
Pull-Through Ureteroneocystostomy for Very Small En Bloc Kidney Transplants from Donors Weighing ≤ 5 kg


Department of Surgery, Division of Transplantation, Allegheny General Hospital, Pittsburgh, PA 15212, USA
Uro 2022, 2(2), 102-108; https://doi.org/10.3390/uro2020013
Submission received: 22 March 2022
/
Revised: 1 May 2022
/
Accepted: 7 May 2022
/
Published: 13 May 2022
(This article belongs to the Special Issue Current Concepts in Transplantation)
{kind=link}
{kind=link}
{kind=link}
Abstract
:Background: Urologic complications are the most dreaded complications of renal transplantation, particularly when pediatric en bloc kidneys (EBKs) are used. Current techniques of ureteroneocystostomy (UNC) are not applicable to the very small ureters of very small en bloc kidneys. We reviewed our experience with the pull-through ureteroneocystostomy in kidney transplantation from donors under or equal to 5 kg weight. Material and Methods: The technique was used in 32 EBKs. Complications and 4-year graft survival are discussed. Results: One single graft thrombosed and required nephrectomy. The remaining kidneys provided good renal function. Hematuria was transient in five patients and did not require fulguration. No leakage was experienced. Delayed graft function occurred in 16% of cases. No primary nonfunction was noted. During the follow-up period, hydronephrosis and/or pyelonephritis were not observed. The 4-year graft survival was 95% with serum creatinine levels averaging 0.9 mg/dl. Conclusions: The procedure proved to be safe and reproducible. It can be applied to the ureteral re-implantation of very small EBKs.
1. Introduction
Renal transplantation is the treatment of choice for patients with end-stage renal disease, as the 5-year survival rate of deceased donor transplants’ recipients is 75% as compared with 40% for patients staying on dialysis [1]. Because of the shortage of organs, the transplant community’s attention has turned toward the use of en bloc transplantation of infant donor kidneys. Our early experience with kidneys from donors under 15 kg showed that EBKs can be performed with low morbidities and provide excellent results [2]. The Lich–Gregoire technique of UNC through a single tunnel was used [2,3,4]. During the 10-year follow-up, these EBKs provide better graft survival and function than the living donor kidney because of the larger amount of nephrons transplanted [5]. We then embarked on taking smaller donor kidneys. Urinary complications, even reduced to the minimal occurrence because of experience, still remained the most dreadful complication following kidney transplantation [6]. Since the literature about the use of kidneys from donors weighing <5 kg is scarce [7,8], the technique of UNC is worth describing in detail since the use of smaller EBKs from donors weighing </=5 kg raises a special problem with regards to handling the very small ureters and re-implanting them. To lessen the damage caused by the surgical manipulation of tiny ureters, our recourse is an atraumatic pull-through UNC which is described herein. Since the study did not identify any patients and records, the study did not require any decision by the Institutional Review Board.
2. Material and Methods
The charts of 32 infant donors were reviewed. Donors were 0.25 +/− 0.01 year old and weighed 4.2 +/−0.9 kg. The kidneys had 20.2 +/−6.8 h of cold ischemia time. All organs were imported. During organ recovery, after cold perfusion was performed via a right iliac artery cannula, efforts were made to procure as much supra and infra renal aorta and vena cava as possible. The ureters were handled with minimal dissection and cut at their junctions with the bladder. The en bloc kidneys were packed in University of Wisconsin perfusate. At the back table and under 2.5 magnifying loupes, the proximal aorta was closed transversally using running 5-0 monofilament polypropylene sutures. The SMA stump, when present, was turned down to cap the cephalad aorta. The cephalad end of the vena cava was closed with 6-0 running sutures. No attempt was made to reconstruct the missing cuffs of the renal artery and the renal vein to avoid post operative thrombosis observed in our early experience [2].To avoid venous congestion due to inadequate venous outflow in case of stenosis of the distal vena cava, proximal cava drainage is indicated. To this effect, a spiral vein graft segment may be fashioned from a donor vessel or recipient saphenous vein to lengthen the proximal vena cava and allow its anastomosis to the iliac vein, as described previously [9]. All non-renal aorta and cava collaterals were suture ligated with 6-0 polypropylene. The hilar region was not dissected to avoid further vascular and ureteral injuries, and post-transplant torsion. The ureters were not dissected. When vascular injuries to the kidneys and the ureters were suspected, the donor aorta was flushed at low pressure with 10 cc of perfusate stained with 1/3 ampule of indigo carmine [10]. The use of methylene blue promoted by other authors is not advised because of the risk of methemoglobinuria. Failure to stain blue immediately of any part of the kidneys or ureters denoted the presence of ischemia and led to organ discard. Delayed staining occurred from diffusion of the dye and gave false information. The same observation holds true with the use of fluorescein which is more cumbersome since it requires the use of Wood lamp. The dye was flushed out immediately with 20 cc of fresh preservation perfusate. The adrenal glands were both dissected and tied together with 3-0 silk ties left long and held by a mosquito clamp to facilitate their orientation and their manipulation until the time of closure of the incision at which time the adrenals were removed. No pulsatile perfusion was used to shorten the cold ischemia time.
Recipients were selected for low panel reactive antibodies to avoid early rejection and tissue loss of the tiny allografts which measured only 2.5–3.5 cm cm in length and for their good cardiac reserve to tolerate a relative post operative arterial hypotension of 90–100 mm Hg to avoid hypertensive injuries to the very small kidneys and to allow them to grow. Induction consisted of a 5-day course of anti-thymocyte preparation (1–1.5 mg/kg body weight) in addition to tacrolimus and mycophenolate mofetil. Only 3 days of 250 mg of methylprednisolone were used. Immunosuppression was maintained with tacrolimus, mycophenolate, and small doses of prednisone for patients with PRA’s >30%. Only one dose of 5000 units of heparin was given intravenously just before vascular clamping. No antiplatelets medication was used prior to and after the transplant procedure. Clinical rejection episodes were treated with three to five days of 250 mg of methylprednisolone. Because of the small size of the graft, no renal biopsy was performed.
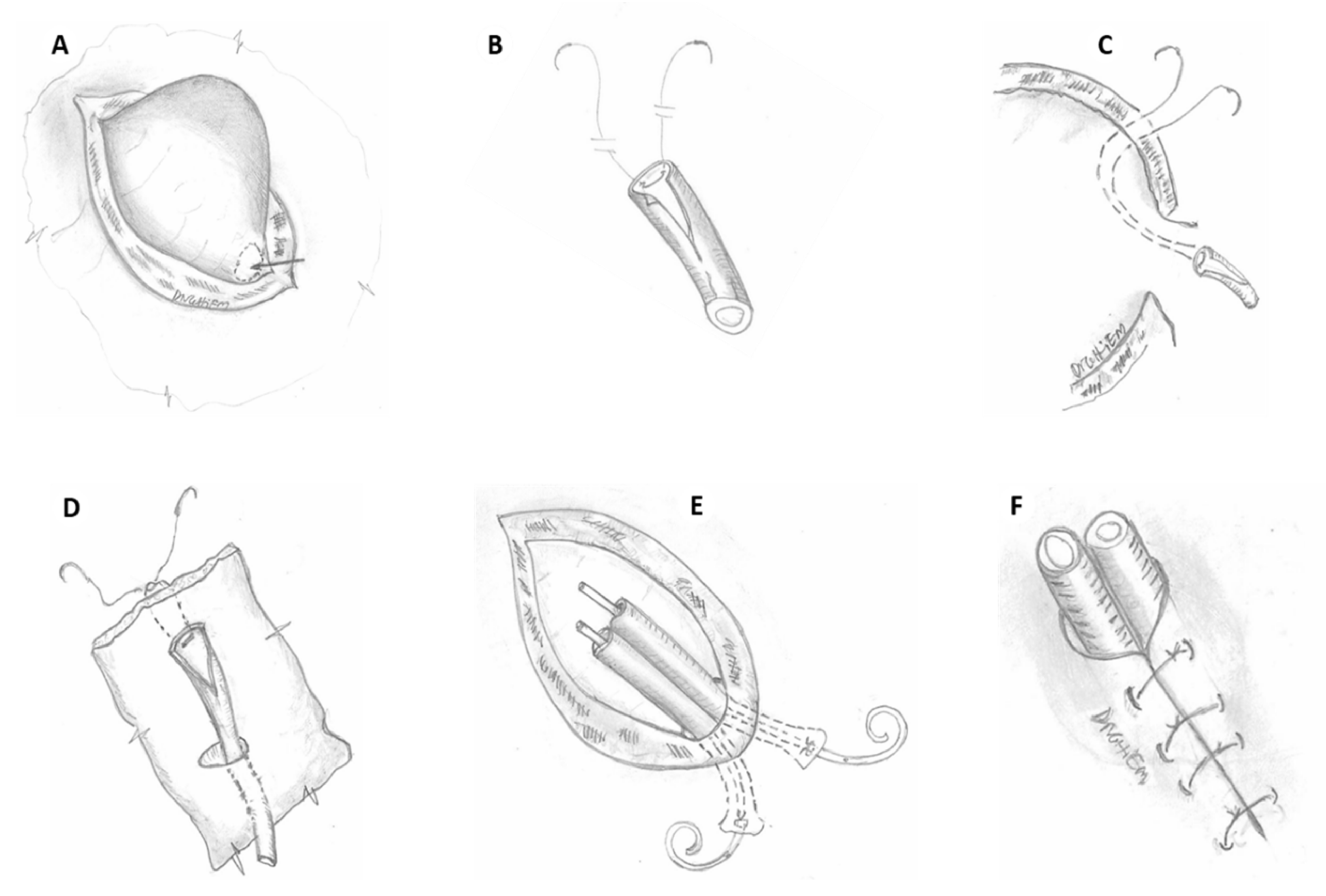
The bladder was lavaged with antibiotic solution (two grams of cephalosporin in one liter of normal saline stained with one ampule of indigo carmine, or 80 mg of gentamicin in the case of allergy to penicillin). The solution was administered at a pressure of 40 cm of water, via a Y connector attached to the Foley catheter. Two hundred and fifty cubic centimeters of irrigating solution was left in the bladder and the Foley catheter was clamped. The right iliac quadrant was preferred because the iliac vessels are more superficial and there is more room than the contralateral side. A regular transplant incision was made and the iliac vessels were dissected off their beds with the lymphatic vessels ligated. The EBKs were inverted 180 degrees to allow donor cava-recipient iliac venous concordance at the pelvic level and avoid donor cava/aorta crossing leading to venous thrombosis. When the left iliac quadrant was used, no anatomic switch was required since the anatomy of the donor cava-recipient iliac vein is concordant. The kidneys were positioned very low in the pelvis to allow the ureters to reach the bladder without tension. Revascularization was obtained with end to side anastomoses between the spatulated distal donor aorta and vena cava to the external iliac artery and vein, respectively, using fine polypropylene sutures. A small aortic punch was used to enlarge the iliac arteriotomy. A 1.5 cm long arteriotomy and venotomy is necessary in anticipation of a high blood flow required by the full grown kidneys. A 1.5–2 cm incision of the dome of the bladder was then performed and carried through the detrusor until the blueish mucosa was reached. The mucosa bulged out readily under the pressure of the irrigating solution (Figure 1A). The mucosa was dissected widely off the detrusor to make room for both ureters. All transverse detrusor bands were severed to avoid ureteral strangulation and stenosis within the tunnel. Hemostasis was carefully secured to mitigate an eventual hematoma. The ureteral tips were freshened up and hemostasis was carefully achieved using low current cauterization. First, the medial ureter was spatulated posteriorly by 1 cm. A full thickness horizontal mattress suture using a double arm 5-0 polydioxanone was placed from the mucosal side (Figure 1B). Then, both needles were brought into the bladder through a small transverse opening of the distal bladder mucosa pouch (Figure 1A, arrow), to exit 1 cm distal and medial to the detrusor myotomy on the dome of the bladder (Figure 1C). Then, a 3.8 F double J ureteral stent was inserted into the ureter, up to the pelvis of the medial kidney. The distal stent tip was inserted into the bladder through the mucosal hole. Care was taken to avoid entangling with the sutures. The use of a temporary soft tip guide wire may be helpful. The sutures were then pulled up, easing the medial ureter into the bladder. The U stitch was tied. Thus, the full thickness ureteral tip was anchored to the full thickness bladder wall (Figure 1D). These same steps were repeated with the lateral ureter which was brought through the same mucosal opening, aiming laterally on the bladder dome. The two knots were 1–1.2 cm apart on the dome of the bladder. The mucosal opening should fit the two ureters snugly (Figure 1E). It was useful to irrigate continuously the bladder to maintain the mucosal hole open at all times, allowing all operative manipulations to be performed without grasping and tearing the thin mucosal flap. Any brisk mucosal leak should be closed at that time. The detrusor was closed loosely over both ureters with interrupted 3-0 polydioxanone to bury the ureterovesical junction and the distal ureters and create the anti-reflux valve (Figure 1F). Then, the bladder was distended again under higher pressure, by elevating the bladder irrigation bag to test for leaks which were closed, generally with one additional stitch. The final aspect of the EBKs is depicted in Figure 2A. The incision was closed in layers over a Jackson Pratt drain kept for 3 days. This technique was applied to 32 EBKs. Pre-operative parenteral antibiotics used for 24 h were switched to oral sulfamethoxazole. Regardless of urine output, a technetium diethylene triamine penta-acetic scan was performed on Day 1, and every 6 months as indicated (Figure 2B). The Foley catheter was removed on Day 5. A bedside ultrasound examination was performed to assess complete bladder emptying before discharge, and repeated every six months as necessary. The patient was instructed to void every hour and as needed. At 6 weeks, the stents were removed by flexible cystoscopy during a clinic visit.
3. Results
Light hematuria was observed in five patients and cleared up spontaneously within 2 days. No endoscopic fulguration was required. One single medial kidney with arterial thrombosis required nephrectomy. At that time the medial ureteral anchoring U knot was simply cut and the ischemic ureter was pulled out of the tunnel. The detrusor was closed with a single stitch. It would be otherwise very demanding to dismantle the anastomosis had it been a side to side regular Lich–Gregoir ureteral anastomosis, and re-perform the ureteral re-implantation. The remaining single kidney maintained a serum creatinine level of 1.6 mg/dl at the end of one year. No urinary leakage and lymplocele was observed in the whole series. No ureteral stenosis was encountered. One patient maintained a very large urine output but did not come off dialysis. The biopsy at 5 months showed diffused glomerulosclerosis, resulting most likely from uncontrolled recipient’s hypertension. Delayed graft function occurred in 16% of cases. Primary non function was not observed. The 4-year graft survival was 95% and serum creatinine levels averaged 0.9 mg/dL.
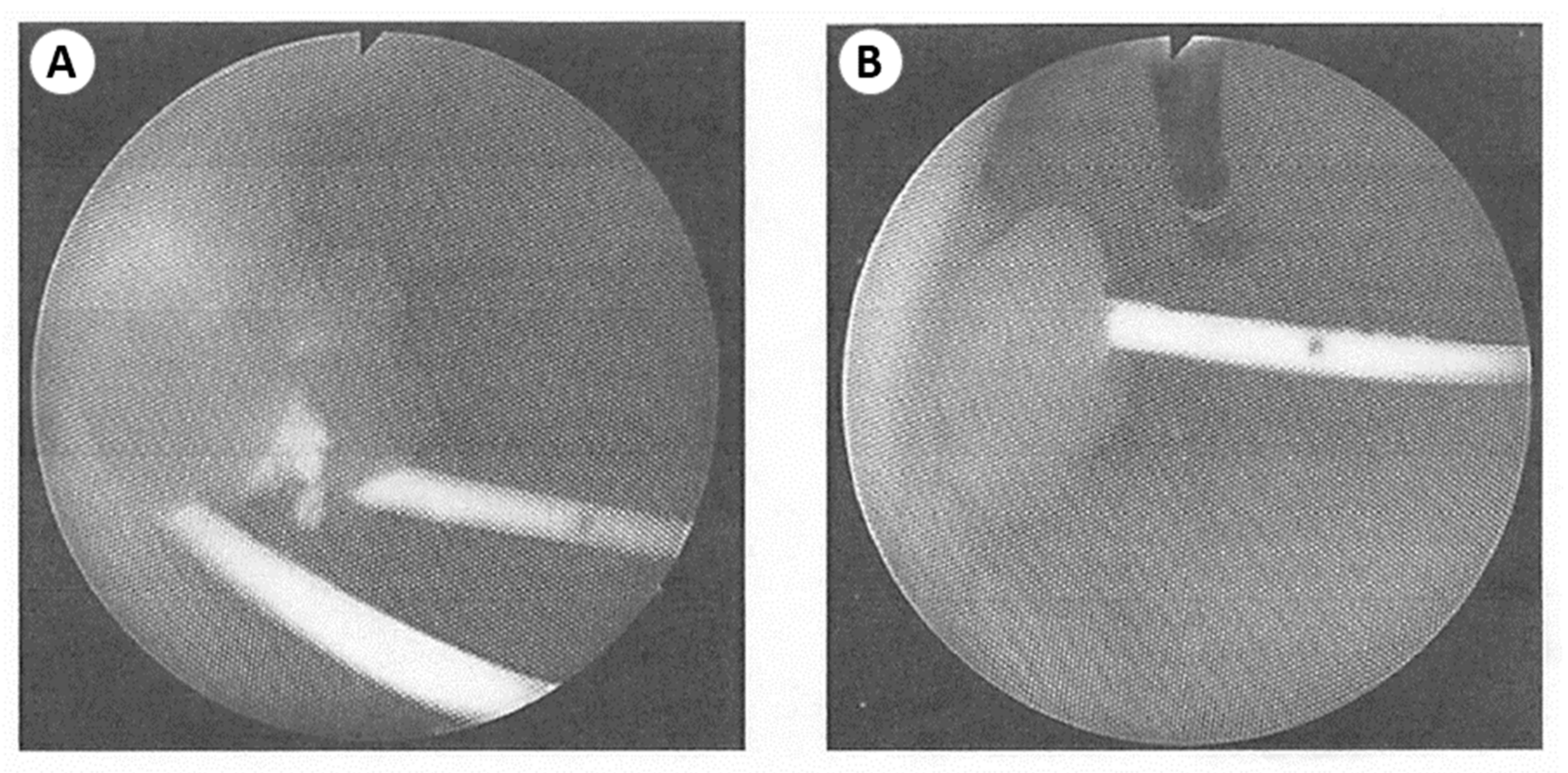
At the time of flexible cystoscopy for stent removal, the bladder mucosa looked normal, not irritated by the stents. The ureteral openings appeared as prominent pink cauliflowers on the front view (Figure 3A) as well as side view (Figure 3B). The distal ureteral segments both pulled into the bladder were well incorporated within the bladder wall and covered by normal looking bladder mucosa. Thus, the true anti-reflux valve created was composed of the 1.5–2 cm extra-mucosal segment created at the dome of the bladder plus the 1 cm intravesical segment covered by normal bladder mucosa (Figure 1D).
4. Discussion
The ureters from larger donors weighing up to 15 kg can be anastomosed to the bladder mucosa through an extra mucosal tunnel created on the dome of the bladder [2,3,4], but the technique is not applicable to the very small and short ureters. The pull-through technique described herein derived from both the extravesical Lich–Gregoir technique published respectively in 1961–1962 [3,4] and that described in 1972 by Shanfield [11]. The latter technique consisted of pulling the tip of the ureter through a small opening of the canine bladder wall and anchoring it to the full thickness dome of the bladder using one U stitch inserted at the distal tip of the ureter. In long-term surviving animals, autopsies have shown the ureter well incorporated into the bladder, simulating a competent valve preventing ureteral reflux despite forceful manual compression of the bladder during exploratory laparotomies. Our technique is safer than the Shanfield procedure by the addition of the extra-mucosal tunnel to reinforce the bladder closure. It is also safer than the Lich–Gregoir technique by internalizing the ureterovesical anastomosis inside the bladder, thus, avoiding any possibility of leakages. It is very possible that the use of a no-touch technique has allowed the anastomoses to be free of complications. Lastly, it provides a fully intravesical soft segment of ureter which collapses readily when intravesical pressure rises and acts as an effective anti-reflux valve. As shown during cystoscopy, this intravesical tunnel far exceeds the 5 to 1 ratio of length of the extra-mucosal ureteral segment/the diameter of the ureter, established by Paquin as a required condition for an effective anti-reflux ureterovesical anastomosis [12].
Unlike the adult kidney transplant procedure where ureteral stenting is still discussed despite the findings of a significant decrease in ureteral complications rate associated with the use of stents in randomized studies [13], the use of small stents is sufficient and necessary in handling the tiny ureters of the very small kidneys. They help to avoid the traumatic manipulation of the anastomoses. They prevent the intraluminal pressure build-up from post-operative edema and polyuria. They decrease the torsion, the acute angulation or twisting of the ureter, and avert external compression by intramural hematoma or perinephric collection. They preserve the patency of the ureteric vessels and allow the implantation site to heal. The short course of steroid therapy certainly facilitated the healing process.
Lastly but most importantly, the readily used indigo carmine angiogram, anytime there was any suspicion of ureteral damage by undue ureteral stretch and skeletonization or missing lower polar arteries from perihilar dissection, helped to avert the ureteral complications caused by ureteral ischemia resulting in early leaks (4%) and delayed ureteral stenosis (5.3%) reported recently [14]. The absence of complications in our series shows that the procedure, described in detail, step by step, is safe and easily reproducible and that bladder segment transplantation advocated previously is not necessary and even dangerous because of the high risk of ischemic bladder wall necrosis [15]. This was confirmed by the first case of en bloc transplantation using kidneys from an anencephalic baby with ureters anastomosed to ileal conduit in 1969 [16].
5. Conclusions
The “no-touch” pull-through UNC procedure described herein is simple to accomplish. It avoids the classic tedious and traumatic distal ureteroureteral vesical anastomoses used in larger kidneys. It shortens significantly the procedure by half (p < 0.02) as compared with the extravesical procedure with 10.2 min vs. 24.6 min, respectively [17]. With a 4-year graft survival of 95%, the technique proved to be a procedure of choice for re-implanting the ureters of very small EBKs. This simple and reproducible technique can be added to the surgeon’s armamentarium and increases the utilization of the very small en bloc kidneys.
Funding
The author has received no funding for the study.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
The author declares no conflict of interest.
References
- Cooper, D.C.; Hara, H.; Iwase, H.; Yamamoto, T.; Jaqdale, A.; Kumar, V.; Mannon, R.B.; Hanaway, M.J.; Anderson, D.J.; Eckhoff, D.E. Clinical Pig Kidney Xenotransplantation. How Close Are We? J. Am. Soc. Nephrol. 2020, 31, 12–21. [Google Scholar] [CrossRef] [PubMed]
- Nghiem, D.D. En Bloc transplantation of kidneys from donors under 15 kg into adult recipients. J. Urol. 1991, 145, 14–16. [Google Scholar] [CrossRef]
- Lich, R., Jr.; Howerton, L.W.; Davis, L.A. Childhood uro-sepsis. J. Ky. Med. Assoc. 1961, 59, 1177–1179. [Google Scholar] [PubMed]
- Gregoir, W. Congenital vesico-ureteral reflux. Acta Belg. 1962, 30, 286–300. [Google Scholar] [CrossRef] [PubMed]
- Nghiem, D.D.; Schlosser, J.D.; Hsia, S.; Nghiem, H.G. En bloc transplantation of infant kidneys. A Ten year experience. J. Am. Coll. Surg. 1998, 4, 402–405. [Google Scholar] [CrossRef]
- Hakim, N.S.; Benedetti, E.; Pirenne, J.; Gillingham, K.J. Complications of uretero-vesical anastomoses in kidney transplant patients: The Minnesota experience. Clin. Transpl. 1994, 8, 504–507. [Google Scholar]
- Zhao, W.Y.; Zhang, L.; Zhu, Y.H.; Chen, Y.; Zhu, F.Y.; Shen, Q.; Xu, H.; Zeng, L. En Bloc Kidneys Transplanted From Infant Donors Less Than 5 kg Into Pediatric Patients. Transplantation 2014, 97, 555–558. [Google Scholar] [CrossRef] [PubMed]
- Peng, J.; Dai, H.; Zhang, H.; Yu, S.; Xie, X.; Peng, F.; Lan, G.; Hu, S.; Wang, Y.; Tang, X.; et al. Comparison of Outcome of Kidney Transplantation From Extremely Low Body Weight </=5 kg Versus Larger Body Weight Pediatric Donors. Front. Immunol. 2021, 12, 738749. [Google Scholar]
- Nghiem, D.D. Rescue of En bloc Pediatric Kidneys Outflow Obstruction Using Proximal Spiral Vein Graft. Transplantation 2008, 86, 1147–1148. [Google Scholar] [CrossRef] [PubMed]
- Nghiem, D.D. Role of bench angiography in the assessment of pancreatic duodenal (PD) graft blood supply. Transpl. Proc. 1998, 30, 256–258. [Google Scholar] [CrossRef]
- Shanfield, I. New experimental methods for implantation for the ureter in bladder and conduit. Transplant. Proc. 1972, 4, 637–638. [Google Scholar] [PubMed]
- Paquin, A.J. Uretero-vesical anastomosis: The description and evaluation of a technique. J. Urol. 1959, 82, 573–583. [Google Scholar] [CrossRef]
- Mangus, R.S.; Hoag, B.W. Stented vs non stented extra-vesical Uretero-neo-cystostomy in Renal Transplantation. Meta. Anal. Am. J. Transpl. 2004, 4, 1889–1896. [Google Scholar] [CrossRef] [PubMed]
- Fananapazir, G.; Tse, G.; Di Geronimo, R.; Mc Vicar, J.; Perez, R.J.; Santhanakrishnan Sageshima, J.; Troppmann, C. Urologic complications after transplantation of 225 en bloc kidneys from small pediatric donors </=20 kg: Incidence, man-agement, and impact on graft survival. Am. J. Transpl. 2020, 20, 2126–2132. [Google Scholar]
- Kato, T.; Selvaggi, G.; Burke, G.; Cianco, G.; Zilleruelob, G.; Hattorid, M.; Gosalbeze, R.; Tsakis, A. Partial bladder transplantation with en bloc kidney transplant-the first case report of a “bladder patch technique“ in a human. Am. J. Transpl. 2008, 8, 1060–1063. [Google Scholar] [CrossRef] [PubMed]
- Martin, L.W.; Gonzalez, L.L.; West, C.D.; Swartz, R.A.; Sutorius, D.J. Homotransplantation of both kidneys from an anencephalic monster to a 17 pound boy with Eagle-Barrett syndrome. Surgery 1969, 66, 603–607. [Google Scholar] [CrossRef] [PubMed]
- Zagar, M.A.; Shahrohk, H.; Mohamadi Fallah, M.R.; Zagar, H. Comparing Taguchi and Anterior Lich-Gregoir uretero-vesical Re-implantation Techniques for Kidney Transplantation. Transplant. Proc. 2005, 37, 3077–3079. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Artistic rendering of the pull-through ureteral re-implantation through a single tunnel: (A) A 1.5–2 cm detrusor myotomy was performed allowing the mucosa to bulge out under the pressure of the irrigating solution, the arrow points to the small transverse opening of the distal mucosal pouch through which both ureters are brought into the bladder; (B) detail of the horizontal mucosal mattress suture at the tip of the ureter; (C) cavalier view of the bladder opening with both needles passing through the mucosal opening as full thickness sutures and exiting 1–1.5 cm from the bladder opening. The mucosal opening was kept open all the times by continuous irrigation of the bladder with indigo carmine stained antibiotic solution, avoiding traumatic manipulation of the mucosa and the ureters. For clarity, the stent was left out; (D) intravesical aspect of the spatulated ureter in place. It showed the ureteral orifice and the length of the “true” anti-reflux valve composed of both extra-mucosal and intravesical segments. For clarity, only one ureteral anastomosis is depicted; (E) schematic drawing of the distal ureters fitting snuggly through the mucosal opening and the stents in place, the ureteral implantation sites are 1–1.5 cm apart on the dome of the bladder; (F) the detrusor closure is represented burying the distal side by side ureters.
Figure 1.
Artistic rendering of the pull-through ureteral re-implantation through a single tunnel: (A) A 1.5–2 cm detrusor myotomy was performed allowing the mucosa to bulge out under the pressure of the irrigating solution, the arrow points to the small transverse opening of the distal mucosal pouch through which both ureters are brought into the bladder; (B) detail of the horizontal mucosal mattress suture at the tip of the ureter; (C) cavalier view of the bladder opening with both needles passing through the mucosal opening as full thickness sutures and exiting 1–1.5 cm from the bladder opening. The mucosal opening was kept open all the times by continuous irrigation of the bladder with indigo carmine stained antibiotic solution, avoiding traumatic manipulation of the mucosa and the ureters. For clarity, the stent was left out; (D) intravesical aspect of the spatulated ureter in place. It showed the ureteral orifice and the length of the “true” anti-reflux valve composed of both extra-mucosal and intravesical segments. For clarity, only one ureteral anastomosis is depicted; (E) schematic drawing of the distal ureters fitting snuggly through the mucosal opening and the stents in place, the ureteral implantation sites are 1–1.5 cm apart on the dome of the bladder; (F) the detrusor closure is represented burying the distal side by side ureters.

Figure 2.
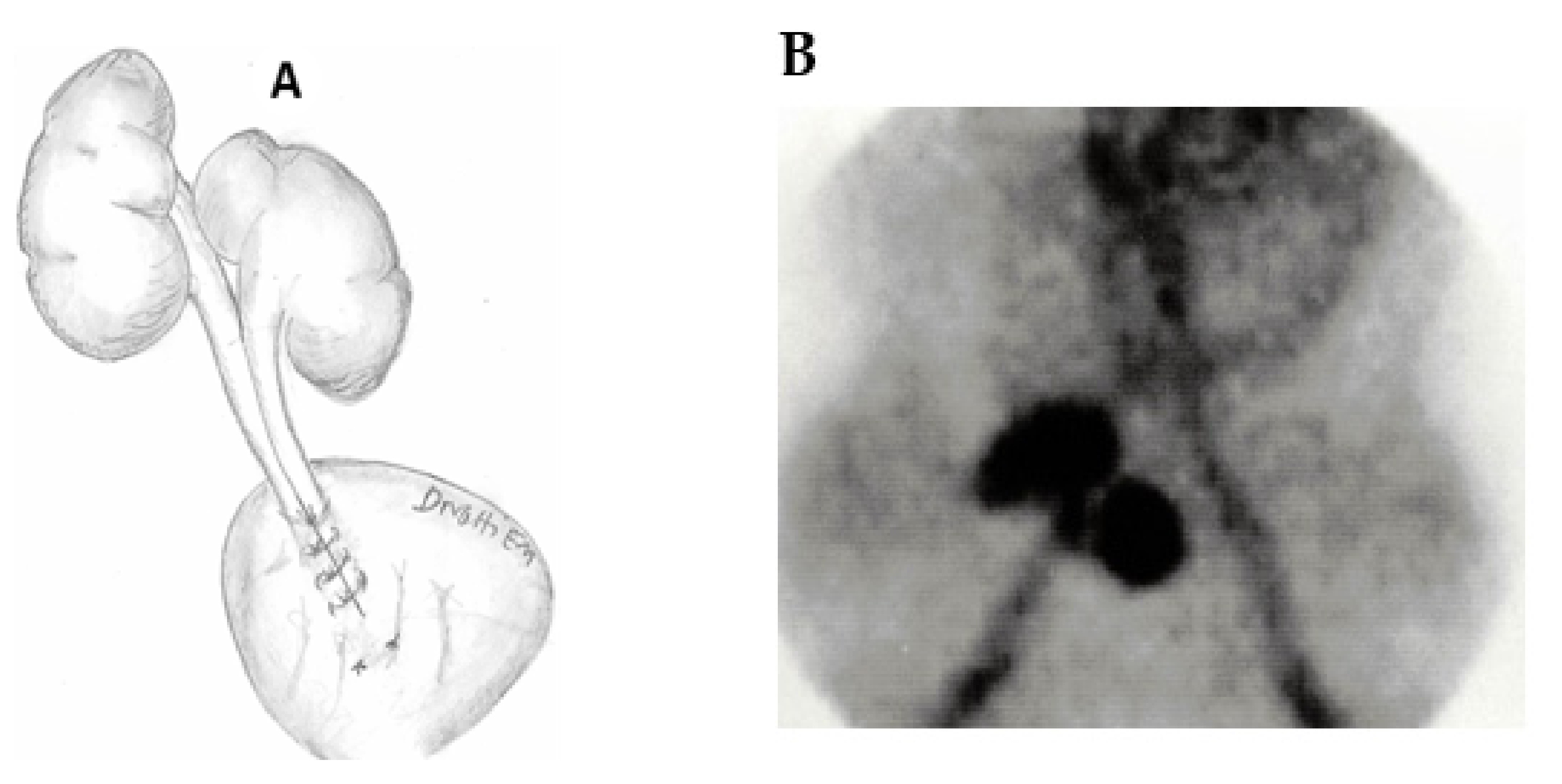
(A) Not in scale drawings of the en bloc kidneys in place, the stents are omitted for clarity; (B) technetium diethyl triamine penta-acetic acid scan on post-operative Day 1 showing the large avascular void in the right iliac fossa from the operative dissection and the very small en bloc kidneys. Compare the size of the kidneys to the size of the iliac arteries.
Figure 2.
(A) Not in scale drawings of the en bloc kidneys in place, the stents are omitted for clarity; (B) technetium diethyl triamine penta-acetic acid scan on post-operative Day 1 showing the large avascular void in the right iliac fossa from the operative dissection and the very small en bloc kidneys. Compare the size of the kidneys to the size of the iliac arteries.

Figure 3.
(A) Cystoscopic view of the ureteral implantation sites prior to stent removal; (B) close-up view of the ureteral nipple. The bladder mucosa looks normal. The distal ureter is well incorporated in the bladder mucosa and is not seen.
Figure 3.
(A) Cystoscopic view of the ureteral implantation sites prior to stent removal; (B) close-up view of the ureteral nipple. The bladder mucosa looks normal. The distal ureter is well incorporated in the bladder mucosa and is not seen.

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Nghiem, D.D. Pull-Through Ureteroneocystostomy for Very Small En Bloc Kidney Transplants from Donors Weighing ≤ 5 kg. Uro 2022, 2, 102-108. https://doi.org/10.3390/uro2020013
AMA Style
Nghiem DD. Pull-Through Ureteroneocystostomy for Very Small En Bloc Kidney Transplants from Donors Weighing ≤ 5 kg. Uro. 2022; 2(2):102-108. https://doi.org/10.3390/uro2020013
Chicago/Turabian StyleNghiem, Dai D. 2022. "Pull-Through Ureteroneocystostomy for Very Small En Bloc Kidney Transplants from Donors Weighing ≤ 5 kg" Uro 2, no. 2: 102-108. https://doi.org/10.3390/uro2020013