
Non-Pharmacological Treatments of Cognitive Impairment in Multiple Sclerosis: A Review


Abstract
:1. Introduction
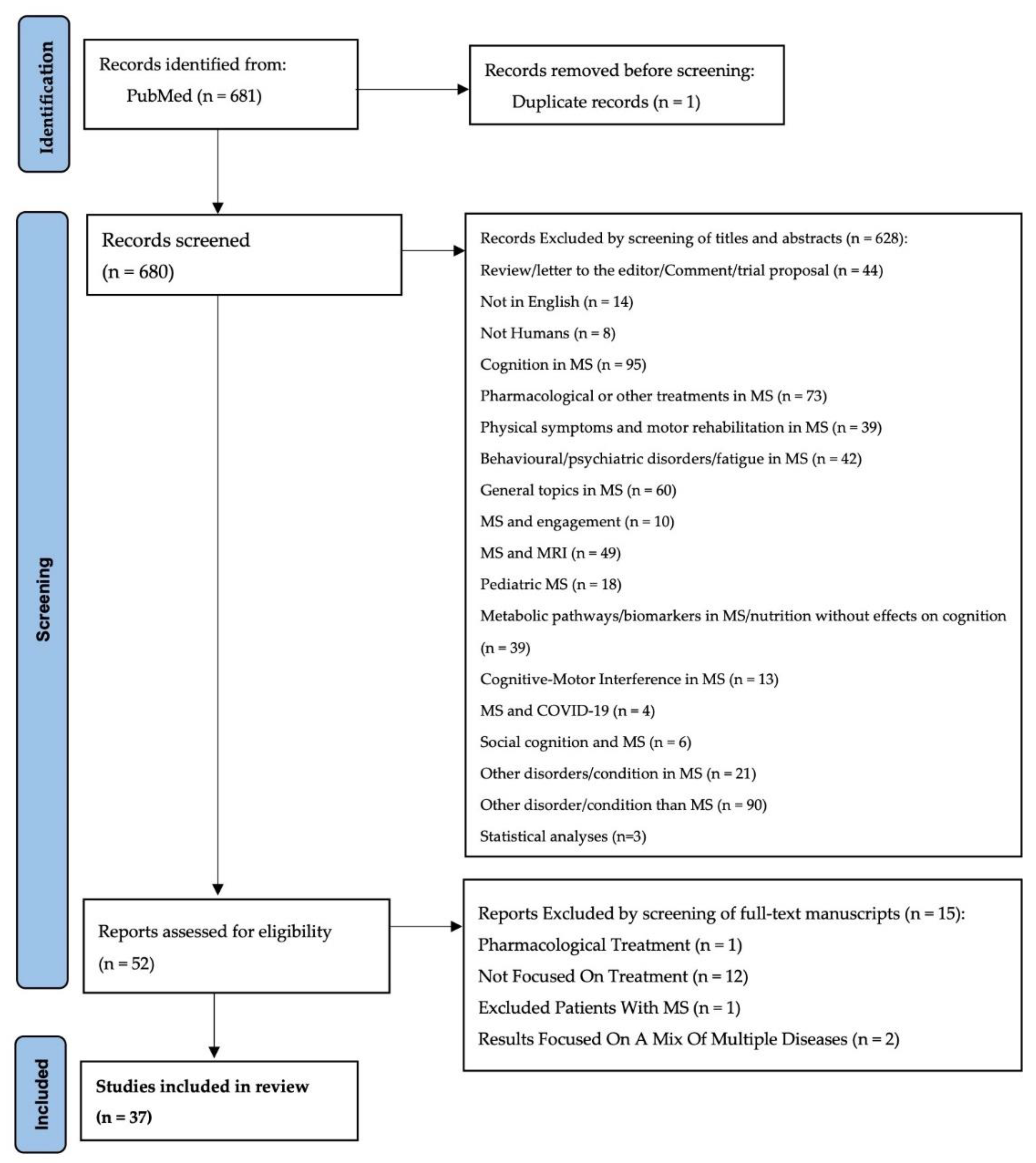
2. Materials and Methods
3. Results
- By screening titles and abstracts;
- By screening of full-text manuscripts.
3.1. Cognitive Rehabilitation
Computerized Cognitive Rehabilitation (CCR)
3.2. Exercise Training (ET)/Physical Activity (PA)
3.3. Non-Invasive Brain Stimulation and Brain Modulation
3.4. Other Interventions
4. Conclusions
- -
- Single session duration (from 20 min to 2 h);
- -
- Entire protocol duration (between 4 and 24 weeks);
- -
- Weekly frequency (2–5 times per week).
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Benedict, R.H.B.; Amato, M.P.; DeLuca, J.; Geurts, J.J.G. Cognitive Impairment in Multiple Sclerosis: Clinical Management, MRI, and Therapeutic Avenues. Lancet Neurol. 2020, 19, 860–871. [Google Scholar] [CrossRef]
- Chen, M.H.; Goverover, Y.; Genova, H.M.; DeLuca, J. Cognitive Efficacy of Pharmacologic Treatments in Multiple Sclerosis: A Systematic Review. CNS Drugs 2020, 34, 599–628. [Google Scholar] [CrossRef] [PubMed]
- Morrow, S.A.; Rosehart, H. Effects of Single Dose Mixed Amphetamine Salts—Extended Release on Processing Speed in Multiple Sclerosis: A Double Blind Placebo Controlled Study. Psychopharmacology 2015, 232, 4253–4259. [Google Scholar] [CrossRef] [PubMed]
- Cotter, J.; Muhlert, N.; Talwar, A.; Granger, K. Examining the Effectiveness of Acetylcholinesterase Inhibitors and Stimulant-Based Medications for Cognitive Dysfunction in Multiple Sclerosis: A Systematic Review and Meta-Analysis. Neurosci. Biobehav. Rev. 2018, 86, 99–107. [Google Scholar] [CrossRef] [PubMed]
- Chen, M.H.; Chiaravalloti, N.D.; DeLuca, J. Neurological Update: Cognitive Rehabilitation in Multiple Sclerosis. J. Neurol. 2021, 268, 4908–4914. [Google Scholar] [CrossRef] [PubMed]
- Brochet, B. Cognitive Rehabilitation in Multiple Sclerosis in the Period from 2013 and 2021: A Narrative Review. Brain Sci. 2021, 12, 55. [Google Scholar] [CrossRef]
- Taylor, L.A.; Mhizha-Murira, J.R.; Smith, L.; Potter, K.-J.; Wong, D.; Evangelou, N.; Lincoln, N.B.; das Nair, R. Memory Rehabilitation for People with Multiple Sclerosis. Cochrane Database Syst. Rev. 2021, 10, CD008754. [Google Scholar] [CrossRef]
- Mousavi, S.; Zare, H.; Etemadifar, M.; Taher Neshatdoost, H. Memory Rehabilitation for the Working Memory of Patients with Multiple Sclerosis (MS). J. Clin. Exp. Neuropsychol. 2018, 40, 405–410. [Google Scholar] [CrossRef]
- Mousavi, S.; Zare, H.; Etemadifar, M. Evaluating the Effectiveness of Cognitive Rehabilitation on Everyday Memory in Multiple Sclerosis Patients. Neuropsychol. Rehabil. 2020, 30, 1013–1023. [Google Scholar] [CrossRef]
- Turtola, Z.P.; Covey, T.J. Working Memory Training Impacts Neural Activity during Untrained Cognitive Tasks in People with Multiple Sclerosis. Exp. Neurol. 2021, 335, 113487. [Google Scholar] [CrossRef]
- Ernst, A.; Sourty, M.; Roquet, D.; Noblet, V.; Gounot, D.; Blanc, F.; de Seze, J.; Manning, L. Benefits from an Autobiographical Memory Facilitation Programme in Relapsing-Remitting Multiple Sclerosis Patients: A Clinical and Neuroimaging Study. Neuropsychol. Rehabil. 2018, 28, 1110–1130. [Google Scholar] [CrossRef] [PubMed]
- Brissart, H.; Omorou, A.Y.; Forthoffer, N.; Berger, E.; Moreau, T.; De Seze, J.; Morele, E.; Debouverie, M. Memory Improvement in Multiple Sclerosis after an Extensive Cognitive Rehabilitation Program in Groups with a Multicenter Double-Blind Randomized Trial. Clin. Rehabil. 2020, 34, 754–763. [Google Scholar] [CrossRef] [PubMed]
- Chiaravalloti, N.D.; Moore, N.B.; DeLuca, J. The Efficacy of the Modified Story Memory Technique in Progressive MS. Mult. Scler. 2020, 26, 354–362. [Google Scholar] [CrossRef] [PubMed]
- Chiaravalloti, N.D.; Moore, N.B.; Weber, E.; DeLuca, J. The Application of Strategy-Based Training to Enhance Memory (STEM) in Multiple Sclerosis: A Pilot RCT. Neuropsychol. Rehabil. 2021, 31, 231–254. [Google Scholar] [CrossRef]
- Goverover, Y.; Chiaravalloti, N.; Genova, H.; DeLuca, J. A Randomized Controlled Trial to Treat Impaired Learning and Memory in Multiple Sclerosis: The Self-GEN Trial. Mult. Scler. J. 2018, 24, 1096–1104. [Google Scholar] [CrossRef]
- Pineau, F.; Socha, J.; Corvol, J.-C.; Louapre, C.; Assouad, R.; Maillart, E.; Lubetzki, C.; Papeix, C. Impact of an Adaptive Program for Cognitive and Emotional Deficits (ADACOG Program) in Multiple Sclerosis Patients with Cognitive Impairments. Rev. Neurol. 2019, 175, 305–312. [Google Scholar] [CrossRef]
- Stimmel, M.B.; Cohen, J.N.; Schneider, S.J.; Portnoy, J.G.; Seng, E.K.; Foley, F.W. A Neuropsychologically-Based Intervention with Increased Follow-up Support for Employed Women with Multiple Sclerosis: A Pilot Randomized Controlled Trial. Clin. Rehabil. 2020, 34, 1292–1302. [Google Scholar] [CrossRef]
- Reilly, S.; Hynes, S.M. A Cognitive Occupation-Based Programme for People with Multiple Sclerosis: A Study to Test Feasibility and Clinical Outcomes. Occup. Ther. Int. 2018, 2018, 1–9. [Google Scholar] [CrossRef]
- Impellizzeri, F.; Leonardi, S.; Latella, D.; Maggio, M.G.; Foti Cuzzola, M.; Russo, M.; Sessa, E.; Bramanti, P.; De Luca, R.; Calabrò, R.S. An Integrative Cognitive Rehabilitation Using Neurologic Music Therapy in Multiple Sclerosis: A Pilot Study. Medicine 2020, 99, e18866. [Google Scholar] [CrossRef]
- Mani, A.; Chohedri, E.; Ravanfar, P.; Mowla, A.; Nikseresht, A. Efficacy of Group Cognitive Rehabilitation Therapy in Multiple Sclerosis. Acta Neurol. Scand. 2018, 137, 589–597. [Google Scholar] [CrossRef]
- Lincoln, N.B.; Bradshaw, L.E.; Constantinescu, C.S.; Day, F.; Drummond, A.E.; Fitzsimmons, D.; Harris, S.; Montgomery, A.A.; das Nair, R.; Morgan, M.; et al. Cognitive Rehabilitation for Attention and Memory in People with Multiple Sclerosis: A Randomized Controlled Trial (CRAMMS). Clin. Rehabil. 2020, 34, 229–241. [Google Scholar] [CrossRef] [PubMed]
- Arsoy, E.; Tüzün, E.; Türkoğlu, R. Effects of Computer-Assisted Cognitive Rehabilitation in Benign Multiple Sclerosis. Turk. J. Med. Sci. 2018, 48, 999–1005. [Google Scholar] [CrossRef] [PubMed]
- Stuifbergen, A.K.; Becker, H.; Perez, F.; Morrison, J.; Brown, A.; Kullberg, V.; Zhang, W. Computer-Assisted Cognitive Rehabilitation in Persons with Multiple Sclerosis: Results of a Multi-Site Randomized Controlled Trial with Six Month Follow-Up. Disabil. Health J. 2018, 11, 427–434. [Google Scholar] [CrossRef]
- Blair, M.; Goveas, D.; Safi, A.; Marshall, C.; Rosehart, H.; Orenczuk, S.; Morrow, S.A. Does Cognitive Training Improve Attention/Working Memory in Persons with MS? A Pilot Study Using the Cogmed Working Memory Training Program. Mult. Scler. Relat. Disord. 2021, 49, 102770. [Google Scholar] [CrossRef]
- De Luca, R.; Russo, M.; Gasparini, S.; Leonardi, S.; Foti Cuzzola, M.; Sciarrone, F.; Zichittella, C.; Sessa, E.; Maggio, M.G.; De Cola, M.C.; et al. Do People with Multiple Sclerosis Benefit from PC-Based Neurorehabilitation? A Pilot Study. Appl. Neuropsychol. Adult 2021, 28, 427–435. [Google Scholar] [CrossRef] [PubMed]
- Bonzano, L.; Pedullà, L.; Pardini, M.; Tacchino, A.; Zaratin, P.; Battaglia, M.A.; Brichetto, G.; Bove, M. Brain Activity Pattern Changes after Adaptive Working Memory Training in Multiple Sclerosis. Brain Imaging Behav. 2020, 14, 142–154. [Google Scholar] [CrossRef]
- Charvet, L.E.; Yang, J.; Shaw, M.T.; Sherman, K.; Haider, L.; Xu, J.; Krupp, L.B. Cognitive Function in Multiple Sclerosis Improves with Telerehabilitation: Results from a Randomized Controlled Trial. PLoS ONE 2017, 12, e0177177. [Google Scholar] [CrossRef]
- Fuchs, T.A.; Ziccardi, S.; Dwyer, M.G.; Charvet, L.E.; Bartnik, A.; Campbell, R.; Escobar, J.; Hojnacki, D.; Kolb, C.; Oship, D.; et al. Response Heterogeneity to Home-Based Restorative Cognitive Rehabilitation in Multiple Sclerosis: An Exploratory Study. Mult. Scler. Relat. Disord. 2019, 34, 103–111. [Google Scholar] [CrossRef]
- Vilou, I.; Bakirtzis, C.; Artemiadis, A.; Ioannidis, P.; Papadimitriou, M.; Konstantinopoulou, E.; Aretouli, E.; Messinis, L.; Nasios, G.; Dardiotis, E.; et al. Computerized Cognitive Rehabilitation for Treatment of Cognitive Impairment in Multiple Sclerosis: An Explorative Study. J. Integr. Neurosci. 2020, 19, 341. [Google Scholar] [CrossRef]
- Darestani, A.; Naeeni Davarani, M.; Hassani-Abharian, P.; Zarrindast, M.-R.; Nasehi, M. The Therapeutic Effect of Treatment with RehaCom Software on Verbal Performance in Patients with Multiple Sclerosis. J. Clin. Neurosci. 2020, 72, 93–97. [Google Scholar] [CrossRef]
- Ozdogar, A.T.; Ertekin, O.; Kahraman, T.; Yigit, P.; Ozakbas, S. Effect of Video-Based Exergaming on Arm and Cognitive Function in Persons with Multiple Sclerosis: A Randomized Controlled Trial. Mult. Scler. Relat. Disord. 2020, 40, 101966. [Google Scholar] [CrossRef] [PubMed]
- Bove, R.; Rowles, W.; Zhao, C.; Anderson, A.; Friedman, S.; Langdon, D.; Alexander, A.; Sacco, S.; Henry, R.; Gazzaley, A.; et al. A Novel In-Home Digital Treatment to Improve Processing Speed in People with Multiple Sclerosis: A Pilot Study. Mult. Scler. 2021, 27, 778–789. [Google Scholar] [CrossRef] [PubMed]
- Leonardi, S.; Maggio, M.G.; Russo, M.; Bramanti, A.; Arcadi, F.A.; Naro, A.; Calabrò, R.S.; De Luca, R. Cognitive Recovery in People with Relapsing/Remitting Multiple Sclerosis: A Randomized Clinical Trial on Virtual Reality-Based Neurorehabilitation. Clin. Neurol. Neurosurg. 2021, 208, 106828. [Google Scholar] [CrossRef] [PubMed]
- Maggio, M.G.; De Luca, R.; Manuli, A.; Buda, A.; Foti Cuzzola, M.; Leonardi, S.; D’Aleo, G.; Bramanti, P.; Russo, M.; Calabrò, R.S. Do Patients with Multiple Sclerosis Benefit from Semi-Immersive Virtual Reality? A Randomized Clinical Trial on Cognitive and Motor Outcomes. Appl. Neuropsychol. Adult 2022, 29, 59–65. [Google Scholar] [CrossRef] [PubMed]
- Barry, A.; Cronin, O.; Ryan, A.M.; Sweeney, B.; O’Toole, O.; Allen, A.P.; Clarke, G.; O’Halloran, K.D.; Downer, E.J. Impact of Short-Term Cycle Ergometer Training on Quality of Life, Cognition and Depressive Symptomatology in Multiple Sclerosis Patients: A Pilot Study. Neurol. Sci. 2018, 39, 461–469. [Google Scholar] [CrossRef]
- Androwis, G.J.; Kwasnica, M.A.; Niewrzol, P.; Popok, P.; Fakhoury, F.N.; Sandroff, B.M.; Yue, G.H.; DeLuca, J. Mobility and Cognitive Improvements Resulted from Overground Robotic Exoskeleton Gait-Training in Persons with MS. In Proceedings of the 2019 41st Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Berlin, Germany, 23–27 July 2019; IEEE: Berlin, Germany, 2019; pp. 4454–4457. [Google Scholar]
- Langeskov-Christensen, M.; Hvid, L.G.; Jensen, H.B.; Nielsen, H.H.; Petersen, T.; Stenager, E.; Hämäläinen, P.; Dalgas, U. Efficacy of High-Intensity Aerobic Exercise on Cognitive Performance in People with Multiple Sclerosis: A Randomized Controlled Trial. Mult. Scler. 2021, 27, 1585–1596. [Google Scholar] [CrossRef]
- Ozkul, C.; Guclu-Gunduz, A.; Eldemir, K.; Apaydin, Y.; Yazici, G.; Irkec, C. Combined Exercise Training Improves Cognitive Functions in Multiple Sclerosis Patients with Cognitive Impairment: A Single-Blinded Randomized Controlled Trial. Mult. Scler. Relat. Disord. 2020, 45, 102419. [Google Scholar] [CrossRef]
- Feys, P.; Moumdjian, L.; Van Halewyck, F.; Wens, I.; Eijnde, B.O.; Van Wijmeersch, B.; Popescu, V.; Van Asch, P. Effects of an Individual 12-Week Community-Located “Start-to-Run” Program on Physical Capacity, Walking, Fatigue, Cognitive Function, Brain Volumes, and Structures in Persons with Multiple Sclerosis. Mult. Scler. 2019, 25, 92–103. [Google Scholar] [CrossRef]
- Van Geel, F.; Geurts, E.; Abasıyanık, Z.; Coninx, K.; Feys, P. Feasibility Study of a 10-Week Community-Based Program Using the WalkWithMe Application on Physical Activity, Walking, Fatigue and Cognition in Persons with Multiple Sclerosis. Mult. Scler. Relat. Disord. 2020, 42, 102067. [Google Scholar] [CrossRef]
- Gholami, M.; Nami, M.; Shamsi, F.; Jaberi, K.R.; Kateb, B.; Rahimi Jaberi, A. Effects of Transcranial Direct Current Stimulation on Cognitive Dysfunction in Multiple Sclerosis. Neurophysiol. Clin. 2021, 51, 319–328. [Google Scholar] [CrossRef]
- Charvet, L.; Shaw, M.; Dobbs, B.; Frontario, A.; Sherman, K.; Bikson, M.; Datta, A.; Krupp, L.; Zeinapour, E.; Kasschau, M. Remotely Supervised Transcranial Direct Current Stimulation Increases the Benefit of At-Home Cognitive Training in Multiple Sclerosis. Neuromodulation Technol. Neural Interface 2018, 21, 383–389. [Google Scholar] [CrossRef] [PubMed]
- Pinter, D.; Kober, S.E.; Fruhwirth, V.; Berger, L.; Damulina, A.; Khalil, M.; Neuper, C.; Wood, G.; Enzinger, C. MRI Correlates of Cognitive Improvement after Home-Based EEG Neurofeedback Training in Patients with Multiple Sclerosis: A Pilot Study. J. Neurol. 2021, 268, 3808–3816. [Google Scholar] [CrossRef] [PubMed]
- Petrou, P.; Ginzberg, A.; Binyamin, O.; Karussis, D. Beneficial Effects of a Nano Formulation of Pomegranate Seed Oil, GranaGard, on the Cognitive Function of Multiple Sclerosis Patients. Mult. Scler. Relat. Disord. 2021, 54, 103103. [Google Scholar] [CrossRef] [PubMed]
- Grzegorski, T.; Losy, J. Cognitive Impairment in Multiple Sclerosis—A Review of Current Knowledge and Recent Research. Rev. Neurosci. 2017, 28, 845–860. [Google Scholar] [CrossRef]
- Motl, R.W.; Pilutti, L.A.; Hubbard, E.A.; Wetter, N.C.; Sosnoff, J.J.; Sutton, B.P. Cardiorespiratory Fitness and Its Association with Thalamic, Hippocampal, and Basal Ganglia Volumes in Multiple Sclerosis. NeuroImage Clin. 2015, 7, 661–666. [Google Scholar] [CrossRef]
- Motl, R.W.; Sandroff, B.M. Exercise as a Countermeasure to Declining Central Nervous System Function in Multiple Sclerosis. Clin. Ther. 2018, 40, 16–25. [Google Scholar] [CrossRef]
- Motl, R.W.; Zivadinov, R.; Bergsland, N.; Benedict, R.H. Thalamus Volume and Ambulation in Multiple Sclerosis: A Cross-Sectional Study. Neurodegener. Dis. Manag. 2016, 6, 23–29. [Google Scholar] [CrossRef]
- Motl, R.W.; Sandroff, B.M.; Benedict, R.H.B. Cognitive dysfunction and multiple sclerosis: Developing a rationale for considering the efficacy of exercise training. Mult. Scler. J. 2011, 17, 1034–1040. [Google Scholar] [CrossRef]
- Ozkul, C.; Guclu-Gunduz, A.; Irkec, C.; Fidan, I.; Aydin, Y.; Ozkan, T.; Yazici, G. Effect of Combined Exercise Training on Serum Brain-Derived Neurotrophic Factor, Suppressors of Cytokine Signaling 1 and 3 in Patients with Multiple Sclerosis. J. Neuroimmunol. 2018, 316, 121–129. [Google Scholar] [CrossRef]
- Razeghi-Jahromi, S.; Doosti, R.; Ghorbani, Z.; Saeedi, R.; Abolhasani, M.; Akbari, N.; Cheraghi-Serkani, F.; Moghadasi, A.N.; Azimi, A.; Togha, M.; et al. A randomized controlled trial investigating the effects of a mediterranean-like diet in patients with multiple sclerosis-associated cognitive impairments and fatigue. Curr. J. Neurol. 2020, 19, 112–121. [Google Scholar] [CrossRef]
- Miller, E.; Morel, A.; Redlicka, J.; Miller, I.; Saluk, J. Pharmacological and Non-pharmacological Therapies of Cognitive Impairment in Multiple Sclerosis. Curr. Neuropharmacol. 2018, 16, 475–483. [Google Scholar] [CrossRef] [PubMed]
- Mitolo, M.; Venneri, A.; Wilkinson, I.D.; Sharrack, B. Cognitive rehabilitation in multiple sclerosis: A systematic review. J. Neurol. Sci. 2015, 354, 1–9. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Cognitive Rehabilitation (CR) | |
|---|---|
| Single-domain treatment (i.e., memory) | Traditional CR [8,9] Adaptive n-back working memory training [10] Mental Visual Imagery (MVI; [11]) |
| Multi-domain treatment | Program Cognitif pour Sclérose En Plaques French (ProCog-SEP program; [12]) Modified Story Memory Technique (mSMT; [13]) Strategy-based Techniques to Enhance Memory (STEM; [14]) Self-generation learning program (self-GEN trial; [15]) Adaptive program for cognitive and emotional deficits (ADACOG program; [16]) Additive interventions [17] Cognitive Occupation-Based Programme for People with Multiple Sclerosis (COB-MS; [18]) Traditional CR/Integrative approach: CR + neurologic music therapy [19] |
| Group cognitive rehabilitation (GCR) | [20,21] |
| Computerized Cognitive Rehabilitation (CCR) | NOROSOFT Mental Exercise Program [22] Memory, Attention, Problem Solving Skills in MS (MAPSS-MS; [23]) Cogmed Working Memory Training (CWMT; [24]) ERICA [25] COGNI-Track [26] Adaptive cognitive remediation (ACR; [27])/BrainHQ [28,29] RehaCom [30] Videogames (VG)/VG-like protocol [31,32] Virtual Reality (VR)/semi-immersive VR rehabilitation protocol [33,34] |
| Exercise Training (ET)/ Physical Activity (PA) | ET: routine cycle ergometry training [35]; gait-training program with a Robotic Exoskeleton [36]; progressive aerobic exercise [37] PA: combined aerobic and Pilates [38]; “Start-to-Run” Program [39]; WalkWithMe application [40] |
| Non-Invasive Brain Stimulation (NIBS) Brain Modulation | Transcranial Direct Current Stimulation (tDCS; [41]) Remotely supervised-tDCS (RS-tDCS; [42]) EEG neurofeedback training [43] |
| Miscellaneous Interventions | Food supplement: GranaGard [44] |
| Authors (Year) | Sample Size | Study Design | Intervention (Technique/Treatment and Duration) | Cognitive Results | MRI Results |
|---|---|---|---|---|---|
| Mousavi et al. (2018) [8] | 60 patients (20 exp; 20 placebo; 20 controls) | RCT | Memory rehabilitation (one-hour sessions on a weekly basis for 8 weeks) | Improvement in working memory | |
| Arsoy et al. (2018) [22] | 21 BMS patients; 22 non-BMS patients; 38 controls | RCT | Computer-assisted cognitive rehabilitation (NOROSOFT Mental Exercise Program; 5 days a week for 50 min) | Improvements in sustained attention, information processing speed, verbal fluency, categorical reasoning and executive functions | |
| Barry et al. (2018) [35] | 19 patients (9 cases; 10 controls) | RCT | PA (cycled for 30 min at 65–75% age-predicted maximal heart rate, twice a week for 8 weeks) | Improvement in attention, executive function/cognitive flexibility and visuospatial memory (via CANTAB battery) | |
| Ernst et al. (2018) [11] | 20 patients (10 cases; 10 controls) | RCT | MVI program (six two-hour individual sessions, one or twice per week) | Improvement in autobiographical memory | Enhanced neural activity in the left medial frontal regions and the right thalamus, in the left middle and inferior frontal gyrus, the left fusiform gyrus and left cerebellum |
| Goverover et al. (2018) [15] | 35 patients (19 treatment; 16 placebo) | RCT | Self-generation learning program (self-GEN trial; six 60 min) | Improved learning and memory, self-regulation, and metacognition (Contextual memory test, memory for intentions test) | |
| Mani et al. (2018) [20] | 34 patients | RCT | GCR (eight 2-h sessions of comprehensive group CR in 4 week) | Improvement in memory and executive function (ACE test, MFQ, WMS-R, WCST and BRIEF-A). No difference in attention (tested with CPT) | |
| Mousavi et al. (2020) [9] | 60 patients | RCT | Compensatory strategies, internal and external memory aids, mnemonics, mental reviews and error-free learning (1-h sessions on a weekly basis for 8 weeks) | Increase of the everyday memory with short duration during FU (<5 weeks) | |
| Reilly et al. (2018) [18] | 12 patients | Longitudinal study | COB-MS (eight sessions over 9 weeks, 60 min each session) | Improvements in verbal memory (CVLT-II), visual memory (BVMT-R), divided attention (TMT part B) and EMQ-R | |
| Androwis et al. (2019) [36] | 4 patients (2 cases; 2 controls) | RCT | RE-gait training (case)/CGT (control) (8-session; 1 h/session) | Improvement in the processing speed (SDMT) | |
| Pineau et al. (2019) [16] | 45 patients (24 cases; 21 controls) | Case- control Study | ADACOG: psycho-educational program focusing on cognitive and emotional dysfunctions (3 modules; each module 2 h every two weeks) | Less subjective self-reported cognitive deficits with MSNQ | |
| Brissart et al. (2020) [12] | 128 patients (64 cases; 64 controls) | RCT | CR program (ProCog-SEP) in group (13 two-hour sessions over six months) | Improvement in learning index (Selective Reminding Test) and verbal and working memory (Digit span backward and Working memory, TAP) | |
| Chiaravalloti et al. (2020) [13] | 30 patients (15 cases; 15 controls) | RCT | mSMT (10 sessions of the mSMT 2×/week for 5 weeks; sessions lasting 45–60 min) | Significant improvements in learning (both objective and self-reported), CVLT-II, SDMT | |
| Darestani et al. (2020) [30] | 60 patients (30 cases; 30 controls) | RCT | Rehacom (10 sessions during 5 weeks—2 sessions per week and each session was 1 h) | Improved verbal performance with COWAT and CVLT-II | |
| Impellizzeri et al. (2020) [19] | 30 patients (15 cases; 15 controls) | RCT | CR (controls: 6 times/week for 8 weeks) CR + NMT (cases: 3 times CR + 3 times NMT a week for 8 weeks) | Improvements in the BRB-N: selective reminding test long term storage, long term retrieval and delayed recall | |
| Lincoln et al. (2020) [21] | 449 patients (205 cases; 204 controls) | RCT | GCR (delivered weekly to 4–6 participants for 10 weeks) | Small improvement on EMQ at both 6 and 12 months (subjective participant and relative reports of memory problems) | |
| Ozdogar et al. (2020) [31] | 60 patients (21 VG; 19 conventional CR; 20 controls) | RCT | CCR (VG) (once a week for 8 weeks) | Improvement in nine-hole peg test (VG and conv. rehab); in VG: CVLT, SDMT and BVMT-R | |
| Ozkul et al. (2020) [38] | 34 patients (17 cases; 17 controls) | RCT | PA (combined aerobic and Pilates; three sessions per week for 8 weeks) | Improvements in long-term verbal memory, visuospatial memory, verbal fluency, information processing speed | |
| Stimmel et al. (2020) [17] | 30 patients (16 cases; 14 controls) | RCT | Additive interventions (in-person feedback and care-coordinator) phone calls | No significant difference pre- and post-intervention | |
| Chiaravalloti et al. (2021) [14] | 20 patients (9 cases; 11 controls) | RCT | Memory Rehab via STEM protocol (Self-generation, spaced learning, and retrieval practice) (8 sessions: 2 sessions/week for 4 weeks; 30–45 min long) | Medium-large effect size on the CVLT-II total learning score | |
| De Luca et al. (2021) [25] | 40 patients (20 cases; 20 controls) | RCT | CCR (ERICA software; 3 times a week for 8 weeks 45 min each session) | Improvements in memory, attention, and processing speed (test trough Montreal cognitive assessment, SDMT, SRT-LTS and SRT-D | |
| Gholami et al. (2021) [41] | 24 patients (12 cases; 12 controls) | RCT | tDCS (8 consecutive daily tDCS sessions over the left DLPFC) | Improvement in reasoning and executive functions (assessed via CBS-CP, RBANS) | |
| Langeskov- Christensen et al. (2021) [37] | 86 patients (43 cases; 43 controls) | RCT | PA (24-weeks progressive aerobic exercise) | Improvement in the SDMT | |
| Leonardi et al. (2021) [33] | 30 patients (15 conventional CR; 15 VR) | RCT | VR (3 times a week for 8 weeks, each session lasting about 45 Min) | Improvement in learning ability, short-term verbal memory and lexical access ability for the VR group | |
| Turtola et al. (2021) [10] | 24 patients (12 cases; 12 controls) | Case- control Study | Adaptive working memory training (20 sessions, each session 25–30 min, recommended rate of 5 sessions/week) | Enhancement of attention and cognitive control on untrained tasks | Potential limitations in the neural plasticity induced by working memory training |
| Maggio et al. (2022) [34] | 60 patients (30 cases; 30 controls) | RCT | Semi-immersive VR training (three sessions/week, each session 60 min, for 8 weeks) | Improvements in visual perception, visuospatial abilities, short term visual memory working memory and executive functions, speed of information processing and sustained attention (PASAT 2′) |
| Authors (Year) | Sample Size | Study Design | Intervention (Technique/Treatment and Duration) | Cognitive Results | MRI Results |
|---|---|---|---|---|---|
| Charvet et al. (2017) [27] | 135 patients (74 cases; 61 controls) | RCT | Online ACR program (research version of BrainHQ program) (1 h/day, 5 days/week over 12 weeks) | Improvement in Processing Speed (PASAT) and Visual Scanning (D-KEFS) in active group | |
| Charvet et al. (2018) [42] | 45 patients (25 cases; 20 controls) | RCT | RS-tDCS + CT (ten 20-min sessions of tDCS paired with a CT program); CT only condition (ten 20-min sessions of training) | Improvement in complex attention and response variability composites (compared to the only CT group) | |
| Stuifbergen et al. (2018) [23] | 183 patients (93 cases; 90 controls) | RCT | CCR (MAPSS-MS intervention: 3 daily sessions of 45 min, three times per week; 8 weeks) | Improvement in the CVLT Delayed Score, PASAT 3′, COWAT and PROMIS Cognitive Abilities scale | |
| Feys et al. (2019) [39] | 42 patients (21 cases; 21 controls) | RCT | PA: Individualized training in preparation of a running event (3 times weekly according to a personalized training intensity schedule; 12 weeks) | No important differences after training except for SPART | |
| Fuchs et al. (2019) [28] | 51 patients | Exploratory Study | BrainHQ (online restorative cognitive training program: 1 training session/day 45–60 min, for 5 days each week) | Improvement in SDMT | |
| Bonzano et al. (2020) [26] | 36 patients (18 cases; 18 controls) | Longitudinal Study | Working memory training: COGNI-TRAcK (8-week training; five 30-min sessions a week) | Improvement in PASAT | Brain activation map during PVSAT more similar to healthy participants after treatment (clusters mainly located in the right cerebellum and in the left hemisphere: precuneus and superior parietal lobule, precentral and superior frontal gyri) |
| Van Geel et al. (2020) [40] | 19 patients | Longitudinal study | PA (WalkWithMe, a personalized mobile application that helps to walk at home; 10 weeks) | Improvements in SDMT and PASAT | |
| Vilou et al. (2020) [29] | 47 RRMS patients (23 cases; 24 controls) | Explorative Study | BrainHQ web-based platform (20 min each session; 6 weeks) | Improvements in BVMT-R, GVLT, TMT-A and BICAMS (memory). No statistically significant difference in SDMT | |
| Blair et al. (2021) [24] | 30 patients (15 cases; 15 controls) | RCT | CCR with CWMT (25 training sessions; 8 exercises daily, approximately 30–45 min) | Improvements in D-KEFS Color-Word Interference Test, Letter-Number Sequencing and Digit Span | |
| Bove et al. (2021) [32] | 44 patients (23 cases; 21 controls) | RCT | Tablet-based VG-like digital treatment (25 min/day, 5 days/week, for 6 weeks) | Improvement in SDMT | |
| Pinter et al. (2021) [43] | 14 patients | Longitudinal Study | EEG-based neurofeedback via tele-rehabilitation (10 training sessions within 3–4 weeks) | Increased microstructural WM integrity in the left corticospinal tract, left anterior thalamic radiation and increased functional connectivity of salience network |
| Authors (Year) | Sample Size | Study Design | Intervention (Technique/Treatment and Duration) | Cognitive Results | MRI Results |
|---|---|---|---|---|---|
| Petrou et al. (2021) [44] | 30 patients (15 cases; 15 controls) | RCT | Diet (GranaGard, food supplement consisting in a self-emulsion nano formulation of pomegranate seed oil) | Improvement in CVLT-II, no change in SDMT |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bossa, M.; Manocchio, N.; Argento, O. Non-Pharmacological Treatments of Cognitive Impairment in Multiple Sclerosis: A Review. NeuroSci 2022, 3, 476-493. https://doi.org/10.3390/neurosci3030034
Bossa M, Manocchio N, Argento O. Non-Pharmacological Treatments of Cognitive Impairment in Multiple Sclerosis: A Review. NeuroSci. 2022; 3(3):476-493. https://doi.org/10.3390/neurosci3030034
Chicago/Turabian StyleBossa, Michela, Nicola Manocchio, and Ornella Argento. 2022. "Non-Pharmacological Treatments of Cognitive Impairment in Multiple Sclerosis: A Review" NeuroSci 3, no. 3: 476-493. https://doi.org/10.3390/neurosci3030034