1. Introduction:
Total hip arthroplasty (THA) remains one of the most frequently performed and successful orthopedic procedures worldwide, with over 1 million THAs conducted annually [
1]. Appropriate preoperative planning is crucial for the successful performance and outcomes of THA. Extensive research over the past several decades has demonstrated the significant value of preoperative planning, as it allows for proper selection of implant size, correction of leg length discrepancy, and reduction in potential complications related to improper implant sizing or positioning. Specifically, preoperative templating enables the surgeon to digitally overlay representations of the prosthetic implant components onto radiographic images and simulate the anticipated results of the surgery. This is accomplished by first calibrating the digital radiographs using radio-opaque markers and then utilizing specialized templating software. Effective preoperative planning and templating has been associated with increased surgical accuracy and precision in reconstructing patient anatomy and mechanics [
2,
3,
4]. With the rising demand for THA in aging populations, appropriate preoperative planning will continue to play a critical role in achieving successful clinical outcomes.
One of the primary goals of total hip arthroplasty (THA) is to recreate the natural center of rotation (COR) of the hip joint. This is accomplished by returning the center of the migrated femoral head to the reconstructed COR of the acetabulum through precise implantation of the prosthetic components [
5]. Proper restoration of the hip COR helps balance stress distribution across the joint, improve range of motion, reduce wear, and prolong the survival of the prosthetic implants [
6,
7]. As re-establishing the native COR is key to optimizing joint function and mechanics after THA, developing accurate methods to evaluate COR restoration is critically important. However, this remains technically challenging due to variability in patient anatomy, surgical techniques, and implant positioning. Prior studies have attempted to quantify COR restoration through a variety of radiographic measurements, computer simulations, and navigation systems with mixed results. Additional research is still needed to determine optimal techniques for assessing the accuracy of COR reconstruction following THA and relating COR restoration to clinical outcomes [
8,
9,
10].
Recreating the natural center of rotation (COR) of the hip joint is a key surgical goal in total hip arthroplasty (THA) to optimize mechanics and implant longevity. Though prior studies propose accurately restoring the COR to within 5 mm of its native anatomy, this remains technically challenging, especially in complex hip pathologies. Digital preoperative templating is now standard practice in THA planning, but its impact on the precision of COR restoration is unclear. While some radiographic studies have shown templating can predict the COR to within 5 mm of operative outcomes, it is unknown if this translates to better clinical function or implant survival. Only a few computational models have estimated differences in joint stresses based on variances in COR. However, no study has directly tied templating accuracy to measurable patient outcomes. Surgeon experience and nuances in surgical technique also contribute to variability in reconstructing the COR [
11,
12,
13].
Given the critical role of the COR in hip biomechanics and the widespread use of digital templating, further research is warranted. Quantitative techniques to evaluate COR positioning could optimize templating protocols. Relating templating accuracy to functional outcomes and implant performance would provide clinically meaningful data. This could enhance preoperative planning to improve surgical precision in restoring the COR. Personalized templating and mixed reality guidance also show promise for increasing accuracy. Overall, understanding the connection between templating, COR restoration, and clinical outcomes will allow a refinement of techniques to maximize results in THA. The goal of our study was to assess whether an inaccurate position of the COR is associated with impairment in clinical outcomes. To our knowledge, no study has previously evaluated the association between accurate preoperative prediction of the COR and clinical outcomes of the hip postoperatively.
2. Materials and Methods
Approval from the Institutional Ethics Research Board was successfully secured for the execution of this retrospective study, reflecting a commitment to ethical research practices. The study cohort comprised individuals aged 50 years and older who had undergone Total Hip Arthroplasty (THA) at our institution during the period spanning from August 2018 to May 2020. The implant components employed in these procedures included the CorailTM stem (manufactured by DePuy Synthes, Warsaw, IN, USA) and the PinnacleTM cup (also from DePuy Synthes, Warsaw, IN, USA).
The surgical approach varied among patients and included options such as anterolateral, posterolateral, or direct anterior, chosen based on individual clinical considerations. The primary surgical indications for all patients enrolled in our study were osteoarthritis and avascular necrosis (AVN), underscoring the need for THA intervention in these cases.
It is important to note that certain exclusion criteria were applied in order to maintain the study’s focus and integrity. Patients with sub capital or intertrochanteric fractures, those with peri-prosthetic fractures, individuals with developmental dysplasia of the hip (DDH) or Perthes disease, patients who had undergone cemented THA, those who had experienced postoperative infections, and individuals with a history of previous hip surgeries were systematically excluded from our analysis. Furthermore, an integral aspect of our methodology was the implementation of preoperative digital templating, facilitated using the King Mark device, ensuring meticulous planning and precision in our THA procedures. This standardized approach to data collection and analysis enhances the robustness and reliability of our findings, contributing to the overall rigor of our study.
2.1. Preoperatively
Preoperatively, patients underwent an anterior–posterior (AP) X-ray of the pelvis while lying supine. The beam source was 100 cm from the X-ray plate and positioned 90° relative to the table. The legs were placed in 15° of internal rotation. The beam was centered at the sacrum.
All patients underwent preoperative digital templating with the aid of the King Mark device where a radiolucent marker pad was placed behind the pelvis, while a marker with radio-opaque balls was placed in front of the pelvis.
2.2. Determination of the COR
Preoperatively, the COR was determined via calibrated radiograph on Trauma Cad software v2.0 (Voyant Health, Petach-Tikva, Israel). The center of a circle that encircled the femoral head determined the preoperative COR. A line was drawn horizontally across the teardrop, which intersected another perpendicular line that was drawn vertically from the COR. This point of intersection measured represented the preoperative distance from the teardrop’s tip to the COR (
Figure 1).
2.3. Postoperatively
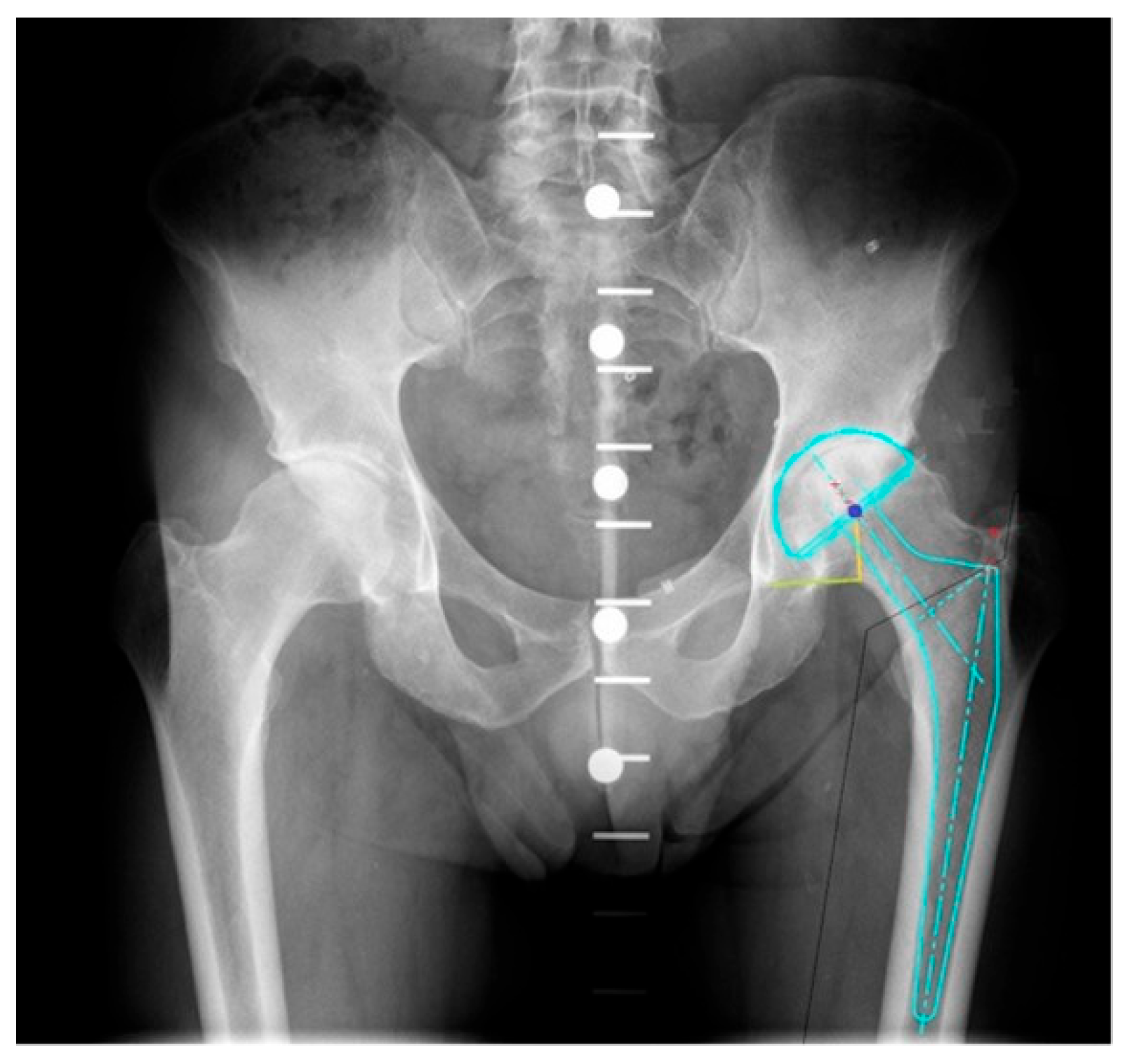
Postoperative radiographs were obtained one day after surgery for all patients. The postoperative COR was determined using the center of a circle encircling the prosthetic femoral head on the ipsilateral side. Radiographs were calibrated according to the prosthetic femoral head. Similar to the preoperative process, we drew a horizontal line from the teardrop and a vertical point from the COR and took the point of intersection (
Figure 2).
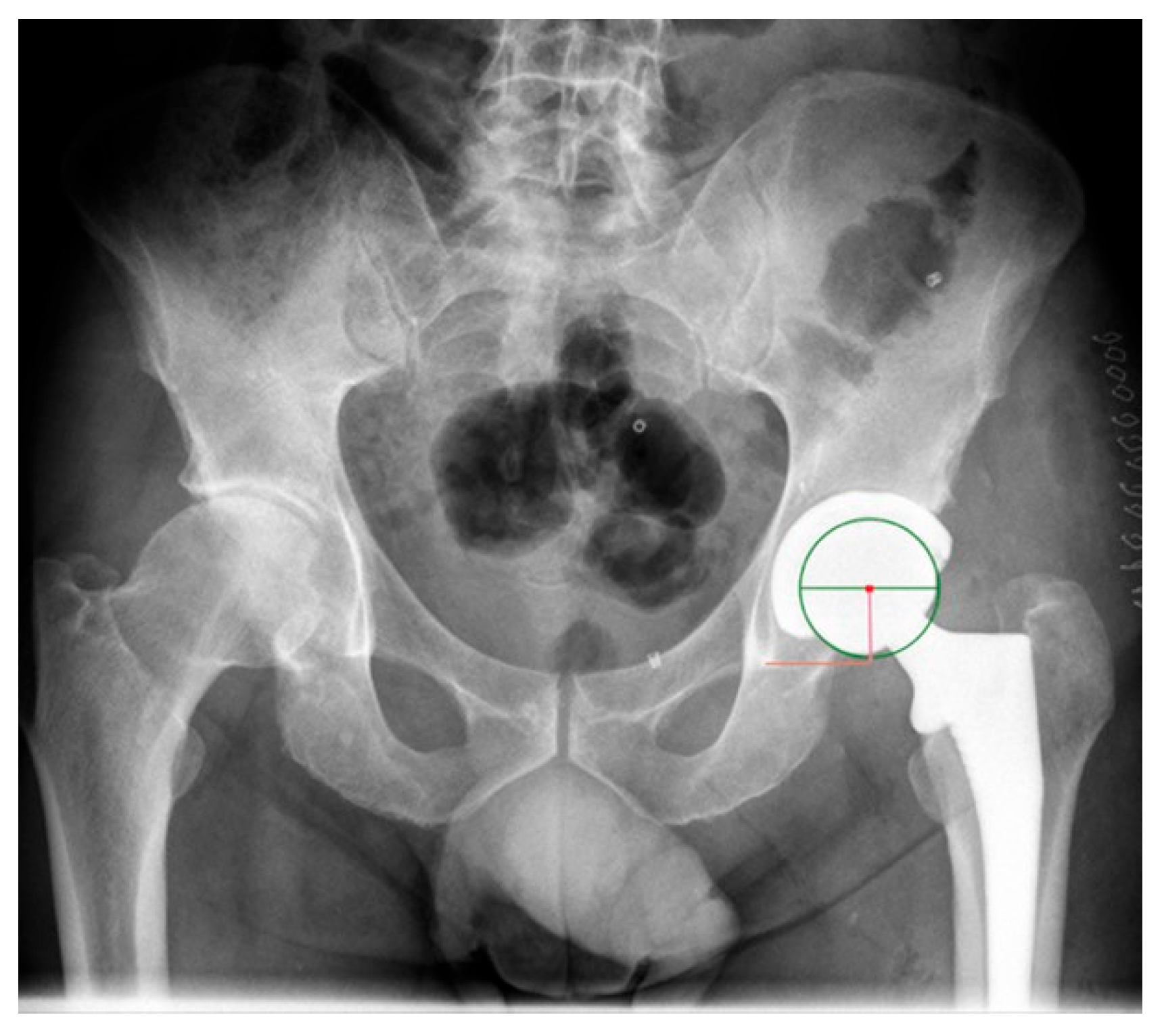
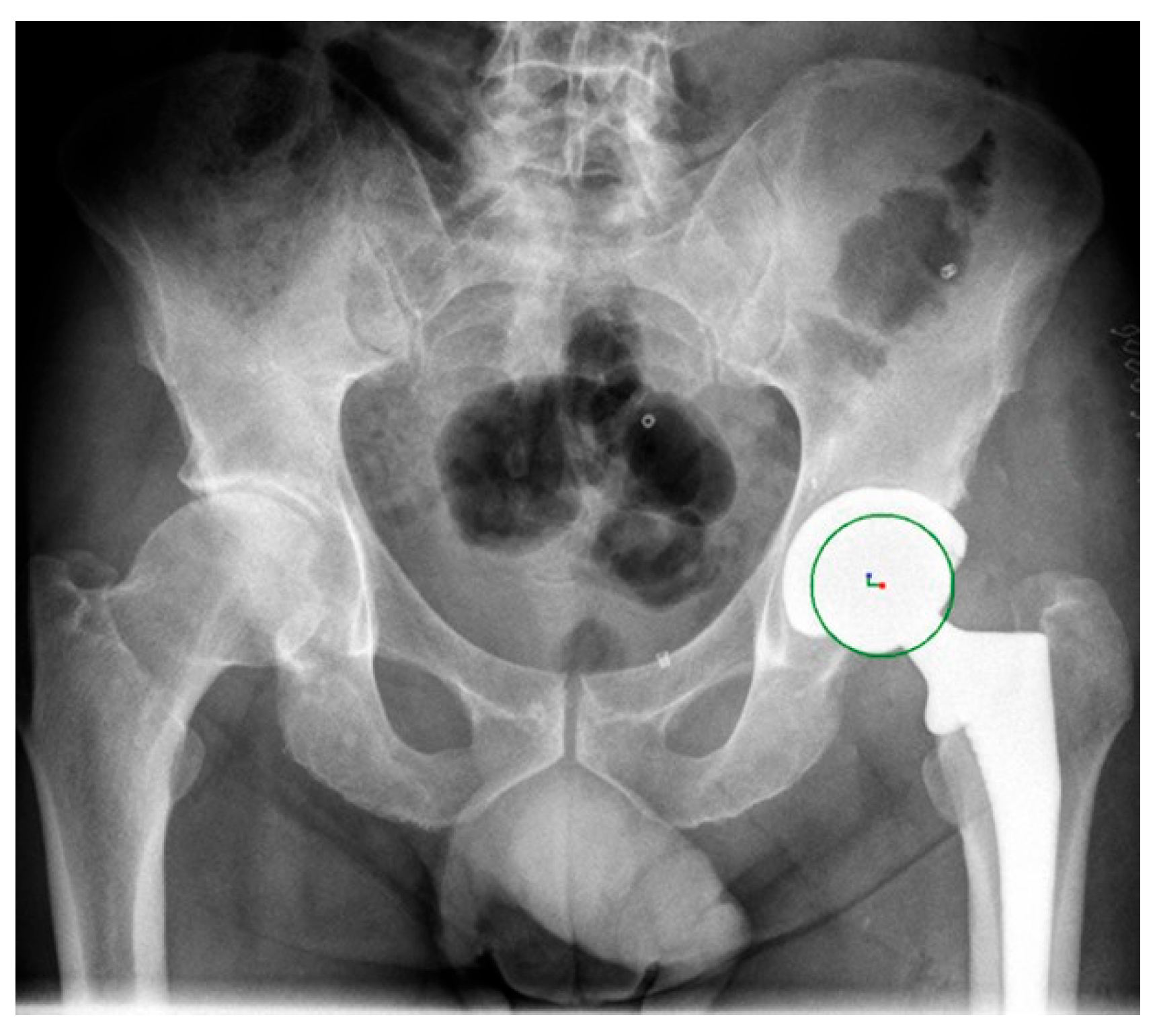
The distance of the COR preoperatively was compared to its postoperative value (
Figure 3).
Patients were subsequently stratified into two subgroups based on if their COR had deviated over or under 5 mm from preoperative limits.
Clinical outcome measures were determined using the physical component scale (PCS), the mental component scale (MCS) of the SF-12, as well as the VAS. All patients subsequently answered a questionnaire comprising a 12-Item Short Form Health Survey (SF-12) and visual analogue scale (VAS), which was completed via a telephone interview.
2.4. Statistical Analysis
Statistical analyses were performed using SPSS version 21 (IBM). Patients’ demographics, surgical characteristics, and outcomes were analyzed using appropriate statistical tests. Chi-square tests were used to assess the association between categorical variables such as gender, BMI category, surgery side, and surgery approach with COR placement. Continuous variables such as BMI, age at surgery, PCS, MCS, and VAS scores were compared between the two COR groups using t-tests or Mann–Whitney U tests, as appropriate, based on the distribution of the data. A p-value less than 0.05 was considered statistically significant.
3. Results
The study population consisted of 100 patients. Eight patients were lost to follow up, one patient had a postoperative infection, and another patient had a peri-prosthetic fracture. Thus, the final study population consisted of 90 patients. 60 patients (66%) had their COR accurately predicted within preoperative limits, whereas 30 (33%) patients had their COR predicted over 5 mm.
Sex was found to have no significant influence on COR in 5 mm increments, with 38 cases in females and 19 cases in males exhibiting COR in the 5 mm range (p = 0.27). Similarly, BMI showed no significant association with COR placement, with a mean BMI of 28.6 for cases within the 5 mm COR range compared to 27.6 for cases outside this range (p = 0.36). When categorized by BMI range, no statistical significance was observed either (p = 0.67). Age at surgery also displayed no substantial effect on COR placement, as the mean age at surgery for cases with COR in the 5 mm range was 68.2, while it was 66.8 for cases outside this range (p = 0.56).
Surgery side demonstrated a significant association with COR placement (
p = 0.028). Patients who underwent THA on the left side were more likely to exhibit COR in the 5 mm range (31 cases) compared to the right side (29 cases). Surgery approach displayed a trend towards significance, with 28 cases in the direct anterior approach, 20 in the posterolateral approach, and 12 in the anterolateral approach showing COR in the 5 mm range (
p = 0.056) (
Table 1).
The analysis revealed no significant association between COR placement and the physical component summary (PCS) score of PROs, as 43.8% of patients with a COR within 5 mm exhibited PCS scores, while 46% of patients with a COR less than 5 mm displayed similar scores (p = 0.33). Likewise, there was no significant impact on the mental component summary (MCS) score based on COR placement, with 54% of patients in the COR within 5 mm group reporting MCS scores, compared to 56.8% in the COR less than 5 mm group (p = 0.16). The visual analog scale (VAS) score, which measures pain perception, also did not display a significant difference between the two COR groups, with a mean VAS score of 3.3 for patients within 5 mm and 2.5 for patients with a COR less than 5 mm (p = 0.12).
Overall, these results indicate that COR placement in THA does not appear to have a substantial impact on patient-reported physical and mental health outcomes or pain perception, as measured by the PCS, MCS, and VAS scores. This suggests that the precision of COR placement may not be a critical factor in achieving desirable PROs, which may provide reassurance to both patients and healthcare providers when considering THA (
Table 2).
4. Discussion
The main finding of our study was that patients whose COR was accurately positioned within preoperative limits did not have improved clinical outcomes, compared to patients whose COR was not predicted accurately.
Digital templating has proven to be a vital aspect of preoperative planning in THA. The essential goal of THA is to re-create the COR in order to increase muscle function and stability and to prolong the survival of the prosthesis [
7]. In regard to restoring the COR, templating functions to predict cup position in terms of height, depth, and angular position. There is a general consensus that an accurate reconstruction of the COR is within 5 mm of its anatomical location [
11,
12,
13]. Using preoperative planning with an uncemented prosthesis, Bjarnason et al. [
11] preserved the COR within 5.0 mm of limits after THA in 55% (
n = 40) of the patients. As clinical outcomes were not measured in this study, the implications of accurately restoring the COR to within 5 mm of its anatomical location are unknown. As a result of this uncertainty, we devised the following study to assess whether an accurate position of the COR in relation to preoperative planning is associated with improved clinical outcomes.
A few well-established factors have been shown to influence accurate restoration of the COR during THA. Meermans et al. [
7] compared the displacement of the COR in patients who underwent a conventional reaming technique to patients who underwent more conservative reaming. Their results showed the COR of the patients in the standard reaming group was significantly more displaced medially and superiorly than in patients that underwent more conservative reaming. Bonnin et al. [
14] presented similar findings regarding the effect of reaming on the COR. Furthermore, Shao et al. [
15] demonstrated that reaming depth is a significant variable that affects reconstruction of the COR.
If the reaming depth is too deep or shallow, it can change the force torque of the reconstructed hip and thus affect the survivorship of the prosthesis [
15]. Precise reaming is therefore an important aspect of successful THA. In certain circumstances, however, such as cup instability or poor bone stock quality, surgeons must alter their reaming method. In the context of bone loss, superior reaming may be necessary to achieve better fixation in the reaming bone, which is likely to superiorly displace the COR [
16]. Moreover, surgeons may elect to alter the acetabular size and positions from the templated plan. Such a decision reflects their evaluation of the remaining acetabular walls during reaming and has a potential effect on the final location of the COR [
17].
We believe these intra-operative decisions contributed to the main finding: that the clinical outcomes between cohorts did not differ. Certain intra-operative factors likely influenced the surgeon’s technique, which resulted in a displacement of the COR to greater than 5 mm of preoperative limits. The findings of our study have important implications. During patient follow-up, if a surgeon notices that the COR was slightly deviated more than 5 mm of within preoperative limits, our results suggest that this is unlikely to have an influence over their future clinical outcome.
It is important to recognize additional factors beyond accurate preoperative planning and center of rotation (COR) reconstruction that can influence total hip arthroplasty outcomes, including surgical competence, perioperative management, patient compliance, and complications. Advanced postoperative imaging and motion analysis techniques, such as radiographs, MRI, CT, and kinematic analysis using motion capture systems, could provide a more comprehensive assessment of COR restoration and prosthesis–COR interaction during activities. Incorporating some of these quantitative assessments in future studies may strengthen the investigation of factors impacting clinical results. A multifaceted approach, integrating careful preoperative planning, precise surgical technique, optimal perioperative care, and advanced biomechanical analysis, will facilitate superior outcomes after total hip arthroplasty. Further research into patient immune factors affecting infection risk may also offer additional insight [
18].
This study has several limitations. Firstly, the sample size in our study could have been larger, which makes it susceptible to sampling bias. We acknowledge that our conclusions may not be applicable to patients whose COR underwent major displacement exceeding 5 mm. Our findings are most likely relevant for patients with minor deviations in their COR, as it is probable that significant displacement would negatively impact their clinical outcomes. Additionally, the utilization of only the coronal view to measure the COR in patients might have influenced our results. The use of a single 5 mm cut-off for subgroup analysis provides limited insight on the impact of more substantial deviations in center of rotation; future studies should incorporate analyses at additional thresholds, such as 10 mm and 20 mm deviations, to fully characterize the relationship between center of rotation change and outcomes. Lastly, the retrospective nature of this study presents an additional limitation, as it limits our ability to establish a causal relationship and control for potential confounding variables.
5. Conclusions
Patients whose COR was accurately predicted within 5 mm of preoperative limits were not associated with improved clinical outcomes, compared to patients whose COR was not accurately predicted. Therefore, during the postoperative evaluation of the COR, surgeons should feel confident if the COR exceeds the preoperative limitations by a slight margin of 5 mm.
Author Contributions
Conceptualization, Y.W.; methodology, N.A.; validation, I.A., A.G. and N.S.; formal analysis, S.M.; investigation, N.A. and O.S.; data curation, O.S.; writing—original draft preparation, S.M., N.A. and Y.W.; writing—review and editing, S.F. and Y.W.; supervision, Y.W. and N.S.; project administration, S.F. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Tel Aviv Medical Center Helsinkey Committee Approval code tlv-0268-21 and date of approval 1 December 2021).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Data are contained in the article.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Karachalios, T.; Komnos, G.; Koutalos, A. Total hip arthroplasty: Survival and modes of failure. EFORT Open Rev. 2018, 3, 232–239. [Google Scholar] [CrossRef] [PubMed]
- Shin, J.K.; Son, S.M.; Kim, T.W.; Shin, W.C.; Lee, J.S.; Suh, K.T. Accuracy and Reliability of Preoperative On-screen Templating Using Digital Radiographs for Total Hip Arthroplasty. Hip Pelvis Korea 2016, 28, 201–207. [Google Scholar] [CrossRef] [PubMed]
- Kosashvili, Y.; Shasha, N.; Olschewski, E.; Safir, O.; White, L.; Gross, A.; Backstein, D. Digital versus conventional templating techniques in preoperative planning for total hip arthroplasty. Can. J. Surg. Can. 2009, 52, 6–11. [Google Scholar]
- Eggli, S.; Pisan, M.; Muller, M.E. The value of preoperative planning for total hip arthroplasty. J. Bone Jt. Surg. Br. Engl. 1998, 80, 382–390. [Google Scholar] [CrossRef]
- Lum, Z.C.; Dorr, L.D. Restoration of center of rotation and balance of THR. J. Orthop. 2018, 15, 992–996. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.; Zhou, J.; Liu, Y.; Guan, J.; Ding, H.; Wang, Z.; Dong, Q. Mid-term and long-term results of restoring rotation center in revision hip arthroplasty. J. Orthop. Surg. Res. 2020, 15, 152. [Google Scholar] [CrossRef] [PubMed]
- Meermans, G.; Doorn JVan Kats, J.-J. Restoration of the centre of rotation in primary total hip arthroplasty: The influence of acetabular floor depth and reaming technique. Bone Joint J. Engl. 2016, 98-B, 1597–1603. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.; Guan, J.Z.; Zhang, Z.; Chen, X.T.; Ma, X.D.; Zhao, J.N.; Zhou, J.S. Restoring Rotation Center in Total Hip Arthroplasty for Developmental Dysplasia of the Hip with the Assistance of Three Dimensional Printing Technology: A Pilot Study. Orthop. Surg. 2022, 14, 119–128. [Google Scholar] [CrossRef] [PubMed]
- Fukushi J ichi Kawano, I.; Motomura, G.; Hamai, S.; Kawaguchi K ichi Nakashima, Y. Does hip center location affect the recovery of abductor moment after total hip arthroplasty? Orthop. Traumatol. Surg. Res. 2018, 104, 1149–1153. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, H.; Yamada, N.; Kurishima, H.; Mori, Y.; Aizawa, T. Association between Hip Center Position and Isokinetic Hip Muscle Performance after Anterolateral Muscle-Sparing Total Hip Arthroplasty. Medicina 2022, 58, 538. [Google Scholar] [CrossRef] [PubMed]
- Bjarnason, J.A.; Reikeras, O. Changes of center of rotation and femoral offset in total hip arthroplasty. Ann. Transl. Med. 2015, 3, 355. [Google Scholar] [PubMed]
- Jolles, B.M.; Zangger, P.; Leyvraz, P.-F. Factors predisposing to dislocation after primary total hip arthroplasty: A multivariate analysis. J. Arthroplast. 2002, 17, 282–288. [Google Scholar] [CrossRef] [PubMed]
- Cassidy, K.A.; Noticewala, M.S.; Macaulay, W.; Lee, J.H.; Geller, J.A. Effect of femoral offset on pain and function after total hip arthroplasty. J. Arthroplast. 2012, 27, 1863–1869. [Google Scholar] [CrossRef] [PubMed]
- Bonnin, M.P.; Archbold, P.H.A.; Basiglini, L.; Fessy, M.H.; Beverland, D.E. Do we medialise the hip centre of rotation in total hip arthroplasty? Influence of acetabular offset and surgical technique. Hip Int. 2012, 22, 371–378. [Google Scholar] [CrossRef] [PubMed]
- Shao, P.; Li, Z.; Yang, M.; Wang, Y.; Liu, T.; Yang, Y.; Duan, L.; Jiang, J.; Zuo, J. Impact of acetabular reaming depth on reconstruction of rotation center in primary total hip arthroplasty. BMC Musculoskelet. Disord. 2018, 19, 425. [Google Scholar] [CrossRef] [PubMed]
- Khlopas, A.; Chughtai, M.; Elmallah, R.K.; Hip-Flores, D.; Malkani, A.L.; Harwin, S.F.; Mont, M.A.; Ries, M.D. Novel Acetabular Cup for Revision THA Improves Hip Center of Rotation: A Radiographic Evaluation. Clin. Orthop. Relat. Res. 2018, 476, 315–322. [Google Scholar] [CrossRef] [PubMed]
- Warschawski, Y.; Shichman, I.; Morgan, S.; Shaked, O.; Garceau, S.; Amzallag, N.; Snir, N.; Gold, A. The accuracy of external calibration markers in digital templating using the double marker and single marker method: A comparative study. Arch. Orthop. Trauma. Surg. 2020, 140, 1559–1565. [Google Scholar] [CrossRef] [PubMed]
- Basile, G.; Gallina, M.; Passeri, A.; Gaudio, R.M.; Castelnuovo, N.; Ferrante, P.; Calori, G.M. Prosthetic joint infections and legal disputes: A threat to the future of prosthetic orthopedics. J. Orthop. Traumatol. 2021, 22, 44. [Google Scholar] [CrossRef] [PubMed]
| Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).

 ,
, 



{kind=link}
{kind=link}
{kind=link}