Q2 | 0.83 |
| [91,92,94] | Research in Developmental Disabilities | Elsevier Inc. | Q2 | 0.77 |
| [87] | JMIR Research Protocols | JMIR Publications Inc. | Q2 | 0.53 |
| [100] | Revista de Neurologia | Revista de Neurologia | Q3 | 0.29 |
| [97] | Adolescent Psychiatry | Bentham Science Publishers B.V. | Not yet assigned | - |
| [110] | Proceedings of the ACM Symposium on Virtual Reality Software and Technology, VRST | Association for Computing Machinery | Not yet assigned | - |
| Source | First Author Name | Total Publications | h-Index | Total Citations |
|---|---|---|---|---|
| [94,95] | Singh, Nirbhay | 612 | 45 | 12,822 |
| [28] | Lunsky, Yona J. | 279 | 37 | 5019 |
| [112] | Veling, Wim | 116 | 31 | 3038 |
| [27] | Huguet, Anna | 64 | 27 | 3752 |
| [96] | Tarrasch, Ricardo | 78 | 26 | 2401 |
| [109] | Lacey, Cameron J. | 105 | 19 | 1436 |
| [90] | Zaccari, Vittorio | 82 | 19 | 1242 |
| [93] | Reese, Hannah | 38 | 17 | 1523 |
| [103] | Chavez, Laura Johnson | 54 | 16 | 678 |
| [108] | Shiban, Youssef | 35 | 15 | 1638 |
| [87] | Cikajlo, Imre | 77 | 14 | 900 |
| [92] | Spek, Annelies | 25 | 13 | 718 |
| [97] | Pradhan, Basant | 31 | 11 | 443 |
| [107,111] | Navarro-Haro, María V. | 25 | 10 | 438 |
| [106] | Gómez, Jocelyn | 11 | 9 | 198 |
| [102] | Modrego-Alarcón, Marta | 13 | 8 | 373 |
| [91] | Juliano, Anthony | 17 | 6 | 548 |
| [89] | Santonastaso, Ornella | 9 | 6 | 125 |
| [105] | Tarrant, Jeffrey M. | 10 | 5 | 236 |
| [104] | Mistry, Divya | 5 | 4 | 50 |
| [83] | Habak, Stephanie | 6 | 3 | 27 |
| [100] | Serra-Pla, Juanfran Francisco | 3 | 3 | 33 |
| [98] | Turanzas, Jorge | 3 | 3 | 32 |
| [110] | Seol, Eunbi | 3 | 3 | 30 |
| [101] | Bossenbroek, Rineke | 3 | 2 | 42 |
| [99] | Olton-Weber, Sophia | 1 | 1 | 28 |
| [113] | Ilioudi, Maria | 1 | 0 | 0 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mitsea, E.; Drigas, A.; Skianis, C. Virtual Reality Mindfulness for Meta-Competence Training among People with Different Mental Disorders: A Systematic Review. Psychiatry Int. 2023, 4, 324-353. https://doi.org/10.3390/psychiatryint4040031
Mitsea E, Drigas A, Skianis C. Virtual Reality Mindfulness for Meta-Competence Training among People with Different Mental Disorders: A Systematic Review. Psychiatry International. 2023; 4(4):324-353. https://doi.org/10.3390/psychiatryint4040031
Chicago/Turabian StyleMitsea, Eleni, Athanasios Drigas, and Charalabos Skianis. 2023. "Virtual Reality Mindfulness for Meta-Competence Training among People with Different Mental Disorders: A Systematic Review" Psychiatry International 4, no. 4: 324-353. https://doi.org/10.3390/psychiatryint4040031