
Evaluation Methods of Detrusor Sphincter Dyssynergia in Spinal Cord Injury Patients: A Literature Review

{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
- (a)
- (b)
- In contrast with the above definition [2] that considers DSD as being striated urethral sphincter overactivity during voiding, detrusor–internal sphincter dyssynergia or bladder neck dyssynergia (BND) is a failure of the smooth muscle of the bladder neck and proximal urethra to relax during detrusor contraction in the voiding phase [4,6]. BND might have implications in the evaluation and management methods of DSD [7];
- (c)
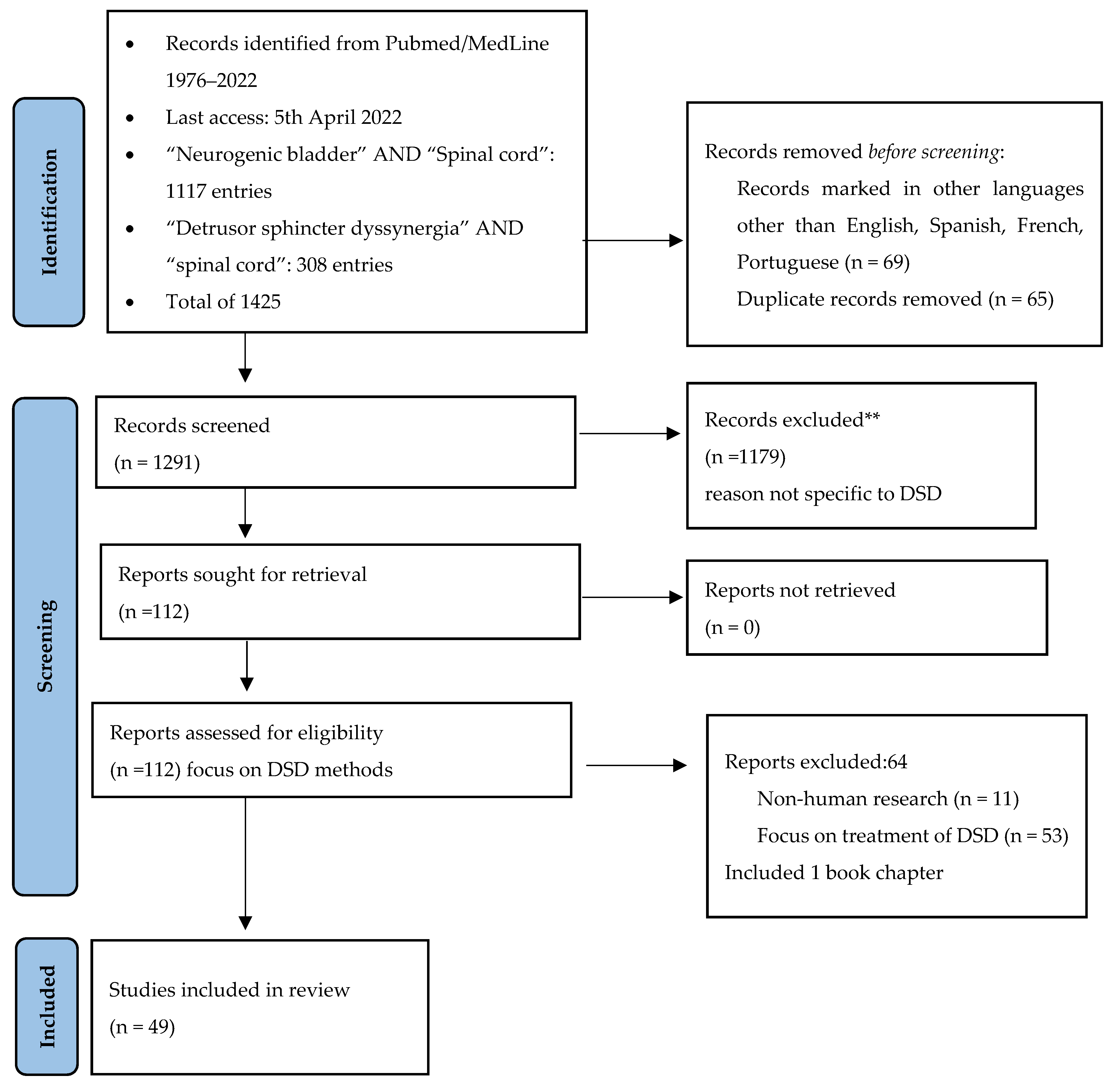
2. Methods
3. Results and Discussion
3.1. Urodynamics Evaluation of DSD in SCI Patients
3.1.1. Filling Cystometry/Pressure-Flow Study/Urethral Pressure
Indirect Assessment of EUS Activity
Voiding Cystourethrography (VCUG) and EUS EMG
EUS Pressure Measurement
3.1.2. DSD and BND
3.1.3. Ultrasound and Urodynamics
3.1.4. Uroflowmetry, Post Void Residual Volume (PVR) and Bladder Diary
3.2. Other Clinical Dimension in Evaluation of DSD in SCI Patients
3.2.1. Anamnesis
3.2.2. Physical Exam
3.2.3. Complementary Diagnostic and Follow-Up
- renal function:
- ○
- routine: plasma concentration of electrolytes, urea, creatinine (or cystatin C), 24 h creatinine clearance.
- ○
- optional or with special indication: kidney scintigraphy.
- upper and lower urinary tract structural changes:
- ○
- routine: upper and lower tract transabdominal ultrasound examination with morphometric measures and PVR estimation, screening for lithiasis, bladder trabeculation, and diverticula.
- ○
- optional or with special indication: VCUG, urethro-cystoscopy, transrectal ultrasound for prostate assessment, long term screening of neoplasms.
- screening for lower urinary tract bacterial colonization. Asymptomatic bacteriuria in these population should not be treated with antibiotics.
3.2.4. Autonomic Dysreflexia and DSD
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| BND | Bladder Neck Dyssynergia |
| DSD | Detrusor External Sphincter Dyssynergia |
| EMG | Electromyography |
| EUS | External Urethral Sphincter |
| ICS | International Continence Society |
| PVR | Post Void Residual Volume |
| SCI | Spinal Cord Injury |
| VCUG | Voiding cystourethrography |
References
- Abrams, P.; Cardozo, L.; Fall, M.; Griffiths, D.; Rosier, P.; Ulmsten, U.; Van Kerrebroeck, P.; Victor, A.; Wein, A.; Standardisation Sub-committee of the International Continence Society. The standardisation of terminology of lower urinary tract function: Report from the standardisation sub-committee of the International Continence Society. Neurourol. Urodyn. 2002, 21, 167–178. [Google Scholar] [CrossRef] [PubMed]
- D’Ancona, C.; Haylen, B.; Oelke, M.; Abranches-Monteiro, L.; Arnold, E.; Goldman, H.; Hamid, R.; Homma, Y.; Marcelissen, T.; Rademakers, K.; et al. The International Continence Society (ICS) report on the terminology for adult male lower urinary tract and pelvic floor symptoms and dysfunction. Neurourol. Urodyn. 2019, 38, 433–477. [Google Scholar] [CrossRef] [PubMed]
- Siroky, M.B.; Krane, R.J. Neurologic Aspects of Detrusor-sphincter Dyssynergia, with Reference to the Guarding Reflex. J. Urol. 1982, 127, 953–957. [Google Scholar] [CrossRef] [PubMed]
- Stoffel, J.T. Detrusor sphincter dyssynergia: A review of physiology, diagnosis, and treatment strategies. Transl. Androl. Urol. 2016, 5, 127–135. [Google Scholar] [CrossRef] [PubMed]
- Blaivas, J.G.; Sinha, H.P.; Zayed, A.A.; Labib, K.B. Detrusor-external Sphincter Dyssynergia: A Detailed Electromyographic Study. J. Urol. 1981, 125, 545–548. [Google Scholar] [CrossRef] [PubMed]
- Yalla, S.V.; Blunt, K.J.; Fam, B.A.; Constantinople, N.L.; Gutes, R.F. Detrusor-Urethral Sphincter Dyssynergia. J. Urol. 1977, 118, 1026–1029. [Google Scholar] [CrossRef]
- Schurch, B.; Yasuda, K.; Rossier, A.B. Detrusor Bladder Neck Dyssynergia Revisited. J. Urol. 1994, 152 Pt 1, 2066–2070. [Google Scholar] [CrossRef]
- Amarenco, G.; Ismael, S.S.; Soler, J.M. The dyssynergic sphincter. In Textbook of the Neurogenic Bladder; Corcos, J., Ginsberg, D., Karsenty, G., Eds.; CRC Press: Boca Raton, FL, USA, 2016; pp. 133–137. [Google Scholar]
- Gross, O.; Leitner, L.; Rasenack, M.; Schubert, M.; Kessler, T.M. Detrusor sphincter dyssynergia: Can a more specific definition distinguish between patients with and without an underlying neurological disorder? Spinal Cord 2021, 59, 1026–1033. [Google Scholar] [CrossRef]
- Wang, Z.; Deng, H.; Li, X.; Liao, L. The Video-Urodynamic and Electrophysiological Characteristics in Patients with Traumatic Spinal Cord Injury. Int. Neurourol. J. 2021, 25, 327–336. [Google Scholar] [CrossRef]
- Ku, J.H.; Choi, W.J.; Lee, K.Y.; Jung, T.Y.; Lee, J.K.; Park, W.H.; Shim, H.B. Complications of the upper urinary tract in patients with spinal cord injury: A long-term follow-up study. Urol. Res. 2005, 33, 435–439. [Google Scholar] [CrossRef]
- Gao, Y.; Danforth, T.; Ginsberg, D.A. Urologic Management and Complications in Spinal Cord Injury Patients: A 40- to 50-year Follow-up Study. Urology 2017, 104, 52–58. [Google Scholar] [CrossRef] [PubMed]
- Hackler, R.H. A 25-Year Prospective Mortality Study in the Spinal Cord Injured Patient: Comparison with the Long-Term Living Paraplegic. J. Urol. 1977, 117, 486–488. [Google Scholar] [CrossRef]
- Wu, C.Q.; Franco, I. Management of vesicoureteral reflux in neurogenic bladder. Investig. Clin. Urol. 2017, 58 (Suppl. 1), S54–S58. [Google Scholar] [CrossRef] [PubMed]
- Perkash, I. Autonomic dysreflexia and detrusor-sphincter dyssynergia in spinal cord injury patients. J. Spinal Cord Med. 1997, 20, 365–370. [Google Scholar]
- World Health Organization. International Classification of Functioning, Disability, and Health: ICF; World Health Organization: Geneva, Switzerland, 2001. [Google Scholar]
- Roy, H.A.; Nettleton, J.; Blain, C.; Dalton, C.; Farhan, B.; Fernandes, A.; Georgopoulos, P.; Klepsch, S.; Lavelle, J.; Martinelli, E.; et al. Assessment of patients with lower urinary tract symptoms where an undiagnosed neurological disease is suspected: A report from an International Continence Society consensus working group. Neurourol. Urodyn. 2020, 39, 2535–2543. [Google Scholar] [CrossRef]
- Ahmed, H.U.; Shergill, I.S.; Arya, M.; Shah, P.J.R. Management of detrusor–external sphincter dyssynergia. Nat. Clin. Pract. Urol. 2006, 3, 368–380. [Google Scholar] [CrossRef]
- Sekido, N.; Igawa, Y.; Kakizaki, H.; Kitta, T.; Sengoku, A.; Takahashi, S.; Takahashi, R.; Tanaka, K.; Namima, T.; Honda, M.; et al. Clinical guidelines for the diagnosis and treatment of lower urinary tract dysfunction in patients with spinal cord injury. Int. J. Urol. 2020, 27, 276–288. [Google Scholar] [CrossRef]
- Rosier, P.F.; Schaefer, W.; Lose, G.; Goldman, H.B.; Guralnick, M.; Eustice, S.; Dickinson, T.; Hashim, H. International Continence Society Good Urodynamic Practices and Terms 2016: Urodynamics, uroflowmetry, cystometry, and pressure-flow study. Neurourol. Urodyn. 2016, 36, 1243–1260. [Google Scholar] [CrossRef]
- Schäfer, W.; Abrams, P.; Liao, L.; Mattiasson, A.; Pesce, F.; Spangberg, A.; Sterling, A.M.; Zinner, N.R.; van Kerrebroeck, P.; International Continence Society. Good urodynamic practices: Uroflowmetry, filling cystometry, and pressure-flow studies. Neurourol. Urodyn. 2002, 21, 261–274. [Google Scholar] [CrossRef]
- Chamorro, M.V.; Casado, J.S.; Zurbano, J.M.A.; del Pino, F.T.; Alba, D.V. Evidence-based medicine. Usefulness of isolated cystomanometry for the diagnosis of periurethral detrusor-sphincter dyssynergia in patients with suprasacral lesion. Arch. Esp. Urol. 1999, 52, 1073–1078. (In Spanish) [Google Scholar]
- Geirsson, G.; Fall, M. The Ice-Water Test in the Diagnosis of Detrusor-External Sphincter Dyssynergia. Scand. J. Urol. Nephrol. 1995, 29, 457–461. [Google Scholar] [CrossRef] [PubMed]
- Chancellor, M.B.; Kaplan, S.A.; Blaivas, J.G. Detrusor-external sphincter dyssynergia. Ciba Found. Symp. 1990, 151, 195–206. [Google Scholar]
- De, E.J.; Patel, C.Y.; Tharian, B.; Westney, O.L.; Graves, D.E.; Hairston, J.C. Diagnostic discordance of electromyography (EMG) versus voiding cystourethrogram (VCUG) for detrusor-external sphincter dyssynergy (DESD). Neurourol. Urodyn. 2005, 24, 616–621. [Google Scholar] [CrossRef] [PubMed]
- Miller, B.D.; Tallman, C.T.; Boone, T.B.; Khavari, R. Low Interrater Reliability of Videourodynamic Diagnosis of Detrusor External Sphincter Dyssynergia. Female Pelvic Med. Reconstr. Surg. 2021, 27, 297–299. [Google Scholar] [CrossRef] [PubMed]
- Spettel, S.; Kalorin, C.; De, E. Combined Diagnostic Modalities Improve Detection of Detrusor External Sphincter Dyssynergia. ISRN Obstet. Gynecol. 2011, 2011, 323421. [Google Scholar] [CrossRef] [Green Version]
- Lose, G.; Griffiths, D.; Hosker, G.; Kulseng-Hanssen, S.; Perucchini, D.; Schäfer, W.; Thind, P.; Versi, E.; Standardization Sub-Committee; International Continence Society. Standardisation of urethral pressure measurement: Report from the standardisation sub-committee of the International Continence Society. Neurourol. Urodyn. 2002, 21, 258–260. [Google Scholar] [CrossRef]
- Dykstra, D.D.; Sidi, A.A.; Scott, A.B.; Pagel, J.M.; Goldish, G.D. Effects of Botulinum a Toxin on Detrusor-Sphincter Dyssynergia in Spinal Cord Injury Patients. J. Urol. 1988, 139, 919–922. [Google Scholar] [CrossRef]
- Bary, P.R.; Day, G.; Lewis, P.; Chawla, J.; Evans, C.; Stephenson, T.P. Dynamic Urethral Function in the Assessment of Spinal Injury Patients. Br. J. Urol. 1982, 54, 39–44. [Google Scholar] [CrossRef]
- Bellucci, C.; Wöllner, J.; Gregorini, F.; Birnböck, D.; Kozomara, M.; Mehnert, U.; Kessler, T.M. External Urethral Sphincter Pressure Measurement: An Accurate Method for the Diagnosis of Detrusor External Sphincter Dyssynergia? PLoS ONE 2012, 7, e37996. [Google Scholar] [CrossRef] [Green Version]
- Corona, L.E.; Cameron, A.P.; Clemens, J.Q.; Qin, Y.; Stoffel, J.T. Urethral Pressure Measurement as a Tool for the Urodynamic Diagnosis of Detrusor Sphincter Dyssynergia. Int. Neurourol. J. 2018, 22, 268–274. [Google Scholar] [CrossRef]
- Soler, J.M.; Previnaire, J.G.; Hadiji, N. Predictors of outcome for urethral injection of botulinum toxin to treat detrusor sphincter dyssynergia in men with spinal cord injury. Spinal Cord 2016, 54, 452–456. [Google Scholar] [CrossRef]
- Perkash, I. Physical medicine and rehabilitation: Sonographic urodynamics. West. J. Med. 1986, 144, 736. [Google Scholar] [PubMed]
- Perkash, I.; Friedland, G.W. Catheter-induced hyperreflexia in spinal cord injury patients: Diagnosis by sonographic voiding cystourethrography. Radiology 1986, 159, 453–455. [Google Scholar] [CrossRef] [PubMed]
- Shapeero, L.; Friedland, G.; Perkash, I. Transrectal sonographic voiding cystourethrography: Studies in neuromuscular bladder dysfunction. Am. J. Roentgenol. 1983, 141, 83–90. [Google Scholar] [CrossRef] [PubMed]
- Shabsigh, R.; Fishman, I.; Krebs, M. Combined Transrectal Ultrasonography and Urodynamics in the Evaluation of Detrusor-sphincter Dyssynergia. Br. J. Urol. 1988, 62, 326–330. [Google Scholar] [CrossRef] [PubMed]
- Ntoulia, A.; Pascual, E.A.; Back, S.J.; Bellah, R.D.; Salazar, V.P.B.; Chan, P.K.J.; Chow, J.S.; Robinot, D.C.; Darge, K.; Duran, C.; et al. Contrast-enhanced voiding urosonography, part 1: Vesicoureteral reflux evaluation. Pediatr. Radiol. 2021, 51, 2351–2367. [Google Scholar] [CrossRef] [PubMed]
- Barnewolt, C.E.; Acharya, P.T.; Pascual, E.A.; Back, S.J.; Salazar, V.P.B.; Chan, P.K.J.; Chow, J.S.; Robinot, D.C.; Darge, K.; Duran, C.; et al. Contrast-enhanced voiding urosonography part 2: Urethral imaging. Pediatr. Radiol. 2021, 51, 2368–2386. [Google Scholar] [CrossRef]
- Amarenco, G.; Ismaël, S.S.; Chesnel, C.; Charlanes, A.; Breton, F.L.E. Diagnosis and clinical evaluation of neurogenic bladder. Eur. J. Phys. Rehabil. Med. 2017, 53, 975–980. [Google Scholar] [CrossRef]
- Chen, C.-Y.; Liao, C.-H.; Kuo, H.-C. Therapeutic effects of detrusor botulinum toxin A injection on neurogenic detrusor overactivity in patients with different levels of spinal cord injury and types of detrusor sphincter dyssynergia. Spinal Cord 2011, 49, 659–664. [Google Scholar] [CrossRef]
- Habchi, H.; Galaup, J.-P.; Morel-Journel, N.; Ruffion, A. Toxine botulique A et dyssynergie vésico-sphinctérienne: Étude rétrospective portant sur 47 patients. Prog. Urol. 2014, 24, 234–239. (In French) [Google Scholar] [CrossRef]
- Drake, M.J.; Apostolidis, A.; Cocci, A.; Emmanuel, A.; Gajewski, J.B.J.B.; Harrison, S.C.W.S.C.; Heesakkers, J.P.F.J.P.; Lemack, G.G.E.; Madersbacher, H.; Panicker, J.N.J.N.; et al. Neurogenic lower urinary tract dysfunction: Clinical management recommendations of the Neurologic Incontinence committee of the fifth International Consultation on Incontinence 2013. Neurourol. Urodyn. 2016, 35, 657–665. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stewart, C.; Gallacher, K.; Nakham, A.; Cruickshank, M.; Newlands, R.; Bond, C.; Myint, P.K.; Bhattacharya, D.; Mair, F.S. Barriers and facilitators to reducing anticholinergic burden: A qualitative systematic review. Int. J. Clin. Pharm. 2021, 43, 1451–1460. [Google Scholar] [CrossRef] [PubMed]
- Amarenco, G.; Guinet, A.; Jousse, M.; Verollet, D.; Ismael, S.S. Pencil and Paper Test: A New Tool to Predict the Ability of Neurological Patients to Practice Clean Intermittent Self-Catheterization. J. Urol. 2011, 185, 578–582. [Google Scholar] [CrossRef] [PubMed]
- Mahfouz, W.; Corcos, J. Management of detrusor external sphincter dyssynergia in neurogenic bladder. Eur. J. Phys. Rehabil. Med. 2011, 47, 639–650. [Google Scholar] [PubMed]
- Kim, D.-I.; Tan, C.O. Alterations in autonomic cerebrovascular control after spinal cord injury. Auton. Neurosci. 2018, 209, 43–50. [Google Scholar] [CrossRef]
- Hou, S.; Rabchevsky, A.G. Autonomic Consequences of Spinal Cord Injury. Compr. Physiol. 2014, 4, 1419–1453. [Google Scholar] [CrossRef]
- Barton, C.H.; Khonsari, F.; Vaziri, N.D.; Byrne, C.; Gordon, S.; Friis, R. The Effect of Modified Transurethral Sphincterotomy on Autonomic Dysreflexia. J. Urol. 1986, 135, 83–85. [Google Scholar] [CrossRef]



Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pereira, J.A.; Debugne, T. Evaluation Methods of Detrusor Sphincter Dyssynergia in Spinal Cord Injury Patients: A Literature Review. Uro 2022, 2, 122-133. https://doi.org/10.3390/uro2020015
Pereira JA, Debugne T. Evaluation Methods of Detrusor Sphincter Dyssynergia in Spinal Cord Injury Patients: A Literature Review. Uro. 2022; 2(2):122-133. https://doi.org/10.3390/uro2020015
Chicago/Turabian StylePereira, José Alexandre, and Thierry Debugne. 2022. "Evaluation Methods of Detrusor Sphincter Dyssynergia in Spinal Cord Injury Patients: A Literature Review" Uro 2, no. 2: 122-133. https://doi.org/10.3390/uro2020015