
A Systematic Review of Economic Evaluations of Insulin for the Management of Type 2 Diabetes

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
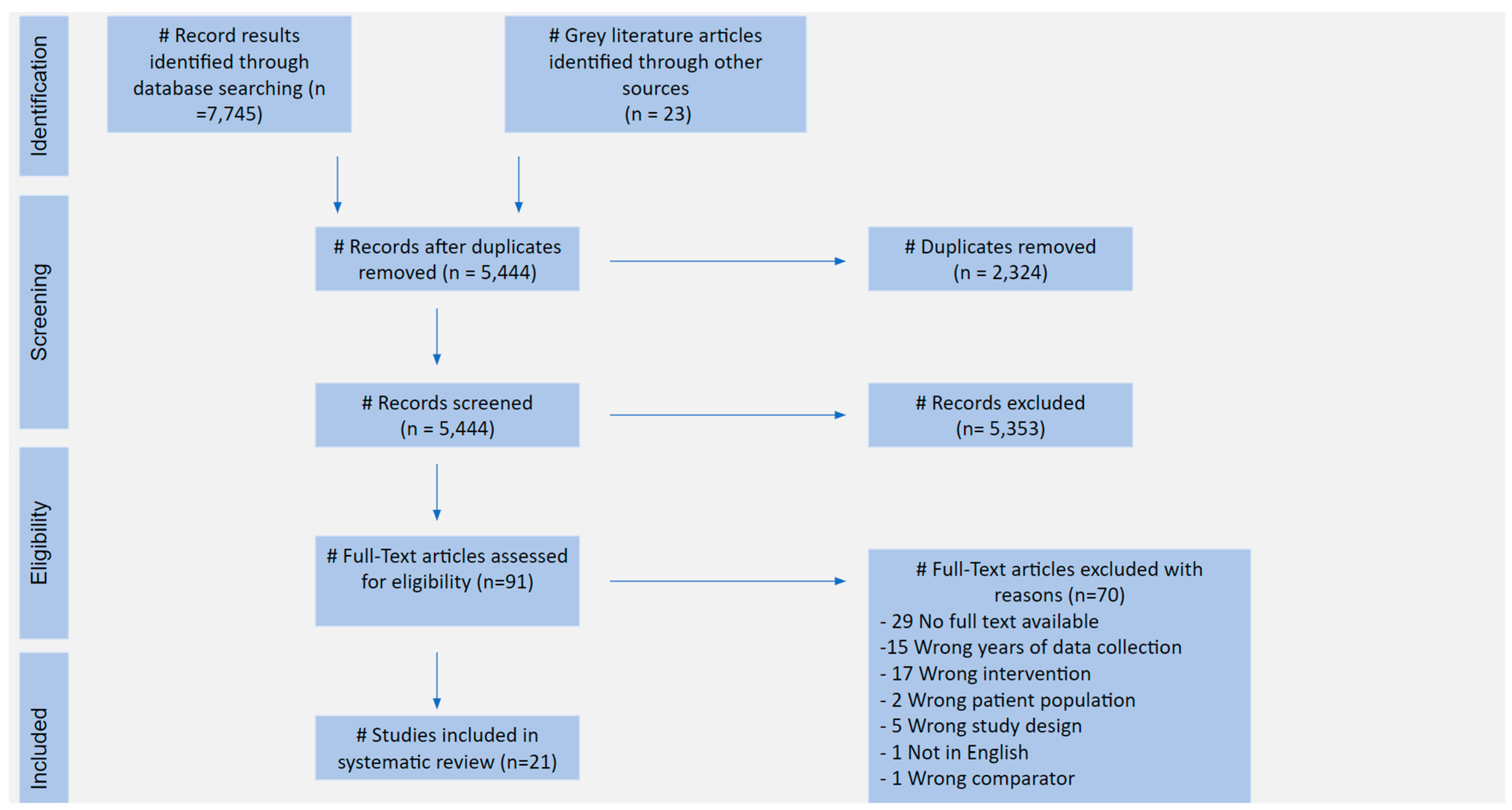
3.1. PRISMA Flowchart
3.2. Studies Selected
3.3. Methodology of Selected Studies
3.4. Quality Appraisal
3.5. Evidence Synthesis
3.5.1. CEA Studies
3.5.2. CUA Studies
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
| Search Strategy | |
|---|---|
| PubMed | (diabetes) AND (insulin) AND (econom* OR economic evaluation). af |
| Embase | (diabetes) AND (insulin) AND (econom OR economic evaluation). af |
| Global Health | (diabetes) AND (insulin) AND (econom* OR economic evaluation). af |
| Medline | (diabetes) AND (insulin) AND (econom* OR economic evaluation). af |
| Limitations | |
| PubMed | 2016–2023 The results of the search were filtered only for English papers |
| Embase | English Language 2016–Current |
| Global Health | English Language 2016–Current |
| Medline | 2016–Current The results of the search were filtered only for English papers |
References
- World Health Organisation: Diabetes. Available online: https://www.who.int/news-room/fact-sheets/detail/diabetes (accessed on 12 September 2023).
- Alshammary, A.F.; Alshammari, A.M.; Alsobaie, S.F.; Alageel, A.A.; Ali Khan, I. Evidence from genetic studies among rs2107538 variant in the CCL5 gene and Saudi patients diagnosed with type 2 diabetes mellitus. Saudi J. Biol. Sci. 2023, 30, 103658. [Google Scholar] [CrossRef]
- Farmaki, P.; Damaskos, C.; Garmpis, N.; Garmpi, A.; Savvanis, S.; Diamantis, E. Complications of the Type 2 Diabetes Mellitus. Curr. Cardiol. Rev. 2020, 16, 249–251. [Google Scholar] [CrossRef]
- Ong, K.L.; Stafford, L.K.; McLaughlin, S.A.; Boyko, E.J.; Vollset, S.E.; Smith, A.E.; Dalton, B.E.; Duprey, J.; Cruz, J.A.; Hagins, H.; et al. Global, regional, and national burden of diabetes from 1990 to 2021, with projections of prevalence to 2050: A systematic analysis for the Global Burden of Disease Study 2021. Lancet 2023, 402, 203–234. [Google Scholar] [CrossRef]
- Davies, M.J.; Aroda, V.R.; Collins, B.S.; Gabbay, R.A.; Green, J.; Maruthur, N.M.; Rosas, S.E.; Del Prato, S.; Mathieu, C.; Mingrone, G.; et al. Management of Hyperglycemia in Type 2 Diabetes, 2022: A Consensus Report by the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD). Diabetes Care 2022, 45, 2753–2786. [Google Scholar] [CrossRef] [PubMed]
- Draznin, B.; Aroda, V.R.; Bakris, G.; Benson, G.; Brown, F.M.; Freeman, R.; Green, J.; Huang, E.; Isaacs, D.; Kahan, S.; et al. Glycemic Targets: Standards of Medical Care in Diabetes-2022. Diabetes Care 2022, 45, S83–S96. [Google Scholar] [CrossRef]
- Viigimaa, M.; Sachinidis, A.; Toumpourleka, M.; Koutsampasopoulos, K.; Alliksoo, S.; Titma, T. Macrovascular Complications of Type 2 Diabetes Mellitus. Curr. Vasc. Pharmacol. 2020, 18, 110–116. [Google Scholar] [CrossRef] [PubMed]
- Faselis, C.; Katsimardou, A.; Imprialos, K.; Deligkaris, P.; Kallistratos, M.; Dimitriadis, K. Microvascular Complications of Type 2 Diabetes Mellitus. Curr. Vasc. Pharmacol. 2020, 18, 117–124. [Google Scholar] [CrossRef] [PubMed]
- Saboo, B.; Kesavadev, J.; Shankar, A.; Krishna, M.B.; Sheth, S.; Patel, V.; Krishnan, G. Time-in-range as a target in type 2 diabetes: An urgent need. Heliyon 2021, 7, e05967. [Google Scholar] [CrossRef]
- Poretsky, L. Principles of Diabetes Mellitus, 2nd ed.; Springer: New York, NY, USA, 2009; pp. 645–658. [Google Scholar]
- Coetzee, A. An introduction to insulin use in type 2 diabetes mellitus. S. Afr. Fam. Pract. 2004, 65, e1–e5. [Google Scholar] [CrossRef]
- Peyrot, M.; Rubin, R.R.; Lauritzen, T.; Skovlund, S.E.; Snoek, F.J.; Matthews, D.R.; Landgraf, R.; Kleinebreil, L. Resistance to insulin therapy among patients and providers: Results of the cross-national Diabetes Attitudes, Wishes, and Needs (DAWN) study. Diabetes Care 2005, 28, 2673–2679. [Google Scholar] [CrossRef]
- Home, P.; Naggar, N.E.; Khamesh, M.; Gonzalez-Galvez, G.; Shen, C.; Chakkarwar, P.; Wenying, Y. An observational non-interventional study of people with diabetes beginning or changed to insulin analogue therapy in non-Western countries: The A1chieve study. Diabetes Res. Clin. Pract. 2022, 94, 352–363. [Google Scholar] [CrossRef]
- Grand Review Research: Insulin Market Size & Share Trends Analysis by Product Type (Rapid-Acting Insulin, Long-Acting Insulin, Combination Insulin, Biosimilar), by Application, by Type (Type 1, Type 2), by Distribution Channel, by Region, and Segment Forecasts, 2022–2030. Available online: https://www.grandviewresearch.com/industry-analysis/insulin-market-report (accessed on 12 September 2023).
- Beran, D.; Lazo-Porras, M.; Mba, C.M.; Mbanya, J.C. A global perspective on the issue of access to insulin. Diabetologia 2021, 64, 954–962. [Google Scholar] [CrossRef] [PubMed]
- Basu, S.; Yudkin, J.S.; Kehlenbrink, S.; Davies, J.I.; Wild, S.H.; Lipska, K.J.; Sussman, J.B.; Beran, D. Estimation of global insulin use for type 2 diabetes, 2018–2030: A microsimulation analysis. Lancet Diabetes Endocrinol. 2019, 7, 25–33. [Google Scholar] [CrossRef] [PubMed]
- Hicks, C.W.; Selvin, E. Epidemiology of Peripheral Neuropathy and Lower Extremity Disease in Diabetes. Curr. Diab. Rep. 2019, 19, 86. [Google Scholar] [CrossRef] [PubMed]
- Kerr, M.; Barron, E.; Chadwick, P.; Evan, T.; Kong, W.M.; Rayman, G.; Sutton-Smith, M.; Todd, G.; Young, B.; Jeffcoate, W.J. The cost of diabetic foot ulcers and amputations to the National Health Service in England. Diabet. Med. 2019, 36, 995–1002. [Google Scholar] [CrossRef]
- Bommer, C.; Sagalova, V.; Heesemann, E.; Manne-Goehler, J.; Atun, R.; Bärnighausen, T.; Davies, J.; Vollmer, S. Global Economic Burden of Diabetes in Adults: Projections from 2015 to 2030. Diabetes Care 2018, 41, 963–970. [Google Scholar] [CrossRef]
- Trikkalinou, A.; Papazafiropoulou, A.K.; Melidonis, A. Type 2 diabetes and quality of life. World J. Diabetes 2017, 8, 120–129. [Google Scholar] [CrossRef]
- Khan, M.A.B.; Hashim, M.J.; King, J.K.; Govender, R.D.; Mustafa, H.; Al Kaabi, J. Epidemiology of Type 2 Diabetes—Global Burden of Disease and Forecasted Trends. J. Epidemiol. Glob. Health 2020, 10, 107–111. [Google Scholar] [CrossRef]
- ISPOR Presentations Database. Available online: https://www.ispor.org/heor-resources/presentations-database/search (accessed on 12 September 2023).
- Tufts Medical Centre: CEA Registry. Available online: https://cear.tuftsmedicalcenter.org/ (accessed on 12 September 2023).
- Houses of Parliament, Parliamentary Office of Science & Technology: Drug Pricing. Available online: https://www.parliament.uk/globalassets/documents/post/postpn_364_Drug_Pricing.pdf (accessed on 12 September 2023).
- PRISMA Transparent Reporting of Systematic Reviews and Meta-Analyses. Available online: http://www.prisma-statement.org/?AspxAutoDetectCookieSupport=1 (accessed on 12 September 2023).
- The BMJ Health Economics Checklist. Available online: https://www.bmj.com/content/suppl/2004/05/06/328.7448.1102.DC1 (accessed on 12 September 2023).
- Equator Network, Consolidated Health Economic Evaluation Reporting Standards 2022 (CHEERS 2022) Statement: Updated Reporting Guidance for Health Economic Evaluations. Available online: https://www.equator-network.org/reporting-guidelines/cheers/ (accessed on 12 September 2023).
- Cannon, A.J.; Bargiota, A.; Billings, L.; Hunt, B.; Leiter, L.A.; Malkin, S.; Mocarski, M.; Ranthe, M.F.; Schiffman, A.; Doshi, A. Evaluation of the Short-Term Cost-Effectiveness of IDegLira versus Basal Insulin and Basal-Bolus Therapy in Patients with Type 2 Diabetes Based on Attainment of Clinically Relevant Treatment Targets. J. Manag. Care Spec. Pharm. 2020, 26, 143–153. [Google Scholar] [CrossRef] [PubMed]
- Cheng, H.; Wan, X.; Ma, J.; Wu, B. Cost-effectiveness of Insulin Degludec versus Insulin Glargine in Insulin-naive Chinese Patients with Type 2 Diabetes. Clin. Ther. 2019, 41, 445–455.e4. [Google Scholar] [CrossRef]
- Dempsey, M.; Mocarski, M.; Langer, J.; Hunt, B. Long-term cost-effectiveness analysis shows that IDegLira is associated with improved outcomes and lower costs compared with insulin glargine U100 plus insulin aspart in the US. J. Med. Econ. 2018, 21, 1110–1118. [Google Scholar] [CrossRef]
- Drummond, R.; Malkin, S.; Du Preez, M.; Lee, X.Y.; Hunt, B. The management of type 2 diabetes with fixed-ratio combination insulin degludec/liraglutide (IDegLira) versus basal-bolus therapy (insulin glargine U100 plus insulin aspart): A short-term cost-effectiveness analysis in the UK setting. Diabetes Obes. Metab. 2018, 20, 2371–2378. [Google Scholar] [CrossRef] [PubMed]
- Evans, M.; Chubb, B.; Malkin, S.J.P.; Berry, S.; Lawson, J.; Hunt, B. Once-weekly semaglutide versus insulin aspart for the treatment of type 2 diabetes in the UK: A long-term cost-effectiveness analysis based on SUSTAIN 11. Diabetes Obes. Metab. 2023, 25, 491–500. [Google Scholar] [CrossRef] [PubMed]
- Gu, S.; Shi, L.; Shao, H.; Wang, X.; Hu, X.; Gu, Y.; Dong, H. Choice across 10 pharmacologic combination strategies for type 2 diabetes: A cost-effectiveness analysis. BMC Med. 2020, 18, 378. [Google Scholar] [CrossRef] [PubMed]
- Han, G.; Hu, S.; Zhang, X.; Qiu, Z.; Huang, Z. Insulin degludec/liraglutide versus its monotherapy on T2D patients: A lifetime cost-utility analysis in China. Front. Pharmacol. 2022, 13, 1011624. [Google Scholar] [CrossRef]
- Hunt, B.; Mocarski, M.; Valentine, W.J.; Langer, J. Evaluation of the Short-Term Cost-Effectiveness of IDegLira Versus Continued Up-Titration of Insulin Glargine U100 in Patients with Type 2 Diabetes in the USA. Adv. Ther. 2017, 34, 954–965. [Google Scholar] [CrossRef]
- Jiang, Y.; Liu, R.; Xuan, J.; Lin, S.; Zheng, Q.; Pang, J. A Cost-effectiveness Analysis of iGlarLixi Versus IDegAsp and Appropriate Price Exploration of iGlarLixi for Type 2 Diabetes Mellitus Patients in China. Clin. Drug Investig. 2023, 43, 251–263. [Google Scholar] [CrossRef]
- Kvapil, M.; Prázný, M.; Holik, P.; Rychna, K.; Hunt, B. Cost-Effectiveness of IDegLira Versus Insulin Intensification Regimens for the Treatment of Adults with Type 2 Diabetes in the Czech Republic. Diabetes Ther. 2017, 8, 1331–1347. [Google Scholar] [CrossRef]
- Langer, J.; Wolden, M.L.; Shimoda, S.; Sato, M.; Araki, E. Short-Term Cost-Effectiveness of Switching to Insulin Degludec in Japanese Patients with Type 2 Diabetes Receiving Basal-Bolus Therapy. Diabetes Ther. 2019, 10, 1347–1356. [Google Scholar] [CrossRef]
- Lau, E.; Salem, A.; Chan, J.C.N.; So, W.Y.; Kong, A.; Lamotte, M.; Luk, A. Insulin glargine compared to Neutral Protamine Hagedorn (NPH) insulin in patients with type-2 diabetes uncontrolled with oral anti-diabetic agents alone in Hong Kong: A cost-effectiveness analysis. Cost Eff. Resour. Alloc. 2019, 17, 13. [Google Scholar] [CrossRef]
- Luo, Q.; Zhou, L.; Zhou, N.; Hu, M. Cost-effectiveness of insulin degludec/insulin aspart versus biphasic insulin aspart in Chinese population with type 2 diabetes. Front. Public Health 2022, 10, 1016937. [Google Scholar] [CrossRef]
- McCrimmon, R.J.; Falla, E.; Sha, J.Z.; Alsaleh, A.J.O.; Lew, E.; Hudson, R.; Baxter, M.; Palmer, K. Cost-Effectiveness of iGlarLixi in People with Type 2 Diabetes Mellitus Suboptimally Controlled on Basal Insulin Plus Metformin in the UK. Diabetes Ther. 2021, 12, 3217–3230. [Google Scholar] [CrossRef] [PubMed]
- McCrimmon, R.J.; Lamotte, M.; Ramos, M.; Alsaleh, A.J.O.; Souhami, E.; Lew, E. Cost-Effectiveness of iGlarLixi Versus iDegLira in Type 2 Diabetes Mellitus Inadequately Controlled by GLP-1 Receptor Agonists and Oral Antihyperglycemic Therapy. Diabetes Ther. 2021, 12, 3231–3241. [Google Scholar] [CrossRef] [PubMed]
- Pöhlmann, J.; Montagnoli, R.; Lastoria, G.; Parekh, W.; Markert, M.; Hunt, B. Value For Money In The Treatment Of Patients With Type 2 Diabetes Mellitus: Assessing The Long-Term Cost-Effectiveness of IDegLira Versus iGlarLixi In Italy. Clin. Outcomes Res. 2019, 11, 605–614. [Google Scholar] [CrossRef]
- Pöhlmann, J.; Russel-Szymczyk, M.; Holík, P.; Rychna, K.; Hunt, B. Treating Patients with Type 2 Diabetes Mellitus Uncontrolled on Basal Insulin in the Czech Republic: Cost-Effectiveness of IDegLira Versus iGlarLixi. Diabetes Ther. 2019, 10, 493–508. [Google Scholar] [CrossRef] [PubMed]
- Pollock, R.F.; Norrbacka, K.; Cameron, C.; Mancillas-Adame, L.; Jeddi, M. A cost-utility analysis of dulaglutide versus insulin glargine as third-line therapy for Type 2 diabetes in Canada. J. Comp. Eff. Res. 2019, 8, 229–240. [Google Scholar] [CrossRef]
- Pollock, R.F.; Valentine, W.J.; Marso, S.P.; Gundgaard, J.; Hallén, N.; Hansen, L.L.; Tutkunkardas, D.; Buse, J.B. DEVOTE 5: Evaluating the Short-Term Cost-Utility of Insulin Degludec versus Insulin Glargine U100 in Basal-Bolus Regimens for Type 2 Diabetes in the UK. Diabetes Ther. 2018, 9, 1217–1232. [Google Scholar] [CrossRef] [PubMed]
- Pollock, R.F.; Valentine, W.J.; Marso, S.P.; Andersen, A.; Gundgaard, J.; Hallén, N.; Tutkunkardas, D.; Magnuson, E.A.; Buse, J.B. Long-term Cost-effectiveness of Insulin Degludec Versus Insulin Glargine U100 in the UK: Evidence from the Basal-bolus Subgroup of the DEVOTE Trial (DEVOTE 16). Appl. Health Econ. Health Policy 2019, 17, 615–627. [Google Scholar] [CrossRef]
- Raya, P.M.; Blasco, F.J.A.; Hunt, B.; Martin, V.; Thorsted, B.L.; Basse, A.; Price, H. Evaluating the long-term cost-effectiveness of fixed-ratio combination insulin degludec/liraglutide (IDegLira) for type 2 diabetes in Spain based on real-world clinical evidence. Diabetes Obes. Metab. 2019, 21, 1349–1356. [Google Scholar] [CrossRef] [PubMed]
- Zhong, Y.; Lin, P.J.; Cohen, J.T.; Winn, A.N.; Neumann, P.J. Cost-utility analyses in diabetes: A systematic review and implications from real-world evidence. Value Health 2015, 18, 308–314. [Google Scholar] [CrossRef]
- Saunders, H.; Pham, B.; Loong, D.; Mishra, S.; Ashoor, H.M.; Antony, J.; Darvesh, N.; Bains, S.K.; Jamieson, M.; Plett, D.; et al. The Cost-Effectiveness of Intermediate-Acting, Long-Acting, Ultralong-Acting, and Biosimilar Insulins for Type 1 Diabetes Mellitus: A Systematic Review. Value Health 2022, 25, 1235–1252. [Google Scholar] [CrossRef] [PubMed]
- Shafie, A.A.; Ng, C.H.; Tan, Y.P.; Chaiyakunapruk, N. Systematic Review of the Cost Effectiveness of Insulin Analogues in Type 1 and Type 2 Diabetes Mellitus. Pharmacoeconomics 2017, 35, 141–162. [Google Scholar] [CrossRef] [PubMed]
- Suh, D.C.; Aagren, M. Cost-effectiveness of insulin detemir: A systematic review. Expert Rev. Pharmacoeconomics Outcomes Res. 2011, 11, 641–655. [Google Scholar] [CrossRef] [PubMed]

| Population | Intervention | Comparator | Outcome | Study Design |
|---|---|---|---|---|
| Patients with T2D * | Insulin | Insulin or other pharmaceutical products | Effectiveness and cost-effectiveness in the management of T2D * | CEA 1 CUA 2 |
| # | First Author | Year of Publication | Setting | Study Type | Comparison |
|---|---|---|---|---|---|
| 1 | Cannon, A.J. [28] | 2020 | USA | Cost-effectiveness analysis | Insulin degludec/liraglutide versus basal insulin and basal-bolus therapy |
| 2 | Cheng, H. [29] | 2019 | China | Cost-effectiveness analysis | Insulin degludec versus insulin glargine |
| 3 | Dempsey, M. [30] | 2018 | USA | Cost-effectiveness analysis | Insulin degludec/liraglutide versus insulin glargine U100 plus insulin aspart |
| 4 | Drummond, R. [31] | 2018 | UK | Cost-effectiveness analysis | Insulin degludec/liraglutide versus insulin glargine U100 plus insulin aspart |
| 5 | Evans, M. [32] | 2023 | UK | Cost-effectiveness analysis | Insulin aspart versus once-weekly semaglutide |
| 6 | Gu, S. [33] | 2020 | China | Cost-effectiveness analysis | Insulin vs. other agents (10 pharmacologic combination strategies overall) |
| 7 | Han, G. [34] | 2022 | China | Cost–utility analysis | Insulin degludec/liraglutide versus its single components—degludec or liraglutide |
| 8 | Hunt, B. [35] | 2017 | USA | Cost-effectiveness analysis | Insulin degludec/liraglutide versus insulin glargine U100 |
| 9 | Jiang, Y. [36] | 2023 | China | Cost-effectiveness analysis | Insulin glargine U100/lixisenatide versus insulin degludec/insulin aspart |
| 10 | Kvapil, M. [37] | 2017 | Czech Republic | Cost-effectiveness analysis | Insulin degludec/liraglutide versus basal insulin intensification strategies |
| 11 | Langer, J. [38] | 2019 | Japan | Cost-effectiveness analysis | Insulin degludec vs. other basal insulins |
| 12 | Lau, E. [39] | 2019 | Hong Kong | Cost-effectiveness analysis | Insulin glargine U100 versus NPH * insulin |
| 13 | Luo, Q. [40] | 2022 | China | Cost-effectiveness analysis | Insulin degludec/insulin aspart versus biphasic insulin aspart 30 |
| 14 | McCrimmon, R.J. (iGlarLixi vs. basal insulin plus metformin) [41] | 2021 | UK | Cost-effectiveness analysis | Insulin glargine U100/lixisenatide versus insulin degludec/liraglutide and the free-combination comparators insulin glargine plus dulaglutide and basal insulin plus liraglutide |
| 15 | McCrimmon, R.J. (iGlarLixi Versus iDegLira) [42] | 2021 | UK | Cost-effectiveness analysis | Insulin glargine U100/lixisenatide versus insulin degludec/liraglutide |
| 16 | Pöhlmann, J. (ClinicoEcon Outcomes) [43] | 2019 | Italy | Cost-effectiveness analysis | Insulin degludec/liraglutide versus insulin glargine U100/lixisenatide |
| 17 | Pöhlmann, J. (Diabetes Ther.) [44] | 2019 | Czech Republic | Cost-effectiveness analysis | Insulin degludec/liraglutide versus insulin glargine U100/lixisenatide |
| 18 | Pollock, R.F. [45] | 2019 | Canada | Cost-utility analysis | Insulin glargine versus dulaglutide |
| 19 | Pollock, R.F. [46] | 2018 | UK | Cost-utility analysis | Insulin degludec versus insulin glargine U100 |
| 20 | Pollock, R.F. (Applied Health Economics and Health Policy) [47] | 2019 | UK | Cost-effectiveness analysis | Insulin degludec versus insulin glargine U100 |
| 21 | Raya, P.M. [48] | 2019 | Spain | Cost-effectiveness | Insulin degludec/liraglutide versus comparator regimens |
| # | First Author | Score on BMJ * Checklist |
|---|---|---|
| 1 | Cannon, A.J. [28] | 34/35 |
| 2 | Cheng, H. [29] | 35/35 |
| 3 | Dempsey, M. [30] | 35/35 |
| 4 | Drummond, R. [31] | 34/35 |
| 5 | Evans, M. [32] | 35/35 |
| 6 | Gu, S. [33] | 34/35 |
| 7 | Han, G. [34] | 35/35 |
| 8 | Hunt, B. [35] | 35/35 |
| 9 | Jiang, Y. [36] | 32/35 |
| 10 | Kvapil, M. [37] | 33/35 |
| 11 | Langer, J. [38] | 35/35 |
| 12 | Lau, E. [39] | 34/35 |
| 13 | Luo, Q. [40] | 35/35 |
| 14 | McCrimmon, R.J. (iGlarLixi vs. basal insulin plus metformin) [41] | 34/35 |
| 15 | McCrimmon, R.J. (iGlarLixi Versus iDegLira) [42] | 34/35 |
| 16 | Pöhlmann, J. (ClinicoEcon Outcomes) [43] | 35/35 |
| 17 | Pöhlmann, J. (Diabetes Ther.) [44] | 34/35 |
| 18 | Pollock, R.F. (2019) [45] | 35/35 |
| 19 | Pollock, R.F. (2018) [46] | 35/35 |
| 20 | Pollock, R.F. (Applied Health Economics and Health Policy) [47] | 35/35 |
| 21 | Raya, P.M. [48] | 34/35 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gkrinia, E.M.M.; Faour, A.K.; Belančić, A.; Bazile, J.; Marland, E.; Vitezić, D. A Systematic Review of Economic Evaluations of Insulin for the Management of Type 2 Diabetes. Diabetology 2023, 4, 440-452. https://doi.org/10.3390/diabetology4040038
Gkrinia EMM, Faour AK, Belančić A, Bazile J, Marland E, Vitezić D. A Systematic Review of Economic Evaluations of Insulin for the Management of Type 2 Diabetes. Diabetology. 2023; 4(4):440-452. https://doi.org/10.3390/diabetology4040038
Chicago/Turabian StyleGkrinia, Elvira Meni Maria, Andrea Katrin Faour, Andrej Belančić, Jacques Bazile, Emma Marland, and Dinko Vitezić. 2023. "A Systematic Review of Economic Evaluations of Insulin for the Management of Type 2 Diabetes" Diabetology 4, no. 4: 440-452. https://doi.org/10.3390/diabetology4040038