
Implementation and Evaluation of a Mobile Retinal Image Acquisition System for Screening Diabetic Retinopathy: Study Protocol


 , and
, and
Abstract
:1. Introduction
1.1. Background and Rationale
1.2. Objectives
1.2.1. Primary Objectives
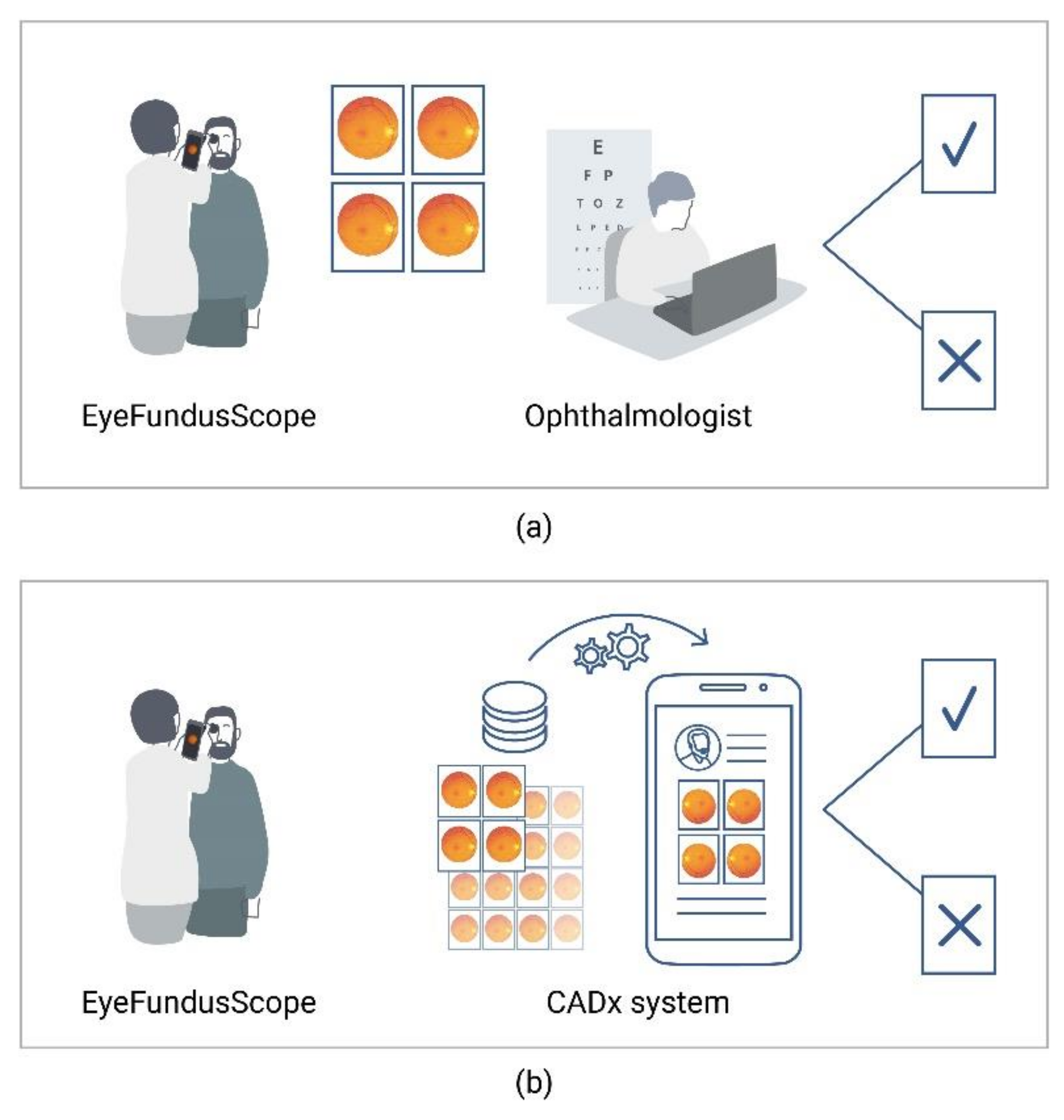
- To assess the diagnostic accuracy of using EyeFundusScope alone and along with the CADx system for diabetic retinopathy classification.
1.2.2. Secondary Objectives
- To assess the image quality and technological functioning of EyeFundusScope in real clinical settings.
- To analyse the association of patients’ clinical characteristics with test accuracy and the quality of images acquired with EyeFundusScope.
- To assess the inter and intraoperator agreement and reliability of EyeFundusScope for diabetic retinopathy classification.
- To assess the usability and acceptance of EyeFundusScope.
- To optimize the ground truth for training an AI software for diabetic retinopathy and image quality automated classification.
2. Methods
2.1. Study Design
- A diagnostic test accuracy cross-sectional study, in which a sample of individuals with diabetes will be prospectively included and screened for diabetic retinopathy by EyeFundusScope (index test) and a tabletop fundus camera (reference standard test); and
- A pilot study using a handheld nonmydriatic fundus camera operated by physicians and nurses not specialists in ophthalmology in another sample of individuals—this study includes image quality, screening results agreement with these images, usability, and acceptance.
2.2. Eligibility Criteria, Study Setting, Recruitment, and Sample Size
2.3. Diagnostic Accuracy Study
2.3.1. Index Test
2.3.2. Reference Test
2.4. Inter and Intraoperator Agreement and Reliability
2.5. Image Quality and Technical Performance
2.6. Usability
2.7. Technology Acceptance
2.8. Data Collection Methods and Management
2.8.1. Data Collection Methods
2.8.2. Data Management
2.9. Monitoring
2.9.1. Data Monitoring
2.9.2. Harms
2.9.3. Auditing
2.10. Ethics and Dissemination
2.11. Statistical Analysis
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| Category | Characteristics |
|---|---|
| Sociodemographic | Age Sex |
| Clinical | Type of diabetes Duration of diabetes Other eye diseases: cataract, glaucoma, age-related macular degeneration, myopia (number of diopters), other Current diabetic retinopathy classification (reference standard) |
| Laboratory | HbA1c |
Appendix B

Appendix C
- Age________
- Sex: Feminine____ Masculine____
- Profession: _______________________________
- Number of years of professional experience ______________
- Do you have a smartphone or have experience using smartphones? Yes____ No____
- Could you give a good and a bad example of using the system?______________________________________________________________________________________________________________________________________________________________________________________________________
- Could you tell us what errors happened while you were using the system? Please describe the context and the problems that occurred.______________________________________________________________________________________________________________________________________________________________________________________________________
- Do you think using the system is simple? Yes____ No____
- If you think not, which aspects in your opinion could be improved?______________________________________________________________________________________________________________________________________________________________________________________________________
- Do you think that this system could be used as part of a regular consultation?Yes____ No____Why?___________________________________________________________________________________________________
- Would you recommend to your colleagues the use of this system in their queries?Yes____ No____
- In your opinion, which factors are favourable to the use of this system in the implementation of screening for diabetic retinopathy in the context of a regular consultation?____________________________________________________________________________________________
- What factors can make it difficult? ________________________________________________________________
- Did you notice some discomfort on users regarding the use of the equipment under study?Yes____ No____If yes, what is the estimated percentage of cases in which this occurred?0%____ 1 a 25%____ 26 a 50%____ 51 a 75%____ 76 a 99%____ 100%____If yes, what did they verbalize?______________________________________________________________________________________________________________________________________________________________________________________________________
- Did you notice some distrust on users regarding the use of the equipment under study?Yes____ No____If so, what is the estimate of cases in which this occurred?0%____ 1 a 25%____ 26 a 50%____ 51 a 75%____ 76 a 99%____ 100%____If yes, what did they verbalize?______________________________________________________________________________________________________________________________________________________________________________________________________
- Overall, is there some aspect of the system that you think could be improved?Yes____ No____What are these aspects?______________________________________________________________________________________________________________________________________________________________________________________________________
Appendix D
- Did you feel some discomfort during the exam with this (new) equipment?Yes____ No____If yes, which? __________________________________________________________________________
- In the next screening, would you do this exam with this (new) equipment again?Yes____ No____
- At the next screening, would you prefer this (new) device over the other?Yes____ No____Why?_____________________________________________________________________________________________________________________________________________________________________________________________
- At the next screening, if only one of the exams was available, which would you prefer?
- Conventional equipment____ New equipment____
References
- Kollias, A.N.; Ulbig, M.W. Diabetic retinopathy: Early diagnosis and effective treatment. Dtsch. Arzteblatt Int. 2010, 107, 75–83. [Google Scholar] [CrossRef]
- Duh, E.J.; Sun, J.K.; Stitt, A.W. Diabetic retinopathy: Current understanding, mechanisms, and treatment strategies. JCI Insight 2017, 2, e93751. [Google Scholar] [CrossRef]
- Annual Report of the National Diabetes Observatory—2016. Available online: https://apdp.pt/publicacoes/relatorio-anual-do-observatorio-nacional-da-diabetes-2016/ (accessed on 1 November 2021).
- Chua, J.; Lim, C.X.Y.; Wong, T.Y.; Sabanayagam, C. Diabetic Retinopathy in the Asia-Pacific. Asia-Pac. J. Ophthalmol. 2018, 7, 3–16. [Google Scholar]
- Pieczyński, J.; Grzybowski, A. Review of Diabetic Retinopathy Screening Methods and Programmes Adopted in Different Parts of the World. Eur. Ophthalmic Rev. 2015, 9, 49–55. [Google Scholar] [CrossRef] [Green Version]
- Panwar, N.; Huang, P.; Lee, J.; Keane, P.A.; Chuan, T.S.; Richhariya, A.; Teoh, S.; Lim, T.H.; Agrawal, R. Fundus Photography in the 21st Century—A Review of Recent Technological Advances and Their Implications for Worldwide Healthcare. Telemed. J. E Health 2016, 22, 198–208. [Google Scholar] [CrossRef]
- Carl Zeiss Meditec Clarus 700 Instructions for Use. Available online: https://www.zeiss.co.uk/content/dam/Meditec/gb/Chris/techsupportsite/usermanuals/clarus_700_user_manual.pdf (accessed on 3 December 2021).
- Tufail, A.; Kapetanakis, V.V.; Salas-Vega, S.; Egan, C.; Rudisill, C.; Owen, C.G.; Lee, A.; Louw, V.; Anderson, J.; Liew, G.; et al. An observational study to assess if automated diabetic retinopathy image assessment software can replace one or more steps of manual imaging grading and to determine their cost-effectiveness. In Health Technol Assess; NIHR Journals Library: Southampton, UK, 2016; Volume 20, pp. 1–72. [Google Scholar]
- Tozer, K.; Woodward, M.A.; Newman-Casey, P.A. Telemedicine and Diabetic Retinopathy: Review of Published Screening Programs. J. Endocrinol. Diabetes 2015, 2, 1–10. [Google Scholar]
- Massin, P.; Chabouis, A.; Erginay, A.; Viens-Bitker, C.; Lecleire-Collet, A.; Meas, T.; Denormandie, P.; Choupot, G.; André, B. OPHDIAT: A Telemedical Network Screening System for Diabetic Retinopathy in the Ile-de-France. Diabetes Metab. 2008, 34, 227–234. [Google Scholar] [CrossRef] [PubMed]
- Indian Health Service—The Federal Health Program for American Indians and Alaska Natives. Teleophthalmology. Available online: https://www.ihs.gov/teleophthalmology (accessed on 2 May 2020).
- Diabetic Retinopathy Screening–Standard no. 016/2018. Available online: https://www.dgs.pt/directrizes-da-dgs/normas-e-circulares-normativas/norma-n-0162018-de-13092018-pdf.aspx (accessed on 2 November 2021).
- Hazin, R.; Barazi, M.K.; Summerfield, M. Challenges to establishing nationwide diabetic retinopathy screening programs. Curr. Opin. Ophthalmol. 2011, 22, 174–179. [Google Scholar] [CrossRef]
- AlHargan, M.H.; AlBaker, K.M.; AlFadhel, A.A.; AlGhamdi, M.A.; AlMuammar, S.M.; AlDawood, H.A. Awareness, knowledge, and practices related to diabetic retinopathy among diabetic patients in primary healthcare centers at Riyadh, Saudi Arabia. J. Fam. Med. Prim. Care 2019, 8, 373–377. [Google Scholar] [CrossRef]
- Glasson, N.M.; Larkins, S.L.; Crossland, L.J. What do patients with diabetes and providers think of an innovative Australian model of remote diabetic retinopathy screening? A qualitative study. BMC Health Serv. Res. 2017, 17, 158. [Google Scholar] [CrossRef] [Green Version]
- Piyasena, M.M.P.N.; Murthy, G.V.S.; Yip, J.L.Y.; Gilbert, C.; Zuurmond, M.; Peto, T.; Gordon, I.; Hewage, S.; Kamalakannan, S. Systematic review on barriers and enablers for access to diabetic retinopathy screening services in different income settings. PLoS ONE 2019, 14, e0198979. [Google Scholar] [CrossRef]
- Kashim, R.M.; Newton, P.; Ojo, O. Diabetic Retinopathy Screening: A Systematic Review on Patients’ Non-Attendance. Int. J. Environ. Res. Public Health 2018, 15, 157. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zimmer-Galler, I.E.; Kimura, A.E.; Gupta, S. Diabetic retinopathy screening and the use of telemedicine. Curr. Opin. Ophthalmol. 2015, 26, 167–172. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Prevention of Blindness from Diabetes Mellitus. Available online: https://www.who.int/diabetes/publications/prevention_diabetes2006/en/ (accessed on 1 May 2020).
- Guariguata, L.; Whiting, D.R.; Hambleton, I.; Beagley, J.; Linnenkamp, U.; Shaw, J.E. Global estimates of diabetes prevalence for 2013 and projections for 2035. Diabetes Res. Clin. Pract. 2014, 103, 137–149. [Google Scholar] [CrossRef] [PubMed]
- Scanlon, P.H. Screening Intervals for Diabetic Retinopathy and Implications for Care. Curr. Diab. Rep. 2017, 17, 96. [Google Scholar] [CrossRef] [PubMed]
- DCCT/EDIC Research Group; Nathan, D.M.; Bebu, I.; Hainsworth, D.; Klein, R.; Tamborlane, W.; Lorenzi, G.; Gubitosi-Klug, R.; Lachin, J.M. Frequency of Evidence-Based Screening for Retinopathy in Type 1 Diabetes. N. Engl. J. Med. 2017, 376, 1507–1516. [Google Scholar]
- Ichhpujani, P.; Thakur, S. Apps and Social Networking Pages for Vitreoretinal and Uveal Diseases. In Smart Resources in Ophthalmology: Applications and Social Networking; Springer: Singapore, 2018; pp. 97–140. [Google Scholar]
- Hong, K.; Collon, S.; Chang, D.; Thakalli, S.; Welling, J.; Oliva, M.; Peralta, E.; Gurung, R.; Ruit, S.; Tabin, G.; et al. Teleophthalmology through handheld mobile devices: A pilot study in rural Nepal. J. Mob. Technol. Med. 2019, 8. [Google Scholar] [CrossRef] [PubMed]
- Giardini, M.E.; Livingstone, I.A.T.; Jordan, S.; Bolster, N.M.; Peto, T.; Burton, M.; Bastawrous, A. A smartphone based ophthalmoscope. In Proceedings of the 2014 36th Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Chicago, IL, USA, 26–30 August 2014; IEEE: Piscataway, NJ, USA, 2014; pp. 2177–2180. [Google Scholar]
- Jin, K.; Lu, H.; Su, Z.; Cheng, C.; Ye, J.; Qian, D. Telemedicine screening of retinal diseases with a handheld portable non-mydriatic fundus camera. BMC Ophthalmol. 2017, 17, 89. [Google Scholar] [CrossRef]
- Tan, C.H.; Kyaw, B.M.; Smith, H.; Tan, C.S.; Tudor Car, L. Use of Smartphones to Detect Diabetic Retinopathy: Scoping Review and Meta-Analysis of Diagnostic Test Accuracy Studies. J. Med. Internet Res. 2020, 22, e16658. [Google Scholar] [CrossRef]
- Micheletti, J.M.; Hendrick, A.M.; Khan, F.N.; Ziemer, D.C.; Pasquel, F.J. Current and Next Generation Portable Screening Devices for Diabetic Retinopathy. J. Diabetes Sci. Technol. 2016, 10, 295–300. [Google Scholar] [CrossRef] [PubMed]
- Ocular CellScope. Available online: https://dil.berkeley.edu/technology-portfolio/current-projects/ocular-cellscope/ (accessed on 2 November 2021).
- Fundus on Phone. Available online: https://www.remidio.com/products/fop (accessed on 2 November 2021).
- D-Eye Portable Ophthalmoscope. Available online: https://www.digitaleyecenter.com/product/d-eye-portable-ophthalmoscope (accessed on 2 November 2021).
- Volk VistaView. Available online: https://www.volk.com/pages/vistaviw (accessed on 2 November 2021).
- Ophtha: Decentralised Screening in Ophthalmology. Available online: https://www.aicos.fraunhofer.pt/en/our_work/portfolio/ophtha.html (accessed on 2 November 2021).
- Pictor Prestige Portable Fundus Camera. Available online: https://www.volk.com/pages/prestige (accessed on 2 November 2021).
- van der Heijden, A.A.; Abramoff, M.D.; Verbraak, F.; an Hecke, M.V.; Liem, A.; Nijpels, G. Validation of automated screening for referable diabetic reti-nopathy with the IDx-DR device in the Hoorn Diabetes Care System. Acta Ophthalmol. 2018, 96, 63–68. [Google Scholar] [CrossRef] [PubMed]
- Medios DR Remidio. Available online: https://www.remidio.com/products/medios-dr (accessed on 2 November 2021).
- Natarajan, S.; Jain, A.; Krishnan, R.; Rogye, A.; Sivaprasad, S. Diagnostic Accuracy of Community-Based Diabetic Retinopathy Screening With an Offline Artificial Intelligence System on a Smartphone. JAMA Ophthalmol. 2019, 137, 1182–1188. [Google Scholar] [CrossRef] [PubMed]
- The Dilated Eye Exam: Why It’s So Important. Available online: https://www.brightfocus.org/glaucoma/article/dilated-eye-exam-why-its-so-important (accessed on 2 December 2021).
- Karakaya, M.; Hacisoftaoglu, R.E. Comparison of smartphone-based retinal imaging systems for diabetic retinopathy detection using deep learning. BMC Bioinform. 2020, 21, 259. [Google Scholar] [CrossRef]
- Goh, J.K.H.; Cheung, C.Y.; Sim, S.S.; Tan, P.C.; Tan, G.S.W.; Wong, T.Y. Retinal Imaging Techniques for Diabetic Retinopathy Screening. J. Diabetes Sci. Technol. 2016, 10, 282–294. [Google Scholar] [CrossRef] [Green Version]
- Minims Tropicamide 0.5% w/v, Eye Drops Solution-Summary of Product Characteristics. Available online: https://www.medicines.org.uk/emc/product/1379/smpc#gref (accessed on 8 December 2021).
- Dervan, E.; Lillis, D.; Flynn, L.; Staines, A.; O’Shea, D. Factors that influence the patient uptake of diabetic retinopathy screening. Ir. J. Med. Sci. 2008, 177, 303–308. [Google Scholar] [CrossRef]
- Nunes, F.; Madureira, P.; Rêgo, S.; Braga, C.; Moutinho, R.; Oliveira, T.; Soares, F. A Mobile Tele-Ophthalmology System for Planned and Opportunistic Screening of Diabetic Retinopathy in Primary Care. IEEE Access 2021, 9, 83740–83750. [Google Scholar] [CrossRef]
- Felgueiras, S.; Costa, J.; Gonçalves, J.; Soares, F. Mobile-based Risk Assessment of Diabetic Retinopathy using a Smartphone and Adapted Ophthalmoscope. In Proceedings of the 11th International Joint Conference on Biomedical Engineering Systems and Technologies; SCITEPRESS-Science and Technology Publications, Funchal, Madeira, Portugal, 19–21 January 2018; pp. 168–175. [Google Scholar]
- Rêgo, S.; Dutra-Medeiros, M.; Soares, F.; Monteiro-Soares, M. Screening for Diabetic Retinopathy Using an Automated Diagnostic System Based on Deep Learning: Diagnostic Accuracy Assessment. Ophthalmologica 2021, 244, 250–257. [Google Scholar] [CrossRef]
- Design Considerations for Pivotal Clinical Investigations for Medical Devices. Available online: https://www.fda.gov/regulatory-information/search-fda-guidance-documents/design-considerations-pivotal-clinical-investigations-medical-devices (accessed on 2 November 2021).
- Braga, C.; Rêgo, S.; Nunes, F. Clinicians’ Perspectives on Using Mobile Eye Fundus Cameras to Screen Diabetic Retinopathy in Primary Care. In Proceedings of the 2020 IEEE International Conference on Healthcare Informatics (ICHI), Oldenburg, Germany, 30 November–3 December 2020; pp. 1–7. [Google Scholar]
- Piyasena, M.M.P.N.; Gudlavalleti, V.S.M.; Gilbert, C.; Yip, J.L.; Peto, T.; MacLeod, D.; Fonseka, C.; Kulatunga, A.; Bandutilake, B.; Dhanapala, M.; et al. Development and Validation of a Diabetic Retinopathy Screening Modality Using a Hand-Held Nonmydriatic Digital Retinal Camera by Physician Graders at a Tertiary-Level Medical Clinic: Protocol for a Validation Study. JMIR Res. Protoc. 2018, 7, e10900. [Google Scholar] [CrossRef]
- Shen, Z.; Fu, H.; Shen, J.; Shao, L. Modeling and Enhancing Low-Quality Retinal Fundus Images. IEEE Trans. Med. Imaging 2021, 40, 996–1006. [Google Scholar] [CrossRef]
- Cohen, J.F.; Korevaar, D.A.; Altman, D.G.; Bruns, D.E.; Gatsonis, C.A.; Hooft, L.; Irwig, L.; Levine, D.; Reitsma, J.B.; de Vet, H.C.W.; et al. STARD 2015 guidelines for reporting diagnostic accuracy studies: Explanation and elaboration. BMJ Open 2016, 6, e012799. [Google Scholar] [CrossRef] [PubMed]
- Retinopatia Diabética-Patologias. Available online: https://www.institutoderetina.pt/patologias/retina/retinopatia-diabetica/10/ (accessed on 2 November 2021).
- Diabetic Retinopathy Screening: A Short Guide. Increase Effectiveness, Maximize Benefits and Minimize Harm. Available online: https://apps.who.int/iris/bitstream/handle/10665/336660/9789289055321-eng.pdf (accessed on 2 November 2021).
- Ruamviboonsuk, P.; Teerasuwanajak, K.; Tiensuwan, M.; Yuttitham, K. Thai Screening for Diabetic Retinopathy Study Group Interobserver agreement in the interpretation of single-field digital fundus images for diabetic retinopathy screening. Ophthalmology 2006, 113, 826–832. [Google Scholar] [CrossRef] [PubMed]
- Gegundez-Arias, M.E.; Ortega, C.; Garrido, J.; Ponte, B.; Alvarez, F.; Marin, D. Inter-observer Reliability and Agreement Study on Early Diagnosis of Diabetic Retinopathy and Diabetic Macular Edema Risk. In Proceedings of the International Conference on Bioinformatics and Biomedical Engineering, Granada, Spain, 20–22 April 2016; pp. 369–379. [Google Scholar]
- Rêgo, S.; Dutra-Medeiros, M.; Bacelar-Silva, G.M.; Borges, T.; Soares, F.; Monteiro-Soares, M. Reliability of Classification by Ophthalmologists with Telescreening Fundus Images for Diabetic Retinopathy and Image Quality. J. Diabetes Sci. Technol. 2021, 15, 710–712. [Google Scholar] [CrossRef] [PubMed]
- Northern Region Diabetic Retinopathy Screening Procedures Manual. Available online: http://www.arsnorte.min-saude.pt/wp-content/uploads/sites/3/2018/01/Manual-Rastreio-da-Retinopatia-Diabetica-ARSN.pdf (accessed on 2 November 2021).
- Simões, B.R.B.A. Image Quality Improvement of Medical Images Using Deep Learning for Computer-Aided Diagnosis. Master’s Thesis, NOVA University Lisbon, Lisbon, Portugal, 2021. [Google Scholar]
- Brooke, J. SUS: A quick and dirty usability scale. In Usability Evaluation in Industry, 1st ed.; Jordan, P.W., Thomas, B., McClelland, I.L., Weerdmeester, B., Eds.; CRC Press: London, UK, 1996. [Google Scholar]
- Martins, A.I.; Rosa, A.F.; Queirós, A.; Silva, A.; Rocha, N.P. European Portuguese Validation of the System Usability Scale (SUS). Procedia Comput. Sci. 2015, 67, 293–300. [Google Scholar] [CrossRef] [Green Version]
- Braun, V.; Clarke, V. Thematic analysis. In APA Handbook of Research Methods in Psychology; Volume 2: Research Designs: Quantitative, Qualitative, Neuropsychological, and Biologica; American Psychological Association: Washington, DC, USA, 2012; pp. 57–71. [Google Scholar]
- ISO 14155: 2020 Clinical Investigation of Medical Devices for Human Subjects—Good Clinical Practice. Available online: https://www.iso.org/standard/71690.html (accessed on 2 November 2021).
- Darma, S.; Zantvoord, F.; Verbraak, F.D. The quality and usability of smartphone and hand-held fundus photography, compared to standard fundus photography. Acta Ophthalmol. 2015, 93, e310–e311. [Google Scholar] [CrossRef]
- Lin, T.-C.; Chiang, Y.-H.; Hsu, C.-L.; Liao, L.-S.; Chen, Y.-Y.; Chen, S.-J. Image quality and diagnostic accuracy of a handheld nonmydriatic fundus camera: Feasibility of a telemedical approach in screening retinal diseases. J. Chin. Med. Assoc. 2020, 83, 962–966. [Google Scholar] [CrossRef] [PubMed]
- Scanlon, P.H. The English National Screening Programme for Diabetic Retinopathy 2003–2016. Acta Diabetol. 2017, 54, 515–525. [Google Scholar] [CrossRef] [PubMed] [Green Version]

| Severity Levels | Characteristics |
|---|---|
| R0 | No retinopathy: any lesion related to DR 1 |
| R1 | Mild non-proliferative retinopathy: microaneurysms, retinal haemorrhages with or without any exudate excluding the definition of DME 2 |
| R2 | Moderate or severe pre-proliferative: “rosary” veins, venous loops and duplications, intra-retinal microvascular anomalies, multiple, deep, cottony exudates |
| R3 | Proliferative: disc neo-vessels, retinal neo-vessels, vitreous or pre-retinal haemorrhage, pre-retinal fibrosis with or without traditional retinal detachment |
| M1 | Maculopathy: Presence of exudates less than 1 DD 3 from the centre of the fovea, or circinate or grouped exudates in the macular area, or retinal thickening to less than 1 DD 3 from the centre of the fovea, or any microaneurysm or haemorrhage less than 1 DD 3 from the centre of the fovea, if associated with an AV 4 < 0.5 |
| P0 | Photocoagulated retina not needing more treatment |
| P1 | Photocoagulated retina needing more treatment |
| Not classifiable | Non-informative image |
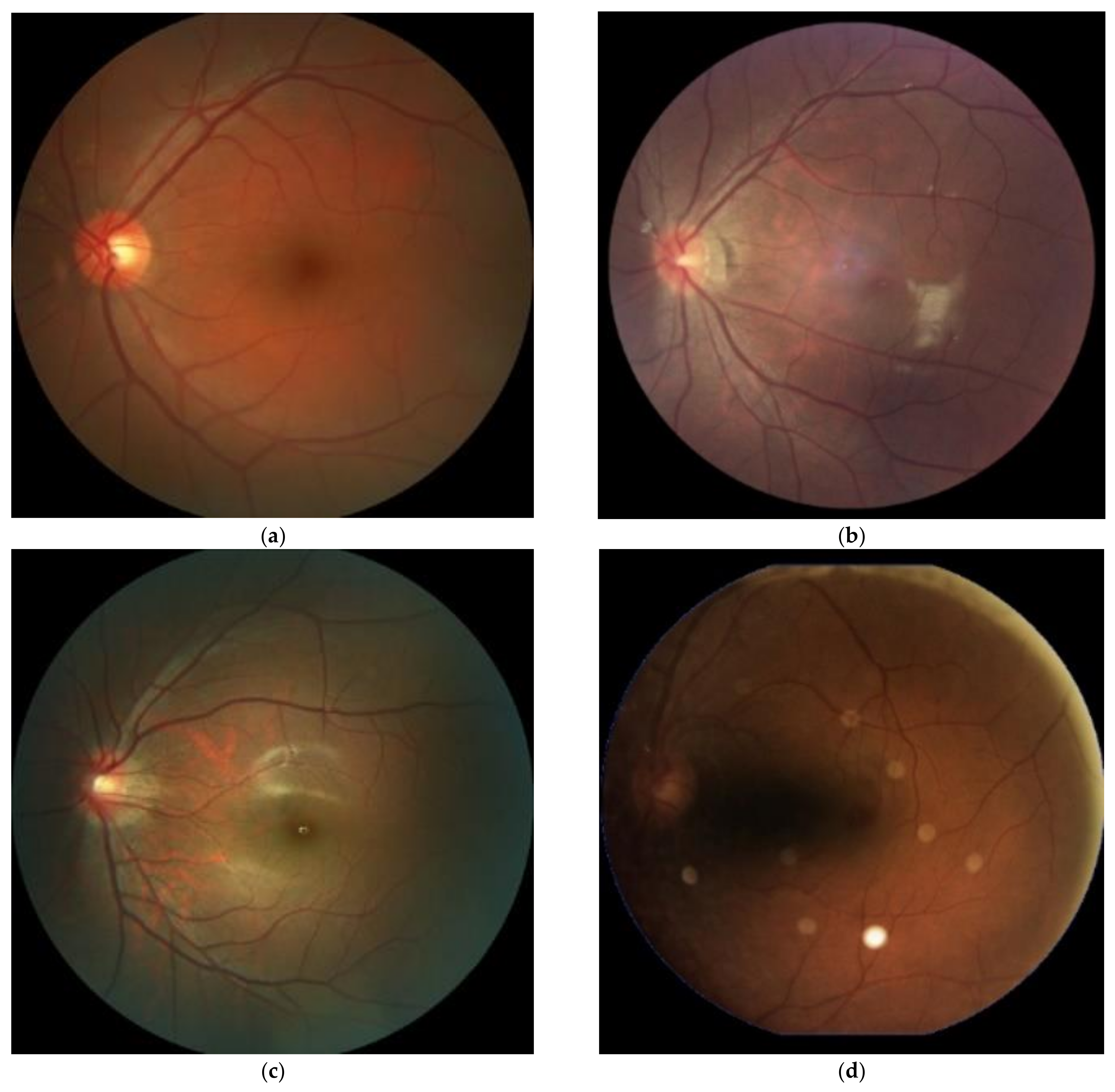
| Image Quality Level | Characteristics |
|---|---|
| Excellent |
|
| Good |
|
| Usable |
|
| Inadequate |
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rêgo, S.; Monteiro-Soares, M.; Dutra-Medeiros, M.; Soares, F.; Dias, C.C.; Nunes, F. Implementation and Evaluation of a Mobile Retinal Image Acquisition System for Screening Diabetic Retinopathy: Study Protocol. Diabetology 2022, 3, 1-16. https://doi.org/10.3390/diabetology3010001
Rêgo S, Monteiro-Soares M, Dutra-Medeiros M, Soares F, Dias CC, Nunes F. Implementation and Evaluation of a Mobile Retinal Image Acquisition System for Screening Diabetic Retinopathy: Study Protocol. Diabetology. 2022; 3(1):1-16. https://doi.org/10.3390/diabetology3010001
Chicago/Turabian StyleRêgo, Sílvia, Matilde Monteiro-Soares, Marco Dutra-Medeiros, Filipe Soares, Cláudia Camila Dias, and Francisco Nunes. 2022. "Implementation and Evaluation of a Mobile Retinal Image Acquisition System for Screening Diabetic Retinopathy: Study Protocol" Diabetology 3, no. 1: 1-16. https://doi.org/10.3390/diabetology3010001