
Holmium Laser Enucleation of the Prostate Efficiency by Prostate Gland Size: Is There a Sweet Spot?


Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Overall Cohort Characteristics
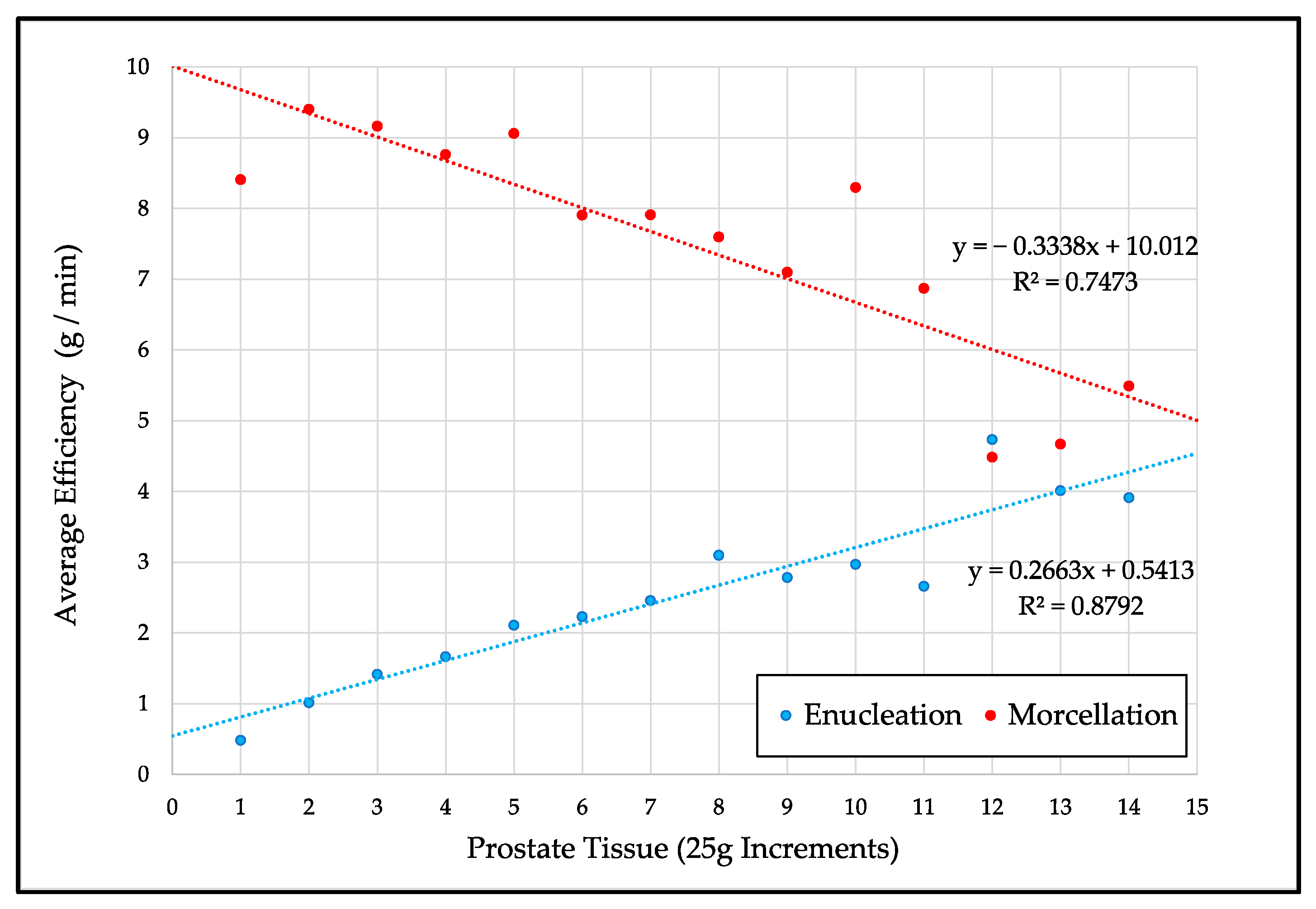
3.2. Enucleation Efficiency
3.3. Morcellation Efficiency
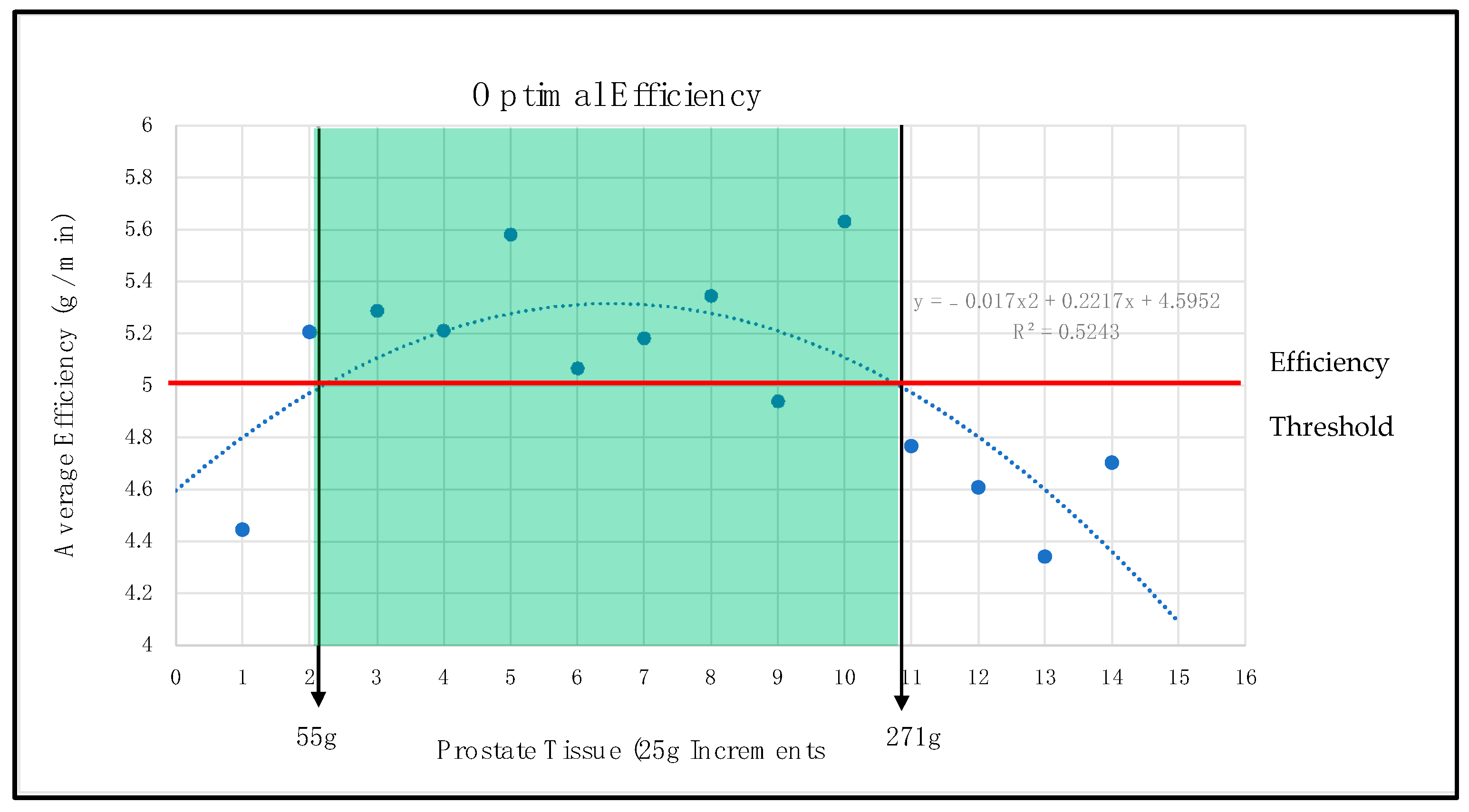
3.4. Overall Operative Efficiency
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Das, A.K.; Teplitsky, S.; Humphreys, M.R. Holmium laser enucleation of the prostate (HoLEP): A review and update. Can. J. Urol. 2019, 26, 13–19. [Google Scholar] [PubMed]
- Lerner, L.B.; McVary, K.T.; Barry, M.J.; Bixler, B.R.; Dahm, P.; Das, A.K.; Gandhi, M.C.; Kaplan, S.A.; Kohler, T.S.; Martin, L.; et al. Management of Lower Urinary Tract Symptoms Attributed to Benign Prostatic Hyperplasia: AUA GUIDELINE PART II-Surgical Evaluation and Treatment. J. Urol. 2021, 206, 818–826. [Google Scholar] [CrossRef] [PubMed]
- Assmus, M.A.; Large, T.; Lee, M.S.; Agarwal, D.K.; Rivera, M.E.; Krambeck, A.E. Same-Day Discharge Following Holmium Laser Enucleation in Patients Assessed to Have Large Gland Prostates (>/=175 cc). J. Endourol. 2021, 35, 1386–1392. [Google Scholar] [CrossRef] [PubMed]
- Krambeck, A.E.; Handa, S.E.; Lingeman, J.E. Holmium Laser Enucleation of the Prostate for Prostates Larger Then 175 Grams. J. Endourol. 2010, 24, 433–437. [Google Scholar] [CrossRef] [PubMed]
- Humphreys, M.R.; Miller, N.L.; Handa, S.E.; Terry, C.; Munch, L.C.; Lingeman, J.E. Holmium laser enucleation of the prostate—Outcomes independent of prostate size? J. Urol. 2008, 180, 2431–2435. [Google Scholar] [CrossRef] [PubMed]
- Magistro, G.; Schott, M.; Keller, P.; Tamalunas, A.; Atzler, M.; Stief, C.G.; Westhofen, T. Enucleation vs. Resection: A Matched-pair Analysis of TURP, HoLEP and Bipolar TUEP in Medium-sized Prostates. Urology 2021, 154, 221–226. [Google Scholar] [CrossRef] [PubMed]
- Chung, K.J.; Kim, J.H.; Min, G.E.; Park, H.K.; Li, S.; Del Giudice, F.; Han, D.H.; Chung, B.I. Changing Trends in the Treatment of Nephrolithiasis in the Real World. J. Endourol. 2019, 33, 248–253. [Google Scholar] [CrossRef] [PubMed]
- Zell, M.A.; Abdul-Muhsin, H.; Navaratnam, A.; Cumsky, J.; Girardo, M.; Cornella, J.; Nevo, A.; Cheney, S.; Humphreys, M.R. Holmium laser enucleation of the prostate for very large benign prostatic hyperplasia (≥200 cc). World J. Urol. 2021, 39, 129–134. [Google Scholar] [CrossRef] [PubMed]
- Dusing, M.W.; Krambeck, A.E.; Terry, C.; Matlaga, B.R.; Miller, N.L.; Humphreys, M.R.; Gnessin, E.; Lingeman, J.E. Holmium laser enucleation of the prostate: Efficiency gained by experience and operative technique. J. Urol. 2010, 184, 635–640. [Google Scholar] [CrossRef] [PubMed]
- Stern, K.L.; McAdams, S.B.; Cha, S.S.; Abdul-Muhsin, H.M.; Humphreys, M.R. A New Laser Platform for Holmium Laser Enucleation of the Prostate: Does the Lumenis Pulse 120H Laser Platform Improve Enucleation Efficiency? Urology 2017, 102, 198–201. [Google Scholar] [CrossRef] [PubMed]
- Kim, K.H.; Kim, K.T.; Oh, J.K.; Chung, K.J.; Yoon, S.J.; Jung, H.; Kim, T.B. Enucleated Weight/Enucleation Time, Is It Appropriate for Estimating Enucleation Skills for Holmium Laser Enucleation of the Prostate? A Consideration of Energy Consumption. World J. Men’s Health 2018, 36, 79–86. [Google Scholar] [CrossRef] [PubMed]
- Rosenhammer, B.; Schonharl, M.; Mayr, R.; Schnabel, M.J.; Burger, M.; Eichelberg, C. Introduction of a New Score to Assess Surgical Efficiency in Holmium Laser Enucleation of the Prostate. Urol. Int. 2020, 104, 914–922. [Google Scholar] [CrossRef] [PubMed]
- Lin, C.H.; Wu, W.J.; Li, C.C.; Wen, S.C. Preoperative predictors of enucleation time during en bloc ‘no-touch’ holmium laser enucleation of the prostate. BMC Urol. 2020, 20, 185. [Google Scholar] [CrossRef] [PubMed]
- Gild, P.; Lenke, L.; Pompe, R.S.; Vetterlein, M.W.; Ludwig, T.A.; Soave, A.; Chun, F.K.; Ahyai, S.; Dahlem, R.; Fisch, M.; et al. Assessing the Outcome of Holmium Laser Enucleation of the Prostate by Age, Prostate Volume, and a History of Blood Thinning Agents: Report from a Single-Center Series of >1800 Consecutive Cases. J. Endourol. 2021, 35, 639–646. [Google Scholar] [CrossRef] [PubMed]
- Marks, L.S.; Partin, A.W.; Dorey, F.J.; Gormley, G.J.; Epstein, J.I.; Garris, J.B.; Macairan, M.L.; Shery, E.D.; Santos, P.B.; Stoner, E.; et al. Long-term effects of finasteride on prostate tissue composition. Urology 1999, 54, 574–580. [Google Scholar] [CrossRef] [Green Version]
- Busetto, G.M.; Del Giudice, F.; Maggi, M.; Antonini, G.; D’Agostino, D.; Romagnoli, D.; Del Rosso, A.; Giampaoli, M.; Corsi, P.; Palmer, K.; et al. Surgical blood loss during holmium laser enucleationof the prostate (HoLEP) is not affected by short-term pretreatment with dutasteride: A double-blind placebo controlled trial on prostate vascularity. Aging 2020, 12, 4337–4347. [Google Scholar] [CrossRef] [PubMed]
- Wisenbaugh, E.S.; Nunez-Nateras, R.; Mmeje, C.O.; Warner, J.N.; Humphreys, M.R. Does prostate morphology affect outcomes after holmium laser enucleation? Urology 2013, 81, 844–848. [Google Scholar] [CrossRef] [PubMed]
- Elshal, A.M.; Soltan, M.; El-Tabey, N.A.; Laymon, M.; Nabeeh, A. Randomised trial of bipolar resection vs holmium laser enucleation vs Greenlight laser vapo-enucleation of the prostate for treatment of large benign prostate obstruction: 3-years outcomes. BJU Int. 2020, 126, 731–738. [Google Scholar] [CrossRef] [PubMed]
- McAdams, S.; Nunez-Nateras, R.; Martin, C.J.; Cha, S.; Humphreys, M.R. Morcellation Efficiency in Holmium Laser Enucleation of the Prostate: Oscillating Morcellator Outperforms Reciprocating Morcellator With no Apparent Learning Curve. Urology 2017, 106, 173–177. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Characteristic | Value (Range) |
|---|---|
| Total patients | 675 |
| Average age (years) | 71.1 (33.1–95.7) |
| Average ASA score | II (I–IV) |
| Preoperative prostate Size (mL) | 111.2 (14.0–672.0) |
| BMI (kg/m2) | 28.6 (18.1–72.7) |
| Average enucleation time (min) | 48.5 (5.0–151.0) |
| Average morcellation time (min) | 10.1 (0.5–113.0) |
| Average energy (kJ) | 110.00 (10.73–340.00) |
| Average intraoperative tissue weight (g) | 72.1 (1.0–448.0 g) |
| N (% of Total) | |
| History of preop urinary retention | 435 (64.4) |
| History of preop prostate cancer | 21 (3.1) |
| History of preop utis | 97 (14.4) |
| History of preop prostatitis | 42 (6.3) |
| History of diabetes | 76 (11.2) |
| Preop alpha blocker use | 519 (77.0) |
| Preop 5-ARi use | 221 (32.9) |
| Preop antiplatelet/anticoagulation medication | 133 (19.8) |
| 56 (8.3) |
| Previous BPH surgery | 48 (7.1) |
| Prostate morphology | |
| 179 (26.5) 496 (73.5) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Assmus, M.A.; Large, T.; Krambeck, A. Holmium Laser Enucleation of the Prostate Efficiency by Prostate Gland Size: Is There a Sweet Spot? Uro 2021, 1, 202-208. https://doi.org/10.3390/uro1040022
Assmus MA, Large T, Krambeck A. Holmium Laser Enucleation of the Prostate Efficiency by Prostate Gland Size: Is There a Sweet Spot? Uro. 2021; 1(4):202-208. https://doi.org/10.3390/uro1040022
Chicago/Turabian StyleAssmus, Mark Alexander, Tim Large, and Amy Krambeck. 2021. "Holmium Laser Enucleation of the Prostate Efficiency by Prostate Gland Size: Is There a Sweet Spot?" Uro 1, no. 4: 202-208. https://doi.org/10.3390/uro1040022