1. Introduction
Attention-deficit Hyperactivity Disorder is one of the most common childhood mental health disorders, affecting about 5.6% of the population worldwide, without respect to socioeconomic factors [
1]. It is characterized by significant motor hyperactivity and inattentiveness that can affect social functioning and cause impairment in other settings [
2]. Symptoms result from dysfunction in the frontal cortex and basal ganglia, with treatment to regulate neurotransmission in these areas [
3]. This disorder is usually clinically diagnosed through current and prior symptoms and impairment [
1,
4]. It is now established that symptoms can persist into adulthood in up to 65% of those diagnosed [
3]. Children diagnosed with attention-deficit hyperactivity disorder (ADHD) are more likely to experience additional mental health issues in adulthood [
2]. These disorders include mood disorders, such as bipolar disorder (BD), and personality and anxiety disorders. The prevalence of adults seeking treatment for at least one additional disorder following an ADHD diagnosis can vary from 57 to 97% [
2].
Several studies have specifically shown a high prevalence of comorbid mood disorders, such as depression and BD, in those diagnosed with ADHD [
1,
2]. In a survey conducted in the US, the National Comorbidity Survey-Replication found the prevalence of comorbid BD in patients diagnosed with ADHD to be 21.2% [
2]. Several common symptoms of ADHD are also found in BD, which are characterized by alternating periods of euthymia and mood disturbances. The inattention and impulsivity of ADHD can be seen in BD’s manic and hypomanic episodes [
2]. Patients with BD can also present from resulting cognitive dysfunction during the premorbid phase into the early course of the disease. Cognitive dysfunction usually results in impairments in learning, memory, and executive function. Comorbid ADHD and treatment with stimulants have been associated with an earlier onset of BD in those with past exposure to stimulants [
2]. These comorbid conditions can also complicate the progression and treatment of BD [
5].
ADHD and BD are both highly heritable and impairing conditions that have been shown to have several similarities and similar links [
4,
5]. The effectiveness of pharmacologic treatment strategies has been proven to be very effective. However, the long-term effectiveness and consequences of the medications are not yet well understood [
1,
4]. One of the major areas of future research on ADHD will be to study the long-term effects, both positive and negative, of the treatment of this disorder [
3]. Moreover, the relationship between ADHD and BD and the progression of each condition has been an area of study. There have been longitudinal studies to assess the development of hypomanic episodes in children with ADHD [
2,
5]. The aim of this manuscript is to discusses the relationship and clinical connections between the two disorders, including the medication induced mania hypothesis, clinical overlap, and genetic disposition in a narrative review format. It also explores effects of treatment on progression of both ADHD and BD.
2. Attention Deficit Hyperactivity Disorder Overview
ADHD exhibits a complex etiology integrating genetic and environmental factors for studied cases [
6,
7,
8,
9]. Further updates in the research literature have advanced our understanding of the disorder [
10]. Existing family and twin studies support genetics as an important factor in the onset of ADHD [
11]. Specifically, twin studies have concluded that the heritability of ADHD is estimated to be 60–90% [
11,
12,
13,
14]. However, when evaluated based on isolated genes and risk variants, ADHD demonstrates a poor correlation to any specific gene [
15,
16].
ADHD typically has had an onset at a young age. In 2013, the DSM V updated the age limit for the onset of qualifying symptoms for ADHD from age 6 to age 12 to prevent the misdiagnosis of normal inattention symptoms in the pediatric population [
17]. For diagnosis, adolescents (17 years or older) can display less hyperactive or inattentive symptoms (at least five). Increasingly, it has become accepted that ADHD can exhibit a late manifestation or maintain symptoms throughout adulthood [
18,
19,
20,
21]. As a baseline for diagnosis, ADHD must also be present in at least two settings where symptoms present in various environments like the home and school.
2.1. Pathophysiology
ADHD presents a variety of cognitive and functional deficits which originate from abnormalities in the brain [
22]. The two most common theories surrounding the mechanisms of ADHD involve a top-down and bottom-up model. Top-down models emphasize cognitive control and executive functioning. Specifically, abnormal executive function manifesting as impaired response inhibition has been used to explain the cognitive symptoms of ADHD [
23,
24,
25,
26]. In contrast, bottom-up models emphasize motivational, incentive, or reward responses.
The use of brain imaging has helped researchers elucidate the mechanisms behind ADHD [
27,
28]. Specifically, structural imaging studies using MRI have determined abnormal symptoms arising from a smaller size of the cerebrum, cerebellum, anterior cingulate cortex, and dorsolateral prefrontal cortex. Imaging studies also support theories about brain developmental patterns, as studies evaluating cortical thickness reported a delay in growth among ADHD patients [
29,
30]. An imaging study using MRI found widespread changes in the maturation of white matter fiber bundles and gray matter density in the brain which lead to structural shape changes in the middle and superior temporal gyrus, and fronto-basal portions of both frontal lobes [
31]. On the circuitry level, dysfunctions in the super longitudinal fasciculus and cortico-limbic areas are found in those with ADHD [
31]. These morphological findings predicted an ADHD diagnosis correctly in up to 83% of the cases in this imaging study [
31]. Furthermore, imaging for ADHD has also supported top-down and bottom-up theories by visualizing the structural environment of the brain [
32].
2.2. Epidemiology
Previous studies have estimated that ADHD affects approximately 2–7% of the global population [
33,
34,
35,
36]. Subsequently, the prevalence of ADHD in adults (between 19 and 45 years) has been estimated at 2.5% [
37] where 40–60% exhibit partial remission of symptoms [
38]. The most comprehensive meta-analysis, which was conducted by Polanczyk and colleagues, estimated a prevalence of 5.29% based upon 153 evaluated studies [
34]. Variability in prevalence values reflected differences in diagnostic criteria, information sources, and functional impairment requirements [
33,
38,
39]. Additionally, point prevalence did not change from 1985 to 2012 or between geographical regions across the globe [
34,
39].
3. Treatment
Pharmacologic treatments for ADHD can be divided into non-stimulants and stimulants. Stimulants, including amphetamine and methylphenidate-based medications, are considered first-line in treating ADHD in children and adults [
40]. These stimulants boost arousal in the prefrontal cortex by increasing norepinephrine and dopamine concentrations in the brain [
41]. Increasing synaptic dopamine and catecholamine are main mechanisms of action of both methylphenidate and amphetamine. However, there are specific differences that affect how they alter concentrations [
40]. The stimulant methylphenidate exerts its effects by inhibiting the dopamine transporters (DAT) and norepinephrine transporters (NET). It increases dopaminergic neurotransmission by inhibiting presynaptic DAT and, as a result, reuptake at the synapse [
40,
41].
Studies have demonstrated that methylphenidate directly interacts with adrenergic receptors to stimulate excitability in the cortex via activation of a2 adrenergic receptors [
40]. Methylphenidate also exerts agonistic activity at the 5-HT1a receptor [
40]. This results in the elevation of extracellular dopamine and norepinephrine levels, and as a result, increased binding to their respective receptors [
40].
Another stimulant used in treating ADHD is an amphetamine salt, whose primary mechanism of action is to increase catecholamine release [
40]. It acts as a competitive inhibitor of DAT and as a pseudo-substrate at norepinephrine binding sites. It acts to increase dopamine release by inhibiting the VMAT-2, or vesicular monoamine transporter 2, and it also inhibits monoamine oxidase activity to decrease the cytosolic breakdown monoamines [
41]. Both methylphenidate and amphetamine increase dopamine release, which increases responsiveness to external stimuli [
40,
41]. These stimulants have
d and
l isomers, with the
d isomer being more potent than its
l counterpart. Specifically, the
d isomer is more potent at the norepinephrine transporter and dopamine transporter binding sites b [
41].
Non-stimulant medication treatment includes atomoxetine and bupropion. Although the mechanism is not completely clear, atomoxetine is thought to selectivity inhibit norepinephrine uptake and preferentially binds to areas of known high distribution of noradrenergic neurons [
42]. Bupropion is an anti-depressant that has a variety of uses, including depression, anxiety, ADHD, and smoking cessation. Its mechanism of action likely involves the reuptake inhibition of the catecholamines, dopamine, and noradrenaline [
43]. This mechanism is like the one for psychostimulants, but bupropion is not a controlled substance. Clonidine is another choice, which is an alpha 2 adrenergic receptor agonist. Clonidine is good for impulsivity and hyperactivity but not useful for symptoms of inattention [
44]. Guanfacine is a direct alpha 2α subtype agonist within the central nervous system leading to reduced peripheral sympathetic outflow and strengthening of regulation of both attention and behavior within the prefrontal cortex through modulation at norepinephrine receptors [
44]. Its actions are found in the locus coeruleus and can result in improved attention [
44]. Clonidine and Guanfacine are considered second or third-line treatments after the use of stimulants has failed [
45].
4. Attention Deficit Hyperactivity Disorder and Bipolar Disorder
There is an overlap in terms of symptoms when looking at ADHD and BD. These two disorders often co-occur, and they are associated with worse outcomes [
46]. There is evidence that children with ADHD have a higher risk of being diagnosed with BD later in life [
47]. There have been attempts to develop neuropsychological testing that can better identify those with both disorders. However, research has shown that these tests have limited power to differentiate between BD adults with and without childhood ADHD [
46].
Symptoms of both ADHD and BD can have overlap which will be further explored in the next section. Mania is associated with bipolar disorder and is highlighted with increased energy and disorganized thinking with the inability to plan which can be seen in the increased goal-related activity. These are things that are also seen in ADHD. Other mood disorders such as depression and anxiety can have decreased concentration, which can also be seen in ADHD. So, at times, it can be hard to separate what diagnosis is correct because of the overlapping symptoms.
Treatment is a question that has been looked at in the research as the overlapping symptoms that cause issues and distress to the patient may be worsened by traditional ADHD treatment of stimulants. There is concern that the use of stimulants may worsen mania and psychosis and further debilitate the patient [
47]. A study performed by Galanter et al. suggests that youth treated with stimulants did not have an increase in mania or psychotic symptoms [
48]. Furthermore, children in the first month of treatment who had ADHD symptoms and manic symptoms had a more robust response to stimulant treatment. However, the studies in adults are less promising. In a review of three cases, the use of stimulants increased psychosis in patients [
49]. The authors concluded that patients need to be monitored for adverse responses to treatment. In the next section, the review will look at the clinical studies regarding the overlap of ADHD and BD.
Genome Wide Association Studies
There have been studies that have looked at genetic loci as conferring genetic risk for both bipolar disorder and ADHD. Demonitis et al. performed a genome-wide association study (GWAS) on 20,183 individuals with ADHD and 35,191 controls [
50]. The study found around 2932 genes that showed significant association with ADHD [
50]. They found that there was also a genetic correlation with both schizophrenia and bipolar disorder, however, this was not significant.
Another GWAS was performed by Mullins et al. looked at genes that could be associated with the increased risk of developing BD [
51]. They performed a GWAS of 41,917 BD cases and 371,549 controls of European ancestry. Their study found 64 associated genomic loci in their study population. These risk alleles were genes in the synaptic signaling pathways and brain-expressed genes, which had high specificity of expression in neurons of the prefrontal cortex and hippocampus [
51]. These are also areas that are implicated to be dysfunctional in ADHD; however, the authors made no connections to ADHD in their study so only references can be drawn.
5. Methods
Studies regarding the clinical overlap, medication-induced mania theory of BD, and co-occurrence of ADHD and BD were searched on PubMed only. Access to other scholarly search engines was not performed as access was lacking to them by the institution. Only articles written in English were included. Search terms of articles included ADHD and Bipolar Disorder, along with the terms overlap, co-occurrence, and genetics. Articles must have been published within the past 20 years for them to be included in this narrative review. There were no articles that were systematically excluded as this was a narrative review.
6. Clinical Studies
Over the past decade, there has been an increased interest in research between the correlation of ADHD and pediatric bipolar disorder (PBD) in children. Clinical trials have been performed and reviewed with multiple hypotheses in mind to attempt to determine if there is a valid association between the two, and if one of the disorders precedes in diagnosis. Some hypothesize that more children are comorbidly diagnosed with ADHD and PBD because of how many clinicians treat children with ADHD. Other factors that may affect the dual diagnoses of ADHD and PBD are overlapping diagnostic criteria for the two disorders, the inevitable biases seen when one disorder is diagnosed without the other, and related risk factors leading to prodromal relationships. By examining clinical trials, a better understanding as to whether ADHD and PBD have a stepwise progression or if other factors influence these comorbidities, such as blurred lines of diagnostic criteria. On the one hand, if the information gathered shows a relationship between these two diagnoses, it will be helpful because precautions can be enacted to prevent the progression from ADHD to BD or vice versa. On the other hand, if the comorbidity of the two disorders is occurring because of a bias or blurred diagnostic criteria, then a necessary change can be made to prevent unnecessary and inaccurate comorbid diagnoses in the pediatric population.
This diagnosis often is accompanied by alternative diagnoses as the child ages. According to a study conducted on a Medicaid population of 22,797 children diagnosed with ADHD in South Carolina, 40.1% were concurrently diagnosed with conduct disorder (CD)/oppositional defiant disorder (ODD), 15% were diagnosed with anxiety disorder, 5.7% were diagnosed with substance use disorder, and 7.8% were diagnosed with BD [
52]. Other studies have found the comorbid incidence of PBD and ADHD to fall in the range of 8% to 16.5% [
53,
54]. The varying percentages of comorbidity is a statistic that should be investigated because the prevalence is above the rates of chance alone. There are currently few explanations for the disparity, such as the size of the population being sampled, surveillance bias, and the cohorts in certain studies from specialized clinics, potentially leading to a form of Berkson’s bias. A more precise incidence of comorbid diagnoses would allow for a better understanding of the two disorders’ effects on one another in our pediatric population. A better understanding of the correlation between these two disorders is important because it could save lives since a diagnosis of PBD comes with an increase in morbidity and mortality.
6.1. False Correlation Hypotheses
Bias can creep its way into research in many different forms and often has the chance to skew scientists’ perspectives of various observations. One form of bias that could be presenting a false correlation between ADHD and PBD is surveillance bias. When children are labeled with a diagnosis of ADHD, they are placed in a category of children that are assessed with a bias by examining them for signs and symptoms of other diagnoses. Clinical trials have shown that those diagnosed with ADHD tend to be assigned additional diagnoses later in their life. One of the major comorbidities diagnosed included CD/ODD. With these diagnoses, one would expect to see these patients more often in a clinical setting due to the disruptions in the home and at school that often occur with these disorders. The behaviors of these categorized children can mimic symptoms of PBD, and the repeated visits to see a physician can lead to more of these children being diagnosed with PBD. This surveillance bias has the potential to skew the number of patients accurately diagnosed with PBD and can lead to greater symptom severity, greater functional impairment, and further comorbid diagnoses [
54].
6.2. Overlapping Criteria
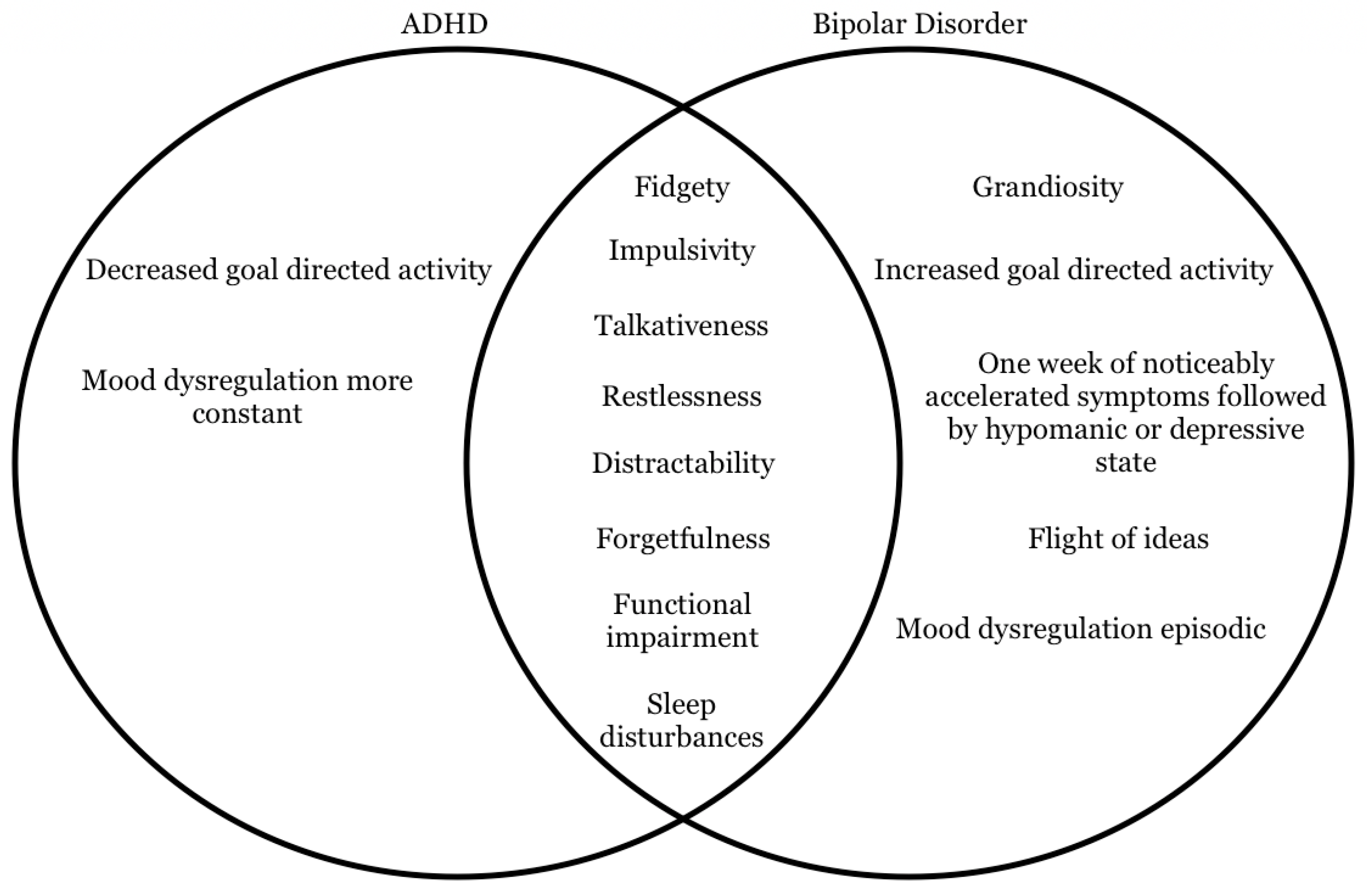
Besides bias playing a part in the misdiagnosis of PBD, the criteria required for a diagnosis of ADHD or PBD could be an issue of concern. The DSM-5 is continuously under revision, and recently there have been changes to certain aspects of diagnostic criteria for ADHD and BD. When studying these diagnostic criteria between these two disorders, we find there is considerable overlap. Patients with ADHD frequently have a vast amount of energy, causing impairment in their performance at school and in the home. With increased overall energy, children with ADHD can also commonly have psychomotor impairment, restlessness, forgetfulness, fidgeting, distractibility, and impulsivity. All of these symptoms in a child with ADHD tend to look very similar and may be mistaken as a manic episode [
55].
Figure 1 below shows a Venn diagram of the overlapping and unique symptoms seen in patients with ADHD and BD, respectively. Related to similar diagnostic criteria between these diagnoses, once ADHD is diagnosed in a child, they immediately meet multiple criteria required to be diagnosed with BD. The same can also be said for patients that are diagnosed with BD first. Suppose the DSM-5 were to be revised to differentiate the criteria of these two disorders a little further. In that case, it could decrease the burden of false diagnoses and morbidity/mortality that accompanies BD.
6.3. Correlation of Risk Factors
Before children are diagnosed with ADHD or BD, a thorough exam of the patient’s background must be completed. Aside from the symptoms required for diagnoses mentioned previously, other aspects of these patients’ lives that are important to consider are family history of mental health problems, a good understanding of home life, and past abuse or trauma. In both ADHD and BD patients, genetics is one of the most important risk factors in determining the probability of future diagnosis with either disorder mentioned. A study on a cohort of children that had no previous diagnosis of ADHD found a significant relationship between the likelihood of being diagnosed with ADHD and parental mental health problems [
56]. Another study analyzing probands diagnosed with BD discovered that the following generations’ odds ratio of being diagnosed with BD was equal to seven [
57]. These studies have found that certain genes are associated with ADHD and BD, but these studies did not separate the genetic aspect from being raised in the home by an adult dealing with a mental health problem.
Further research should be performed to eliminate potential confounding bias by separating the genetics aspect from the upbringing aspect since they are both major risk factors. For both ADHD and BD, community involvement, family climate, and self-efficacy are strong protective factors in preventing a mental health problem [
56]. Similar to how the diagnostic criteria of these two disorders are similar, so are the risk factors and protective factors. The blurred lines of diagnostic criteria can lead to more false-positive diagnoses of BD and ADHD. Still, the risk factors could be a possible explanation for these two disorders coinciding with one another.
6.4. Medication-Induced Mania Theory
When ADHD is diagnosed in the United States, there are a couple of options for treatment, as previously mentioned. With mainstay therapy in the US being stimulants, some speculate that the overuse of stimulants could induce manic symptoms in the pediatric population. When these patients are treated with an anti-depressant, without a thorough examination to rule out BD, treatment-induced mania or hypomania is possible. A study examining the frequency of PBD diagnoses in the United States compared to the Netherlands gives good insight into such a correlation. When comparing these two countries, there are stark differences in the number of patients given stimulants and anti-depressants as treatments for ADHD and depression, respectively [
58]. The research went on to show no significance of the stimulant treatment for ADHD and induction of BD but did, however, point out that one of the first signs of BD disorder in pediatric patients was depression. Therefore, the increase in PBD patients in the United States compared to the Netherlands could be attributed to anti-depressants.
A study conducted on a large cohort of pediatric patients from Taiwan examined the usage of methylphenidate and atomoxetine in those diagnosed with ADHD. Groups were separated into short-term treatment, long-term treatment, and no treatment and then followed up to see if any manic episodes or symptoms had developed. Their research showed that the odds of being diagnosed with BD while on long-term therapy of methylphenidates were decreased. The odds of being diagnosed with BD while on short-term methylphenidate treatment were not significant compared to the ADHD group that was not receiving treatment. When it came to atomoxetine, the odds of being diagnosed with BD for long-term and short-term treatment patients were not connected [
59]. One significant aspect discovered during this study was when compared to the control group of pediatric patients, those diagnosed with ADHD were seven times more likely to be diagnosed with BD at some point in their lives. This study shows some good data on the short-term effects of stimulants and the odds of being diagnosed with BD. When it comes to long-term odds of showing BD symptoms, it was capped at 12 years. This inevitably could cause researchers to miss some emergent cases of BD.
Another study performed examined BD patients that were taking methylphenidates with and without mood stabilizers. With the high percentage of BD patients also having comorbid ADHD, it is important to see if methylphenidates treating the ADHD symptoms also affects these patients’ BD eliciting more manic episodes. This study showed that the risk of developing mania while using methylphenidate as a monotherapy elevated the number of incidences, but it was not statistically significant. There was no increase in the risk of treatment-induced mania when the patients took methylphenidates while concomitantly taking a mood stabilizer [
60].
Stanford University School of Medicine conducted a study of anti-depressants usage in our pediatric population with depression and stimulants in pediatric ADHD patients. This research was performed with interest in these treatments and their chances of inducing mania. The research concluded, based on multiple sources, that stimulants did not increase treatment-induced mania and may even be protective against manic episodes. More manic episodes were seen when SSRIs were used as a monotherapy for BD with depression. SSRIs and mood stabilizers, when used together, work well to treat pediatric patients with BD with depressive symptoms. This study also showed that if stimulants become problematic during treatment or ineffective, atomoxetine can be used and is relatively safe [
60]. See
Table 1 below for a summary of studies mentioned on treatment-induced mania.
There is an increased incidence of depression, ADHD, BD, and other serious disorders across the board in our pediatric patient population. With the literature currently published in journals, there does not seem to be an association between ADHD and medication-induced BD. There are overlapping criteria between the two, and it would be advantageous to further differentiate the criteria of these two disorders. More research should be conducted on depression and its correlation with ADHD and PBD. It is known that patients with ADHD have an increased likelihood of having depressive symptoms. These patients have a high chance of being prescribed an SSRI in the United States to treat the depressive symptoms, but if these patients are not screened for BD, it could increase manic episodes and overall diagnoses of BD.
7. Limitations of the Manuscript
Limitations of this manuscript include the fact that this is a narrative review. The evidence is reported in a narrative format and the quality of the evidence was not weighed for inclusion or exclusion. The reason for this, with the information gathered being presented in this way, it that it enables the reader to draw conclusions for themselves. Another limitation is that none of the studies conducted above were performed by the authors.
8. Conclusions
ADHD is a common mental health disorder that is complex. Symptoms and variation among patients are most likely due to the variation of pathophysiology in the prefrontal cortex. There have been previous links of genetic and environmental factors associated with ADHD. Its progression in those diagnosed is often complicated by comorbid disorders, including substance use disorders, mood disorders, and personality disorders. Those with ADHD are also at an increased risk of impairment at work and in social settings. This manuscript attempts to explore both progression of this disease and its clinical connections to other disorders.
The clinical connections and links between ADHD and BD have recently been investigated and studied through clinical trials. There are currently hypotheses that center around the potential association between comorbid disorders in children. Those diagnosed with ADHD are at increased risk of comorbid mood disorders, such as BD. These disorders also share several symptoms that may make distinguishing the disorders difficult. According to some clinical trials, this link may be partly related to how we treat and manage these disorders. The management has classically involved both pharmacotherapy and psychosocial therapy, with stimulants being the first line of treatment. Specifically, the use and side effects of stimulants have been studied in those diagnosed with ADHD, along with the relationship between SSRI use in ADHD for managing depressive symptoms and the risk of subsequent mania.
In conclusion, there are currently several established links between ADHD and other conditions, such as BD. These links seem to be due, at least in part, to the side effects of the pharmacological treatment. Variation in dopaminergic receptors in the brain may contribute to the different effects of stimulants and is an area for future research in the field.
Author Contributions
Conceptualization, A.N.E.; writing—original draft, A.N.E., J.D.H., J.J.R. and T.L.A.; writing—review and editing, A.N.E., E.M.C., A.M.K. and A.D.K. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Data Availability Statement
The data in the manuscript can be found on the pubmed database of articles.
Conflicts of Interest
The authors have no conflict of interest to declare.
References
- Gavin, B.; McNicholas, F. ADHD: Science, stigma and service implications. Ir. J. Psychol. Med. 2018, 35, 169–172. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Salvi, V.; Ribuoli, E.; Servasi, M.; Orsolini, L.; Volpe, U. ADHD and Bipolar Disorder in Adulthood: Clinical and Treatment Implications. Medicina 2021, 57, 466. [Google Scholar] [CrossRef] [PubMed]
- Cortese, S.; Coghill, D. Twenty years of research on Attention-Deficit/Hyperactivity Disorder (ADHD): Looking back, looking forward. Evid.-Based Ment. Health 2018, 21, 173–176. [Google Scholar] [CrossRef] [PubMed]
- Posner, J.; Polanczyk, G.V.; Sonuga-Barke, E. Attention-deficit hyperactivity disorder. Lancet 2020, 395, 450–462. [Google Scholar] [CrossRef]
- Solé, B.; Jiménez, E.; Torrent, C.; Reinares, M.; Bonnin, C.D.; Torres, I.; Varo, C.; Grande, I.; Valls, E.; Salagre, E.; et al. Cognitive Impairment in Bipolar Disorder: Treatment and Prevention Strategies. Int. J. Neuropsychopharmacol. 2017, 20, 670–680. [Google Scholar] [CrossRef]
- Tistarelli, N.; Fagnani, C.; Troianiello, M.; Stazi, M.A.; Adriani, W. The nature and nurture of ADHD and its comorbidities: A narrative review on twin studies. Neurosci. Biobehav. Rev. 2020, 109, 63–77. [Google Scholar] [CrossRef]
- Craig, F.; Savino, R.; Fanizza, I.; Lucarelli, E.; Russo, L.; Trabacca, A. A systematic review of coping strategies in parents of children with attention deficit hyperactivity disorder (ADHD). Res. Dev. Disabil. 2020, 98, 103571. [Google Scholar] [CrossRef]
- Nilsen, F.M.; Tulve, N.S. A systematic review and meta-analysis examining the interrelationships between chemical and non-chemical stressors and inherent characteristics in children with ADHD. Environ. Res. 2020, 180, 108884. [Google Scholar] [CrossRef]
- Hamza, M.; Halayem, S.; Bourgou, S.; Daoud, M.; Charfi, F.; Belhadj, A. Epigenetics and ADHD: Toward an Integrative Approach of the Disorder Pathogenesis. J Atten. Disord. 2019, 23, 655–664. [Google Scholar] [CrossRef] [PubMed]
- Matthews, M.; Nigg, J.T.; Fair, D.A. Attention deficit hyperactivity disorder. Curr. Behav. Neurosci. 2014, 16, 235–266. [Google Scholar]
- Tripp, G.; Wickens, J.R. Neurobiology of ADHD. Neuropharmacology 2009, 57, 579–589. [Google Scholar] [CrossRef] [PubMed]
- Burt, S.A. Rethinking environmental contributions to child and adolescent psychopathology: A meta-analysis of shared environmental influences. Psychol. Bull. 2009, 135, 608–637. [Google Scholar] [CrossRef] [PubMed]
- Faraone, S.V.; Biederman, J. What is the prevalence of adult ADHD? Results of a population screen of 966 adults. J. Atten. Disord. 2005, 9, 384–391. [Google Scholar] [CrossRef] [PubMed]
- Seidman, L.J.; Valera, E.M.; Makris, N.; Monuteaux, M.C.; Boriel, D.L.; Kelkar, K.; Kennedy, D.N.; Caviness, V.S.; Bush, G.; Aleardi, M.; et al. Dorsolateral prefrontal and anterior cingulate cortex volumetric abnormalities in adults with attention-deficit/hyperactivity disorder identified by magnetic resonance imaging. Biol. Psychiatry 2006, 60, 1071–1080. [Google Scholar] [CrossRef]
- Faraone, S.V.; Larsson, H. Genetics of attention deficit hyperactivity disorder. Mol. Psychiatry 2019, 24, 562–575. [Google Scholar] [CrossRef] [Green Version]
- Grimm, O.; Kranz, T.M.; Reif, A. Genetics of ADHD: What Should the Clinician Know? Curr. Psychiatry Rep. 2020, 22, 18. [Google Scholar] [CrossRef] [Green Version]
- American Psychiatric Association. American Psychiatric Association: Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Publishing: Arlington, TX, USA, 2013; 89p. [Google Scholar]
- Zalsman, G.; Shilton, T. Adult ADHD: A new disease? Int. J. Psychiatry Clin. Pract. 2016, 20, 70–76. [Google Scholar] [CrossRef]
- Lazzaro, I.; Gordon, E.; Whitmont, S.; Plahn, M.; Li, W.; Clarke, S.; Dosen, A.; Meares, R. Quantified EEG activity in adolescent attention deficit hyperactivity disorder. Clin. Electroencephalogr. 1998, 29, 37–42. [Google Scholar] [CrossRef]
- Anbarasan, D.; Kitchin, M.; Adler, L.A. Screening for Adult ADHD. Curr. Psychiatry Rep. 2020, 22, 72. [Google Scholar] [CrossRef]
- Young, J.L.; Goodman, D.W. Adult Attention-Deficit/Hyperactivity Disorder Diagnosis, Management, and Treatment in the DSM-5 Era. Prim. Care Companion CNS Disord. 2016, 6, 18. [Google Scholar] [CrossRef] [Green Version]
- Magnus, W.; Nazir, S.; Anilkumar, A.C.; Shaban, K. Attention Deficit Hyperactivity Disorder. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2021; Volume 121, pp. 65–94. [Google Scholar]
- Barkley, R.A. Behavioral inhibition, sustained attention, and executive functions: Constructing a unifying theory of ADHD. Psychol. Bull. 1997, 121, 65–94. [Google Scholar] [CrossRef] [Green Version]
- Nigg, J.T. The ADHD response-inhibition deficit as measured by the stop task: Replication with DSM-IV combined type, extension, and qualification. J. Abnorm. Child Psychol. 1999, 27, 393–402. [Google Scholar] [CrossRef] [PubMed]
- Nigg, J.T. Is ADHD a disinhibitory disorder? Psychol. Bull. 2001, 127, 571–598. [Google Scholar] [CrossRef] [PubMed]
- Toward defining a neuropsychology of attention deficit-hyperactivity disorder: Performance of children and adolescents from a large clinically referred sample. Postgrad. Med. 2010, 122, 97–109.
- Wilens, T.E.; Spencer, T.J. Understanding Attention-Deficit/Hyperactivity Disorder from Childhood to Adulthood. Postgrad Med. 2010, 122, 97–109. [Google Scholar] [CrossRef]
- Klein, M.; Onnink, M.; van Donkelaar, M.; Wolfers, T.; Harich, B.; Shi, Y.; Dammers, J.; Arias-Vásquez, A.; Hoogman, M.; Franke, B. Brain imaging genetics in ADHD and beyond—Mapping pathways from gene to disorder at different levels of complexity. Neurosci. Biobehav. Rev. 2017, 80, 115–155. [Google Scholar] [CrossRef]
- Shaw, P.; Eckstrand, K.; Sharp, W.; Blumenthal, J.; Lerch, J.P.; Greenstein, D.E.; Clasen, L.; Evans, A.; Giedd, J.; Rapoport, J.L. Attention-deficit/hyperactivity disorder is characterized by a delay in cortical maturation. Proc. Natl. Acad. Sci. USA 2007, 104, 19649–19654. [Google Scholar] [CrossRef] [Green Version]
- Makris, N.; Biederman, J.; Valera, E.M.; Bush, G.; Kaiser, J.; Kennedy, D.N.; Caviness, V.S.; Faraone, S.V.; Seidman, L.J. Cortical thinning of the attention and executive function networks in adults with attention-deficit/hyperactivity disorder. Cereb. Cortex 2007, 17, 1364–1375. [Google Scholar] [CrossRef] [Green Version]
- Gehricke, J.G.; Kruggel, F.; Thampipop, T.; Alejo, S.D.; Tatos, E.; Fallon, J.; Muftuler, L.T. The brain anatomy of attention-deficit/hyperactivity disorder in young adults—A magnetic resonance imaging study. PLoS ONE 2017, 12, e0175433. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Casey, B.J.; Durston, S. From behavior to cognition to the brain and back: What have we learned from functional imaging studies of attention deficit hyperactivity disorder? Am. J. Psychiatry 2006, 163, 957–960. [Google Scholar] [CrossRef] [PubMed]
- Sayal, K.; Prasad, V.; Daley, D.; Ford, T.; Coghill, D. ADHD in children and young people: Prevalence, care pathways, and service provision. Lancet Psychiatry 2018, 5, 175–186. [Google Scholar] [CrossRef]
- Polanczyk, G.; de Lima, M.S.; Horta, B.L.; Biederman, J.; Rohde, L.A. The worldwide prevalence of ADHD: A systematic review and metaregression analysis. Am. J. Psychiatry 2007, 164, 942–948. [Google Scholar] [CrossRef] [PubMed]
- Erskine, H.E.; Ferrari, A.J.; Nelson, P.; Polanczyk, G.V.; Flaxman, A.D.; Vos, T.; Whiteford, H.A.; Scott, J.G. Research Review: Epidemiological modelling of attention-deficit/hyperactivity disorder and conduct disorder for the Global Burden of Disease Study 2010. J. Child Psychol. Psychiatry 2013, 54, 1263–1274. [Google Scholar] [CrossRef] [PubMed]
- Willcutt, E.G. The prevalence of DSM-IV attention-deficit/hyperactivity disorder: A meta-analytic review. Neurotherapeutics 2012, 9, 490–499. [Google Scholar] [CrossRef] [Green Version]
- Simon, V.; Czobor, P.; Bálint, S.; Mészáros, A.; Bitter, I. Prevalence and correlates of adult attention-deficit hyperactivity disorder: Meta-analysis. Br. J. Psychiatry J. Ment. Sci. 2009, 194, 204–211. [Google Scholar] [CrossRef] [PubMed]
- Biederman, J.; Fried, R.; DiSalvo, M.; Woodworth, K.Y.; Biederman, I.; Driscoll, H.; Noyes, E.; Faraone, S.V.; Perlis, R.H. Further evidence of low adherence to stimulant treatment in adult ADHD: An electronic medical record study examining timely renewal of a stimulant prescription. Psychopharmacology 2020, 237, 2835–2843. [Google Scholar] [CrossRef]
- Polanczyk, G.V.; Salum, G.A.; Sugaya, L.S.; Caye, A.; Rohde, L.A. Annual research review: A meta-analysis of the worldwide prevalence of mental disorders in children and adolescents. J. Child Psychol. Psychiatry 2015, 56, 345–365. [Google Scholar] [CrossRef] [PubMed]
- Faraone, S.V. The Pharmacology of Amphetamine and Methylphenidate: Relevance to the Neurobiology of Attention-Deficit/Hyperactivity Disorder and Other Psychiatric Comorbidities. Neurosci. Biobehav. Rev. 2018, 87, 255–270. [Google Scholar] [CrossRef]
- Brown, K.A.; Samuel, S.; Patel, D.R. Pharmacologic management of attention deficit hyperactivity disorder in children and adolescents: A review for practitioners. Transl. Pediatr. 2018, 7, 36–47. [Google Scholar] [CrossRef] [Green Version]
- Garnock-Jones, K.P.; Keating, G.M. Atomoxetine: A review of its use in attention-deficit hyperactivity disorder in children and adolescents. Drugs 2009, 11, 203–226. [Google Scholar] [CrossRef]
- Verbeeck, W.; Bekkering, G.E.; Van den Noortgate, W.; Kramers, C. Bupropion for attention deficit hyperactivity disorder (ADHD) in adults. Cochrane Database Syst. Rev. 2017, 2017, CD009504. [Google Scholar] [CrossRef]
- Kolar, D.; Keller, A.; Golfinopoulos, M.; Cumyn, L.; Syer, C.; Hechtman, L. Treatment of adults with attention-deficit/hyperactivity disorder. Neuropsychiatr. Dis. Treat. 2008, 4, 389–403. [Google Scholar]
- ADHD Medications: Strattera, Antidepressants & More. Cleveland Clinic. Available online: https://my.clevelandclinic.org/health/drugs/12959-attention-deficit-hyperactivity-disorder-adhd-nonstimulant-therapy-strattera--other-adhd-drugs (accessed on 9 October 2021).
- Sparding, T.; Clements, C.; Rydén, E.; Landén, M. Neuropsychological profiles of adult bipolar disorder patients with and without comorbid attention-deficit hyperactivity disorder. Int. J. Bipolar Disord. 2019, 7, 14. [Google Scholar]
- Girard, R.; Joober, R. Treatment of ADHD in patients with bipolar disorder. J. Psychiatry Neurosci. 2017, 42, E11–E12. [Google Scholar] [CrossRef] [Green Version]
- Galanter, C.A.; Carlson, G.A.; Jensen, P.S.; Greenhill, L.L.; Davies, M.; Li, W.; Chuang, S.Z.; Elliott, G.R.; Arnold, L.E.; March, J.S. Response to methylphenidate in children with attention deficit hyperactivity disorder and manic symptoms in the multimodal treatment study of children with attention deficit hyperactivity disorder titration trial. J. Child Adolesc. Psychopharmacol. 2003, 13, 123–136. [Google Scholar] [CrossRef]
- Kraemer, M.; Uekermann, J.; Wiltfang, J.; Kis, B. Methylphenidate-induced psychosis in adult attention-deficit/hyperactivity disorder: Report of 3 new cases and review of the literature. Clin. Neuropharmacol. 2010, 33, 204–206. [Google Scholar] [CrossRef]
- Demontis, D.; Walters, R.K.; Martin, J.; Mattheisen, M.; Als, T.D.; Agerbo, E.; Baldursson, G.; Belliveau, R.; Bybjerg-Grauholm, J.; Bækvad-Hansen, M.; et al. Discovery of the first genome-wide significant risk loci for attention deficit/hyperactivity disorder. Nat. Genet. 2019, 51, 63–75. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mullins, N.; Forstner, A.J.; O’Connell, K.S.; Coombes, B.; Coleman, J.R.; Qiao, Z.; Als, T.D.; Bigdeli, T.B.; Børte, S.; Bryois, J.; et al. Genome-wide association study of over 40,000 bipolar disorder cases provides new insights into the underlying biology. Nat. Genet. 2021, 53, 817. [Google Scholar] [CrossRef] [PubMed]
- Jerrell, J.M.; McIntyre, R.S.; Park, Y.-M.M. Correlates of incident bipolar disorder in children and adolescents diagnosed with attention-deficit/hyperactivity disorder. J. Clin. Psychiatry 2014, 75, e1278–e1283. [Google Scholar] [CrossRef] [PubMed]
- Youngstrom, E.A.; Arnold, L.E.; Frazier, T.W. Bipolar and ADHD comorbidity: Both artifact and outgrowth of shared mechanisms. Clin. Psychol. Sci. Pract. 2010, 17, 350–359. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arnold, L.E.; Demeter, C.; Mount, K.; Frazier, T.W.; Youngstrom, E.A.; Fristad, M.; Birmaher, B.; Findling, R.L.; Horwitz, S.M.; Kowatch, R.; et al. Pediatric bipolar spectrum disorder and ADHD: Comparison and comorbidity in the LAMS clinical sample: ADHD and BPSD in LAMS children. Bipolar Disord. 2011, 13, 509–521. [Google Scholar] [CrossRef]
- DSM-5 Changes: Implications for Child Serious Emotional Disturbance. p. 73. Available online: https://www.samhsa.gov/data/sites/default/files/NSDUH-DSM5ImpactChildSED-2016.pdf (accessed on 20 August 2021).
- Risk and Protective Factors for the Development of ADHD Symptoms in Children and Adolescents: Results of the Longitudinal BELLA Study. Available online: https://journals.plos.org/plosone/article?id=10.1371/journal.pone.0214412 (accessed on 3 October 2021).
- Craddock, N.; Jones, I. Genetics of bipolar disorder. J. Med. Genet. 1999, 36, 585–594. [Google Scholar] [CrossRef] [PubMed]
- Reichart, C.G.; Nolen, W.A. Earlier onset of bipolar disorder in children by antidepressants or stimulants? An hypothesis. J. Affect. Disord. 2004, 78, 81–84. [Google Scholar] [CrossRef]
- Wang, L.J.; Shyu, Y.C.; Yuan, S.S.; Yang, C.J.; Yang, K.C.; Lee, T.L.; Lee, S.Y. Attention-deficit hyperactivity disorder, its pharmacotherapy, and the risk of developing bipolar disorder: A nationwide population-based study in Taiwan. J. Psychiatr. Res. 2016, 72, 6–14. [Google Scholar] [CrossRef] [PubMed]
- Viktorin, A.; Rydén, E.; Thase, M.E.; Chang, Z.; Lundholm, C.; D’Onofrio, B.M.; Almqvist, C.; Magnusson, P.K.; Lichtenstein, P.; Larsson, H.; et al. The Risk of Treatment-Emergent Mania with Methylphenidate in Bipolar Disorder. Am. J. Psychiatry 2017, 174, 341–348. [Google Scholar] [CrossRef] [PubMed]
| Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).


 ,
, 


{kind=link}