
Targeted Antimicrobial Prophylaxis with Cefmetazole Based on Presence of Fluoroquinolone-Resistant Isolates to Prevent Post-Prostate Biopsy Infectious Complications
 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population, Rectal Swab Method, and Endpoints
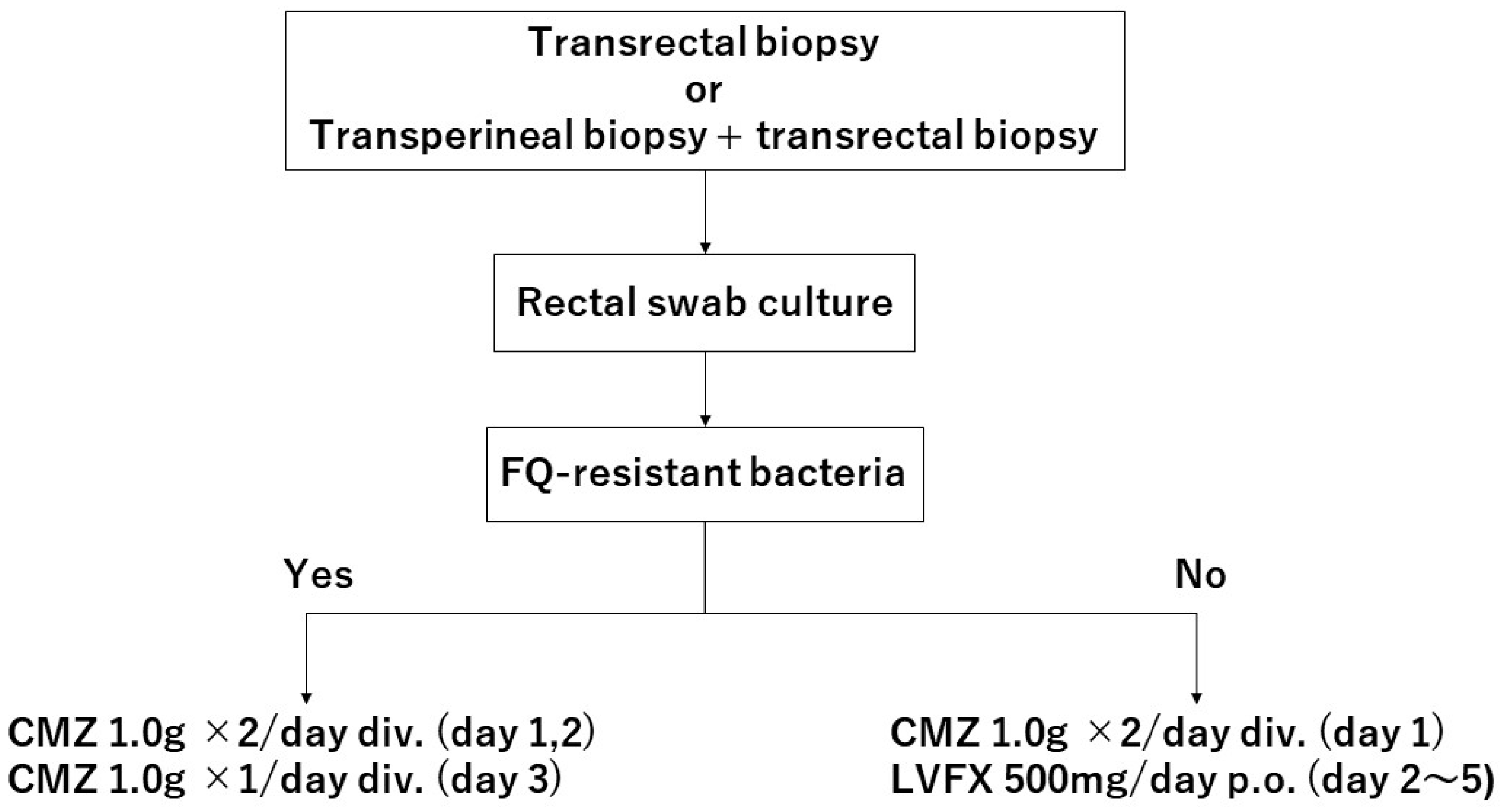
2.2. Antibiotic Prophylaxis before and after Prostate Biopsy
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Katanoda, K.; Hori, M.; Saito, E.; Shibata, A.; Ito, Y.; Minami, T.; Ikeda, S.; Suzuki, T.; Matsuda, T. Updated Trends in Cancer in Japan: Incidence in 1985–2015 and Mortality in 1958–2018—A Sign of Decrease in Cancer Incidence. J. Epidemiol. 2021, 31, 426–450. [Google Scholar] [CrossRef]
- Pilatz, A.; Dimitropoulos, K.; Veeratterapillay, R.; Yuan, Y.; Omar, M.I.; MacLennan, S.; Cai, T.; Bruyère, F.; Bartoletti, R.; Köves, B.; et al. Antibiotic Prophylaxis for the Prevention of Infectious Complications following Prostate Biopsy: A Systematic Review and Meta-Analysis. J. Urol. 2020, 204, 224–230. [Google Scholar] [CrossRef]
- Pradere, B.; Veeratterapillay, R.; Dimitropoulos, K.; Yuan, Y.; Omar, M.I.; MacLennan, S.; Cai, T.; Bruyère, F.; Bartoletti, R.; Köves, B.; et al. Nonantibiotic Strategies for the Prevention of Infectious Complications following Prostate Biopsy: A Systematic Review and Meta-Analysis. J. Urol. 2021, 205, 653–663. [Google Scholar] [CrossRef]
- Ishikawa, K.; Matsumoto, T.; Yasuda, M.; Hattori, R.; Uehara, S.; Muratani, T.; Yagisawa, M.; Sato, J.; Niki, Y.; Totsuka, K.; et al. The nationwide study of bacterial pathogens associated with urinary tract infections conducted by the Japanese Society of Chemotherapy. J. Infect. Chemother. 2011, 17, 126–138. [Google Scholar] [CrossRef] [Green Version]
- Carignan, A.; Roussy, J.F.; Lapointe, V.; Valiquette, L.; Sabbagh, R.; Pépin, J. Increasing risk of infectious complications after transrectal ultrasound-guided prostate biopsies: Time to reassess antimicrobial prophylaxis? Eur. Urol. 2012, 62, 453–459. [Google Scholar] [CrossRef]
- Pilatz, A.; Veeratterapillay, R.; Dimitropoulos, K.; Omar, M.I.; Pradere, B.; Yuan, Y.; Cai, T.; Mezei, T.; Devlies, W.; Bruyère, F.; et al. European Association of Urology Position Paper on the Prevention of Infectious Complications Following Prostate Biopsy. Eur. Urol. 2021, 79, 11–15. [Google Scholar] [CrossRef]
- Lightner, D.J.; Wymer, K.; Sanchez, J.; Kavoussi, L. Best Practice Statement on Urologic Procedures and Antimicrobial Prophylaxis. J. Urol. 2020, 203, 351–356. [Google Scholar] [CrossRef] [Green Version]
- Togo, Y.; Yamamoto, S. Prevention of infectious complications after prostate biopsy procedure. Int. J. Urol. 2017, 24, 486–492. [Google Scholar] [CrossRef] [Green Version]
- Chung, H.S.; Hwang, E.C.; Yu, H.S.; Jung, S.I.; Lee, S.J.; Lim, D.H.; Cho, W.J.; Choe, H.S.; Park, S.W. Prevalence of fluoroquinolone-resistant rectal flora in patients undergoing transrectal ultrasound-guided prostate needle biopsy: A prospective multicenter study. Int. J. Urol. 2018, 25, 278–283. [Google Scholar] [CrossRef]
- Hiyama, Y.; Takahashi, S.; Uehara, T.; Ichihara, K.; Hashimoto, J.; Matsukawa, M.; Taguchi, K.; Kunishima, Y.; Hotta, H.; Yanase, M.; et al. Selective culture of Escherichia coli to prevent infective complications of transrectal ultrasound-guided prostate biopsy: Clinical efficacy and analysis of characteristics of quinolone-resistant Escherichia coli. Int. J. Urol. 2019, 26, 655–660. [Google Scholar] [CrossRef]
- Liss, M.A.; Taylor, S.; Batura, D.; Steensels, D.; Chayakulkeeree, M.; Soenens, C.; Rao, G.G.; Dash, A.; Park, S.; Patel, N.; et al. Fluoroquinolone Resistant Rectal Colonization Predicts Risk of Infectious Complications after Transrectal Prostate Biopsy. J. Urol. 2014, 192, 1673–1678. [Google Scholar] [CrossRef] [PubMed]
- Concepcion, R.S.; Schaeffer, E.M.; Shore, N.D. The Effect of Local Antibiogram-based Augmented Antibiotic Prophylaxis on Infection-related Complications Following Prostate Biopsy. Rev. Urol. 2019, 21, 93–101. [Google Scholar] [PubMed]
- Taylor, A.K.; Zembower, T.R.; Nadler, R.B.; Scheetz, M.H.; Cashy, J.P.; Bowen, D.; Murphy, A.B.; Dielubanza, E.; Schaeffer, A.J. Targeted Antimicrobial Prophylaxis Using Rectal Swab Cultures in Men Undergoing Transrectal Ultrasound Guided Prostate Biopsy is Associated with Reduced Incidence of Postoperative Infectious Complications and Cost of Care. J. Urol. 2012, 187, 1275–1279. [Google Scholar] [CrossRef] [PubMed]
- Tops, S.C.; Kolwijck, E.; Koldewijn, E.L.; Somford, D.M.; Delaere, F.J.; van Leeuwen, M.A.; Breeuwsma, A.J.; de Vocht, T.F.; Broos, H.J.; Schipper, R.A.; et al. Cost Effectiveness of Rectal Culture-based Antibiotic Prophylaxis in Transrectal Prostate Biopsy: The Results from a Randomized, Nonblinded, Multicenter Trial. Eur. Urol. Open Sci. 2023, 50, 70–77. [Google Scholar] [CrossRef]
- Tops, S.C.; Kolwijck, E.; Koldewijn, E.L.; Somford, D.M.; Delaere, F.J.; van Leeuwen, M.A.; Breeuwsma, A.J.; de Vocht, T.F.; Broos, H.J.; Schipper, R.A.; et al. Rectal Culture-Based Versus Empirical Antibiotic Prophylaxis to Prevent Infectious Complications in Men Undergoing Transrectal Prostate Biopsy: A Randomized, Nonblinded Multicenter Trial. Clin. Infect. Dis. 2023, 76, 1188–1196. [Google Scholar] [CrossRef]
- Scott, S.; Harris, P.N.; Williamson, D.A.; Liss, M.A.; Doi, S.A.R.; Roberts, M.J. The effectiveness of targeted relative to empiric prophylaxis on infectious complications after transrectal ultrasound-guided prostate biopsy: A meta-analysis. World J. Urol. 2018, 36, 1007–1017. [Google Scholar] [CrossRef]
- Özden, E.; Bostanci, Y.; Yakupoglu, K.Y.; Akdeniz, E.; Yılmaz, A.F.; Tulek, N.; Sarıkaya, S. Incidence of Acute Prostatitis Caused by Extended-spectrum β-Lactamase-producing Escherichia coli after Transrectal Prostate Biopsy. Urology 2009, 74, 119–123. [Google Scholar] [CrossRef]
- Kanda, Y. Investigation of the freely available easy-to-use software ‘EZR’ for medical statistics. Bone Marrow Transpl. 2013, 48, 452–458. [Google Scholar] [CrossRef] [Green Version]
- Sadahira, T.; Wada, K.; Araki, M.; Ishii, A.; Watanabe, T.; Nasu, Y.; Tsugawa, M.; Takenaka, T.; Nasu, Y.; Kumon, H. Impact of selective media for detecting fluoroquinolone-insusceptible/extended-spectrum beta-lactamase-producing Escherichia coli before transrectal prostate biopsy. Int. J. Urol. 2017, 24, 842–847. [Google Scholar] [CrossRef] [Green Version]
- Sieczkowski, M.; Gibas, A.; Bronk, M.; Matuszewski, M. Fluoroquinolone-based antimicrobial prophylaxis in patients undergoing transrectal ultrasound-guided prostate biopsy. Eur. J. Clin. Microbiol. Infect. Dis. 2015, 34, 1815–1821. [Google Scholar] [CrossRef] [Green Version]
- Tsu, J.H.-L.; Ma, W.-K.; Chan, W.K.-W.; Lam, B.H.-S.; To, K.-C.; To, W.-K.; Ng, T.-K.; Liu, P.-L.; Cheung, F.-K.; Yiu, M.-K. Prevalence and Predictive Factors of Harboring Fluoroquinolone-resistant and Extended-spectrum β-Lactamase–producing Rectal Flora in Hong Kong Chinese Men Undergoing Transrectal Ultrasound-guided Prostate Biopsy. Urology 2015, 85, 15–22. [Google Scholar] [CrossRef] [PubMed]
- Nys, S.; Okeke, I.; Kariuki, S.; Dinant, G.J.; Driessen, C.; Stobberingh, E.E. Antibiotic resistance of faecal Escherichia coli from healthy volunteers from eight developing countries. J. Antimicrob. Chemother. 2004, 54, 952–955. [Google Scholar] [CrossRef] [PubMed]
- Togo, Y.; Kubo, T.; Taoka, R.; Hiyama, Y.; Uehara, T.; Hashimoto, J.; Kurimura, Y.; Takahashi, S.; Tsukamoto, T.; Miyazaki, J.; et al. Occurrence of infection following prostate biopsy procedures in Japan. J. Infect. Chemother. 2014, 20, 232–237. [Google Scholar] [CrossRef] [PubMed]
- Roberts, M.J.; Williamson, D.A.; Hadway, P.; Doi, S.A.; Gardiner, R.A.; Paterson, D.L. Baseline prevalence of antimicrobial resistance and subsequent infection following prostate biopsy using empirical or altered prophylaxis: A bias-adjusted meta-analysis. Int. J. Antimicrob. Agents 2014, 43, 301–309. [Google Scholar] [CrossRef]
- Batura, D.; Rao, G.G.; Nielsen, P.B. Prevalence of antimicrobial resistance in intestinal flora of patients undergoing prostatic biopsy: Implications for prophylaxis and treatment of infections after biopsy. BJU Int. 2010, 106, 1017–1020. [Google Scholar] [CrossRef]
- Zowawi, H.M.; Harris, P.N.; Roberts, M.J.; Tambyah, P.A.; Schembri, M.A.; Pezzani, M.D.; Williamson, D.A.; Paterson, D.L. The emerging threat of multidrug-resistant Gram-negative bacteria in urology. Nat. Rev. Urol. 2015, 12, 570–584. [Google Scholar] [CrossRef]
- Tan, W.P.; Papagiannopoulos, D.; Latchamsetty, K.C.; Wilson, N.; O’block, N.; Raff, L.; Lora, A.M.; Coogan, C.L.; Abern, M.R. Predictors of fluoroquinolone-resistant bacteria in the rectal vault of men undergoing prostate biopsy. Prostate Cancer Prostatic Dis. 2019, 22, 268–275. [Google Scholar] [CrossRef]
- Steensels, D.; Slabbaert, K.; De Wever, L.; Vermeersch, P.; Van Poppel, H.; Verhaegen, J. Fluoroquinolone-resistant E. coli in intestinal flora of patients undergoing transrectal ultrasound-guided prostate biopsy-should we reassess our practices for antibiotic prophylaxis? Clin. Microbiol. Infect. 2012, 18, 575–581. [Google Scholar] [CrossRef] [Green Version]
- Kamei, J.; Yagihara, Y.; Kume, H.; Horiuchi, T.; Sato, T.; Nakagawa, T.; Fujimura, T.; Fukuhara, H.; Moriya, K.; Homma, Y. Prevalence and characteristics of fecal antimicrobial-resistant Escherichia coli in a cohort of Japanese men undergoing prostate biopsy. Int. J. Urol. 2017, 24, 295–300. [Google Scholar] [CrossRef] [Green Version]
- Williamson, D.A.; Barrett, L.K.; Rogers, B.A.; Freeman, J.T.; Hadway, P.; Paterson, D.L. Infectious Complications Following Transrectal Ultrasound-Guided Prostate Biopsy: New Challenges in the Era of Multidrug-Resistant Escherichia coli. Clin. Infect. Dis. 2013, 57, 267–274. [Google Scholar] [CrossRef] [Green Version]
- Miyazaki, M.; Yamada, Y.; Matsuo, K.; Komiya, Y.; Uchiyama, M.; Nagata, N.; Takata, T.; Jimi, S.; Imakyure, O. Change in the Antimicrobial Resistance Profile of Extended-Spectrum β-Lactamase-Producing Escherichia coli. J. Clin. Med. Res. 2019, 11, 635–641. [Google Scholar] [CrossRef] [Green Version]
- Yamaguchi, K.; Ishii, Y.; Iwata, M.; Watanabe, N.; Shinagawa, M.; Yasujima, M.; Suwabe, A.; Kuroda, M.; Kaku, M.; Kitagawa, M.; et al. Nationwide surveillance of parenteral antibiotics containing meropenem activities against clinically isolated strains in 2009. Jpn. J. Antibiot. 2011, 64, 53–95. [Google Scholar] [PubMed]
- Yamaguchi, K.; Ishii, Y.; Tateda, K.; Iwata, M.; Watanabe, N.; Shinagawa, M.; Kayaba, H.; Kimura, M.; Suwabe, A.; Kaku, M.; et al. Nationwide surveillance of parenteral antibiotics containing meropenem activities against clinically isolated strains in 2012. Jpn. J. Antibiot. 2014, 67, 73–107. [Google Scholar] [PubMed]
- Namikawa, H.; Yamada, K.; Fujimoto, H.; Oinuma, K.-I.; Tochino, Y.; Takemoto, Y.; Kaneko, Y.; Shuto, T.; Kakeya, H. Clinical Characteristics of Bacteremia Caused by Extended-spectrum Beta-lactamase-producing Escherichia coli at a Tertiary Hospital. Intern. Med. 2017, 56, 1807–1815. [Google Scholar] [CrossRef] [Green Version]
- Nasu, Y.; Sako, S.; Yano, T.; Kosaka, N. Surveillance of Antimicrobial Resistant Escherichia coli by Rectal Swab Method—Annual Change of Prevalence of Quinolone-resistant and ESBL Producing Strains from 2009 to 2013. J. Jpn. Assoc. Infect. Dis. 2015, 89, 583–587. [Google Scholar] [CrossRef] [Green Version]
- Shigemura, K.; Tanaka, K.; Yamamichi, F.; Arakawa, S.; Fujisawa, M. Prophylactic efficacy of cephamycin plus fluoroquinolones in high risk patients on inhibiting infectious complications after transrectal prostate biopsy. J. Chemother. 2016, 28, 513–516. [Google Scholar] [CrossRef]
- Kakehi, Y.; Naito, S. Japanese Urological Association Complication rates of ultrasound-guided prostate biopsy: A nation-wide survey in Japan. Int. J. Urol. 2008, 15, 319–321. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, S.; Shigemura, K.; Kiyota, H.; Wada, K.; Hayami, H.; Yasuda, M.; Takahashi, S.; Ishikawa, K.; Hamasuna, R.; Arakawa, S.; et al. Essential Japanese guidelines for the prevention of perioperative infections in the urological field: 2015 edition. Int. J. Urol. 2016, 23, 814–824. [Google Scholar] [CrossRef] [Green Version]
- Lin, R.D.; Chin, Y.P.; Lee, M.H. Antimicrobial activity of antibiotics in combination with natural flavonoids against clinical extended-spectrum beta-lactamase (ESBL)-producing Klebsiella pneumoniae. Phytother. Res. 2005, 19, 612–617. [Google Scholar] [CrossRef]
- Liss, M.A.; Nakamura, K.K.; Meuleners, R.; Kolla, S.B.; Dash, A.; Peterson, E.M. Screening Rectal Culture to Identify Fluoroquinolone-resistant Organisms Before Transrectal Prostate Biopsy: Do the Culture Results between Office Visit and Biopsy Correlate? Urology 2013, 82, 67–73. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| All (n = 723) | FQ-Resistant Bacteria | p Value | ||
|---|---|---|---|---|
| Yes (n = 289) | No (n = 434) | |||
| Median age | 69 ± 8.1 | 69 ± 7.6 | 68 ± 8.4 | p = 0.116 *1 |
| Median BMI | 23.7 ± 3.0 | 23.7 ± 3.3 | 23.6 ± 2.8 | p = 0.961 *1 |
| PSA (ng/dL) | 7.8 ± 630.0 | 7.8 ± 814.8 | 7.9 ± 469.2 | p = 0.777 *1 |
| Prostate volume (mL) | 30.9 ± 25.6 | 29.9 ± 24.2 | 39.8± 24.8 | p < 0.001 *1 |
| History of prostate biopsy | 166 (23.0 %) | 67 (23.2 %) | 99 (22.8 %) | p = 0.907 *2 |
| Diabetes mellitus | 112 (15.5 %) | 39 (13.5 %) | 73 (16.8 %) | p = 0.226 *2 |
| Use of antimicrobial within the last 1 year | 155 (26.8 %) | 65 (28.4 %) | 90 (25.8 %) | p = 0.491 *2 |
| Case | Age | BMI | PSA | Prostate Volume | History of Prostate Biopsy | Use of Antimicrobial within the Last 1 Year | Diabetes Mellitus | FQ-Resistant Bacteria | Blood Culture | Antimicrobial | Remarks |
|---|---|---|---|---|---|---|---|---|---|---|---|
| (ng/mL) | (mL) | ||||||||||
| 1 | 69 | 25.5 | 20.63 | 112.2 | No | No | No | No | negative | CMZ | |
| 2 | 61 | 25.8 | 3.42 | 38 | No | Yes | Yes | Yes | Escherichia coli | DRPM | |
| (Drug unknown) | (FQ-resistant) | ||||||||||
| 3 | 50 | 25.1 | 5.46 | 11.9 | No | Yes | No | Yes | negative | MEPM | Suspicious of diverticulitis |
| (Drug unknown) | |||||||||||
| 4 | 76 | 23.6 | 17.4 | 45 | Yes | Unknown | Yes | No | negative | MEPM | |
| 5 | 57 | 24.7 | 4.47 | 45 | No | Yes (CAM) | No | No | negative | MEPM → VCM → CTRX | Fever after 15 days |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Higashi, S.; Yoshio, Y.; Kanda, H.; Nishikawa, T.; Kato, M.; Sugino, Y.; Sasaki, T.; Kato, M.; Masui, S.; Nishikawa, K.; et al. Targeted Antimicrobial Prophylaxis with Cefmetazole Based on Presence of Fluoroquinolone-Resistant Isolates to Prevent Post-Prostate Biopsy Infectious Complications. Uro 2023, 3, 168-176. https://doi.org/10.3390/uro3020018
Higashi S, Yoshio Y, Kanda H, Nishikawa T, Kato M, Sugino Y, Sasaki T, Kato M, Masui S, Nishikawa K, et al. Targeted Antimicrobial Prophylaxis with Cefmetazole Based on Presence of Fluoroquinolone-Resistant Isolates to Prevent Post-Prostate Biopsy Infectious Complications. Uro. 2023; 3(2):168-176. https://doi.org/10.3390/uro3020018
Chicago/Turabian StyleHigashi, Shinichiro, Yuko Yoshio, Hideki Kanda, Taketomo Nishikawa, Momoko Kato, Yusuke Sugino, Takeshi Sasaki, Manabu Kato, Satoru Masui, Kouhei Nishikawa, and et al. 2023. "Targeted Antimicrobial Prophylaxis with Cefmetazole Based on Presence of Fluoroquinolone-Resistant Isolates to Prevent Post-Prostate Biopsy Infectious Complications" Uro 3, no. 2: 168-176. https://doi.org/10.3390/uro3020018