
Analysing the Impacts of Financial Expenditure of Prefectures on Methods of Suicide Completion in Japan


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Independent Variables
2.2. Dependent Variables
2.3. Statistical Analysis
3. Results
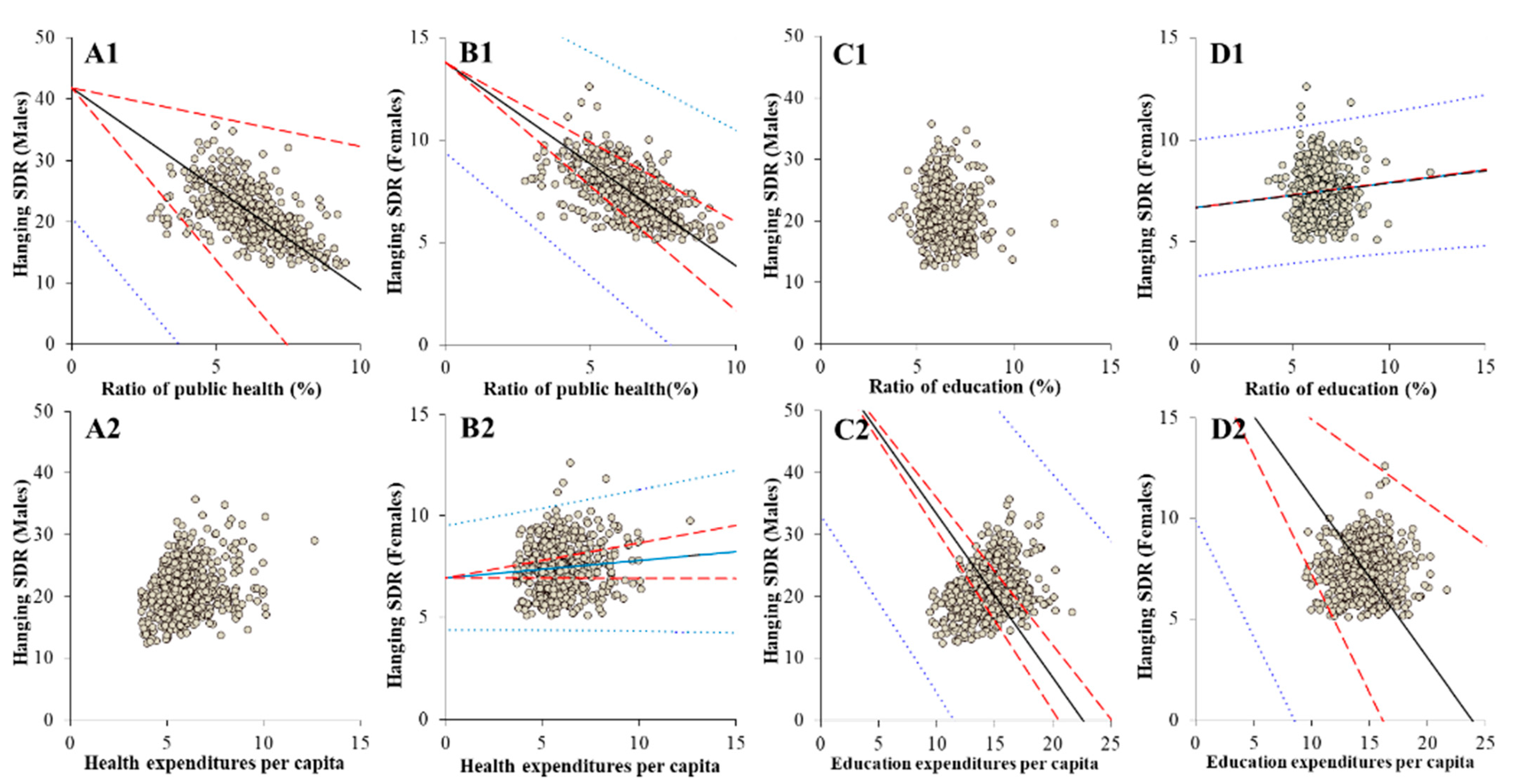
3.1. Effects of Ratio of the Expenditure of Six Divisions per Total Amount of the Regional Governmental Expenditure on Suicide Mortalities Disaggregated by Major Five Means (Model-1)
3.2. Effects of Regional Expenditure of Six Divisions per Capita on Suicide Mortalities Disaggregated by Major Five Means (Model-2)
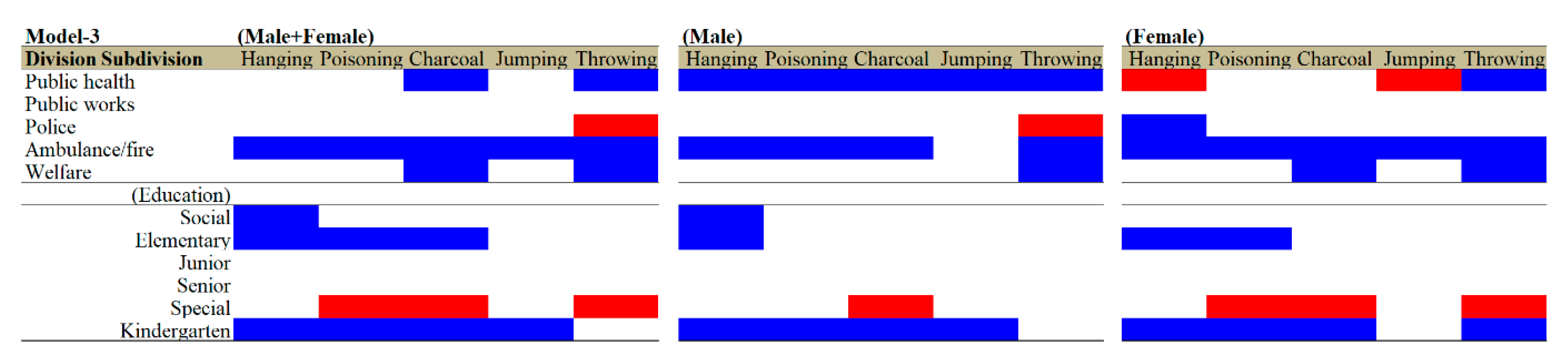
3.3. Effects of Expenditure per Capita of Divisions and Subdivision of Education on Suicide Mortalities by Five Major Means (Model-3)
3.4. Effects of Expenditure per Capita of Divisions and Subdivision of Education and Welfare on Suicide Mortalities by Five Major Means (Model-4)
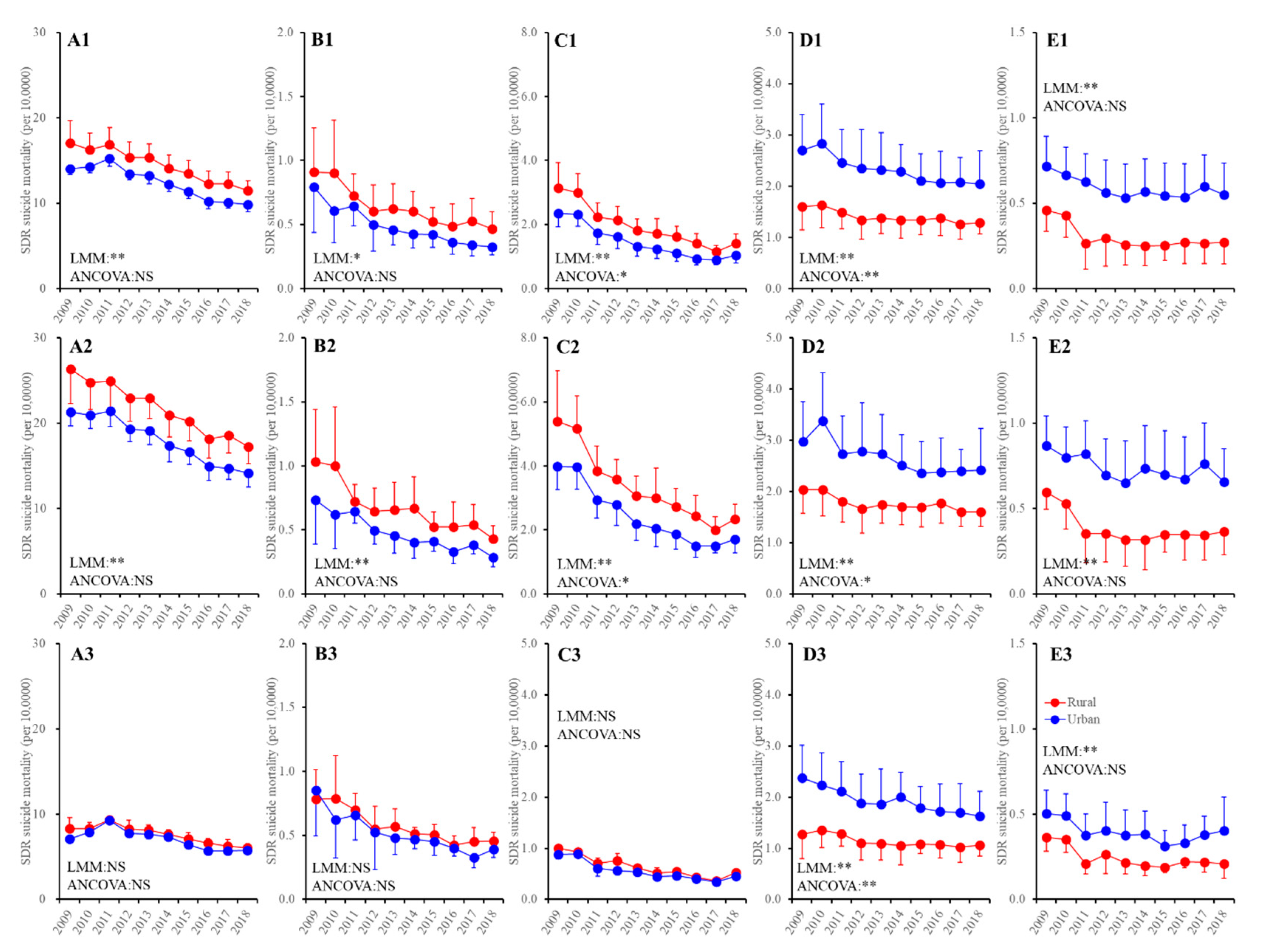
3.5. Trends of Suicide Mortalities Disaggregated by Regional, Gender and Means Factors during 2009–2018 in Japan
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Orsolini, L.; Latini, R.; Pompili, M.; Serafini, G.; Volpe, U.; Vellante, F.; Fornaro, M.; Valchera, A.; Tomasetti, C.; Fraticelli, S.; et al. Understanding the complex of suicide in depression: From research to clinics. Psychiatry Investig. 2020, 17, 207–221. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Berardis, D.; Olivieri, L.; Rapini, G.; Serroni, N.; Fornaro, M.; Valchera, A.; Carano, A.; Vellante, F.; Bustini, M.; Serafini, G.; et al. Religious coping, hopelessness, and suicide ideation in subjects with first-episode major depression: An exploratory study in the real world clinical practice. Brain Sci. 2020, 10, 912. [Google Scholar] [CrossRef]
- Ministry of Health, Labour and Welfare. Basic Data on Suicide in the Region. Available online: https://www.mhlw.go.jp/stf/seisakunitsuite/bunya/0000140901.html (accessed on 1 September 2021).
- Ministry of Health, Labour and Welfare. 2019 White Paper on Suicide Prevention. Available online: https://www.mhlw.go.jp/wp/hakusyo/jisatsu/19/index.html (accessed on 14 November 2020).
- Ministry of Health, Labour and Welfare. 2020 White Paper on Suicide Prevention. Available online: https://www.mhlw.go.jp/stf/seisakunitsuite/bunya/hukushi_kaigo/seikatsuhogo/jisatsu/jisatsuhakusyo2020.html (accessed on 1 June 2021).
- Ministry of Health, Labour and Welfare. Regional Suicide Countermeasures Emergency Enhancement Fund. Available online: https://www.mhlw.go.jp/stf/seisakunitsuite/bunya/hukushi_kaigo/seikatsuhogo/jisatsu/kyoukakikin.html (accessed on 18 November 2021).
- Ministry of Health, Labour and Welfare. Grant for Enhance Community-Based Suicide Countermeasures. Available online: https://www.mhlw.go.jp/stf/seisakunitsuite/bunya/hukushi_kaigo/seikatsuhogo/jisatsu/tiikijisatsutaisakukyokazigyo.html (accessed on 1 June 2021).
- Ministry of Health, Labour and Welfare. National Plan for Prevention of Suicide. Available online: https://www.mhlw.go.jp/kokoro/nation/about.html (accessed on 18 November 2021).
- Okada, M.; Hasegawa, T.; Kato, R.; Shiroyama, T. Analysing regional unemployment rates, GDP per capita and financial support for regional suicide prevention programme on suicide mortality in Japan using governmental statistical data. BMJ Open 2020, 10, e037537. [Google Scholar] [CrossRef]
- Kato, R.; Okada, M. Can financial support reduce suicide mortality rates? Int. J. Environ. Res. Public Health 2019, 16, 4797. [Google Scholar] [CrossRef] [Green Version]
- Shiroyama, T.; Fukuyama, K.; Okada, M. Effects of financial expenditure of prefectures/municipalities on regional suicide mortality in Japan. Int. J. Environ. Res. Public Health 2021, 18, 8639. [Google Scholar] [CrossRef]
- Nakano, T.; Hasegawa, T.; Okada, M. Analysing the impacts of financial support for regional suicide prevention programmes on suicide mortality caused by major suicide motives in Japan using statistical government data. Int. J. Environ. Res. Public Health 2021, 18, 3414. [Google Scholar] [CrossRef] [PubMed]
- Antonakakis, N.; Collins, A. The impact of fiscal austerity on suicide: On the empirics of a modern Greek tragedy. Soc. Sci. Med. 2014, 112, 39–50. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Antonakakis, N.; Collins, A. The impact of fiscal austerity on suicide mortality: Evidence across the ‘Eurozone periphery’. Soc. Sci. Med. 2015, 145, 63–78. [Google Scholar] [CrossRef] [Green Version]
- Branas, C.C.; Kastanaki, A.E.; Michalodimitrakis, M.; Tzougas, J.; Kranioti, E.F.; Theodorakis, P.N.; Carr, B.G.; Wiebe, D.J. The impact of economic austerity and prosperity events on suicide in Greece: A 30-year interrupted time-series analysis. BMJ Open 2015, 5, e005619. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karanikolos, M.; Mladovsky, P.; Cylus, J.; Thomson, S.; Basu, S.; Stuckler, D.; Mackenbach, J.P.; McKee, M. Financial crisis, austerity, and health in Europe. Lancet 2013, 381, 1323–1331. [Google Scholar] [CrossRef]
- Rachiotis, G.; Stuckler, D.; McKee, M.; Hadjichristodoulou, C. What has happened to suicides during the Greek economic crisis? Findings from an ecological study of suicides and their determinants (2003–2012). BMJ Open 2015, 5, e007295. [Google Scholar] [CrossRef] [Green Version]
- Simou, E.; Koutsogeorgou, E. Effects of the economic crisis on health and healthcare in Greece in the literature from 2009 to 2013: A systematic review. Health Policy 2014, 115, 111–119. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tapia Granados, J.A.; Rodriguez, J.M. Health, economic crisis, and austerity: A comparison of Greece, Finland and Iceland. Health Policy 2015, 119, 941–953. [Google Scholar] [CrossRef]
- Reeves, A.; Basu, S.; McKee, M.; Marmot, M.; Stuckler, D. Austere or not? UK coalition government budgets and health inequalities. J. R. Soc. Med. 2013, 106, 432–436. [Google Scholar] [CrossRef] [Green Version]
- Toffolutti, V.; Suhrcke, M. Does austerity really kill? Econ. Hum. Biol. 2019, 33, 211–223. [Google Scholar] [CrossRef] [PubMed]
- Barr, B.; Kinderman, P.; Whitehead, M. Trends in mental health inequalities in England during a period of recession, austerity and welfare reform 2004 to 2013. Soc. Sci Med. 2015, 147, 324–331. [Google Scholar] [CrossRef]
- Barr, B.; Taylor-Robinson, D.; Scott-Samuel, A.; McKee, M.; Stuckler, D. Suicides associated with the 2008-10 economic recession in England: Time trend analysis. BMJ 2012, 345, e5142. [Google Scholar] [CrossRef] [Green Version]
- Rambotti, S. Is there a relationship between welfare-state policies and suicide rates? Evidence from the US States, 2000–2015. Soc. Sci. Med. 2020, 246, 112778. [Google Scholar] [CrossRef] [Green Version]
- Hasegawa, T.; Matsumoto, R.; Yamamoto, Y.; Okada, M. Analysing effects of financial support for regional suicide prevention programmes on methods of suicide completion in Japan between 2009 and 2018 using governmental statistical data. BMJ Open 2021, 11, e049538. [Google Scholar] [PubMed]
- Cabinet Office. Outline of Measures for Society with Decreasing Birthrate. Available online: https://www8.cao.go.jp/shoushi/shoushika/law/taikou2.html (accessed on 1 June 2021).
- Swain, P.K.; Tripathy, M.R.; Priyadarshini, S.; Acharya, S.K. Forecasting suicide rates in India: An empirical exposition. PLoS ONE 2021, 16, e0255342. [Google Scholar] [CrossRef]
- You, B.S.; Jeong, K.H.; Cho, H.J. Regional suicide rate change patterns in Korea. Int. J. Environ. Res. Public Health 2020, 17, 6973. [Google Scholar] [CrossRef] [PubMed]
- Mattei, G.; Pistoresi, B. Unemployment and suicide in Italy: Evidence of a long-run association mitigated by public unemployment spending. Eur. J. Health Econ. 2019, 20, 569–577. [Google Scholar] [CrossRef]
- Mattei, G.; Pistoresi, B.; De Vogli, R. Impact of the economic crises on suicide in Italy: The moderating role of active labor market programs. Soc. Psychiatry Psychiatr. Epidemiol. 2019, 54, 201–208. [Google Scholar] [CrossRef] [PubMed]
- Robinson, R.J.; Palka, J.M.; Brown, E.S. The relationship between state mental health agency and medicaid spending with outcomes. Community Ment. Health J. 2021, 57, 307–314. [Google Scholar] [CrossRef]
- Matsumoto, R.M.E.; Fukuyama, K.; Shiroyama, T.; Okada, M. Determining what changed Japanese suicide mortality in 2020 Using Governmental Database. J. Clin. Med. 2021, 10, 5199. [Google Scholar] [CrossRef]
- Fushimi, M. The importance of studying the increase in suicides and gender differences during the COVID-19 pandemic. QJM 2021, hcab130. [Google Scholar] [CrossRef]
- Sakamoto, H.; Ishikane, M.; Ghaznavi, C.; Ueda, P. Assessment of suicide in Japan during the COVID-19 pandemic vs previous years. JAMA Netw. Open 2021, 4, e2037378. [Google Scholar] [CrossRef] [PubMed]
- Nomura, S.; Kawashima, T.; Harada, N.; Yoneoka, D.; Tanoue, Y.; Eguchi, A.; Gilmour, S.; Kawamura, Y.; Hashizume, M. Trends in suicide in Japan by gender during the COVID-19 pandemic, through December 2020. Psychiatry Res. 2021, 300, e113913. [Google Scholar] [CrossRef]
- Seposo, X.T. COVID-19 threatens decade-long suicide initiatives in Japan. Asian J. Psychiatry 2021, 60, 102660. [Google Scholar] [CrossRef]
- Eguchi, A.; Nomura, S.; Gilmour, S.; Harada, N.; Sakamoto, H.; Ueda, P.; Yoneoka, D.; Tanoue, Y.; Kawashima, T.; Hayashi, T.I.; et al. Suicide by gender and 10-year age groups during the COVID-19 pandemic vs previous five years in Japan: An analysis of national vital statistics. Psychiatry Res. 2021, 305, 114173. [Google Scholar] [CrossRef]
- Tanaka, T.; Okamoto, S. Increase in suicide following an initial decline during the COVID-19 pandemic in Japan. Nat. Hum. Behav. 2021, 5, 229–238. [Google Scholar] [CrossRef] [PubMed]
- Gunnell, D.; Bennewith, O.; Hawton, K.; Simkin, S.; Kapur, N. The epidemiology and prevention of suicide by hanging: A systematic review. Int. J. Epidemiol. 2005, 34, 433–442. [Google Scholar] [CrossRef] [PubMed]
- Chapman, S.; Alpers, P.; Agho, K.; Jones, M. Australia’s 1996 gun law reforms: Faster falls in firearm deaths, firearm suicides, and a decade without mass shootings. Inj. Prev. 2006, 12, 365–372. [Google Scholar] [CrossRef] [Green Version]
- Havarneanu, G.M.; Burkhardt, J.M.; Paran, F. A systematic review of the literature on safety measures to prevent railway suicides and trespassing accidents. Accid. Anal. Prev. 2015, 81, 30–50. [Google Scholar] [CrossRef]
- Chang, S.S.; Chen, Y.Y.; Yip, P.S.; Lee, W.J.; Hagihara, A.; Gunnell, D. Regional changes in charcoal-burning suicide rates in East/Southeast Asia from 1995 to 2011: A time trend analysis. PLoS Med. 2014, 11, e1001622. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miller, M.; Hemenway, D. Guns and suicide in the United States. N. Engl. J. Med. 2008, 359, 989–991. [Google Scholar] [CrossRef] [PubMed]
- Yamasawa, K.; Nishimukai, H.; Ohbora, Y.; Inoue, K. A statistical study of suicides through intoxication. Acta Med. Leg. Soc. (Liege) 1980, 30, 187–192. [Google Scholar]
- Yip, P.S.; Lee, D.T. Charcoal-burning suicides and strategies for prevention. Crisis 2007, 28 (Suppl. S1), 21–27. [Google Scholar] [CrossRef]
- Yoshioka, E.; Saijo, Y.; Kawachi, I. Spatial and temporal evolution of the epidemic of charcoal-burning suicide in Japan. Soc. Psychiatry Psychiatr. Epidemiol. 2016, 51, 857–868. [Google Scholar] [CrossRef]
- Yip, P.S.; Caine, E.; Yousuf, S.; Chang, S.S.; Wu, K.C.; Chen, Y.Y. Means restriction for suicide prevention. Lancet 2012, 379, 2393–2399. [Google Scholar] [CrossRef]
- Okolie, C.; Wood, S.; Hawton, K.; Kandalama, U.; Glendenning, A.C.; Dennis, M.; Price, S.F.; Lloyd, K.; John, A. Means restriction for the prevention of suicide by jumping. Cochrane Database Syst. Rev. 2020, 2, CD013543. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health, Labour and Welfare. Special Homepage of Life Support during Pandemic. Available online: https://www.mhlw.go.jp/stf/newpage_22325.html (accessed on 12 December 2021).
- Cabinet Office. Extraordinary Special Benefits for Child-Rearing Households. Available online: https://www5.cao.go.jp/keizai1/kosodatesetaikyufu/index.html (accessed on 12 December 2021).
- Statistics Bureau of Ministry of Internal Affairs and Communications. White Paper on Local Public Finance. Available online: https://www.soumu.go.jp/menu_seisaku/hakusyo/chihou/r03data/index.html (accessed on 1 May 2021).
- Statistics Bureau of Ministry of Internal Affairs and Communications. Survey on Local Public Finance. Available online: https://www.e-stat.go.jp/en/statistics/00200251 (accessed on 1 May 2021).
- Statistics Bureau of Ministry of Internal Affairs and Communications. Surveys of Population, Population Change and the Number of Households Based on the Basic Resident Registration. Available online: https://www.e-stat.go.jp/stat-search/files?page=1toukei=00200241tstat=000001039591 (accessed on 1 September 2021).
- Kawaguchi, H.; Koike, S. Association between the density of physicians and suicide rates in Japan: Nationwide ecological study using a spatial bayesian model. PLoS ONE 2016, 11, e0148288. [Google Scholar] [CrossRef] [PubMed]
- Nakamoto, M.; Nakagawa, T.; Murata, M.; Okada, M. Impacts of dual-income household rate on suicide mortalities in Japan. Int. J. Environ. Res. Public Health 2021, 18, 5670. [Google Scholar] [CrossRef]
- WHO. Preventing suicide: A Resource for Pesticide Registrars and Regulators. Available online: https://www.who.int/publications/i/item/9789241516389 (accessed on 18 November 2020).
- WHO. Preventing Suicide: A Global Imperative. Available online: https://www.who.int/publications/i/item/preventing-suicide-a-global-imperative (accessed on 18 November 2021).
- WHO. Preventing Suicide: A Resource for Filmmakers and Others Working on Stage and Screen. Available online: https://www.who.int/publications/i/item/preventing-suicide-a-resource-for-filmmakers-and-others-working-on-stage-and-screen (accessed on 18 November 2020).
- WHO. Suicide in the World. Available online: https://apps.who.int/iris/bitstream/handle/10665/326948/WHO-MSD-MER-19.3-eng.pdf (accessed on 18 November 2020).
- Okada, M.; Matsumoto, R.; Yamamoto, Y.; Fukuyama, K. Effects of subchronic administrations of vortioxetine, lurasidone, and escitalopram on thalamocortical glutamatergic transmission associated with serotonin 5-ht7 receptor. Int. J. Mol. Sci. 2021, 22, 1351. [Google Scholar] [CrossRef] [PubMed]
- Nakano, T.; Hasegawa, T.; Suzuki, D.; Motomura, E.; Okada, M. Amantadine combines astroglial system xc(-) activation with glutamate/nmda receptor inhibition. Biomolecules 2019, 9, 191. [Google Scholar] [CrossRef] [Green Version]
- Ajdacic-Gross, V.; Weiss, M.G.; Ring, M.; Hepp, U.; Bopp, M.; Gutzwiller, F.; Rossler, W. Methods of suicide: International suicide patterns derived from the who mortality database. Bull. World Health Organ. 2008, 86, 726–732. [Google Scholar] [CrossRef] [Green Version]
- WHO. Suicide: One Person Dies Every 40 Seconds. Available online: https://www.who.int/news/item/09-09-2019-suicide-one-person-dies-every-40-seconds (accessed on 18 November 2020).
- Wong, P.W.; Chan, W.S.; Lau, T.K.; Morgan, P.R.; Yip, P.S. Suicides by jumping from iconic bridges in Hong Kong. Crisis 2009, 30, 79–84. [Google Scholar] [CrossRef] [PubMed]
- Park, S.; Lee, H.B.; Lee, S.Y.; Lee, G.E.; Ahn, M.H.; Yi, K.K.; Hong, J.P. Trends in suicide methods and rates among older adults in South Korea: A comparison with Japan. Psychiatry Investig. 2016, 13, 184–189. [Google Scholar] [CrossRef] [Green Version]
- Yoshioka, E.; Hanley, S.J.; Kawanishi, Y.; Saijo, Y. Time trends in method-specific suicide rates in Japan, 1990–2011. Epidemiol. Psychiatr. Sci. 2016, 25, 58–68. [Google Scholar] [CrossRef] [PubMed]
- Choo, C.C.; Harris, K.M.; Ho, R.C. Prediction of lethality in suicide attempts: Gender matters. Omega J. Death Dying 2019, 80, 87–103. [Google Scholar] [CrossRef] [PubMed]
- Morovatdar, N.; Moradi-Lakeh, M.; Malakouti, S.K.; Nojomi, M. Most common methods of suicide in eastern mediterranean region of who: A systematic review and meta-analysis. Arch. Suicide Res. 2013, 17, 335–344. [Google Scholar] [CrossRef] [PubMed]
- Hedegaard, H.; Curtin, S.C.; Warner, M. Quickstats: Age-adjusted suicide rates* for females and males, by method(dagger)—national vital statistics system, United States, 2000 and 2014. Morb. Mortal. Wkly. Rep. (MMRW) 2016, 65, 503. [Google Scholar]
- Hasegawa, T.; Fukuyama, K.; Okada, M. Relationships between Expenditure of Regional Governments and Suicide Mortalities Caused by Six Major Motives in Japan. Int. J. Environ. Res. Public Health 2022, 19, 84. [Google Scholar]
- Statistics Bureau of the Ministry of Internal Affairs and Communications. Family Income and Expenditure Survey. Available online: https://www.e-stat.go.jp/en/stat-search/files?page=1layout=normaltoukei=00200561 (accessed on 1 May 2021).
- Cabinet Office. Annual Report on Government Measures for Persons with Disabilities (Summary) 2020. Available online: https://www8.cao.go.jp/shougai/english/annualreport/2020/index-pdf.html (accessed on 1 May 2021).
- Shiratori, Y.; Tachikawa, H.; Nemoto, K.; Endo, G.; Aiba, M.; Matsui, Y.; Asada, T. Network analysis for motives in suicide cases: A cross-sectional study. Psychiatry Clin. Neurosci. 2014, 68, 299–307. [Google Scholar] [CrossRef] [PubMed]






Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kashimoto, K.; Okada, M. Analysing the Impacts of Financial Expenditure of Prefectures on Methods of Suicide Completion in Japan. Psychiatry Int. 2022, 3, 1-16. https://doi.org/10.3390/psychiatryint3010001
Kashimoto K, Okada M. Analysing the Impacts of Financial Expenditure of Prefectures on Methods of Suicide Completion in Japan. Psychiatry International. 2022; 3(1):1-16. https://doi.org/10.3390/psychiatryint3010001
Chicago/Turabian StyleKashimoto, Kanae, and Motohiro Okada. 2022. "Analysing the Impacts of Financial Expenditure of Prefectures on Methods of Suicide Completion in Japan" Psychiatry International 3, no. 1: 1-16. https://doi.org/10.3390/psychiatryint3010001