
Exploring the Literature on Narcolepsy: Insights into the Sleep Disorder That Strikes during the Day


Abstract
:1. Introduction
2. Development of the First Knowledge of Narcolepsy—A Timeline
3. Information about Narcolepsy in Different Populations
4. Age of Onset
5. Causes and Risk Factors of Narcolepsy
5.1. Hypocretin (Orexin) Deficiency
5.2. Loci Associated with Susceptibility to Narcolepsy
5.3. Variations in the Specific Human Leukocyte Antigen (HLA) Gene
5.4. Environmental Factors
5.5. Brain Injuries
6. Functional Changes in Narcolepsy
- Excessive daytime sleepiness (EDS): people with narcolepsy often feel drowsy and fatigued during the day, regardless of how much sleep they obtain at night.
- Cataplexy: This is a sudden loss of muscle tone that can cause a person to collapse or become weak. It is usually triggered by strong emotions such as laughter or anger.
- Sleep attacks: narcoleptics may experience sudden and irresistible urges to sleep during the day.
- Sleep paralysis: this is a temporary inability to move or speak while falling asleep or waking up.
- Hallucinations: hypnagogic hallucinations, which occur as one is falling asleep, and hypnopompic hallucinations, which occur as one is waking up, can occur with narcolepsy.
7. Symptoms of Narcolepsy
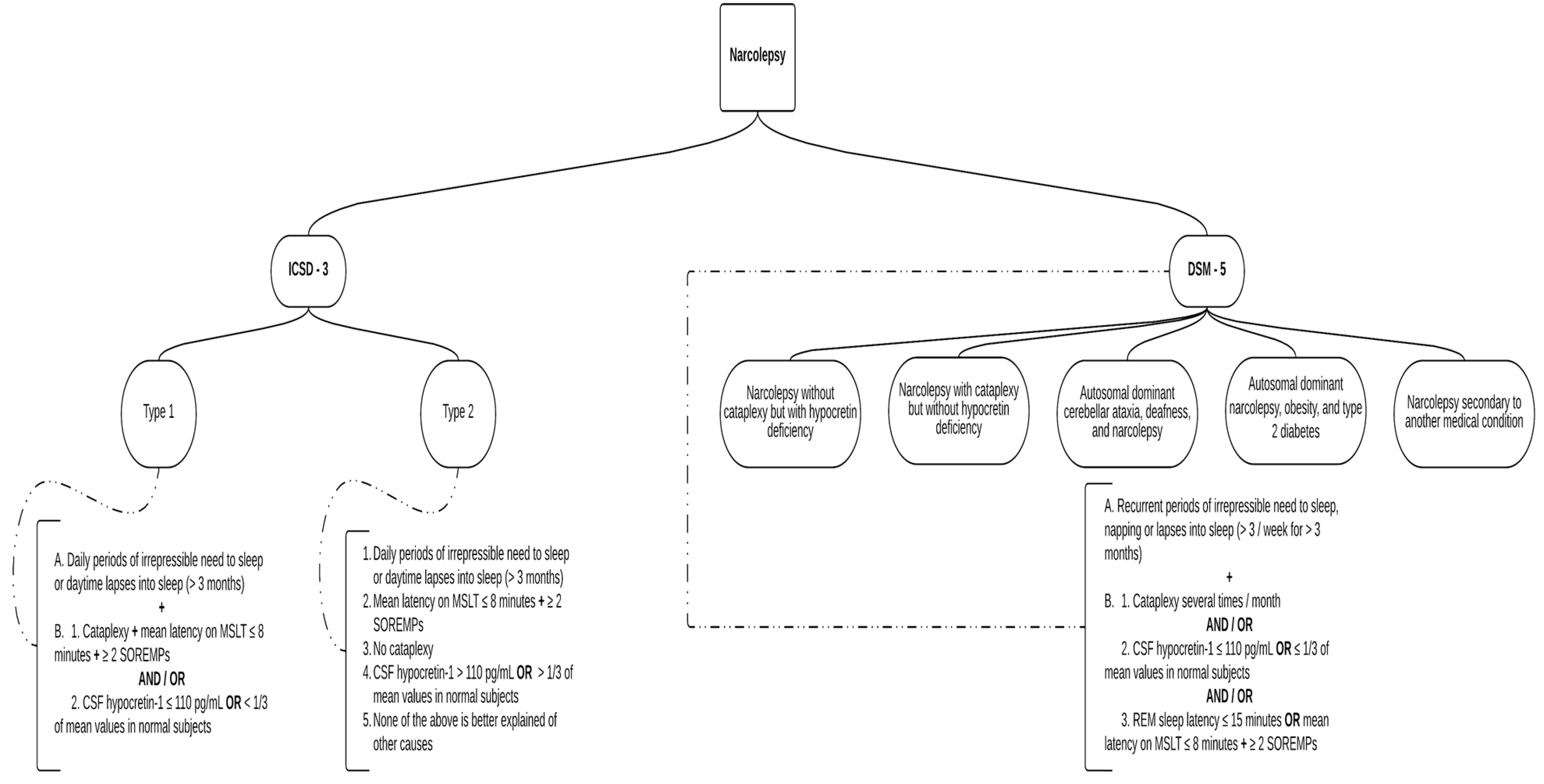
8. Classification and Diagnosis
- Type 1 narcolepsy.
- Type 2 narcolepsy.
- Narcolepsy without cataplexy but with hypocretin deficiency;
- Narcolepsy with cataplexy but without hypocretin deficiency;
- Autosomal dominant cerebellar ataxia, deafness, and narcolepsy;
- Autosomal dominant narcolepsy, obesity, and type 2 diabetes;
- Narcolepsy secondary to another medical condition.
- A Nocturnal Polysomnogram (NPSG), which records an electroencephalogram, eye movement, an electrocardiogram, and pulse oximetry during sleep [90].
- A Multiple Sleep Latency Test (MSLT), which measures the time from the moment lights are out to the first epoch of any stage of sleep [91].
- Additionally, with the short nocturnal rapid eye movement sleep latency (REML), calculated within an NPSG, comes a more accurate narcolepsy diagnosis [92]. To identify patients at risk of developing narcolepsy, especially in familial cases, the HLA haplotype and predisposition genes can also be tested.
9. Comorbidities
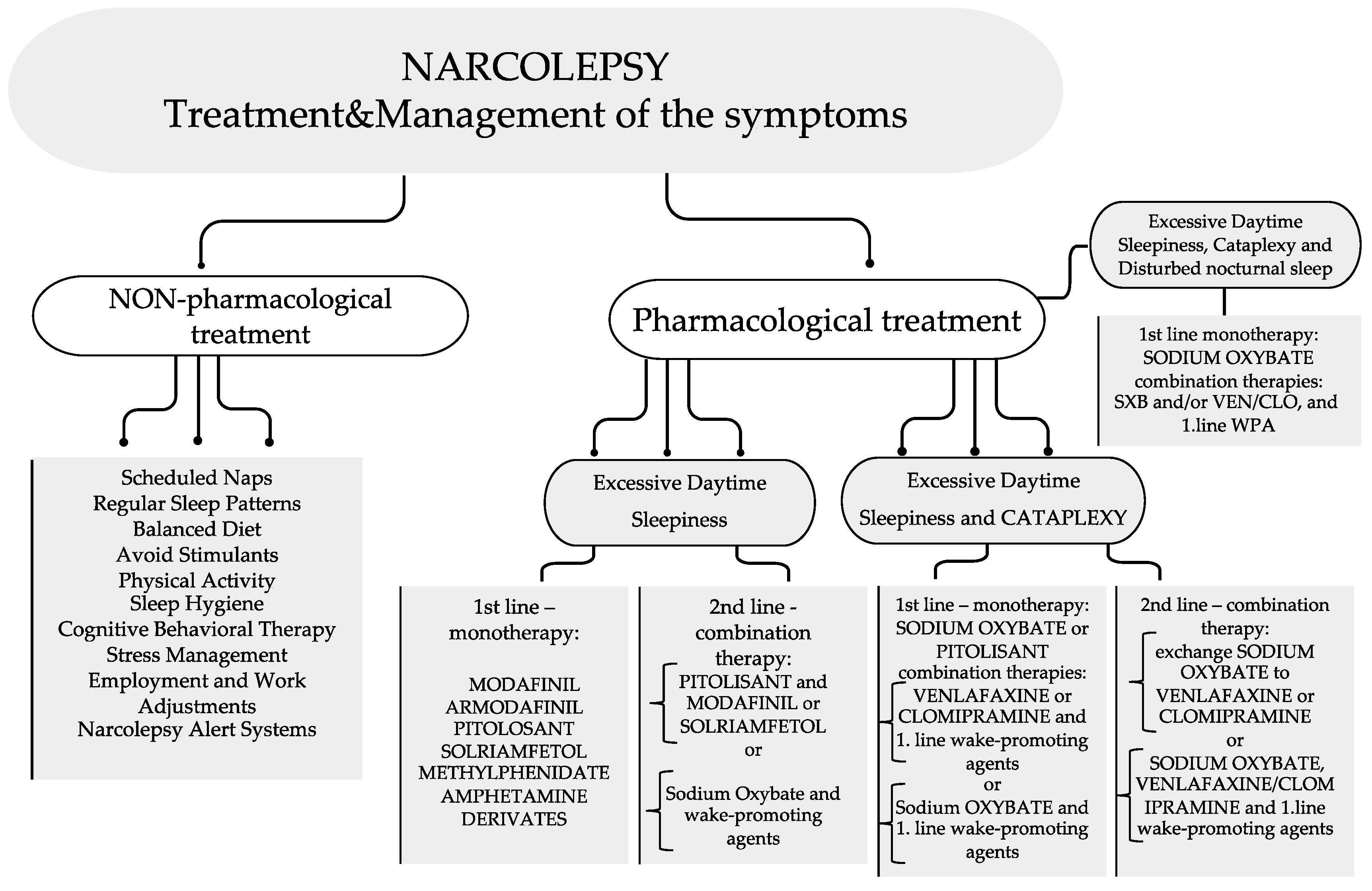
10. Treatments
10.1. Non-Pharmacological Treatment
10.2. Pharmacological Treatment
10.2.1. Treatment for Excessive Daytime Sleepiness
10.2.2. Treatment for Cataplexy
10.3. Treatments for Special Narcoleptic Groups
11. Prevention
12. Prognosis
13. Daily Life
14. Limitations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- American Academy of Sleep Medicine. International Classification of Sleep Disorders, 3rd ed.; American Academy of Sleep Medicine: Darien, IL, USA, 2014. [Google Scholar]
- Orphanet: Narcolepsy (ORPHA:619284). Available online: https://www.orpha.net/consor/cgibin/Disease_Search.php?lng=EN&data_id=10493&disease=Rare-sleep-disorder&search=Disease_Search_Simple (accessed on 4 January 2023).
- Schenck, C.H.; Bassetti, C.L.; Arnulf, I.; Mignot, E. English translations of the first clinical reports on narcolepsy and cataplexy by Westphal and Gélineau in the late 19th century, with commentary. J. Clin. Sleep Med. 2007, 3, 301–311. [Google Scholar] [CrossRef] [PubMed]
- Mignot, E.J. History of narcolepsy at Stanford University. Immunol. Res. 2014, 58, 315–339. [Google Scholar] [CrossRef] [PubMed]
- Guilleminault, C.; Huang, Y.S.; Lin, C.M. Narcolepsy syndrome: A new view at the beginning of the second millennium. In Clinical Pharmacology of Sleep; Pandi-Perumal, S.R., Monti, J.M., Eds.; Birkhäuser Basel: Basel, Switzerland, 2006. [Google Scholar] [CrossRef]
- Daniels, L.E. Narcolepsy. Medicine 1934, 13, 1–122. [Google Scholar] [CrossRef]
- Yoss, R.E.; Daly, D. Criteria for the diagnosis of the narcoleptic syndrome. Proc. Staff. Meet. Mayo Clin. 1957, 32, 320–328. [Google Scholar] [PubMed]
- Fromherz, S.; Mignot, E. Narcolepsy research: Past, present, and future perspectives. Arch. Ital. Biol. 2004, 142, 479–486. [Google Scholar] [PubMed]
- Longstreth, W.T., Jr.; Koepsell, T.D.; Ton, T.G.; Hendrickson, A.F.; van Belle, G. The epidemiology of narcolepsy. Sleep 2007, 30, 13–26. [Google Scholar] [CrossRef]
- Kornum, B.; Knudsen, S.; Ollila, H.; Pizza, F.; Jennum, P.J.; Dauvilliers, Y.; Overeem, S. Narcolepsy. Nat. Rev. Dis. Primers 2017, 3, 16100. [Google Scholar] [CrossRef] [PubMed]
- Ohayon, M.M.; Priest, R.G.; Zulley, J.; Smirne, S.; Paiva, T. Prevalence of narcolepsy symptomatology and diagnosis in the European general population. Neurology 2002, 58, 1826–1833. [Google Scholar] [CrossRef]
- Heier, M.S.; Evsiukova, T.; Wilson, J.; Abdelnoor, M.; Hublin, C.; Ervick, S. Prevalence of narcolepsy with cataplexy in Norway. Acta Neurol. Scand. 2009, 120, 276–280. [Google Scholar] [CrossRef] [PubMed]
- Hublin, C.; Kaprio, J.; Partinen, M.; Kokenvuo, M.; Heikkila, K.; Koskimies, S.; Guilleminault, C. The prevalence of narcolepsy: An epidemiological study of the Finnish Twin Cohort. Ann. Neurol. 1994, 35, 709–716. [Google Scholar] [CrossRef] [PubMed]
- Doherty, L.; Crowe, C.; Sweeney, B. National narcolepsy survey. Ir. Med. J. 2010, 103, 112–113. [Google Scholar]
- Roth, B. Narcolepsy and Hypersomnia; Broughton, R., Translator; Karger: New York, NY, USA, 1980; Chapter 10; pp. 94–100. [Google Scholar]
- Tió, E.; Gaig, C.; Giner-Soriano, M.; Romero, O.; Jurado, M.J.; Sansa, G.; Pujol, M.; Sans, O.; Álvarez-Guerrico, I.; Caballol, N.; et al. The prevalence of narcolepsy in Catalunya (Spain). J. Sleep Res. 2018, 27, e12640. [Google Scholar] [CrossRef] [PubMed]
- Lavie, P.; Peled, R. Letter to the Editor: Narcolepsy is a Rare Disease in Israel. Sleep 1987, 10, 608–609. [Google Scholar] [PubMed]
- Tashiro, T.; Kanbayashi, T.; Iijima, S.; Hishikawa, Y. An epidemiological study of narcolepsy in Japanese (abstract). J. Sleep Res. 1992, 1, 228. [Google Scholar]
- Imanishi, A.; Kamada, Y.; Shibata, K.; Sakata, Y.; Munakata, H.; Ishii, M. Prevalence, incidence, and medications of narcolepsy in Japan: A descriptive observational study using a health insurance claims database. Sleep Biol. Rhythms 2022, 20, 585–594. [Google Scholar] [CrossRef]
- Park, H.R.; Song, P.; Lee, S.Y.; on behalf of Epidemiology Committee of Korean Sleep Research. National Estimates of Narcolepsy in Korea. J. Clin. Neurol. 2023, 19, 83–89. [Google Scholar] [CrossRef] [PubMed]
- Wing, Y.K.; Li, R.H.; Lam, C.W.; Ho, C.K.; Fong, S.Y.; Leung, T. The prevalence of narcolepsy among Chinese in Hong Kong. Ann. Neurol. 2002, 51, 578–584. [Google Scholar] [CrossRef] [PubMed]
- Han, F.; Chen, E.; Wei, H.; Dong, X.; He, Q.; Ding, D.; Strohl, K.P. Childhood narcolepsy in North China. Sleep 2001, 24, 321–324. [Google Scholar] [CrossRef] [PubMed]
- Solomon, P. Narcolepsy in Negroes. Dis. Nerv. Sys. 1945, 6, 179–183. [Google Scholar]
- Dement, W.C.; Carskadon, M.; Ley, R. The prevalence of narcolepsy II. Sleep Res. 1973, 2, 147. [Google Scholar]
- Silber, M.H.; Krahn, L.E.; Olson, E.J.; Pankratz, V.S. The epidemiology of narcolepsy in Olmsted County, Minnesota: A population-based study. Sleep 2002, 25, 197–202. [Google Scholar] [CrossRef]
- Scheer, D.; Schwartz, S.W.; Parr, M.; Zgibor, J.; Sanchez-Anguiano, A.; Rajaram, L. Prevalence and incidence of narcolepsy in a US health care claims database, 2008–2010. Sleep 2019, 42, zsz091. [Google Scholar] [CrossRef] [PubMed]
- Acquavella, J.; Mehra, R.; Bron, M.; Suomi, J.M.-H.; Hess, G.P. Prevalence of narcolepsy, other sleep disorders, and diagnostic tests from 2013–2016: Insured patients actively seeking care. J. Clin. Sleep Med. 2020, 16, 1255–1263. [Google Scholar] [CrossRef] [PubMed]
- Al Rajeh, S.; Bademosi, O.; Ismail, H.; Awada, A.; Dawodu, A.; Al-Freihi, H.; Assuhaimi, S.; Borollosi, M.; Al-Shammasi, S. A community survey of neurological disorders in Saudi Arabia: The Thugbah study. Neuroepidemiology 1993, 12, 164–178. [Google Scholar] [CrossRef] [PubMed]
- Partinen, M.; Saarenpää-Heikkilä, O.; Ilveskoski, I.; Hublin, C.; Linna, M.; Olsén, P.; Nokelainen, P.; Alén, R.; Wallden, T.; Espo, M. Increased incidence and clinical picture of childhood narcolepsy following the 2009 H1N1 pandemic vaccination campaign in Finland. PLoS ONE 2012, 7, e33723. [Google Scholar] [CrossRef] [PubMed]
- Heier, M.S.; Gautvik, K.M.; Wannag, E.; Bronder, K.H.; Midtlyng, E.; Kamaleri, Y.; Storsaeter, J. Incidence of narcolepsy in Norwegian children and adolescents after vaccination against H1N1 influenza A. Sleep Med. 2013, 14, 867–871. [Google Scholar] [CrossRef]
- Szakács, A.; Darin, N.; Hallböök, T. Increased childhood incidence of narcolepsy in Western Sweden after H1N1 influenza vaccination. Neurology 2013, 80, 1315–1321. [Google Scholar] [CrossRef]
- Wijnans, L.; Lecomte, C.; de Vries, C.; Weibel, D.; Sammon, C.; Hviid, A.; Svanstrom, H.; Molgaard-Nielsen, D.; Heijbel, H.; Dahlstrom, L.A. The incidence of narcolepsy in Europe: Before, during, and after the influenza A(H1N1) pdm09 pandemic and vaccination campaigns. Vaccine 2013, 31, 1246–1254. [Google Scholar] [CrossRef] [PubMed]
- Han, F.; Lin, L.; Warby, S.C.; Faraco, J.; Li, J.; Dong, S.X.; An, P.; Zhao, L.; Wang, L.H.; Li, Q.Y. Narcolepsy onset is seasonal and increased following the 2009 H1N1 pandemic in China. Ann. Neurol. 2011, 70, 410–417. [Google Scholar] [CrossRef] [PubMed]
- Wu, H.; Zhuang, J.; Stone, W.S.; Zhang, L.; Zhao, Z.; Wang, Z.; Yang, Y.; Li, X.; Zhao, X.; Zhao, Z. Symptoms, and occurrences of narcolepsy: A retrospective study of 162 patients during a 10-year period in Eastern China. Sleep Med. 2014, 15, 607–613. [Google Scholar] [CrossRef]
- Choe, Y.J.; Bae, G.R.; Lee, D.H. No association between influenza A(H1N1)pdm09 vaccination and narcolepsy in South Korea: An ecological study. Vaccine 2012, 30, 7439–7442. [Google Scholar] [CrossRef] [PubMed]
- Duffy, J.; Weintraub, E.; Vellozzi, C.; DeStefano, F. Vaccine Safety Datalink. Narcolepsy and influenza A(H1N1) pandemic 2009 vaccination in the United States. Neurology 2014, 83, 1823–1830. [Google Scholar] [CrossRef] [PubMed]
- Weibel, D.; Sturkenboom, M.; Black, S.; de Ridder, M.; Dodd, C.; Bonhoeffer, J.; Vanrolleghem, A.; van der Maas, N.; Lammers, G.J.; Overeem, S. Narcolepsy and adjuvanted pandemic influenza A (H1N1) 2009 vaccines: Multi-country assessment. Vaccine 2018, 36, 6202–6211. [Google Scholar] [CrossRef] [PubMed]
- Spruyt, K. Narcolepsy Presentation in Diverse Populations: An Update. Curr. Sleep Med. Rep. 2020, 6, 239–250. [Google Scholar] [CrossRef] [PubMed]
- Avidan, A.Y. Sleep and Its Disorders Chapter 101 in Bradley and Daroff’s Neurology in Clinical Practice, 8th ed.; Elsevier: Amsterdam, The Netherlands, 2022; pp. 1664–1744. [Google Scholar]
- Dauvilliers, Y.; Montplaisir, J.; Molinari, N.; Carlander, B.; Ondze, B.; Besset, A.; Billiard, M. Age at onset of narcolepsy in two large populations of patients in France and Quebec. Neurology 2001, 57, 2029–2033. [Google Scholar] [CrossRef] [PubMed]
- Chemelli, R.M.; Willie, J.T.; Sinton, C.M.; Elmquist, J.K.; Scammell, T.; Lee, C.; Richardson, J.A.; Williams, S.C.; Xiong, Y.; Kisanuki, Y. Narcolepsy in orexin knockout mice: Molecular genetics of sleep regulation. Cell 1999, 98, 437–451. [Google Scholar] [CrossRef]
- Diniz Behn, C.G.; Klerman, E.B.; Mochizuki, T.; Lin, S.C.; Scammell, T.E. Abnormal sleep/wake dynamics in orexin knockout mice. Sleep 2010, 33, 297–306. [Google Scholar] [CrossRef] [PubMed]
- Mignot, E.; Lammers, G.J.; Ripley, B.; Okun, M.; Nevsimalova, S.; Overeem, S.; Vankova, J.; Black, J.; Harsh, J.; Bassetti, C. The role of cerebrospinal fluid hypocretin measurement in the diagnosis of narcolepsy and other hypersomnias. Arch. Neurol. 2002, 59, 1553–1562. [Google Scholar] [CrossRef] [PubMed]
- Thannickal, T.; Moore, C.; Nienhuis, R.Y.; Ramanathan, R.; Gulyani, S.; Aldrich, M.; Cornford, M.; Siegel, J.M. Reduced number of hypocretin neurons in human narcolepsy. Neuron 2000, 27, 469–474. [Google Scholar] [CrossRef]
- Peyron, C.; Faraco, J.; Rogers, W.; Ripley, B.; Overeem, S.; Charnay, Y.; Nevsimalova, S.; Aldrich, M.; Reynolds, D.; Albin, R. A mutation in a case of early onset narcolepsy and a generalized absence of hypocretin peptides in human narcoleptic brains. Nat. Med. 2000, 6, 991–997. [Google Scholar] [CrossRef] [PubMed]
- Valko, P.O.; Gavrilov, Y.V.; Yamamoto, M.; Reddy, H.; Haybaeck, J.; Mignot, E.; Baumann, C.R.; Scammell, T.E. Increase of histaminergic tuberomammillary neurons in narcolepsy. Ann. Neurol. 2013, 74, 794–804. [Google Scholar] [CrossRef]
- John, J.; Thannickal, T.C.; McGregor, R.; Ramanathan, L.; Ohtsu, H.; Nishino, S.; Sakai, N.; Yamanaka, A.; Stone, C.; Cornford, M.; et al. Greatly increased numbers of histamine cells in human narcolepsy with cataplexy. Ann Neurol. 2013, 74, 786–793. [Google Scholar] [CrossRef] [PubMed]
- Hor, H.; Bartesaghi, L.; Kutalik, Z.; Vicário, J.L.; de Andrés, C.; Pfister, C.; Lammers, G.J.; Guex, N.; Chrast, R.; Tafti, M.; et al. A missense mutation in myelin oligodendrocyte glycoprotein as a cause of familial narcolepsy with cataplexy. Am. J. Hum. Genet. 2011, 89, 474–479, Erratum in Am. J. Hum. Genet. 2012, 91, 396. [Google Scholar] [CrossRef]
- Narcolepsy 1. Available online: https://www.omim.org/entry/161400?search=narcolepsy&highlight=narcolepsy%20narcoleptic#31 (accessed on 23 January 2023).
- Mignot, E. Genetic and familial aspects of narcolepsy. Neurology 1998, 50 (Suppl. S1), S16–S22. [Google Scholar] [CrossRef]
- Winkelmann, J.; Lin, L.; Schormair, B.; Kornum, B.R.; Faraco, J.; Plazzi, G.; Melberg, A.; Cornelio, F.; Urban, A.E.; Pizza, F.; et al. Mutations in DNMT1 cause autosomal dominant cerebellar ataxia, deafness, and narcolepsy. Hum. Mol. Genet. 2012, 21, 2205–2210. [Google Scholar] [CrossRef] [PubMed]
- Miyagawa, T.; Tokunaga, K. Genetics of narcolepsy. Hum. Genome Var. 2019, 6, 4. [Google Scholar] [CrossRef]
- Kawashima, M.; Tamiya, G.; Oka, A.; Hohjoh, H.; Juji, T.; Ebisawa, T.; Honda, Y.; Inoko, H.; Tokunaga, K. Genomewide association analysis of human narcolepsy and a new resistance gene. Am. J. Hum. Genet. 2006, 79, 252–263. [Google Scholar] [CrossRef]
- Lin, L.; Hungs, M.; Mignot, E. Narcolepsy and the HLA region. J. Neuroimmunol. 2001, 117, 9–20. [Google Scholar] [CrossRef]
- Hor, H.; Bartesaghi, L.; Kutalik, Z.; Vicário, J.L.; de Andrés, C.; Pfister, C.; Lammers, G.J.; Guex, N.; Chrast, R.; Tafti, M.; et al. Genome-wide association study identifies new HLA class II haplotypes strongly protective against narcolepsy. Nat. Genet. 2010, 42, 786–789. [Google Scholar] [CrossRef] [PubMed]
- Mignot, E.; Lin, L.; Rogers, W.; Honda, Y.; Qiu, X.; Lin, X.; Okun, M.; Hohjoh, H.; Miki, T.; Hsu, S.H. Complex HLA-DR and -DQ interactions confer risk of narcolepsy-cataplexy in three ethnic groups. Am. J. Hum. Genet. 2001, 68, 686–699. [Google Scholar] [CrossRef] [PubMed]
- Yong, E. Narcolepsy confirmed as autoimmune disease. Nature 2013. [Google Scholar] [CrossRef]
- Martinez-Orozco, F.J.; Vicario, J.L.; De Andres, C.; Fernandez-Arquero, M.; Peraita-Adrados, R. Comorbidity of Narcolepsy Type 1 With Autoimmune Diseases and Other Immunopathological Disorders: A Case-Control Study. J. Clin. Med. Res. 2016, 8, 495–505. [Google Scholar] [CrossRef] [PubMed]
- Kornum, B.R.; Kawashima, M.; Faraco, J.; Lin, L.; Rico, T.J.; Hesselson, S.; Axtell, R.C.; Kuipers, H.; Weiner, K.; Hamacher, A. Common variants in P2RY11 are associated with narcolepsy. Nat. Genet. 2011, 43, 66–71. [Google Scholar] [CrossRef] [PubMed]
- Hallmayer, J.; Faraco, J.; Lin, L.; Hesselson, S.; Winkelmann, J.; Kawashima, M.; Mayer, G.; Plazzi, G.; Nevsimalova, S.; Bourgin, P.; et al. Narcolepsy is strongly associated with the T-cell receptor alpha locus. Nat. Genet. 2009, 41, 708–711. [Google Scholar] [CrossRef] [PubMed]
- Latorre, D.; Kallweit, U.; Armentani, E.; Foglierini, M.; Mele, F.; Cassotta, A.; Jovic, S.; Jarrossay, D.; Mathis, J.; Zellini, F. T cells in patients with narcolepsy target self-antigens of hypocretin neurons. Nature 2018, 562, 63–68. [Google Scholar] [CrossRef] [PubMed]
- Pedersen, N.W.; Holm, A.; Kristensen, N.P.; Bjerregaard, A.-M.; Bentzen, A.K.; Marquard, A.M.; Tamhane, T.; Burgdorf, K.S.; Ullum, H.; Jennum, P. CD8+ T cells from patients with narcolepsy and healthy controls recognize hypocretin neuron-specific antigens. Nat. Commun. 2019, 10, 837. [Google Scholar] [CrossRef] [PubMed]
- WebMD—Narcolepsy vs. Insomnia: What’s the Difference? Available online: https://www.webmd.com/sleep-disorders/narcolepsy-insomnia-difference (accessed on 26 April 2023).
- Roberts, H.J. The syndrome of narcolepsy and diabetogenic (“functional”) hyperinsulinism, with special reference to obesity, diabetes, idiopathic oedema, cerebral dysrhythmias, and multiple sclerosis (200 patients). J. Am. Geriatr. Soc. 1964, 12, 926–976. [Google Scholar] [CrossRef]
- Dahmen, N.; Bierbrauer, J.; Kasten, M. Increased prevalence of obesity in narcoleptic patients and relatives. Eur. Arch. Psychiatry Clin. Neurosci. 2001, 251, 85–89. [Google Scholar] [CrossRef] [PubMed]
- Straat, M.E.; Schinkelshoek, M.S.; Fronczek, R.; Lammers, G.J.; Rensen, P.C.N.; Boon, M.R. Role of Brown Adipose Tissue in Adiposity Associated with Narcolepsy Type 1. Front. Endocrinol. 2020, 11, 145. [Google Scholar] [CrossRef] [PubMed]
- Seifinejad, A.; Ramosaj, M.; Shan, L.; Possovre, M.-L.; Pfister, C.; Fronczek, R.; Garrett-Shnha, L.A.; Frieser, D.; Honda, M.; Arribat, Y. Epigenetic silencing of selected hypothalamic neuropeptides in narcolepsy with cataplexy. Proc. Natl. Acad. Sci. USA 2023, 120, e2220911120. [Google Scholar] [CrossRef]
- Billiard, M.; Orellana, C. Chapter 40 Environmental Factors in Narcolepsy in Narcolepsy and Hypersomnia, 1st ed.; Bassetti, C., Billiard, M., Mignot, E., Eds.; CRC Press: Boca Raton, FL, USA, 2007. [Google Scholar]
- Viola-Saltzman, M.; Musleh, C. Traumatic brain injury-induced sleep disorders. Neuropsychiatr. Dis. Treat. 2016, 12, 339–348. [Google Scholar] [CrossRef] [PubMed]
- Thannickal, T.C.; Nienhuis, R.; Siegel, J.M. Localized loss of hypocretin (orexin) cells in narcolepsy without cataplexy. Sleep 2009, 32, 993–998. [Google Scholar] [CrossRef] [PubMed]
- Baumann-Vogel, H.; Schreckenbauer, L.; Valko, P.O.; Werth, E.; Baumann, C.R. Narcolepsy type 2: A rare, yet existing entity. J. Sleep Res. 2021, 30, e13203. [Google Scholar] [CrossRef]
- The National Health Service: Narcolepsy. Available online: https://www.nhs.uk/conditions/narcolepsy/symptoms/ (accessed on 10 January 2023).
- Morse, A.M. Narcolepsy in Children and Adults: A Guide to Improved Recognition, Diagnosis and Management. Available online: https://www.mendeley.com/catalogue/2a501988-2588-338f-83be-50c64f067366/ (accessed on 10 January 2023).
- Wang, Y.G.; Benmedjahed, K.; Lambert, J.; Evans, C.J.; Hwang, S.; Black, J.; Johns, M.W. Assessing Narcolepsy with Cataplexy in Children and Adolescents: Development of a Cataplexy Diary and the ESS-CHAD. Available online: https://www.mendeley.com/catalogue/fd022331-f7c2-312f-8b41-2085cc51c92b/ (accessed on 11 January 2023).
- American Psychiatric Association. Sleep-wake disorders. In Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Association: Washington, DC, USA, 2013; pp. 361–422. [Google Scholar]
- Orphanet: Narcolepsy Type 1 (ORPHA:2073). Available online: https://www.orpha.net/consor/cgi-bin/Disease_Search.php?lng=EN&data_id=3637&Disease_Disease_Search_diseaseGroup=narcolepsy&Disease_Disease_Search_diseaseType=Pat&Disease(s)/group%20of%20diseases=Narcolepsy-type-1&title=Narcolepsy%20type%201&search=Disease_Search_Simple (accessed on 14 January 2023).
- Ruoff, C.; Rye, D. The ICSD-3 and DSM-5 guidelines for diagnosing narcolepsy: Clinical relevance and practicality. Curr. Med. Res. Opin. 2016, 32, 1611–1622. [Google Scholar] [CrossRef]
- Sateia, M.J. International classification of sleep disorders-third edition: Highlights and modifications. Chest 2014, 146, 1387–1394. [Google Scholar] [CrossRef] [PubMed]
- Li, S.-B.; de Lecea, L. The hypocretin (orexin) system: From a neural circuitry perspective. Neuropharmacology 2020, 167, 107993. [Google Scholar] [CrossRef] [PubMed]
- Ebrahim, I.O.; Howard, R.S.; Kopelman, M.D.; Sharief, M.K.; Williams, A.J. The hypocretin/orexin system. J. R. Soc. Med. 2002, 95, 227–230. [Google Scholar] [CrossRef] [PubMed]
- Nishino, S.; Sakurai, E.; Nevsimalova, S.; Yoshida, Y.; Watanabe, T.; Yanai, K.; Mignot, E. Decreased CSF histamine in narcolepsy with and without low CSF hypocretin-1 in comparison to healthy controls. Sleep 2009, 32, 175–180. [Google Scholar] [CrossRef]
- Krahn, L.E.; Zee, P.C.; Thorpy, M.J. Current Understanding of Narcolepsy 1 and its Comorbidities: What Clinicians Need to Know. Adv. Ther. 2022, 39, 221–243. [Google Scholar] [CrossRef]
- Babiker, M.O.; Prasad, M. Narcolepsy in children: A diagnostic and management approach. Pediatr. Neurol. 2015, 52, 557–565. [Google Scholar] [CrossRef]
- Zhang, M.; Thieux, M.; Inocente, C.O.; Vieux, N.; Arvis, L.; Villanueva, C.; Lin, J.S.; Plancoulaine, S.; Guyon, A.; Franco, P. Characterization of rapid weight gain phenotype in children with narcolepsy. CNS Neurosci. Ther. 2022, 28, 829–841. [Google Scholar] [CrossRef] [PubMed]
- Chung, I.-H.; Chin, W.-C.; Huang, Y.-S.; Wang, C.-H. Pediatric Narcolepsy—A Practical Review. Children 2022, 9, 974. [Google Scholar] [CrossRef] [PubMed]
- Narcolepsy Fact Sheet. Available online: https://www.ninds.nih.gov/health-information/patient-caregiver-education/fact-sheets/narcolepsy-fact-sheet#3201_6 (accessed on 14 January 2023).
- Andlauer, O.; Moore, H., 4th; Hong, S.C.; Dauvilliers, Y.; Kanbayashi, T.; Nishino, S.; Han, F.; Silber, M.H.; Rico, T.; Einen, M.; et al. Predictors of hypocretin (orexin) deficiency in narcolepsy without cataplexy. Sleep 2012, 35, 1247–1255. [Google Scholar] [CrossRef] [PubMed]
- Andlauer, O.; Moore, H.; Jouhier, L.; Drake, C.; Peppard, P.E.; Han, F.; Hong, S.C.; Poli, F.; Plazzi, G.; O’Hara, R.; et al. Nocturnal rapid eye movement sleep latency for identifying patients with narcolepsy/hypocretin deficiency. JAMA Neurol. 2013, 70, 891–902, Erratum in JAMA Neurol. 2013, 70, 1332. [Google Scholar] [CrossRef] [PubMed]
- Maeda, M.; Tamaoka, A.; Hayashi, A.; Mizusawa, H.; Shoji, S. A case of HLA-DR2, DQw1 negative post-traumatic narcolepsy. Rinsho Shinkeigaku=Clin. Neurol. 1995, 35, 811–813. [Google Scholar]
- Berry, R.B. Chapter 14—Subjective and Objective Measures of Daytime Sleepiness. In Fundamentals of Sleep Medicine; Saunders, W.B., Ed.; Elsevier: Amsterdam, The Netherlands, 2012; pp. 219–235. ISBN 9781437703269. [Google Scholar] [CrossRef]
- Arand, D.; Bonnet, M.; Hurwitz, T.; Mitler, M.; Rosa, R.; Sangal, R.B. A review by the MSLT and MWT-Task Force of the Standards of Practice Committee of the AASM. The clinical use of the MSLT and MWT. Sleep 2005, 28, 123–144. [Google Scholar] [CrossRef]
- Smit, L.S.; Lammers, G.J.; Catsman-Berrevoets, C.E. Cataplexy leading to the diagnosis of Niemann-Pick disease type C. Pediatr. Neurol. 2006, 35, 82–84. [Google Scholar] [CrossRef]
- Ebrahim, I.O.; Peacock, K.W.; Williams, A.J. Posttraumatic narcolepsy—Two case reports and a mini review. J. Clin. Sleep Med. 2005, 1, 153–156. [Google Scholar] [CrossRef]
- Division of Sleep Medicine: Harvard Medical School. Available online: https://healthysleep.med.harvard.edu/narcolepsy/living-with-narcolepsy/dailylife (accessed on 14 January 2023).
- MedScape. Available online: https://emedicine.medscape.com/article/1188433-overview#a6 (accessed on 16 January 2023).
- Ahmed, I.; Thorpy, M. Clinical features, diagnosis, and treatment of narcolepsy. Clin. Chest. Med. 2010, 31, 371–381. [Google Scholar] [CrossRef]
- Rundo, J.V.; Downey, R., 3rd. Polysomnography. Handb. Clin. Neurol. 2019, 160, 381–392. [Google Scholar] [CrossRef]
- Amira, S.A.; Johnson, T.S.; Logowitz, N.B. Diagnosis of narcolepsy using the multiple sleep latency test: Analysis of current laboratory criteria. Sleep 1985, 8, 325–331. [Google Scholar] [CrossRef] [PubMed]
- Berry, R.B. Chapter 13—Polysomnography, Portable Monitoring, and Actigraphy. In Fundamentals of Sleep Medicine; Saunders, W.B., Ed.; Elsevier: Amsterdam, The Netherlands, 2012; pp. 189–218. ISBN 9781437703269. [Google Scholar] [CrossRef]
- Prinzmetal, M.; Bloomberg, W. The Use of Benzedrine for the Treatment of Narcolepsy. JAMA 1935, 105, 2051–2054. [Google Scholar] [CrossRef]
- Billiard, M.; Bassetti, C.; Dauvilliers, Y.; Dolenc-Groselj, L.; Lammers, G.J.; Mayer, G.; Pollmächer, T.; Reading, P.; Sonka, K. EFNS guidelines on management of narcolepsy. Eur. J. Neurol. 2006, 13, 1035–1048. [Google Scholar] [CrossRef] [PubMed]
- Morgenthaler, T.I.; Kapur, V.K.; Brown, T.M.; Swick, T.J.; Alessi, C.; Aurora, R.N.; Boehlecke, B.; Chesson, A.L., Jr.; Friedman, L.; Maganti, R.; et al. Practice parameters for the treatment of narcolepsy and other hypersomnias of central origin. Sleep 2007, 30, 1705–1711. [Google Scholar] [CrossRef] [PubMed]
- Golden, E.C.; Lipford, M.C. Narcolepsy: Diagnosis and management. Cleve Clin. J. Med. 2018, 85, 959–969. [Google Scholar] [CrossRef] [PubMed]
- Narcolepsy. Available online: https://www.nhs.uk/conditions/narcolepsy/treatment/ (accessed on 3 February 2023).
- Bassetti, C.L.A.; Adamantidis, A.; Burdakov, D.; Han, F.; Gay, S.; Kallweit, U.; Khatami, R.; Koning, F.; Kornum, B.R.; Lammers, G.J.; et al. Narcolepsy—clinical spectrum, aetiopathophysiology, diagnosis and treatment. Nat. Rev. Neurol. 2019, 15, 519–539. [Google Scholar] [CrossRef] [PubMed]
- Bassetti, C.L.A.; Kallweit, U.; Vignatelli, L.; Plazzi, G.; Lecendreux, M.; Baldin, E.; Dolenc-Groselj, L.; Jennum, P.; Khatami, R.; Manconi, M.; et al. European guideline, and expert statements on the management of narcolepsy in adults and children. J. Sleep Res. 2021, 30, e13387. [Google Scholar] [CrossRef]
- Mignot, E.J. A practical guide to the therapy of narcolepsy and hypersomnia syndromes. Neurotherapeutics 2012, 9, 739–752. [Google Scholar] [CrossRef]
- Franceschini, C.; Pizza, F.; Antelmi, E.; Folli, M.C.; Plazzi, G. Narcolepsy treatment: Pharmacological and behavioral strategies in adults and children. Sleep Breath. 2020, 24, 615–627. [Google Scholar] [CrossRef]
- Scammell, T.E.; Estabrooke, I.V.; McCarthy, M.T.; Chemelli, R.M.; Yanagisawa, M.; Miller, M.S.; Saper, C.B. Hypothalamic Arousal Regions Are Activated during Modafinil-Induced Wakefulness. J. Neurosci. 2000, 20, 8620–8628. [Google Scholar] [CrossRef]
- Barateau, L.; Dauvilliers, Y. Recent advances in treatment for narcolepsy. Ther. Adv. Neurol. Disord. 2019, 12, 1756286419875622. [Google Scholar] [CrossRef] [PubMed]
- Chabas, D.; Foulon, C.; Gonzalez, J.; Nasr, M.; Lyon-Caen, O.; Willer, J.C.; Derenne, J.P.; Arnulf, I. Eating disorder and metabolism in narcoleptic patients. Sleep 2007, 30, 1267–1273. [Google Scholar] [CrossRef] [PubMed]
- Barateau, L.; Lopez, R.; Dauvilliers, Y. Treatment Options for Narcolepsy. CNS Drugs 2016, 30, 369–379. [Google Scholar] [CrossRef] [PubMed]
- Drake, C.; Roehrs, T.; Shambroom, J.; Roth, T. Caffeine effects on sleep taken 0, 3, or 6 hours before going to bed. J. Clin. Sleep Med. 2013, 9, 1195–1200. [Google Scholar] [CrossRef] [PubMed]
- Narcolepsy. Available online: https://www.mayoclinic.org/diseases-conditions/narcolepsy/diagnosis-treatment/drc-20375503#:~:text=Stimulants.,habit%2Dforming%20as%20older%20stimulants (accessed on 30 January 2023).
- Matoulek, M.; Tuka, V.; Fialová, M.; Nevšímalová, S.; Šonka, K. Cardiovascular fitness in narcolepsy is inversely related to sleepiness and the number of cataplexy episodes. Sleep Med. 2017, 34, 7–12. [Google Scholar] [CrossRef] [PubMed]
- Syed, Y.Y. Pitolisant: First Global Approval. Drugs 2016, 76, 1313–1318. [Google Scholar] [CrossRef] [PubMed]
- Lamb, Y.N. Pitolisant: A Review in Narcolepsy with or without Cataplexy. CNS Drugs 2020, 34, 207–218. [Google Scholar] [CrossRef] [PubMed]
- Dominguez, A.; Soca Gallego, L.; Parmar, M. Sodium Oxybate; [Updated 2023 Jan 17]; StatPearls: Treasure Island, FL, USA, 2023. Available online: https://www.ncbi.nlm.nih.gov/books/NBK562283/ (accessed on 1 February 2023).
- Drugs and Supplements: Sodium Oxybate (Oral Route). Available online: https://www.mayoclinic.org/drugs-supplements/sodium-oxybate-oral-route/side-effects/drg-20067727 (accessed on 22 February 2023).
- My Life with Narcolepsy. Available online: https://sleepeducation.org/life-with-narcolepsy/ (accessed on 16 January 2023).
- Franceschini, C.; Fante, C.; Filardi, M.; Folli, M.C.; Brazzi, F.; Pizza, F.; D’Anselmo, A.; Ingravallo, F.; Antelmi, E.; Plazzi, G. Can a Peer Support the Process of Self-Management in Narcolepsy? A Qualitative Narrative Analysis of a Narcoleptic Patient. Front. Psychol. 2020, 11, 1353. [Google Scholar] [CrossRef] [PubMed]
- Daily Life. Available online: https://sleep.hms.harvard.edu/education-training/public-education/sleep-and-health-education-program/sleep-health-education-5 (accessed on 26 January 2003).
- Schiappa, C.; Scarpelli, S.; D’Atri, A.; Gorgoni, M.; De Gennaro, L. Narcolepsy, and emotional experience: A review of the literature. Behav. Brain Funct. 2018, 14, 19. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Population/Country | Prevalence (%) | Authors, Year of Publication |
|---|---|---|
| Europe (Five-country study: UK, Germany, Italy, Portugal, and Spain) | 0.047 | Ohayon et al., 2002 [11] |
| Norway | 0.022 | Heier et al., 2009 [12] |
| Finland (twin cohort) | 0.026 | Hublin et al., 1994 [13] |
| Ireland | 0.005 | Doherty et al., 2010 [14] |
| Czechoslovakia | 0.02–0.03 | Roth B., 1980 [15] |
| Spain (Catalunya) | 0.0052 | Tio et al., 2017 [16] |
| Israel | 0.002 | Lavie and Peled, 1987 [17] |
| Japan | 0.16–0.59 0.0185 | Tashiro et al., 1992 [18] Imanishi et al., 2022 [19] |
| Korea | 0.0084 | Park et al., 2023 [20] |
| Hong Kong | 0.034 | Wing et al., 2002 [21] |
| China | 0.04 (among children and adolescents) | Han et al., 2001 [22] |
| USA | 0.02–0.0794 | [23,24,25,26,27] |
| Phenotype | Gene/Locus | Location |
|---|---|---|
| Narcolepsy 2 | NRCLP2 | 4p13-q21 |
| Narcolepsy 7 | MOG | 6p22.1 |
| Narcolepsy 5 | NRCLP5 | 14q11.2 |
| Narcolepsy 1 | HCRT or NRCLP1 | 17q21.2 |
| Narcolepsy 6 | NRCLP6 | 19p13.2 |
| Narcolepsy 3 | NRCLP3 | 21q11.2 |
| Narcolepsy 4 | NRCLP4 | 22q13 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mațotă, A.-M.; Bordeianu, A.; Severin, E.; Jidovu, A. Exploring the Literature on Narcolepsy: Insights into the Sleep Disorder That Strikes during the Day. NeuroSci 2023, 4, 263-279. https://doi.org/10.3390/neurosci4040022
Mațotă A-M, Bordeianu A, Severin E, Jidovu A. Exploring the Literature on Narcolepsy: Insights into the Sleep Disorder That Strikes during the Day. NeuroSci. 2023; 4(4):263-279. https://doi.org/10.3390/neurosci4040022
Chicago/Turabian StyleMațotă, Ana-Maria, Andrei Bordeianu, Emilia Severin, and Alexandra Jidovu. 2023. "Exploring the Literature on Narcolepsy: Insights into the Sleep Disorder That Strikes during the Day" NeuroSci 4, no. 4: 263-279. https://doi.org/10.3390/neurosci4040022