1. Introduction
There is a growing scientific literature pointing at the negative consequences of the 2019 coronavirus disease (COVID-19) pandemic lockdowns for public health and psychological well-being [
1,
2,
3,
4,
5,
6,
7,
8]. However, the impact of lockdowns differed between individuals. Various factors have been suggested to influence the magnitude of the impact of lockdowns on mood and wellbeing, including but not limited to the duration of the lockdown, the extent of disruption of daily routines [
6], the level of social isolation [
9], the lack of psychological or physical coping strategies [
10], financial and career consequences [
6], and the impact of changes in lifestyle such as sleep, substance use, and nutrition [
6,
11].
Most governments around the world took preventive measures to limit the spread of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), including lockdowns. In the Netherlands, the first lockdown was enforced from 15th March to 11th May 2020, including the closure of schools, bars, restaurants, and all businesses except supermarkets and pharmacies. Except for those with essential occupations, such as the police and health workers, people were advised to work from home where possible. Leaving home was only allowed for essential activities, and meetings with more than three people were not allowed.
The first Dutch lockdown period was associated with a significant reduction in positive COVID-19 cases [
12,
13]. However, lockdown periods had a significant negative impact on people’s lives and psychological well-being. For example, lockdown periods have been associated with increased reporting of stress, anxiety, and depression [
4,
5,
6,
7,
8,
11]. However, several factors impacted the level at which individuals were affected by lockdown measures, including but not limited to a lack of coping strategies, financial burdens (e.g., job loss), lifestyle changes (e.g., sleep and dietary patterns), and disruption of daily routines [
6].
Of particular concern are vulnerable populations of individuals who are at increased risk when becoming infected with SARS-CoV-2, such as the elderly [
14], and those with underlying diseases, such as diabetes, asthma, and cardiovascular diseases [
15]. As these vulnerable populations may be more susceptible to lockdown-associated stress, this may lead to relapse or worsening of the course of their illness [
16,
17]. A systematic review [
18] confirmed that the psychological impact of the COVID-19 pandemic on the mental health of vulnerable populations was significantly greater compared to the general population.
The negative impact of mood changes during the COVID-19 pandemic among vulnerable populations should not be underestimated. For example, a study found that anxiety was the second highest risk factor of death among individuals with underlying diseases [
15]. When considering the impact of age on psychological well-being during the COVID-19 pandemic, one should take into account that the elderly more often have underlying diseases than younger adults. Several studies have described the impact of age on mental health responses during the COVID-19 pandemic. Studies revealed that older adults tend to report greater emotional well-being than younger people [
19,
20] and better coping strategies [
21]. The latter may be due to the fact that the ability of young people to cope with distressed situations and emotions may not be fully developed yet [
22,
23]. Research further showed that the elderly had less negativity towards the COVID-19 crisis than younger adults [
24]. The loss of social and work-related activities during lockdown periods may have had a greater negative impact on mental health among young adults. This could be related to the fact that the elderly more often already lived alone or did not participate in economic activities. However, other studies found increased levels of anxiety and depression among the elderly [
25,
26,
27,
28]. This was related to increased levels of social disconnectedness among the elderly and reduced access to health services [
29,
30,
31,
32]. Taken together, studies show mixed results regarding the impact of age on COVID-19 lockdown effects. Depending on the sociodemographic and health characteristics of individuals, increased levels of psychological distress during the COVID-19 pandemic [
33], or the absence thereof [
34], has been reported for both young adults and the elderly, and more research is needed on what factors make individuals more or less resilient to the health effects associated with COVID-19 lockdowns [
35].
Previous research revealed that immune fitness plays a central role in health and disease [
36] and also significantly impacted an individual’s vulnerability during the COVID-19 pandemic [
37]. Immune fitness can be defined as the body’s capacity to respond to health challenges (such as infections) by activating an appropriate immune response, which is essential to maintain health and prevent disease [
36]. Previous research revealed that poorer immune fitness in 2019 was the strongest predictor of reporting a greater number of COVID-19 symptoms and higher symptom severity ratings during the start of the pandemic [
37]. Therefore, in the current study, immune fitness was also assessed.
The first aim of the current study was to investigate the effects of the first COVID-19 lockdown in the Netherlands on mood, lifestyle factors, and coping strategies and whether these were different among vulnerable groups. To this extent, analyses were conducted to contrast subsamples according to sex, age, and having underlying diseases. A second aim of the study was to relate these findings with experienced immune fitness and the number and severity of reported COVID-19 symptoms. Taken together, the analysis aimed to identify vulnerable groups at risk that may need additional support from health professionals and service managers.
2. Methods
Directly after the first lockdown period in the Netherlands (between the 24th of June and the 26th of July 2020), an online survey was conducted among the Dutch general population [
38]. Participants were approached via Facebook advertisement, and the survey was designed in SurveyMonkey. Individuals could participate if they were aged 18 years and older. There were no exclusion criteria. The Ethics Committee of the Faculty of Social and Behavioral Sciences of Utrecht University approved the study (approval code: FETC17-061, approval date: 8 June 2017), and electronic informed consent was obtained from all participants. The survey comprised two parts. In Part I, demographics, mood, health correlates, and the number and severity of COVID-19 symptoms were assessed. In Part II, lifestyle factors and coping were assessed. A detailed description of the study methodology is published elsewhere [
38].
For the current analysis, demographic information on sex and age were considered. In addition, participants reported whether they had chronic health conditions, including the most common chronic diseases and conditions in Dutch adults and the elderly [
39]. These comprised cardiovascular diseases or hypertension, diabetes, liver disease, neurological diseases, immune disorders, allergy, kidney disease, pulmonary diseases, anxiety, depression, sleep disorders, or “other”. The open answers in the category “other” were reviewed by the study physician (J.B.), and if warranted, these were allocated to the appropriate disease category.
The assessments of mood, quality of life, lifestyle, immune fitness, and the number and severity of COVID-19 symptoms were made retrospectively for the period before the lockdown and for the first lockdown period.
Mood was assessed via single-item scales, with scores ranging from 0 (absent) to 10 (extreme). The assessed items included stress, anxiety, depression, fatigue, hostility, loneliness, and happiness. Quality of life was assessed using a single-item scale ranging from 0 (poor) to 10 (excellent). The mood and quality of life single-item scales have been validated previously and have a high test-retest reliability [
40,
41,
42]. Lifestyle factors of importance for coping and emotion regulation were assessed using a modified version of the FANTASTIC Lifestyle Checklist [
38,
43,
44,
45,
46]. For the domains ‘support of family and friends’, ‘physical activity level’, ‘nutrition’, and ‘coping with stress’ sum scores were computed, whereas single item scores were used for the items sleep (“I sleep well and feel rested”) and optimism (“I am a positive or optimistic thinker”). Higher scores on items or domains correspond to a better or healthier lifestyle. Finally, ‘being active’ was assessed with a 1-item scale, ranging from 0 (extremely inactive) to 10 (very active) [
42].
Immune fitness was assessed with a single-item scale ranging from 0 (poor) to 10 (excellent) [
36]. The number and severity of COVID-19 symptoms were assessed with a scale including the items: sneezing, running nose, sore throat, cough, malaise/feeling sick, high temperature (up to 38 Celsius), fever (38 Celsius and higher), shortness of breath, and chest pain [
38]. The items were rated as none (0), mild (1), moderate (2) or severe (3). The COVID-19 symptom severity score was computed as the sum score of the nine items (range 0 to 27), with higher scores implying a greater severity. The number of COVID-19 symptoms was the sum of items with a severity score greater than zero.
Data Analysis
The data were analyzed with SPSS (IBM Corp. Released 2013. IBM SPSS Statistics for Windows, Version 29.0. Armonk, NY, USA, IBM Corp.). Mean and standard deviation (SD) were computed for all variables, and distributions were checked for normality with the Kolmogorov–Smirnov test and by visual inspection. Demographics for men and women were compared using the Independent Samples Mann–Whitney U Test. Sex differences were considered significant if p < 0.05. Differences between ‘before COVID-19′ and ‘during the first COVID-19 lockdown’ were analyzed with the Related-Samples Wilcoxon Signed Ranks Test. Differences were considered significant if p < 0.00625 (applying a Bonferroni’s correction for multiple comparisons). For demographics and health correlates, the difference was considered significant if p < 0.05. Difference scores (Δ, during lockdown—before COVID-19) were computed for all variables. Spearman’s correlations were computed between these variables. Correlations were considered significant if p < 0.00625 (applying a Bonferroni’s correction for multiple comparisons).
3. Results
N = 1415 participants, with an age range of 18 to 94 years old, completed Part I of the survey. Their demographics are summarized in
Table 1. N = 514 participants also completed Part II of the survey, which included the assessments of lifestyle factors and coping. Significantly more women (64.5%) than men completed the survey. Women were significantly younger and had a lower BMI than men. The study outcomes are summarized in
Table 2.
For the lockdown period, significantly poorer mood and lifestyle ratings were reported, immune fitness was significantly poorer, and COVID-19 symptoms severity ratings were significantly higher.
Table 3 summarizes the correlations of the difference scores (during lockdown—before COVID-19) for mood, lifestyle factors, and health correlates with immune fitness and the number and severity of COVID-19 symptoms. The analysis revealed significant negative correlations between mood and immune fitness and significant positive correlations between mood and the number and severity of COVID-19 symptoms.
Significant correlations were found between changes in mood, immune fitness, and the number and severity of COVID-19 symptoms (see
Table 3). Most lifestyle factors also correlated significantly with immune fitness. Sleep, being active, and physical activity correlated significantly with the number and severity of COVID-19 symptoms. Coping with stress correlated significantly with the number of COVID-19 symptoms, but not with the severity score. Finally, reduced quality of life was associated with poorer immune fitness and reporting greater COVID-19 symptom severity.
3.1. Sex
The data for men (N = 503, 35.5%) and women (N = 912, 64.5%) are summarized in
Table A1. Significant sex differences were observed, both before COVID-19 and during lockdown. Women reported poorer mood than men, both before COVID-19 and during lockdown. Immune fitness was poorer in women, and women reported more COVID-19 symptoms than men. However, the COVID-19 severity scores were significantly lower among women. Women reported poorer coping with stress and poorer sleep than men. On the other hand, women experienced greater support from family and friends than men. During lockdown, women were significantly less optimistic than men, reported poorer sleep, and had a significantly poorer ability to cope with stress.
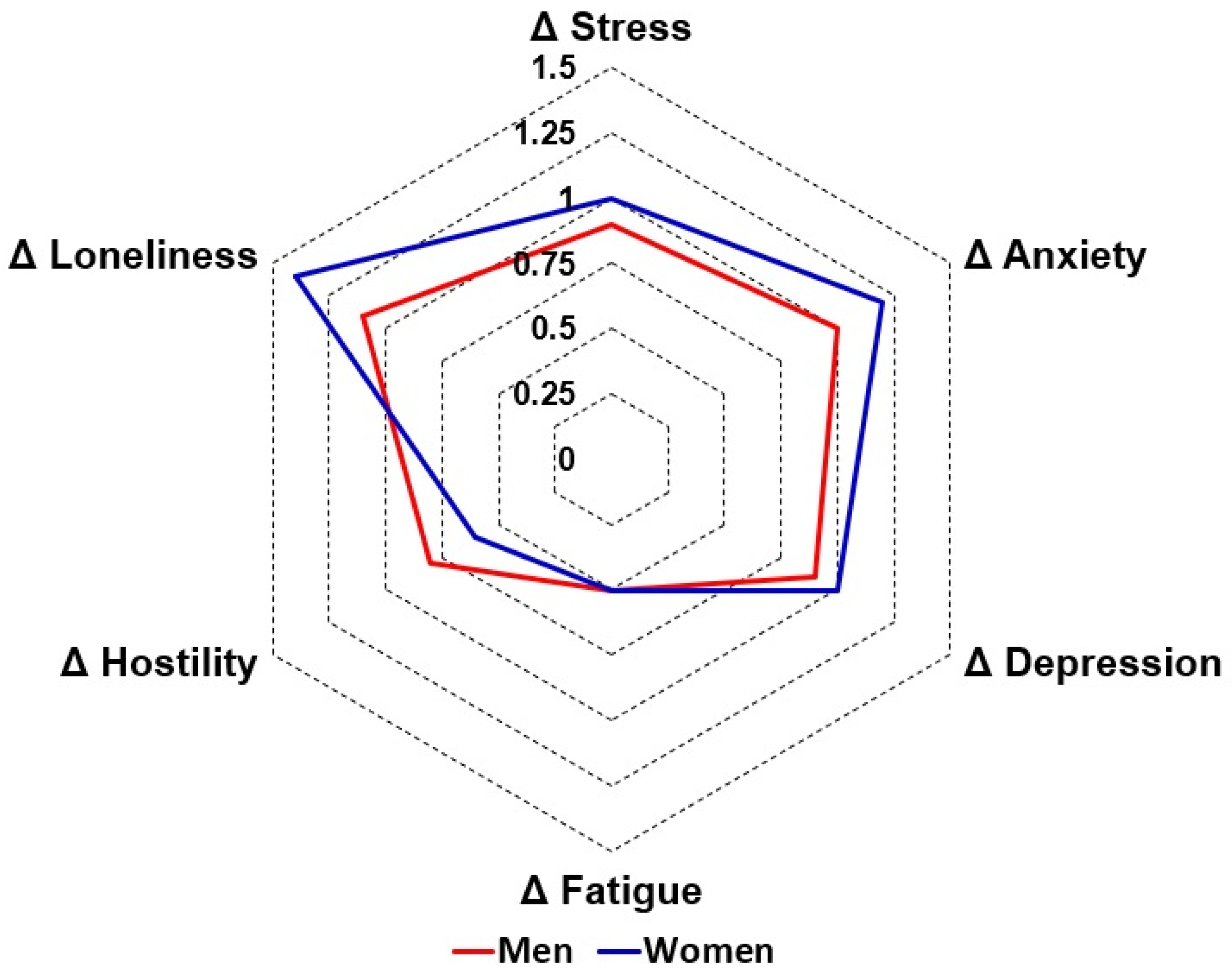
Data on the difference scores (during lockdown—before COVID-19) are visualized in
Figure 1. The analysis revealed that the lockdown did not differentially affect men and women with regard to mood, health correlates, and most lifestyle factors. Significant sex differences were found only for nutrition and support of family and friends (i.e., a healthier diet and more support in women), but the magnitude of these differences was small.
3.2. Age
To evaluate possible age effects, participants were allocated to one of the following age groups: ‘young adults’ (18–35 years old, N = 678, 35.5%), ‘adults’ (36–65 years old, N = 901, 47.2%), or ‘elderly’ (>65 years old, N = 331, 17.3%). The data for the age groups are summarized in
Table A2 and
Table A3. Compared to before COVID-19, all age groups reported poorer mood, lifestyle, and quality of life during lockdown. Age differences in these measures were already present before COVID-19. That is, mood was poorest among young adults and best among the elderly (See
Table A2). The ability to cope with stress increases with increasing age, while physical activity and being active decreases with increasing age.
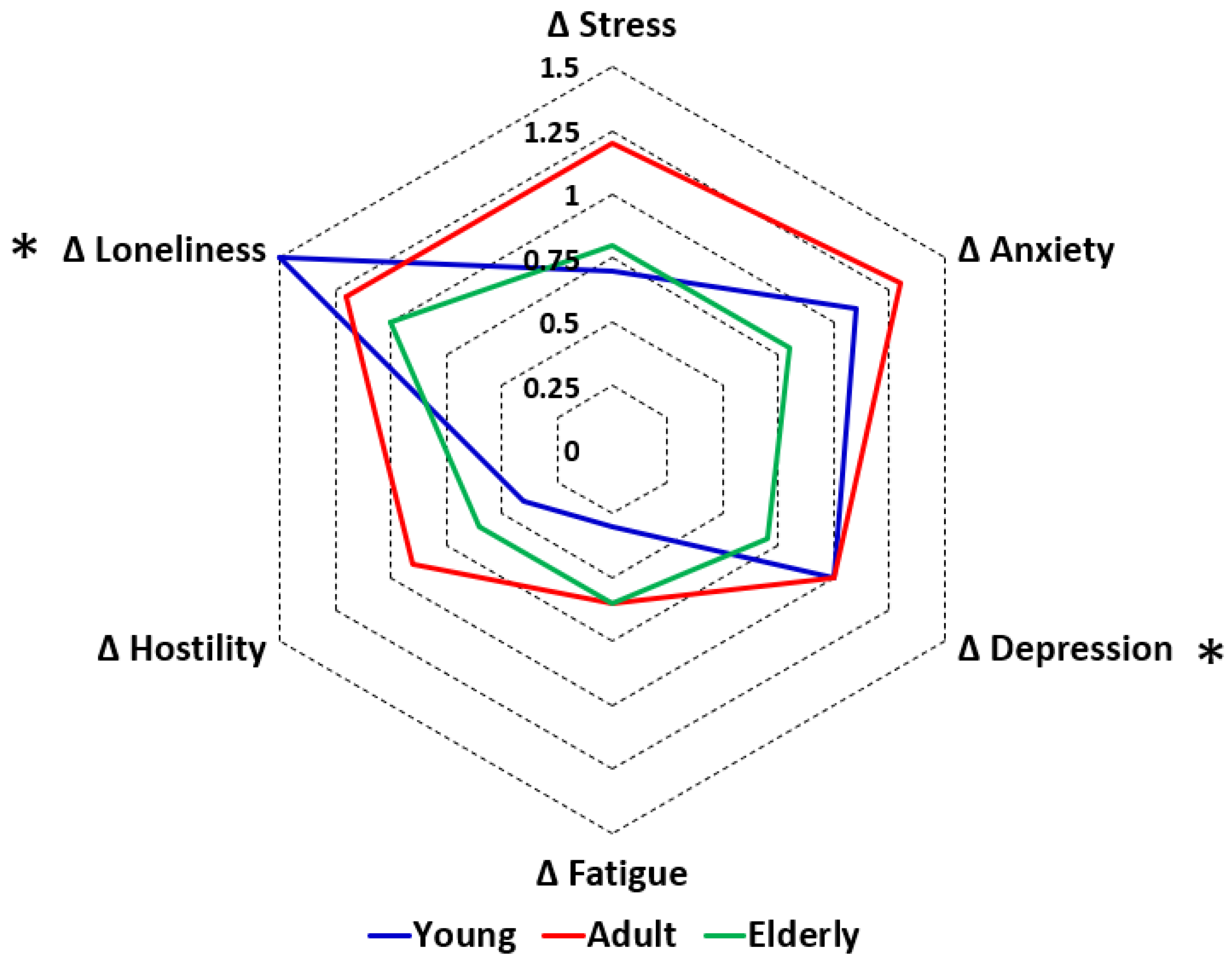
With regard to the lockdown effect, the difference scores (during lockdown—before COVID-19) were compared between the age groups. The lockdown effects on mood are summarized in
Figure 2. Compared to the older age groups, for young adults the lockdown had a significantly greater negative impact on depression and loneliness, and was associated with a significant decrease in being active and physical activity. Compared to the elderly, young adults reported a significantly greater reduction in quality of life during the lockdown. No age differences were found for the assessed health correlates.
3.3. Underlying Disease
Of the sample, N = 484 (34.5%) reported no underlying diseases. N = 920 (65.5%) reported having one or more underlying diseases (See
Table 4).
Of the participants who reported underlying diseases, more than half reported having one underlying disease (N = 518, 56.3%), and the other participants reported a combination of two or more underlying diseases. The most frequently reported combinations were allergy and lung diseases (N = 26), diabetes and cardiovascular diseases (N = 21), sleep disorders and allergy (N = 16), allergy and cardiovascular diseases (N = 14), and lung diseases and cardiovascular diseases (N = 13).
The impact of underlying disease status is summarized in
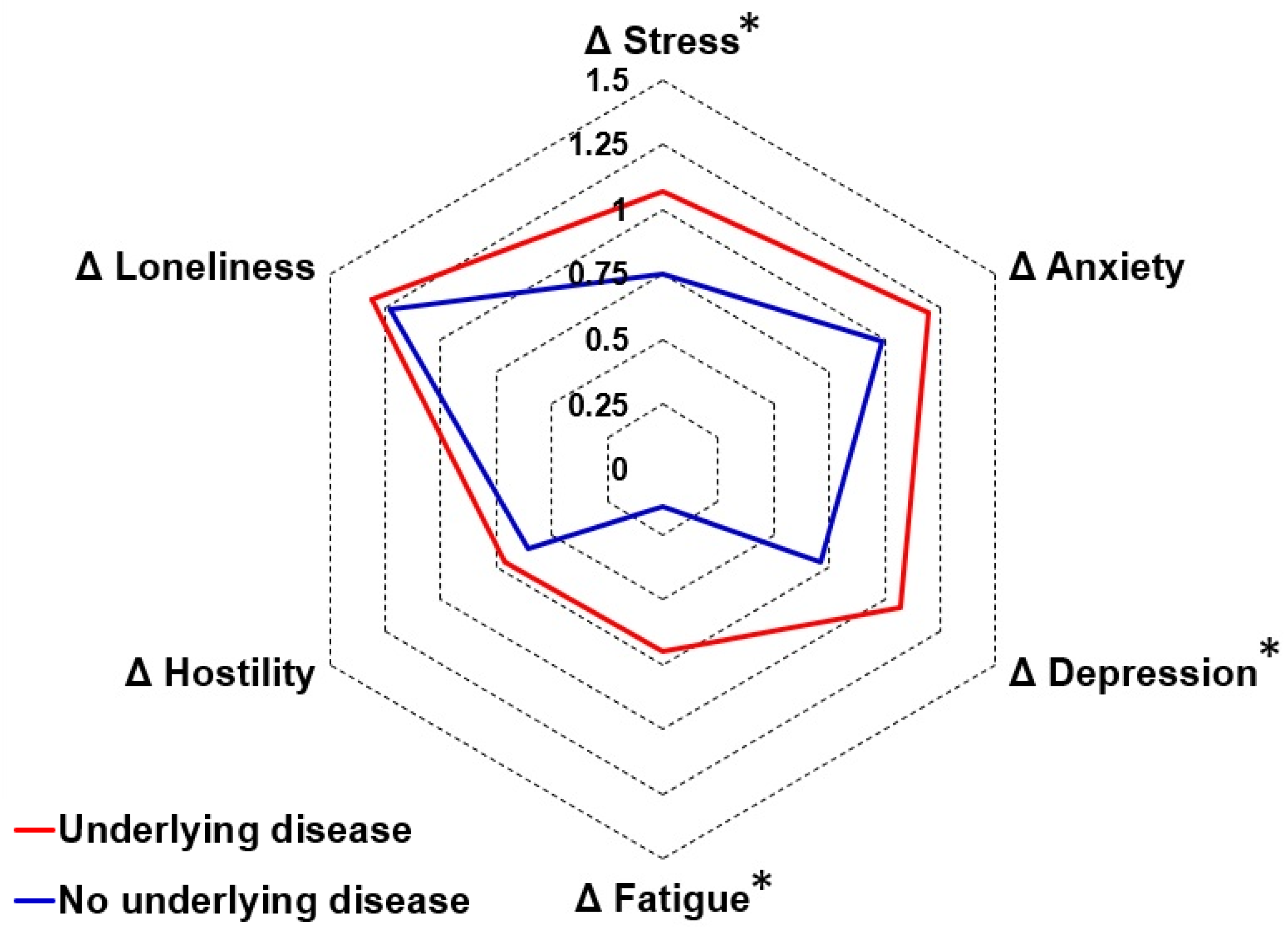
Table A4. Both before COVID-19 and during the lockdown, participants with underlying diseases reported significantly poorer mood, lifestyle, and health correlates compared to participants without underlying diseases. When directly comparing the difference scores (during lockdown—before COVID-19) of the group with and without underlying diseases, the analysis revealed no significant differences in lifestyle or health correlates. For mood, significantly greater negative changes were found for depression, stress, and fatigue among participants with underlying diseases (see
Figure 3).
4. Discussion
The first COVID-19 lockdown in the Netherlands was associated with significant negative effects on mood and lifestyle, reduced quality of life, and poorer immune fitness. These effects were accompanied by a significant increase in the number and severity of reported COVID-19 symptoms. Lifestyle factors, such as support of family and friends, coping with stress, adequate sleep, and attaining a healthy diet, reduced the negative lockdown effects on mood, immune fitness, and quality of life. However, the impact of lifestyle factors varied greatly between individuals.
Factors that differentially influenced the lockdown effects on mood included age and having underlying diseases, whereas no differential lockdown effects according to sex were observed. With regard to age, the lockdown had a significantly greater negative impact on ratings of depression and loneliness among younger individuals. This highlights the vulnerability of younger individuals in the face of prolonged social restrictions and limited opportunities for social interaction. For individuals with underlying diseases, the lockdown effects on depression, fatigue, and stress were significantly more pronounced compared to individuals without underlying diseases. This suggests that individuals with pre-existing health conditions may face additional challenges adapting to the lockdown measures and managing their psychological well-being.
Differential effects for lifestyle factors were found for sex and age. Women reported a significantly greater increase in support of family and friends than men. Whereas men reported significantly poorer nutrition during lockdown, the positive difference score in women suggested a small improvement in nutrition. These findings emphasize the importance of considering sex-specific needs and challenges when implementing public health measures. With regard to age, younger individuals reported a significantly greater impact of the lockdown on being active and physical activity compared to older individuals. The magnitude of changes in lifestyle factors did not significantly differ between participants with and without underlying diseases.
In a previous article, we reported that immune fitness before the COVID-19 pandemic was the strongest predictor of the presence and severity of COVID-19 symptoms during the first lockdown in the Netherlands [
37]. The results reported here show that this relationship was not differentially impacted by sex, age, or having underlying diseases. This observation is in line with the regression analyses presented by Kiani et al. [
37], which yielded models that did not include these variables as significant predictors of the number or severity of COVID-19 symptoms. Studies from the Netherlands and Germany conducted among young adults also reported poorer immune fitness during lockdown periods, which significantly correlated with negative mood changes and reduced quality of life [
47,
48]. The current study confirmed these findings for the general Dutch population.
A strength of the study is its adequate sample size to allow the planned comparisons according to age, sex, and underlying disease status. Although, as expected, the elderly were underrepresented, the sample size was adequate for age group comparisons and had a considerable age range. There was a good diversity of underlying diseases among the sample. However, the sample was a convenience sample, which may impact generalizability. A limitation of the study included the fact that all data were collected retrospectively and were self-reported. Given the latter, recall bias may have influenced the study outcomes. The survey was conducted after the first COVID-19 lockdown in the Netherlands. At that time, knowledge on COVID-19 was limited, and there were no standardized questionnaires available to assess COVID-19 severity. The scale used in the current study was developed in the first quarter of 2020 and included symptoms that at that time were known for the alpha variant of SARS-CoV-2, as listed by the National Institute for Public Health and the Environment. The scale mostly comprised respiratory symptoms. However, it should be noted that COVID-19 is not limited to respiratory symptoms: as many other organ systems may be affected, extra-pulmonary symptoms (e.g., loss of smell and taste) may also be experienced [
49]. Although it was asked whether participants were tested for infection with SARS-CoV-2, at the beginning of the COVID-19 pandemic, self-tests for COVID-19 were not available. Therefore, the actual COVID-19 status of the majority of the participants of the current study was not confirmed. The study consisted of a primary survey (Part 1) and a second survey (Part 2). After completion of Part 1, participants were invited to also complete Part 2. As expected from previous research [
50], the sample that participated in Part 2 was much smaller than the number of participants that completed Part 1. Nevertheless, the sample size of Part 2 was appropriate to conduct the presented analyses with sufficient statistical power.

 ,
, 

{kind=link}
{kind=link}
{kind=link}


