
Study Protocol: Strategies and Techniques for the Rehabilitation of Cognitive and Motor Deficits in Patients with Multiple Sclerosis

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
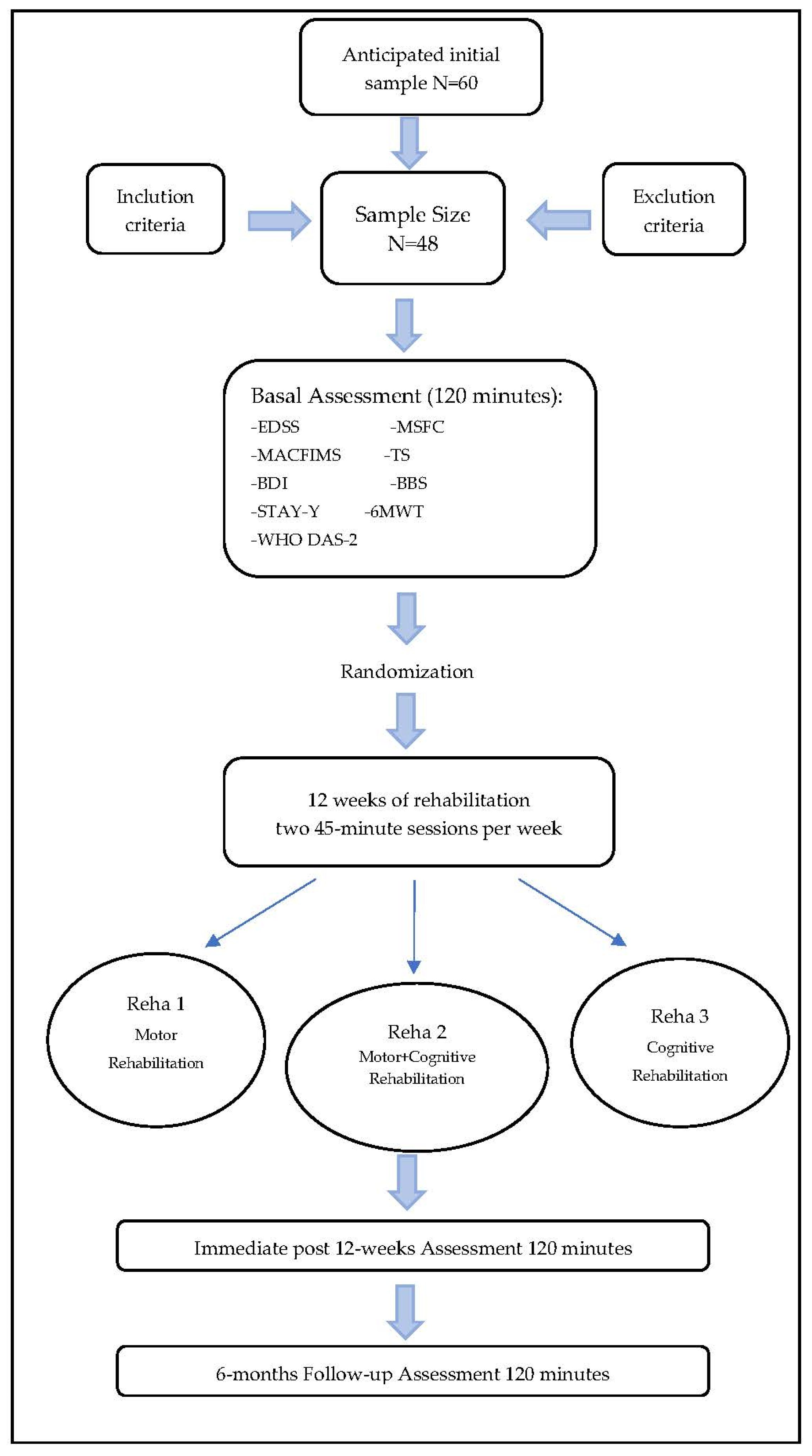
2.1. Aim, Design and Setting of This Study
- Compare three forms of rehabilitation—cognitive, motor and combined (cognitive–motor)—in three groups of MS patients.
- Check whether a combined rehabilitation approach can induce a significantly greater improvement on memory efficiency of MS patients, than cognitive rehabilitation performed alone.
- Evaluate whether self-perception and objective improvement correspond.
- Evaluate the impact of each rehabilitation program on patients’ overall disability.
- Monitor the effects of the three rehabilitation conditions after 6 months.
- Reha 2: is composed by a combined rehabilitation program with the use of the four verbal memory sessions of RehaCom together with a motor rehabilitation program. Each patient will carry out one 45-min session of cognitive rehabilitation and one 45-min session of motor rehabilitation each week for 12 weeks;
- Reha 3: is composed of two 45-min sessions of motor rehabilitation training each week for a total duration of 12 weeks.
2.2. Recruitment and Screening of Participants
2.3. Assessment Procedures
- Accurate collection of personal, anamnestic and clinical information;
- Expanded Disability Status Scale (EDSS) [24]: is a rating scale administered by a trained physician, aimed at evaluating functional CNS sub-systems. EDSS is used also to identify disease progression in MS patients and to evaluate the effectiveness of therapeutic interventions in clinical trials. It consists of an ordinal classification system ranging from 0 (normal neurological status) to 10 (death for MS) in increments of 0.5 (when EDSS 1 is reached). The lower values of the EDSS scale measure deficits based on neurological examination, while the upper range of the scale (>EDSS 6) measures the handicaps of MS patients [25]. The determination of the 4–6 interval of the EDSS strongly depends on aspects concerning walking [25].
- Neuropsychological evaluation through the Minimal Assessment of Cognitive Functioning in Multiple Sclerosis battery (MACFIMS) [26], in the Italian version [27]. This battery consists of seven tests:
- ○
- The California Verbal Learning Test-II (measurement of verbal learning and memory; CVLT-II) [28,29] requires the learning of a 16 words list (made up of 4 words from four different categories) read by the examiner across five trials. After each trial the subject has to recall as many words as possible in any order; the number of words correctly recalled for each trial is recorded. The total Immediate Recall (IR) score is the sum of the words correctly recalled across the five trials, ranging from 0 to 80. After having performed some interference tests the patient has to repeat the previously learned words (Delayed Recall; DR).
- ○
- The Brief Visuospatial Memory Test—Revised (visuospatial memory test; BVMT-R) [30] consists of three consecutive trials in which the subject views for 10 s a display of six non-iconic figures, arranged in a 2 × 3 matrix. After that the subject has to reproduce each figure in the correct locations on the page. Patient is asked to reproduce the figures again after a 25-min interval without any further exposure to the stimuli. Scoring is based on the subject’s reproduction accuracy and location of each figure [31]. Each figure reproduced can receive 0 to 2 points score [32]. The Immediate Recall (IR) corresponded to the scores’ sum obtained across the three trials while the Delayed Recall (DR) is the score obtained in the 25-min delayed trial. The BVMT-R offers six equivalent alternative forms [33].
- ○
- The Symbol Digit Modalities Test (information processing speed; SDMT; oral version) features a series of nine symbols, each of which is paired with a single-digit number in a pattern at the top of a sheet. The rest of the page has a pseudo-randomized sequence of these symbols. The patient is asked to say the digit associated with each symbol as quickly as possible in 90 s. The SDMT was originally designed for both written or oral responses, but the expert group recommended oral administration with MS patients to minimize complaints due to upper limb weakness or incoordination. The dependent variable is the total number of correct answers in 90 s [33,34].
- ○
- The Benton Judgment of Line Orientation test (measures the accuracy of spatial orientation judgments; BJLO) [35] requires subjects to identify the angle defined by two stimulus lines among those reported in a visual series of lines spanning 180 degrees. The dependent variable of the BJLO is the total number of correct answers [33].
- ○
- The Controlled Oral Word Association Test (measure of phonemic fluency; COWAT) gives subjects three 1-min time intervals each to generate as many words as possible beginning with three different input letters. Given that the subject’s performance is strongly influenced by the efficiency and speed of the search into one’s own lexicon, the COWAT cannot be considered a test of “pure” language. The total score is the total number of words generated in all three tests. Two equivalent alternative forms are available [33].
- ○
- The Delis–Kaplan Executive Function System Sorting Test (D-KEFS ST) is a composite measure of: concept formation skills, specific problem-solving skills for verbal/non-verbal aspects and ability to explain the abstract ordering of concepts [36]. It is able to explore reasoning, categorization skills, problem solving, abstraction, flexibility of thought and conceptual training skills, and it also provides good validity [37] and adequate reliability [38]. The test involves the presentation of six mixed cardstocks having different perceptual and semantic characteristics. The participant is asked to divide the cards into two groups (categorization), with three cards each, based on objective criteria and to describe the concepts used to generate each categorization (description). Each of the two sets of cards has a maximum of eight types of categories: three based on the semantic meaning of the printed words and five based on the cards’ visuo-spatial characteristics or patterns. The participant has a maximum of 4 min (for each set of cards) to find as many categorizations as possible [39]. The Sorting Score (SS) represents the total number of correct categorizations made by the subject; the Point Score (PS) represents the quality of the description (classifications) made for all the SS.
- ○
- The Paced Auditory Serial Addition Test in 3 and 2 s versions (measure of working memory; PASAT). It takes 20 min to administer and has adequate sensitivity and specificity (approximately 75% and 90%, respectively) in discriminating compromised patients from intact ones [40,41] In this test the patients asks some digit numbers each 3 or 2 s. He/she is asked to sum the number just said with the previous and say each time the correct sum.
- The Beck Depression Inventory (BDI) [42] is a self-report tool that allows you to assess the severity of depression in patients of at least 13 years of age. The test consists of 13 items with a score ranging from 0 to 3 from which a total score is derived. The test was developed as an indicator of the presence and intensity of depressive symptoms at the time of administration. It is useful in assessing depressive mood changes, estimating suicide risk and correctly assessing depressive symptoms in primary prevention, intervention and follow-up.
- The State–Trait Anxiety Inventory Y form (STAI Y) [43] is made up of two subtests of 20 items each with a 4-level response scale of intensity (e.g., from “almost never” to “almost always”). The first subtest evaluates how subjects feel at the time of testing, the second focuses on how subjects generally feel. The two scales refer, respectively, to state anxiety (considered a temporary interruption of the emotional continuum), conceived as a particular experience, a feeling of insecurity, of helplessness in the face of a perceived damage that can lead either to worry or to escape and avoidance; and trait anxiety (considered a relatively stable personality characteristic or a behavioral attitude) which reflects the tendency to perceive stimuli and environmental situations as dangerous or threatening [44].
- The World Health Organization—Disability Assessment Schedule (WHO-DAS 2—Disability level assessment questionnaire) is a tool developed by the WHO in 1998 in order to evaluate the limitations of activities and restrictions on participation experienced by a patient due to its medical condition. The WHODAS-2 is made up of 36 items that evaluate the functioning and the disability of the subject in a time window of 30 days [45]. The questionnaire covers 6 domains: cognitive functions (6 items), mobility (5 items), self-care (4 items), interaction with others (5 items), daily life activities [domestic activities (4 items), work/school (4 items)], participation in social life (8 items). The answer options range from 0 (no difficulty) to 5 (total difficulty) [46].
- The Multiple Sclerosis Neuropsychological Questionnaire (MSNQ) [47] is a brief self-administered test with 15 questions that reflect neuropsychological competence during activities of daily living. Each item is rated on a 5-point Likert scale, which goes from 0 (never, never happens) to four (very often, very seriously). A total score is obtained from the sum of the points of each single item.
- The Multiple Sclerosis Functional Composite (MSFC) is a functional assessment consisting of three tests:
- 1.
- The Timed 25 Foot Walk (T25FW) is a quantitative measure of the function of the lower limbs. The patient is directed to the end of a clearly indicated path and is asked to walk 7.62 m as quickly as possible, but safely. The activity is immediately repeated making the patient return to the initial starting point. If necessary, patients can use an assistive device during the test. Three scores are obtained: two relating to single walks and one given by the averaged time of the two paths [48].
- 2.
- The Nine Hole Peg Test (NHPT) is a simple and relatively quick evidence-based test that measures the functions of the upper limbs (hand and arm) [49]. It consists of a standardized test apparatus consisting of a platform with nine holes and nine pegs to insert. Participants are seated and then asked to insert and then remove the nine pegs from the nine holes, one at a time, as quickly as possible. Both dominant and non-dominant hands are tested twice (two consecutive dominant hand trials, immediately followed by two consecutive non-dominant hand trials) [48]. At the end of the test, 6 scores are obtained: 2 relating to the time taken to perform the task with the dominant hand, 2 scores relating to the time spent with the non-dominant hand and finally two scores representing the average time taken to perform the test with the dominant and the non-dominant hands.
- 3.
- The PASAT (see on the previous page).
- The Six Minutes Walking Test (6MWT) is a test developed by Balke in 1963 [50], as an index of motor resistance [51]. The test requires the subject to walk for 6 min without interruption, following a path marked by the therapist through the aid of cones that delineate the boundaries. The subject is allowed to rest when necessary [50]. The distance traveled is measured in meters by a special tool: the measuring wheel.
- The Tinetti Scale (TS) is a clinical tool that allows the assessment of patient’s balance and walking performance by assigning an objective score to the motor performance. The Tinetti scale is composed of a section that evaluates static balance, characterized by 9 items with a global score between 0 and 16, and a section that evaluates gait, composed of 7 items with a global score between 0 and 12. Both sections can be scored by the examiner on a 3-point ordinal scale (0 = inability to execute the request; 1 = ability to execute with adaptations or aids; 2 = ability to execute it without adaptation) or 2-point ordinal scale (0 = inability to execute the request; 1 = ability to execute it without adaptation). The patient can obtain a total score between 0 and 28. Thanks to the obtained score, the examiner is able to quantify the risk of falling and has a basis on which to develop personalized rehabilitation programs [52].
- The Berg Balance Scale (BBS) is one of the most common clinical measures of static and dynamic balance [53]. The BBS includes 14 items that assess a person’s ability to maintain balance while performing activities of different difficulty (e.g., going from sitting to standing, picking up an object from the floor, turning 360°). A score is assigned to each item on a 4-point ordinal scale from 0 (=unable to perform) to 4 (=normal performance), accounting for the patient’s ability in performing the exercises without any aid. The BBS has a strong inter-rater and test–retest reliability [54].
2.4. Randomization
3. Rehabilitation
3.1. Cognitive RehabilitationRehaCom Modules
RehaCom Modules
- Strategic memory training (LEST): The patient will be presented with a pair of words on the PC screen to memorize (the number of words could increase or decrease according to the performance of the subject). The task will be to find the objects that correspond to the memorized words. When the patient recognizes an object, he will have to click on it and repeat the operation until he/she has clicked on all recognized objects. The task will end when all the objects are identified. The correct choice will be marked in green, the wrong one in red. For each group of images presented, the subject will have three possibilities of error, after which the exercise will return to the opening words and the patient is asked to memorize them again. The words to be memorized will change only when all the images are recognized without making mistakes. Patients can use any personal memorization strategies: some will memorize the words according to the presentation order, others by dividing them into semantic categories and others by building stories. Between memorizing words and recognition, participants will be asked to perform a distracting task: move a basket from one side of the screen to the other to collect all the fruits that fall from a tree.
- Working memory (WOME): The patient will be presented with three decks of cards (a deck of poker cards, a deck of colored cards and one characterized by unusual symbols) from which he/she can choose his/her favorite. Then, the program asks the patient to follow some specific indications (e.g., to memorize all the cards presented, to memorize the cards in the presentation order, and to memorize only cards with certain characteristics). In the event that the patient does not perform the exercise correctly, this will be repeated a second time with the same cards. To increase the difficulty of the exercise, a distractor (e.g., a question of general knowledge) may be introduced between the memorization of the cards and their recognition.
- Figurative memory (BILD): Words to be memorized without time limits will appear on the PC screen. Once all the words are memorized, the patient will see a series of figures moving across the screen from right to left. When the patient sees one of the figures, corresponding to the objects memorized before, passing through a red highlighted area, he must press the “ok” button. The number of figures will progressively increase with the improvement of the patient’s performance.
- Verbal memory (VERB): The patient will see a short text in which he/she has to memorize names, numbers, objects and events. Subsequently, the subject is asked to answer some questions about what has been read, choosing from four answer options. The difficulty of the task may decrease or increase by varying the length of the passage and the amount of information depending on the patient’s performance. Furthermore, the settings of the task can be changed: for example, the exercise can be set in such a way as to have the patient read two passages, one after the other, and then answer questions asked about the first one, or the patient can be asked to answer with open answers.
3.2. Motor Rehabilitation
4. Statistics and Outcome
4.1. Data Analysis
- “Within-group” analyses. These statistical analyses will be aimed at evaluating any improvement in patients’ cognitive performance. Within each group of patients, the assessments at T0 will be compared with that at T1 and T2 through a repeated measures ANOVA between the scores of the cognitive assessments. In case of significance, post hoc tests will be carried out to which a Bonferroni correction will be applied with significance set at p < 0.016. Similarly, the same analysis will be conducted to compare the levels of anxiety and depression, the self-perception of cognitive deficit and the level of perceived disability.
- “Between-group” analyses. These statistical analyses will be aimed at comparing the results obtained by the groups at T0, T1, and T2 by performing an ANOVA between the scores of the cognitive assessments. In case of significance, post hoc tests will be performed to which a Bonferroni correction will be applied with significance set at p < 0.016. Additionally, in this case, the same comparative analysis will be carried out on the following variables: levels of anxiety and depression, self-perception of one’s cognitive difficulties and level of perceived disability.
4.2. Outcomes
5. Ethics and Dissemination
6. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kasser, S.L.; Jacobs, J.V.; Foley, J.; Cardinal, B.J.; Maddalozzo, G.F. A Prospective Evaluation of Balance, Gait, and Strength to Predict Falling in Women With Multiple Sclerosis. Arch. Phys. Med. Rehabil. 2011, 92, 1840–1846. [Google Scholar] [CrossRef] [PubMed]
- Chiaravalloti, N.D.; DeLuca, J. Cognitive impairment in multiple sclerosis. Lancet Neurol. 2008, 7, 1139–1151. [Google Scholar] [CrossRef]
- Barbarulo, A.M.; Lus, G.; Signoriello, E.; Trojano, L.; Grossi, D.; Esposito, M.; Costabile, T.; Lanzillo, R.; Saccà, F.; Morra, V.B.; et al. Integrated Cognitive and Neuromotor Rehabilitation in Multiple Sclerosis: A Pragmatic Study. Front. Behav. Neurosci. 2018, 12, 196. [Google Scholar] [CrossRef] [PubMed]
- Amato, M.P.; Portaccio, E.; Zipoli, V. Are there protective treatments for cognitive decline in MS? J. Neurol. Sci. 2006, 245, 183–186. [Google Scholar] [CrossRef]
- Goretti, B.; Portaccio, E.; Zipoli, V.; Hakiki, B.; Siracusa, G.; Sorbi, S.; Amato, M.P. Coping strategies, psychological variables and their relationship with quality of life in multiple sclerosis. Neurol. Sci. 2009, 30, 15–20. [Google Scholar] [CrossRef]
- Nocentini, U.; Caltagirone, C.; Tedeschi, G. Neuropsychiatric Dysfunction in Multiple Sclerosis; Springer Science & Business Media: Berlin/Heidelberg, Germany, 2012. [Google Scholar]
- Van Asch, P. Impact of Mobility Impairment in Multiple Sclerosis 2—Patients’ Perspectives. Eur. Neurol. Rev. 2011, 6, 115–120. [Google Scholar] [CrossRef]
- Leone, C.; Patti, F.; Feys, P. Measuring the cost of cognitive-motor dual tasking during walking in multiple sclerosis. Mult. Scler. J. 2014, 21, 123–131. [Google Scholar] [CrossRef]
- Kesselring, J.; Beer, S. Symptomatic therapy and neurorehabilitation in multiple sclerosis. Lancet Neurol. 2005, 4, 643–652. [Google Scholar] [CrossRef]
- Beer, S.; Khan, F.; Kesselring, J. Rehabilitation interventions in multiple sclerosis: An overview. J. Neurol. 2012, 259, 1994–2008. [Google Scholar] [CrossRef]
- Argento, O.; Incerti, C.C.; Pisani, V.; Magistrale, G.; Di Battista, G.; Romano, S.; Ferraro, E.; Caltagirone, C.; Nocentini, U. Domestic accidents and multiple sclerosis: An exploratory study of occurrence and possible causes. Disabil. Rehabil. 2014, 36, 2205–2209. [Google Scholar] [CrossRef]
- Incerti, C.C.; Argento, O.; Magistrale, G.; Ferraro, E.; Caltagirone, C.; Pisani, V.; Nocentini, U. Adverse working events in patients with multiple sclerosis. Neurol. Sci. 2016, 38, 349–352. [Google Scholar] [CrossRef] [PubMed]
- Chiaravalloti, N.D.; DeLuca, J. Self-generation as a means of maximizing learning in multiple sclerosis: An application of the generation effect. Arch. Phys. Med. Rehabil. 2002, 83, 1070–1079. [Google Scholar] [CrossRef] [PubMed]
- Chiaravalloti, N.D.; Moore, N.B.; Nikelshpur, O.M.; DeLuca, J. An RCT to treat learning impairment in multiple sclerosis: The MEMREHAB trial. Neurology 2013, 81, 2066–2072. [Google Scholar] [CrossRef] [PubMed]
- EMS Sistemi Elettromedicali. Available online: http://www.emsmedical.net (accessed on 29 October 2018).
- Flavia, M.; Stampatori, C.; Zanotti, D.; Parrinello, G.; Capra, R. Efficacy and specificity of intensive cognitive rehabilitation of attention and executive functions in multiple sclerosis. J. Neurol. Sci. 2010, 288, 101–105. [Google Scholar] [CrossRef]
- Mattioli, F.; Stampatori, C.; Bellomi, F.; Danni, M.; Compagnucci, L.; Uccelli, A.; Pardini, M.; Santuccio, G.; Fregonese, G.; Pattini, M.; et al. A RCT Comparing Specific Intensive Cognitive Training to Aspecific Psychological Intervention in RRMS: The SMICT Study. Front. Neurol. 2015, 5, 278. [Google Scholar] [CrossRef] [Green Version]
- Chiaravalloti, N.D.; Wylie, G.; Leavitt, V.; DeLuca, J. Increased cerebral activation after behavioral treatment for memory deficits in MS. J. Neurol. 2012, 259, 1337–1346. [Google Scholar] [CrossRef]
- Benedict, R.H.; Holtzer, R.; Motl, R.W.; Foley, F.W.; Kaur, S.; Hojnacki, D.; Weinstock-Guttman, B. Upper and Lower Extremity Motor Function and Cognitive Impairment in Multiple Sclerosis. J. Int. Neuropsychol. Soc. 2011, 17, 643–653. [Google Scholar] [CrossRef]
- Motl, R.W.; Cadavid, D.; Sandroff, B.; Pilutti, L.A.; Pula, J.H.; Benedict, R.H. Cognitive processing speed has minimal influence on the construct validity of Multiple Sclerosis Walking Scale-12 scores. J. Neurol. Sci. 2013, 335, 169–173. [Google Scholar] [CrossRef]
- Argento, O.; Spanò, B.; Pisani, V.; Incerti, C.C.; Bozzali, M.; Foti, C.; Caltagirone, C.; Nocentini, U. Dual-Task Performance in Multiple Sclerosis’ Patients: Cerebellum Matters? Arch. Clin. Neuropsychol. 2021, 36, 517–526. [Google Scholar] [CrossRef]
- Motl, R.W.; Sandroff, B.; DeLuca, J. Exercise Training and Cognitive Rehabilitation: A Symbiotic Approach for Rehabilitating Walking and Cognitive Functions in Multiple Sclerosis? Neurorehabilit. Neural Repair 2015, 30, 499–511. [Google Scholar] [CrossRef]
- Cerasa, A.; Gioia, M.C.; Valentino, P.; Nisticò, R.; Chiriaco, C.; Pirritano, D.; Tomaiuolo, F.; Mangone, G.; Trotta, M.; Talarico, T.; et al. Computer-Assisted Cognitive Rehabilitation of Attention Deficits for Multiple Sclerosis: A randomized trial with fMRI correlates. Neurorehabilit. Neural Repair 2012, 27, 284–295. [Google Scholar] [CrossRef] [PubMed]
- Kurtzke, J.F. Rating neurologic impairment in multiple sclerosis: An expanded disability status scale (EDSS). Neurology 1983, 33, 1444–1452. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Meyer-Moock, S.; Feng, Y.-S.; Maeurer, M.; Dippel, F.-W.; Kohlmann, T. Systematic literature review and validity evaluation of the Expanded Disability Status Scale (EDSS) and the Multiple Sclerosis Functional Composite (MSFC) in patients with multiple sclerosis. BMC Neurol. 2014, 14, 58. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Benedict, R.H.; Cookfair, D.; Gavett, R.; Gunther, M.; Munschauer, F.; Garg, N.; Weinstock-Guttman, B. Validity of the minimal assessment of cognitive function in multiple sclerosis (MACFIMS). J. Int. Neuropsychol. Soc. 2006, 12, 549–558. [Google Scholar] [CrossRef] [PubMed]
- Argento, O.; Incerti, C.C.; Quartuccio, M.E.; Magistrale, G.; Francia, A.; Caltagirone, C.; Pisani, V.; Nocentini, U. The Italian validation of the minimal assessment of cognitive function in multiple sclerosis (MACFIMS) and the application of the Cognitive Impairment Index scoring procedure in MS patients. Neurol. Sci. 2018, 39, 1237–1244. [Google Scholar] [CrossRef]
- Delis, D.C.; Kramer, J.H.; Kaplan, E.; Ober, B.A. California Verbal Learning Test-Second Edition (CVLT –II); Psychological Corporation: San Antonio, TX, USA, 2000. [Google Scholar] [CrossRef]
- Argento, O.; Pisani, V.; Incerti, C.C.; Magistrale, G.; Caltagirone, C.; Nocentini, U. The California Verbal Learning Test-II: Normative data for two Italian alternative forms. Clin. Neuropsychol. 2014, 19, 561–567. [Google Scholar] [CrossRef]
- Benedict, R.H.B.; Schretlen, D.; Groninger, L.; Dobraski, M.; Shpritz, B. Revision of the Brief Visuospatial Memory Test: Studies of normal performance, reliability, and validity. Psychol. Assess. 1996, 8, 145–153. [Google Scholar] [CrossRef]
- Argento, O.; Smerbeck, A.; Pisani, V.; Magistrale, G.; Incerti, C.C.; Caltagirone, C.; Benedict, R.H.B.; Nocentini, U. Regression-Based Norms for the Brief Visuospatial Memory Test-Revised in Italian population and application in MS patients. Clin. Neuropsychol. 2016, 30, 1469–1478. [Google Scholar] [CrossRef]
- Benedict, R.H.B. Brief Visuospatial Memory Test-Revised: Professional Manual; Psychological Assessment Resources: Odessa, FL, USA, 1997. [Google Scholar]
- Benedict, R.H.; Fischer, J.S.; Archibald, C.J.; Arnett, P.A.; Beatty, W.W.; Bobholz, J.; Chelune, G.J.; Fisk, J.D.; Langdon, D.; Caruso, L.; et al. Minimal Neuropsychological Assessment of MS Patients: A Consensus Approach. Clin. Neuropsychol. 2002, 16, 381–397. [Google Scholar] [CrossRef]
- Nocentini, U.; Giordano, A.; Di Vincenzo, S.; Panella, M.; Pasqualetti, P. The Symbol Digit Modalities Test—Oral version: Italian normative data. Funct. Neurol. 2006, 21, 93–96. [Google Scholar]
- Benton, A.L.; Sivan, A.; Hamsher, K.; Varney, N.; Spreen, O. Contributions to Neuropsychology Assessment: A Clinical Manual, 2nd ed.; Oxford University Press: New York, NY, USA, 1994. [Google Scholar]
- Delis, D.C.; Kaplan, E.; Kramer, J. Delis Kaplan Executive Function System; The Psychological Corporation: San Antonio, TX, USA, 2001. [Google Scholar] [CrossRef]
- Parmenter, B.A.; Zivadinov, R.; Kerenyi, L.; Gavett, R.; Weinstock-Guttman, B.; Dwyer, M.G.; Garg, N.; Munschauer, F.; Benedict, R.H.B. Validity of the Wisconsin Card Sorting and Delis–Kaplan Executive Function System (DKEFS) Sorting Tests in multiple sclerosis. J. Clin. Exp. Neuropsychol. 2007, 29, 215–223. [Google Scholar] [CrossRef] [PubMed]
- Strauss, E.; Sherman, E.M.S.; Spreen, O.; Spreen, O. A Compendium of Neuropsychological Tests: Administration, Norms, and Commentary; Oxford University Press: Oxford, UK, 2006. [Google Scholar]
- Mattioli, F.; Stampatori, C.; Bellomi, F.; Scarpazza, C.; Galli, P.; Guarneri, C.; Corso, B.; Montomoli, C.; Niccolai, C.; Goretti, B.; et al. Assessing executive function with the D-KEFS sorting test: Normative data for a sample of the Italian adult population. Neurol. Sci. 2014, 35, 1895–1902. [Google Scholar] [CrossRef] [PubMed]
- Rao, S.M.; Leo, G.J.; Bernardin, L.; Unverzagt, F. Cognitive dysfunction in multiple sclerosis.: I. Frequency, patterns, and prediction. Neurology 1991, 41, 685–691. [Google Scholar] [CrossRef] [PubMed]
- Aupperle, R.L.; Beatty, W.W.; Shelton, F.D.N.A.P.; Gontkovsky, S.T. Three screening batteries to detect cognitive impairment in multiple sclerosis. Mult. Scler. J. 2002, 8, 382–389. [Google Scholar] [CrossRef] [PubMed]
- Beck, A.T.; Steer, R.A.; Brown, G.K. Beck depression inventory (BDI-II); Pearson: London, UK, 1996. [Google Scholar]
- Spielberger, C.D. Manual for the State-Trait Anxiety Inventory (Form Y) (‘Self-Evaluation Questionnaire’); Consulting Psychologists Press: Palo Alto, CA, USA, 1983. [Google Scholar]
- Marteau, T.M.; Bekker, H. The development of a six-item short-form of the state scale of the Spielberger State—Trait Anxiety Inventory (STAI). Br. J. Clin. Psychol. 1992, 31, 301–306. [Google Scholar] [CrossRef]
- Magistrale, G.; Pisani, V.; Argento, O.; Incerti, C.C.; Bozzali, M.; Cadavid, D.; Caltagirone, C.; Medori, R.; DeLuca, J.; Nocentini, U. Validation of the World Health Organization Disability Assessment Schedule II (WHODAS-II) in patients with multiple sclerosis. Mult. Scler. J. 2015, 21, 448–456. [Google Scholar] [CrossRef]
- Garin, O.; Ayuso-Mateos, J.L.; Almansa, J.; Nieto, M.; Chatterji, S.; Vilagut, G.; Alonso, J.; Cieza, A.; Svetskova, O.; Burger, H.; et al. Validation of the “World Health Organization Disability Assessment Schedule, WHODAS-2” in patients with chronic diseases. Heal. Qual. Life Outcomes 2010, 8, 51. [Google Scholar] [CrossRef] [Green Version]
- Benedict, R.H.B.; Munschauer, F.; Linn, R.; Miller, C.; Murphy, E.; Foley, F.; Jacobs, L. Screening for multiple sclerosis cognitive impairment using a self-administered 15-item questionnaire. Mult. Scler. J. 2003, 9, 95–101. [Google Scholar] [CrossRef]
- Fischer, J.S.; Jak, A.J.; Judith, M.A.; Richard, A.; Rudick, M.D.; Gary, C. Multiple Sclerosis Functional Composite (MSFC). Administration and Scoring Manual; National Multiple Sclerosis Society: Denver, CO, USA, 2001. [Google Scholar]
- Grice, K.O.; Vogel, K.A.; Le, V.; Mitchell, A.; Muniz, S.; Vollmer, M.A. Adult Norms for a Commercially Available Nine Hole Peg Test for Finger Dexterity. Am. J. Occup. Ther. 2003, 57, 570–573. [Google Scholar] [CrossRef] [Green Version]
- Gijbels, D.; Eijnde, B.; Feys, P. Comparison of the 2- and 6-minute walk test in multiple sclerosis. Mult. Scler. J. 2011, 17, 1269–1272. [Google Scholar] [CrossRef]
- Cederberg, K.L.; Sikes, E.; Bartolucci, A.A.; Motl, R.W. Walking endurance in multiple sclerosis: Meta-analysis of six-minute walk test performance. Gait Posture 2019, 73, 147–153. [Google Scholar] [CrossRef] [PubMed]
- Tinetti, M.E. Performance-Oriented Assessment of Mobility Problems in Elderly Patients. J. Am. Geriatr. Soc. 1986, 34, 119–126. [Google Scholar] [CrossRef]
- Berg, K.O.; Wood-Dauphinee, S.L.; Williams, J.I.; Maki, B. Measuring balance in the elderly: Validation of an instrument. Can. J. Public Health Rev. Can. Sante Publique 1992, 83, S7–S11. [Google Scholar]
- Moore, J.L.; Potter, K.; Blankshain, K.; Kaplan, S.; O’Dwyer, L.; Sullivan, J.E. A Core Set of Outcome Measures for Adults With Neurologic Conditions Undergoing Rehabilitation: A Clinical Practice Guideline. J. Neurol. Phys. Ther. 2018, 42, 174–220. [Google Scholar] [CrossRef] [PubMed]
- Associazione Italiana Sclerosis Multipla AISM Barometer. 2018. Available online: https://www.aism.it/ (accessed on 20 June 2018).
- Faul, F.; Erdfelder, E.; Buchner, A.; Lang, A.-G. Statistical power analyses using G*Power 3.1: Tests for correlation and regression analyses. Behav. Res. Methods 2009, 41, 1149–1160. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yogev-Seligmann, G.; Hausdorff, J.M.; Giladi, N. The role of executive function and attention in gait. Mov. Disord. 2008, 23, 329–342. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hamilton, F.; Rochester, L.; Paul, L.; Rafferty, D.; O’Leary, C.P.; Evans, J.J. Walking and talking: An investigation of cognitive—motor dual tasking in multiple sclerosis. Mult. Scler. J. 2009, 15, 1215–1227. [Google Scholar] [CrossRef]
- Leavitt, V.M.; Cirnigliaro, C.; Cohen, A.; Farag, A.; Brooks, M.; Wecht, J.M.; Wylie, G.R.; Chiaravalloti, N.D.; DeLuca, J.; Sumowski, J.F. Aerobic exercise increases hippocampal volume and improves memory in multiple sclerosis: Preliminary findings. Neurocase 2014, 20, 695–697. [Google Scholar] [CrossRef]


{kind=link}
| Inclusion Criteria | |
|---|---|
| Diagnosis | Diagnosis of MS defined according to McDonald’s diagnostic criteria revisited in 2011 |
| Age | 18–65 years |
| Phenotype | RRMS or SPMS |
| Language | Italian mother tongue |
| EDSS | <6.0 |
| Exlcusion Criteria | |
| Pathologies | Neurological or psychiatric conditions other than MS that can interfere with cognitive functioning |
| Neurological history | Clinical relapses in the three months prior to enrollment, neurological pathologies other than MS and severe enough to interfere with cognitive functioning, and clinical relapse or disease activity highlighted on MRI magnetic during the treatment period |
| Severe mental illness | Psychiatric disorders severe enough to interfere with cognitive functioning |
| Medications | Steroid therapy in the 3 months prior to enrollment |
| Motor limitations | Dysfunction of the upper limbs (paralysis or tremor) that do not allow to hold the PC mouse |
| Sensory limitations | Visual acuity impaired enough not to allow reading of the instructions to the various tests |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Argento, O.; Piacentini, C.; Bossa, M.; Caltagirone, C.; Santamato, A.; Saraceni, V.; Nocentini, U. Study Protocol: Strategies and Techniques for the Rehabilitation of Cognitive and Motor Deficits in Patients with Multiple Sclerosis. NeuroSci 2022, 3, 395-407. https://doi.org/10.3390/neurosci3030029
Argento O, Piacentini C, Bossa M, Caltagirone C, Santamato A, Saraceni V, Nocentini U. Study Protocol: Strategies and Techniques for the Rehabilitation of Cognitive and Motor Deficits in Patients with Multiple Sclerosis. NeuroSci. 2022; 3(3):395-407. https://doi.org/10.3390/neurosci3030029
Chicago/Turabian StyleArgento, Ornella, Chiara Piacentini, Michela Bossa, Carlo Caltagirone, Andrea Santamato, Vincenzo Saraceni, and Ugo Nocentini. 2022. "Study Protocol: Strategies and Techniques for the Rehabilitation of Cognitive and Motor Deficits in Patients with Multiple Sclerosis" NeuroSci 3, no. 3: 395-407. https://doi.org/10.3390/neurosci3030029