1. Introduction
The etiology of mandibular fractures has always been associated with facial trauma, polytrauma, physical aggression, falls, and tumours [
1,
2,
3,
4,
5,
6,
7,
8]. With the evolution of dental treatments and new technologies, dental implant surgery has become one of the best treatment options for oral rehabilitation when one or more teeth are missing. Since 1985, when the first long-term clinical studies were published, the treatment of totally edentulous patients with implant-borne prostheses has been gaining ground in the academic and clinical community [
9,
10,
11]. The so-called overdenture has two or more implants, which are placed in the mandible and/or maxilla and connected to a structural component that is connected to a laboratory-manufactured or 3D-printed total prosthesis [
12,
13]. With advances in technology and understanding of the osseointegration process, more and more immediate treatments are being proposed, where the prosthesis is fitted on the same day or within a few weeks after the surgical placement of the dental implants. Also known as the “immediate implant protocol”, this procedure has become the standard for fully edentulous patients, especially in the mandible.
Mandibular fractures immediately following dental implant treatment are rare in the literature [
14,
15,
16], and it is important to discuss and better understand when they occur. The limited literature on the subject always points to the atrophic mandible associated with age-related bone loss, peri-implantitis, and iatrogenesis as the causes of these fractures [
15]. Mandibular fractures with chronic bone infection, known as osteomyelitis, are difficult to treat and carry a higher risk of local and systemic complications that disrupt and prolong any proposed treatment [
17,
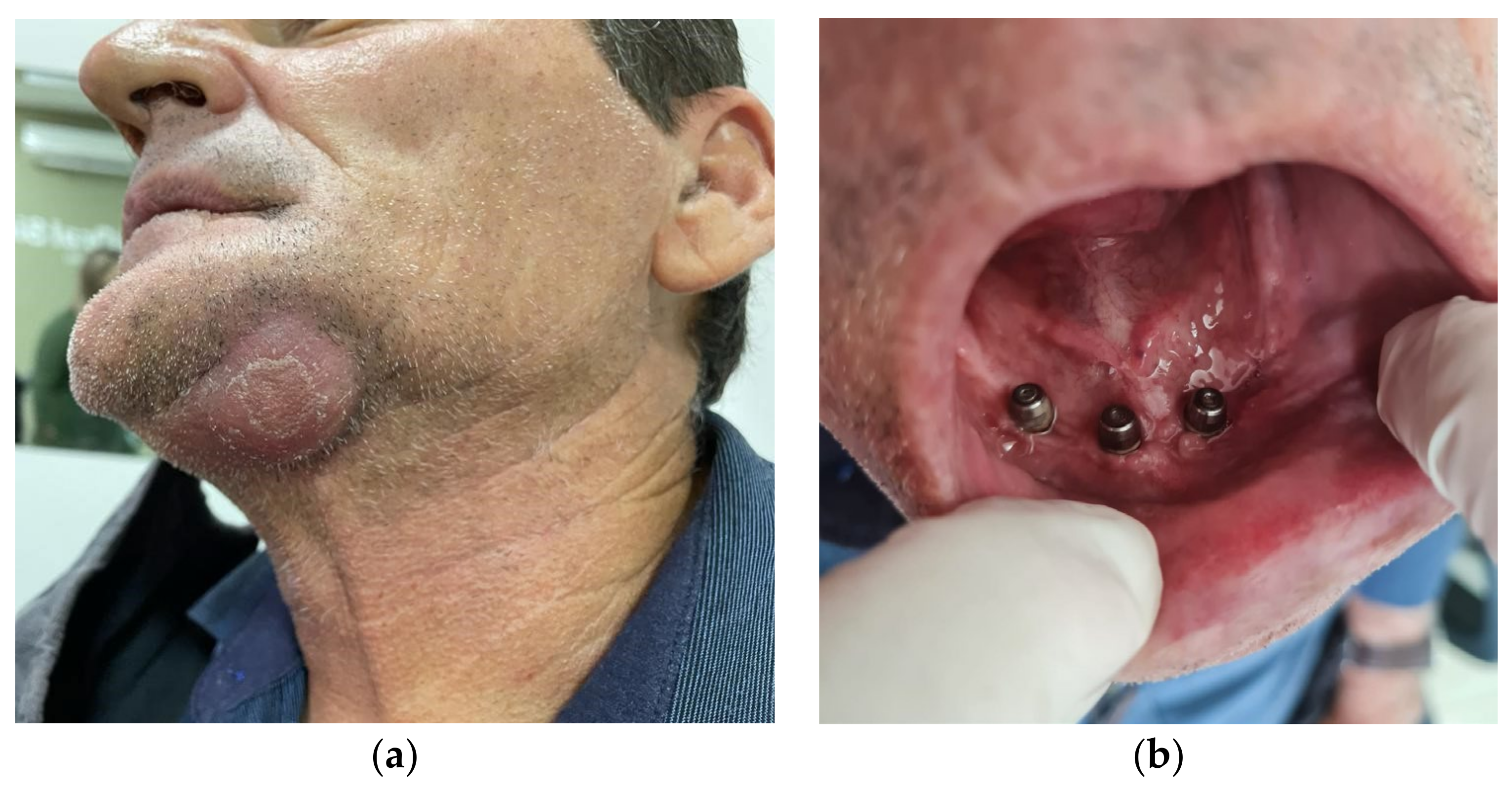
18]. Particularly in cases of oral rehabilitation where bone healing is desired, such as dental implant surgery, the presence of a localised infectious process with necrotic bone detachment makes such treatment impossible. Several stages of surgical treatment are necessary, depending on the organic response to these proposals, until the final treatment is completed. In this paper we describe a complex case of fracture of the left mandibular parasymphysis (
Figure 1) with osteomyelitis and submandibular suppurative drainage.
Treatment of the osteomyelitis was performed in two stages (surgical and clinical): removal of the bone fragments in the fracture, debridement of the soft tissues and curettage of the necrotic hard tissues in the area, rigid internal fixation of the mandible with 2.0 mini-plates, and antibiotic treatment for 2 weeks. The patient was evaluated every 3 days until successful treatment of the osteomyelitis was confirmed. Given the complications that may be associated with this type of fracture, a DEXA scan was requested to assess the patient’s risk of osteoporosis, which was confirmed. The patient was referred for specialist medical treatment and calcium replacement. Two months later, with no signs of infection and mandibular continuity restored, oral rehabilitation was performed with a prosthesis on the 3 remaining implants and occlusal adjustment. The patient was followed up for one year with no signs of recurrence or complaints about the proposed treatment.
Surgical planning for dental implants must be thorough and always consider the patient’s general condition [
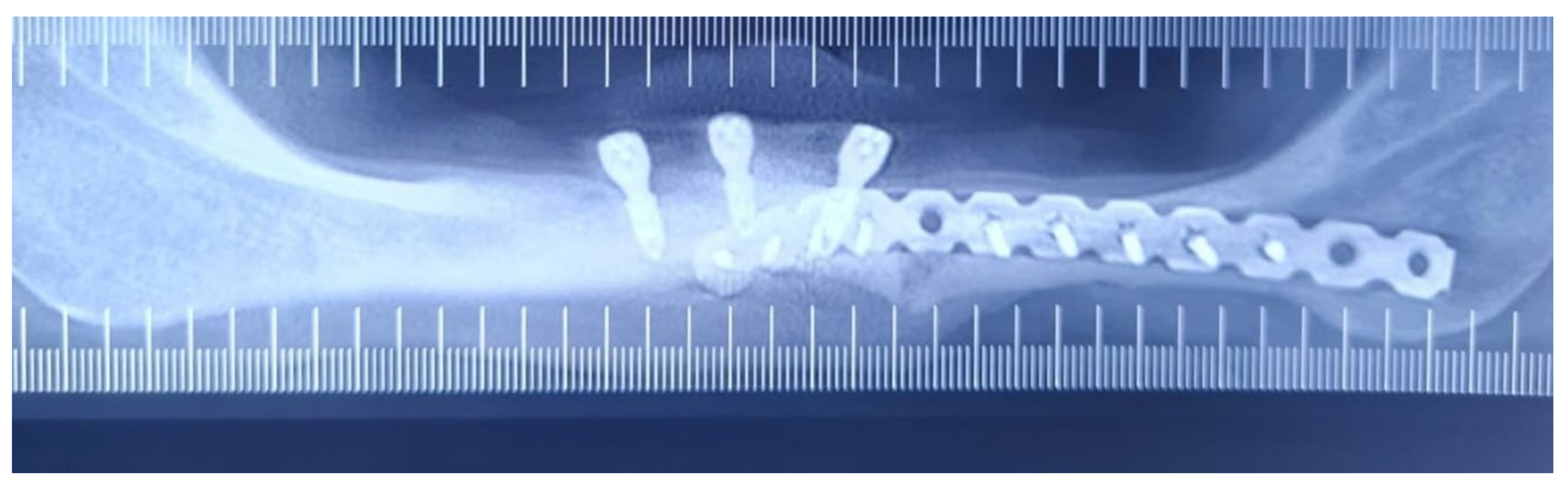
19]. Assessment of the cause of tooth loss is essential for the proposed rehabilitation to ensure longevity and a better chance of success. Following the diagnosis of osteoporosis, the patient’s panoramic radiograph (
Figure 2) showed diffuse radiolucent images, suggesting a high degree of bone involvement and resorption in this unusual case of a man under 60 years of age. The anterior mandibular bone image was normal for the patient’s age, with no limiting atrophy, making it even more difficult to determine the local bone density in advance. As the patient reported that extractions and immediate implant placement were performed during the dental implant surgery, the diagnosis of bone quality via surgery is limited by the smaller number of perforations required during the surgical procedure.
The proposed treatment to eradicate the osteomyelitis, fix the mandibular fracture, and rehabilitate the occlusion was uneventful and well accepted by the patient, who preferred not to have further implants at time of writing. One-year follow-up revealed a good buccal condition with normal function and acceptable aesthetics.
2. Case Report
A 55-year-old male patient was admitted to the Unimed Hospital in Sao Carlos, Sao Paulo, Brazil, as an emergency patient on 28 December 2022. He reported having undergone dental implant surgery (four implants in the mandible for immediate prosthesis placement) in November 2022. A full denture was fitted over the implants one week later. He reported severe pain in the fracture area on the day the prosthesis was fitted. In December of the same year, the pain increased. Physical examination revealed gingival bleeding in the region of implant related to tooth 34, a left submandibular abscess with fistula and suppuration. Crepitus and mobility suggestive of fracture were noted, as well as pain on palpation and mouth opening. The complete blood count showed an elevated white blood cell count (11.1 million red blood cells per microliter of blood), confirming osteomyelitis, which was also clinically diagnosed via signs and symptoms for more than 3 weeks, as well as X-rays showing bone damage.
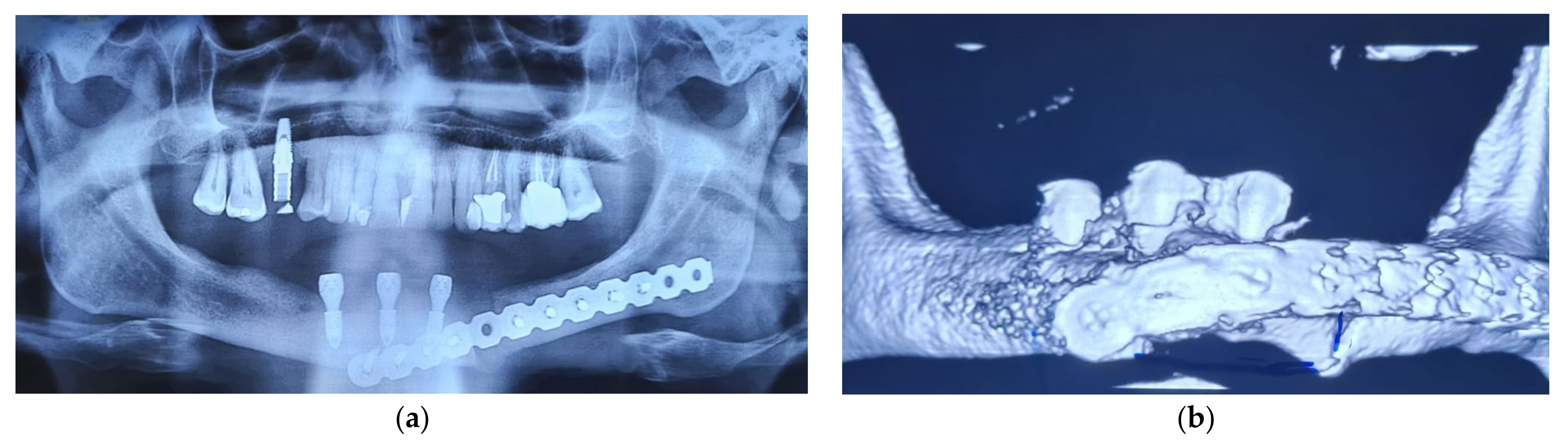
Treatment planning can be divided into two parts: clinical and surgical. Both are complementary and depend on intensive monitoring to assess the evolution of the infectious process (osteomyelitis). Urgent therapy was started immediately in the emergency department due to localized pain and a localized abscess (
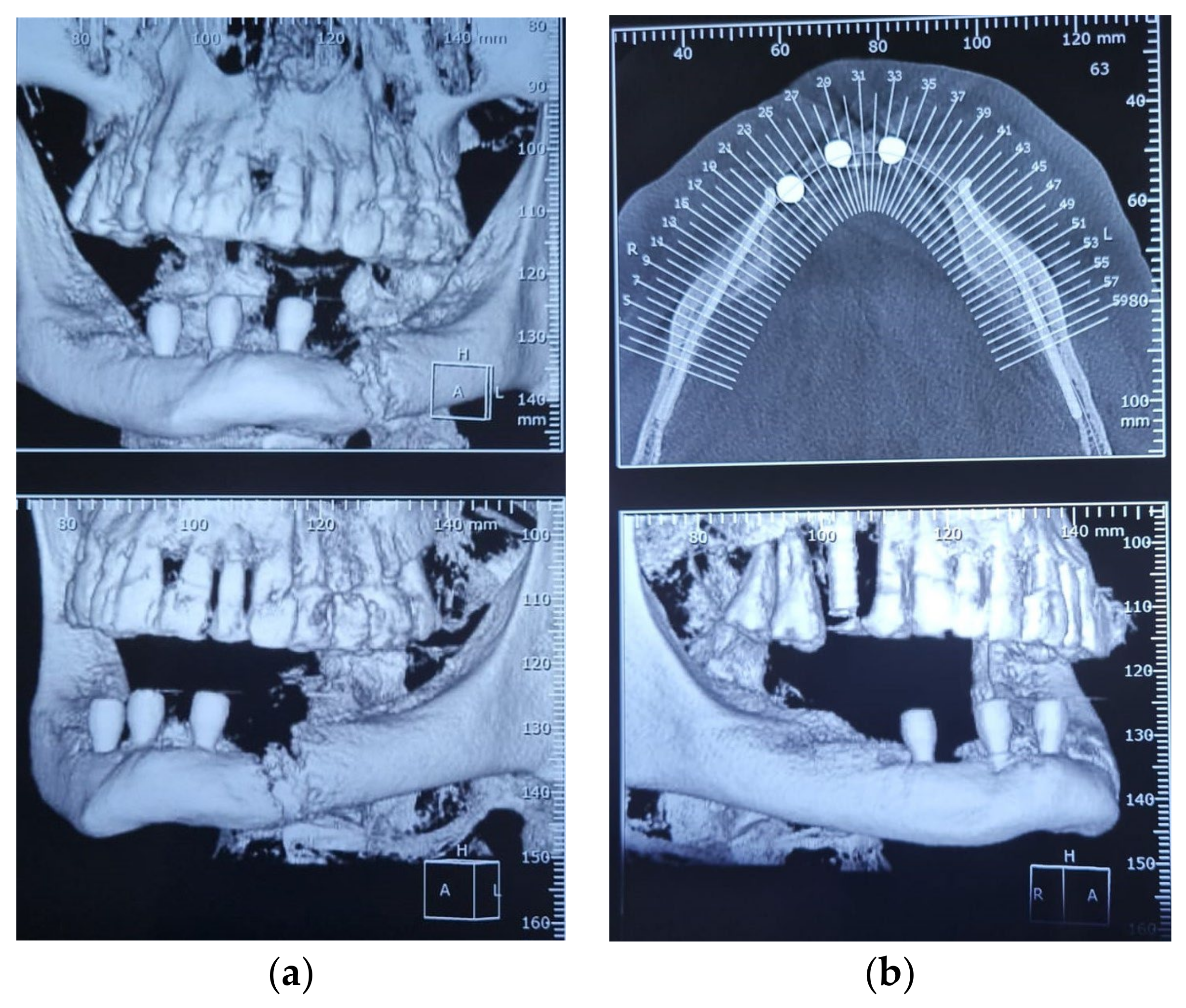
Figure 1a). Antibiotic therapy was started with a combination of amoxicillin and clavulanic acid 875 g 8/8 h continued for 15 days. Mouthwash every 4/4 h (malvona solution) for the entire duration of the proposed treatment. A CT scan of the mandible and craniofacial region was obtained (
Figure 3). The abscess was drained extra-orally and Penrose drains were placed to ensure maximum removal of necrotic material to facilitate organ response. During the drainage of the abscess, material was collected for culture and antibiogram in case the proposed antibiotic treatment failed, thus speeding up the identification of the causative agents of the infection. Analgesics were administered (metamizole 1 g 8/8 h 5 days), and the patient was discharged for outpatient follow-up. The Penrose drain was removed after 5 days.
Three weeks after abscess drainage and antibiotic therapy, the patient had no clinical signs of infection, and the wound was not communicating with the oral environment. Laser therapy [wavelength: 660 nm (red laser) and 808 nm (infrared laser), MMO Optics, Sao Carlos SP, Brazil] was applied twice a week for the duration of the remaining treatment. Routine preoperative tests were ordered for the management of the pathological mandibular fracture, with the addition of a diagnostic test for osteoporosis (dual energy X-ray absorptiometry, DEXA) given the patient’s fracture. DEXA confirmed the diagnosis of severe osteoporosis (a T-score greater than −2.5), which had not been observed prior to the previous implant surgery.
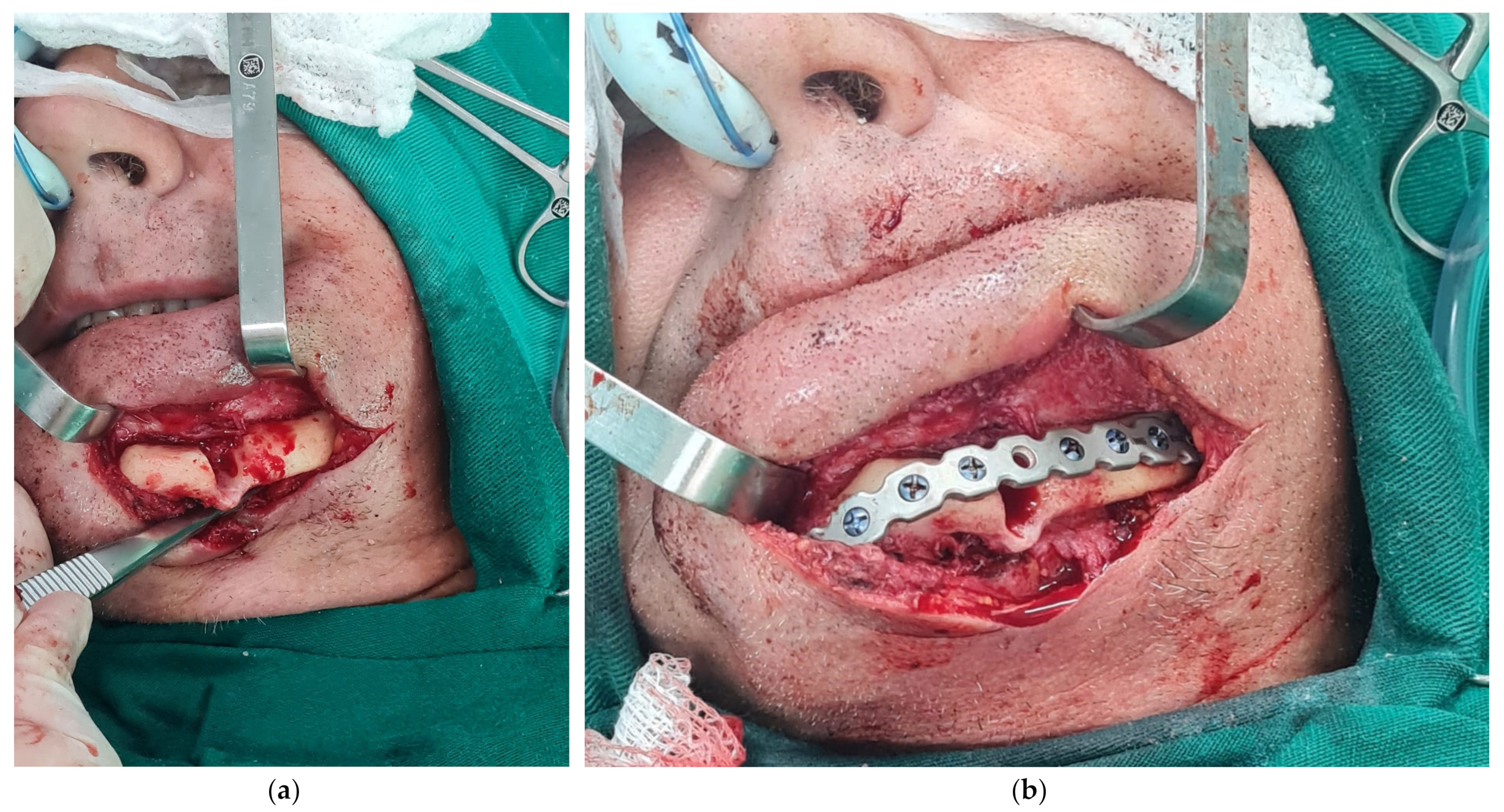
The operation to treat the mandibular fracture was planned under general anaesthesia and naso-tracheal intubation with monitoring of vital parameters. The patient was placed in a supine position under aseptic and antiseptic conditions. Surgical drapes were placed to isolate the surgical field from contamination, leaving the left side of the mandible exposed. A regional anaesthetic block was applied to the mandibular inferior alveolar nerve with lidocaine 2% adrenaline (1:200,000) and local infiltration of the surgical area. A submandibular incision was made, following the facial lines, and dissected in planes until the fractured mandible was fully exposed. The necrotic tissue was debrided and removed, leaving vivid bleeding at the margins of the fractured segments of the mandible (
Figure 4). The fracture was manually aligned and repositioned using stabilizing clamps, and a 2.0 mini plate was adapted to the anatomy of the mandible for fixation. Titanium screws included in the 2.0/2.4 mm locking system kit (Toride Company Ltd., Mogi Mirim, Sao Paulo, Brazil) were used to fix and stabilize the mandibular fracture. Tissue was repositioned and sutured in planes. The skin was sutured with 3.0 nylon sutures as a strong wound closure was required to avoid recontamination of the deep bone planes. The operation was uneventful, and the patient was taken to the post-anaesthesia room for 4 h and then returned to his bed. He was discharged from hospital the following day and continued to be monitored on an outpatient basis.
The patient was treated with prophylactic antibiotics (amoxicillin and clavulanic acid 875 mg 8/8 h for 7 days) and the sutures were removed after 7 days with no evidence of recurrent infection. Three months after surgery, oral rehabilitation began with a prosthesis on the three remaining implants. A transfer mould was used to fabricate the metal structure in the laboratory to support the overdenture and also to adjust the occlusion with the upper dental arch with permanent teeth. Careful occlusal adjustment is essential, especially considering the force distribution of the natural teeth on the weakened mandible with osteoporosis and the presence of dental implants in the region. A less rigid material (composite resin) was used to fabricate the prosthetic teeth in order to better distribute the mechanical chewing forces. After the prosthesis was fitted, weekly occlusal adjustments were made until a good distribution of contact points was achieved with maximum intercuspation and mandibular laterality (
Figure 5b). The patient was followed up for one year without any abnormalities, complaints of pain, or parafunctions.
3. Results
The results obtained were satisfactory considering the complexity of osteomyelitis treatment and the potential complicating treatment factors, particularly in cases of oral microbiota contamination. The patient’s fracture was adequately aligned and immobilized without compromising occlusal rehabilitation with the prosthesis on the implants. It was decided not to place new implants in the region, mainly due to the patient’s lack of enthusiasm for this treatment option. The patient was informed of the risks and benefits of the proposed treatment and gave his informed consent for his case to be published. The case was followed for one year postoperatively (
Figure 5b) with no complaints or complications. There were no patient-reported symptoms or signs of paraesthesia at any time during treatment.
4. Discussion
The clinical case presented in this article discusses basic concepts and principles that all surgeons should be familiar with. It also examines an atypical situation of a mandibular fracture associated with osteomyelitis and osteoporosis in a male patient under the age of 60, following an immediate dental implant protocol in a fully edentulous mandible. The fracture in the left parasymphyseal area of the mandible may be related to osteoporosis, bone perforation for implants, and the general location of the mental foramen, which is usually posteriorized in totally edentulous individuals [
20]. Considering the anatomical features discovered during the surgical procedure, it is likely that there was a vestibular misalignment of the implant at this site, as shown in
Figure 3 and
Figure 4. The adaptive bone response at the base of the mandible can also be seen in these images, altering its typical anatomy. The presence of a drainage and extraoral fistula, despite the presence of intraoral communication, suggests that the fracture occurred in microcracks during the drilling and screwing of the dental implant for fixation [
21,
22,
23].
It is known that osteoporosis associated with bone loss due to tooth loss or edentulism and the corresponding alveolar bone are factors that contribute to the weakening of the mandibular resistance and the consequent increased risk of fracture [
24,
25]. A better understanding of the fracture risks in immediate dental implant protocols enriches the safety and efficacy of treatment and provides more information that allows better control of the short and long-term outcomes of osseointegrated implants. The occurrence of localized infection and its development into chronic infection in cases of implant treatment demonstrates the need for a shorter follow-up period between consultations in these cases, in addition to the patient’s own clarification of the necessary personal care [
26,
27].
The authors were unable to find a study describing a case of a patient with both osteoporosis and osteomyelitis. It was found that by removing the source of infection (implant at the fracture site, necrotic soft and hard tissues), reviving medullary bleeding in the mandible, repositioning, and immobilisation with rigid internal fixation, it was possible to treat the osteomyelitis and fracture simultaneously with the proposed treatment without major complications and without the need for prolonged antibiotic treatment. It is thought that the lower bone density did not compromise blood flow, allowing for continuous and appropriate antibiotic dosing to the infected area—thus allowing for permeability [
28,
29]. Treatment of mandibular fractures in totally edentulous patients can be performed without an intermaxillary block, as the fine occlusal adjustment is made during prosthesis fitting. The use of the Miniplate 2.0, used in cases with a greater need to withstand mechanical forces, was determined based on the absence of the intermaxillary block, which guarantees the immobility of the bone segments in the presence of a poor fit between them due to resorption caused by chronic infection and low bone density, avoiding as much as possible the need for a second surgical treatment [
30].
Clinical evaluations throughout the treatment period revealed a tendency for plaque to form around the implant healers. The probable cause of the loss of the natural teeth was a trauma to the occlusion, aggravating the periodontal disease, and the process was repeated with the dental implants, where the jaw was weakened by the vestibular insertion of the implant in the region of the alveolus of tooth 34 and the low bone density favoured the occurrence of fractures after the immediate placement of the implant prosthesis [
14,
15,
16]. There is also the possibility that the fracture was pathological, with periimplantitis contaminating the deep tissues due to the absence of the vestibular (external) cortical bone wall (
Figure 3 and
Figure 4), and that the fracture occurred at the most fragile site due to the low bone density and high masticatory force of the natural teeth in the maxillary arch. In this case, the diagnosis would be a pathological fracture due to iatrogeny, which cannot be ruled out or confirmed because the patient was not followed by the same team during the initial rehabilitation and immediately after the fracture. Implant-supported overdentures conserve bone because of their positive load-related effect on the jaw, so keeping the implants in place and actively loading the overdenture improved the long-term results. Making general practitioners and specialists aware of the possibility of diagnosing osteoporosis through routine dental X-rays, such as panoramic X-rays (
Figure 6 and
Figure 7), will increase the chances of preventing these diseases from becoming more serious and allow more accurate treatment decisions to be made [
31,
32].
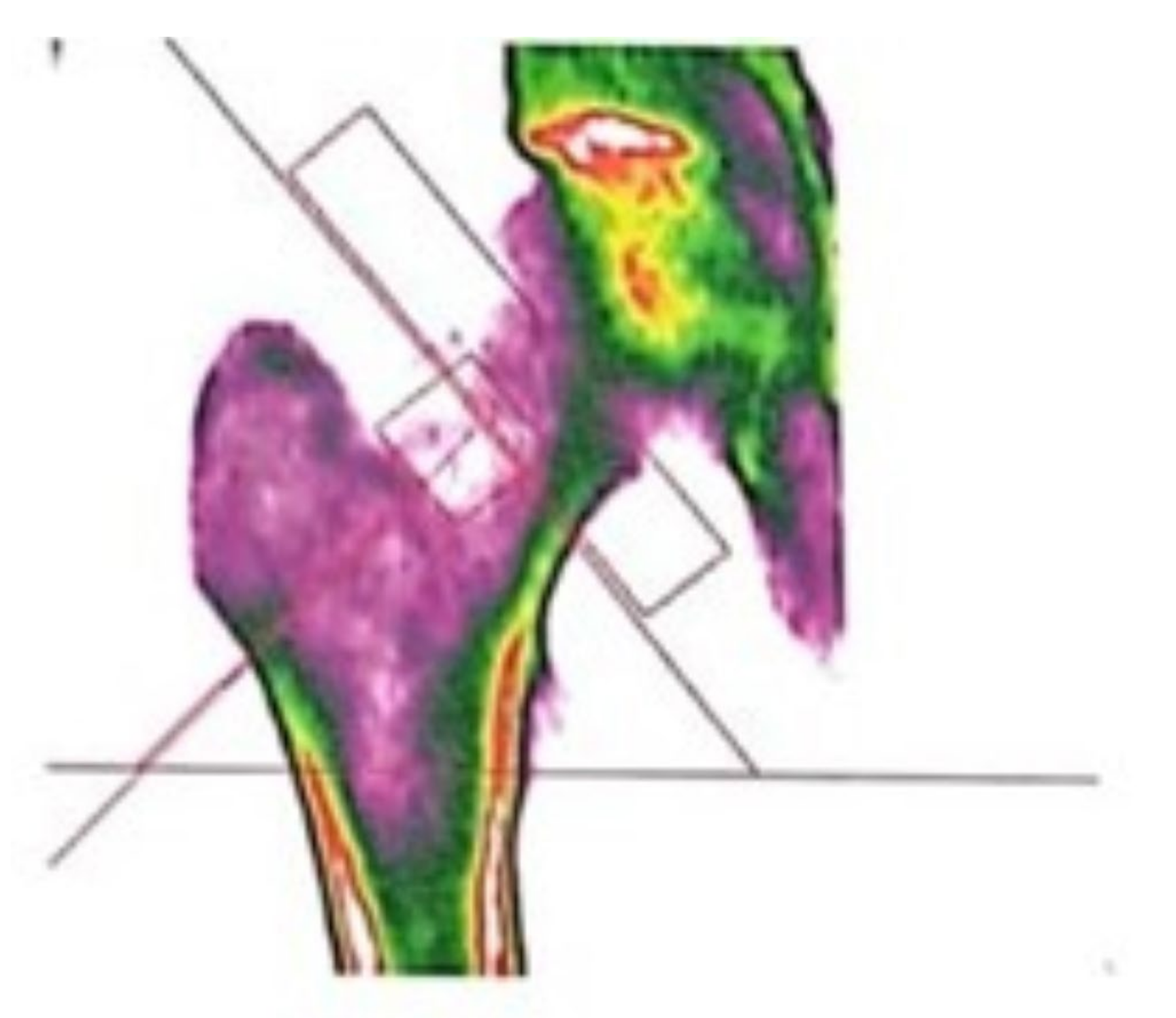
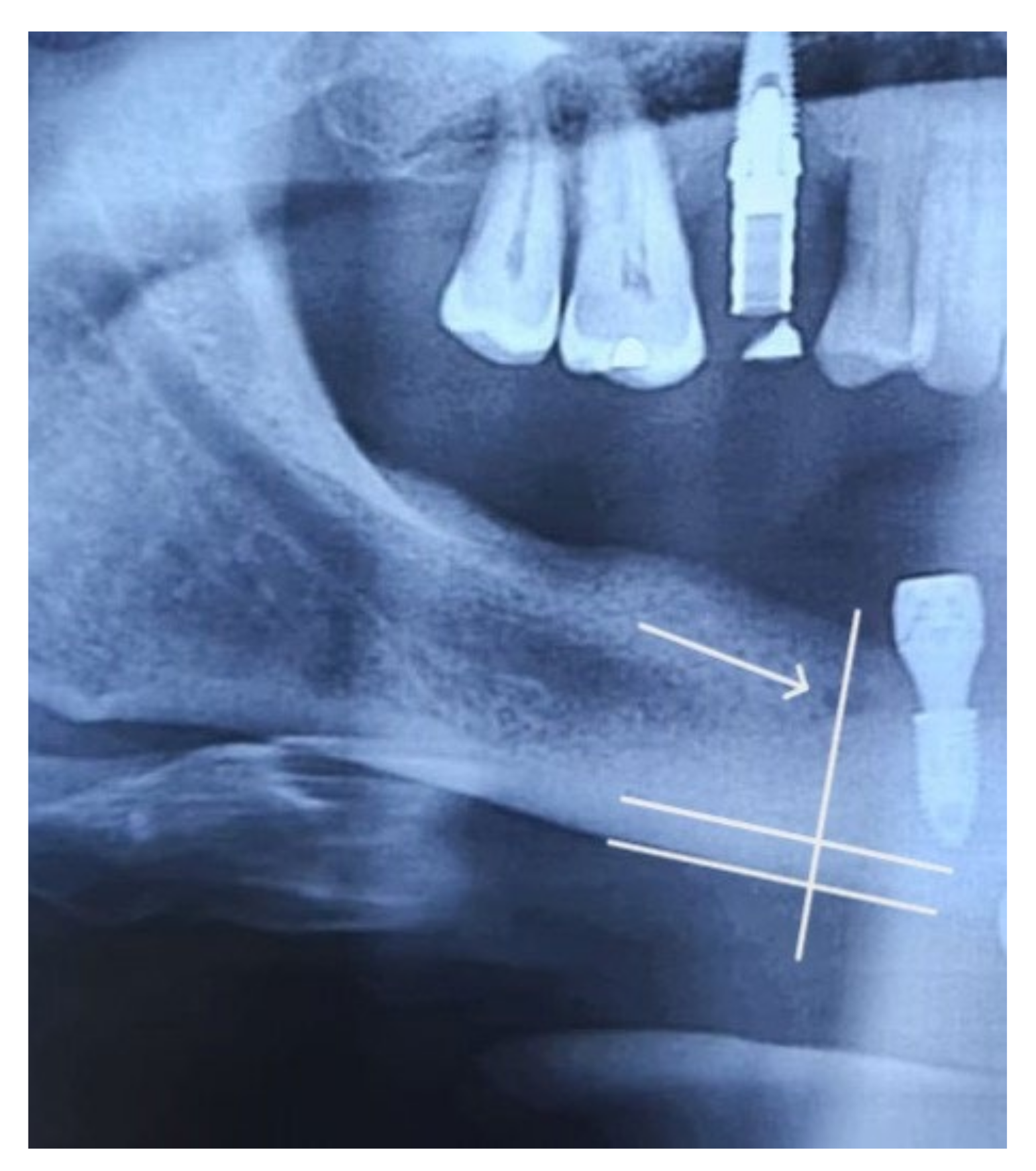
To assess osteoporotic changes in the oral cavity, several investigators have proposed indices derived from panoramic radiographs, such as the mandibular cortical index, the mandibular panoramic index, and the Wical and Swoope technique (
Figure 8). All of these techniques assess the basal region of the mandible, posterior to the mandibular foramen, because this area meets the requirement for less inter- and intra-individual variation in anatomy, shape, bone structure, and function. This would allow dentists to correctly refer patients for specific treatment and also to assess the patient’s bone quality, which is of great importance when planning dental implants [
33,
34]. Identifying asymptomatic people at risk of osteoporosis in general dental practice could help to reduce the incidence of first fractures, secondary fractures, medical costs, and mortality associated with osteoporotic fragility fractures.
Assessment of the cause of the loss of natural teeth, the relationship of occlusal forces between the dental arches based on the presence or absence of natural teeth and/or dentures, and fine occlusal adjustment are fundamental to the short- and long-term success of oral rehabilitation. The patient’s general condition contributes to and determines the progress of the proposed treatment. The importance of the clinician managing the complications of mandibular fractures and mastering the occlusion and overall oral pathophysiology has already been established in order to achieve excellence in treatment. The management of craniofacial trauma is a multidisciplinary field and should therefore be considered whenever necessary for the benefit of the patient. The need for continuing professional development is undeniable, as is the need for further research in this area. Although this is a case report, the combined concepts described here may assist in the planning of future cases and highlight the need for further research into the effects of severe infectious processes in patients with osteoporosis.
5. Conclusions
An accurate initial emergency diagnosis, confirmed and supported as definitive by complementary examinations, is the fundamental factor in selecting and planning the emergency treatment that will provide the best biological conditions for achieving the best results in the face of the proposed definitive treatment. The attention paid to the accurate initial diagnosis of osteomyelitis in the presence of a pathological fracture following the fixation of dental implants and prostheses in the mandible made it possible to choose a simple and effective emergency therapy, consisting of draining the localized abscess, cleaning the wound, antibiotic therapy, taking a culture, and an antibiogram. The proposed definitive treatment, once the infection had been eliminated and the wound properly closed extra- and intra-orally, allowed the necrotic tissue to be removed through an extra-oral submandibular surgical approach and the mandibular segments to be prepared to restore the continuity of the mandible bone after the fracture had been repositioned and fixed with a rigid mini-plate and screws. Oral rehabilitation with an implant-borne prosthesis provided the function and aesthetics desired by the patient, and the one-year follow-up demonstrated the success of the proposed treatment.
Author Contributions
Conceptualization, C.A.A. (Carlos Aurelio Andreucci) and C.A.A. (Calber Artur Andreucci); methodology, C.A.A. (Calber Artur Andreucci); formal analysis, C.A.A. (Carlos Aurelio Andreucci); investigation, M.M.; resources, M.M.; writing—original draft preparation, C.A.A. (Carlos Aurelio Andreucci); writing—review and editing, C.A.A. (Carlos Aurelio Andreucci); visualization, C.A.A. (Calber Artur Andreucci); supervision, C.A.A. (Calber Artur Andreucci); project administration, C.A.A. (Carlos Aurelio Andreucci). All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Written informed consent has been obtained from the patient to publish this paper.
Data Availability Statement
The data presented in this study are available on request from the corresponding author. The data are not publicly available due to privacy.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Rowe, N.L. The history of the treatment of maxillo-facial trauma. Ann. R. Coll. Surg. Engl. 1971, 49, 329–349. [Google Scholar] [PubMed]
- Brocke, T.; Barr, J. The History of Wound Healing. Surg. Clin. N. Am. 2020, 100, 787–806. [Google Scholar] [CrossRef] [PubMed]
- Lisiak-Myszke, M.; Marciniak, D.; Bieliński, M.; Sobczak, H.; Garbacewicz, Ł.; Drogoszewska, B. Application of Finite Element Analysis in Oral and Maxillofacial Surgery—A Literature Review. Materials 2020, 13, 3063. [Google Scholar] [CrossRef] [PubMed]
- Woodard, S.C. The Story of the Mobile Army Surgical Hospital. Mil. Med. 2003, 168, 503–513. [Google Scholar] [CrossRef]
- King, B.; Jatoi, I. The mobile Army surgical hospital (MASH): A military and surgical legacy. J. Natl. Med. Assoc. 2005, 97, 648–656. [Google Scholar] [PubMed]
- Garry, D.J. Successful Health Care Delivery Using Ambulatory Hospitals-Past, Present, and Future. Am. J. Med. 2020, 133, e539–e540. [Google Scholar] [CrossRef] [PubMed]
- Munante-Cardenas, J.L.; Nunes, P.H.F.; Passeri, L.A. Etiology, treatment, and complications of mandibular fractures. J. Craniofac. Surg. 2015, 26, 611–615. [Google Scholar] [CrossRef] [PubMed]
- Chrcanovic, B.R.; Abreu, M.H.; Freire-Maia, B.; Souza, L.N. 1454 mandibular fractures: A 3-year study in a hospital in Belo Horizonte, Brazil. J. Craniomaxillofac. Surg. 2012, 40, 116–123. [Google Scholar] [CrossRef]
- Kern, J.S.; Kern, T.; Wolfart, S.; Heussen, N. A systematic review and meta-analysis of removable and fixed implant-supported prostheses in edentulous jaws: Post-loading implant loss. Clin. Oral Implant. Res. 2016, 27, 174–195. [Google Scholar] [CrossRef]
- Papaspyridakos, P.; Chen, C.J.; Chuang, S.K.; Weber, H.P. Implant loading protocols for edentulous patients with fixed prostheses: A systematic review and meta-analysis. Int. J. Oral Maxillofac. Implant. 2014, 29, 256–270. [Google Scholar] [CrossRef]
- Darriba, I.; Seidel, A.; Moreno, F.; Botelho, J.; Machado, V.; Mendes, J.J.; Leira, Y.; Blanco, J. Influence of low insertion torque values on survival rate of immediately loaded dental implants: A systematic review and meta-analysis. J. Clin. Periodontol. 2023, 50, 158–169. [Google Scholar] [CrossRef]
- Elawady, D.M.; Ibrahim, W.I.; Osman, R.B. Clinical evaluation of implant overdentures fabricated using 3D-printing technology versus conventional fabrication techniques: A randomized clinical trial. Int. J. Comput. Dent. 2021, 24, 375–384. [Google Scholar] [PubMed]
- Yang, Y.; Yang, Z.; Lin, W.S.; Chen, L.; Tan, J. Digital Duplication and 3D Printing for Implant Overdenture Fabrication. J. Prosthodont. 2021, 30, 139–142. [Google Scholar] [CrossRef] [PubMed]
- Chrcanovic, B.R.; Custódio, A.L. Mandibular fractures associated with endosteal implants. Oral Maxillofac. Surg. 2009, 13, 231–238. [Google Scholar] [CrossRef] [PubMed]
- Naval-Gías, L.; Rodriguez-Campo, F.; Naval-Parra, B.; Sastre-Pérez, J. Pathological mandibular fracture: A severe complication of periimplantitis. J. Clin. Exp. Dent. 2015, 7, e328–e332. [Google Scholar] [CrossRef] [PubMed]
- Carls, F.R.; Pajarola, G.; Sailer, H.F. Unterkieferfrakturen infolge Implantatversorgung--Inzidenz, Verletzungsmechanismen und therapeutische Besonderheiten [Mandibular fractures due to implant management--incidence, mechanism of injury and therapeutic characteristics]. Fortschr. Kiefer Gesichtschir. 1996, 41, 106–108. [Google Scholar] [PubMed]
- Suei, Y.; Taguchi, A.; Tanimoto, K. Diagnosis and classification of mandibular osteomyelitis. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2005, 100, 207–214. [Google Scholar] [CrossRef] [PubMed]
- Fenelon, M.; Gernandt, S.; Aymon, R.; Scolozzi, P. Identifying Risk Factors Associated with Major Complications and Refractory Course in Patients with Osteomyelitis of the Jaw: A Retrospective Study. J. Clin. Med. 2023, 12, 4715. [Google Scholar] [CrossRef]
- Conejo, J.; Atria, P.J.; Schweitzer, D.; Blatz, M.B. Digital Implant Planning and Surgical Guides: Tools for Clinical Success. Compend. Contin. Educ. Dent. 2021, 42, 400–401. [Google Scholar]
- Charalampakis, A.; Kourkoumelis, G.; Psari, C.; Antoniou, V.; Piagkou, M.; Demesticha, T.; Kotsiomitis, E.; Troupis, T. The position of the mental foramen in dentate and edentulous mandibles: Clinical and surgical relevance. Folia Morphol. 2017, 76, 709–714. [Google Scholar] [CrossRef]
- Li, Z.; Helms, J.A. Drill Hole Models to Investigate Bone Repair. Methods Mol. Biol. 2021, 2221, 193–204. [Google Scholar] [CrossRef]
- Pérez-Pevida, E.; Brizuela-Velasco, A.; Chávarri-Prado, D.; Jiménez-Garrudo, A.; Sánchez-Lasheras, F.; Solaberrieta-Méndez, E.; Diéguez-Pereira, M.; Fernández-González, F.J.; Dehesa-Ibarra, B.; Monticelli, F. Biomechanical Consequences of the Elastic Properties of Dental Implant Alloys on the Supporting Bone: Finite Element Analysis. Biomed Res. Int. 2016, 2016, 1850401. [Google Scholar] [CrossRef]
- Isidor, F. Influence of forces on peri-implant bone. Clin. Oral Implant. Res. 2006, 17, 8–18. [Google Scholar] [CrossRef]
- Korabi, R.; Shemtov-Yona, K.; Dorogoy, A.; Rittel, D. The Failure Envelope Concept Applied to the Bone-Dental Implant System. Sci. Rep. 2017, 7, 2051. [Google Scholar] [CrossRef]
- LeBoff, M.S.; Greenspan, S.L.; Insogna, K.L.; Lewiecki, E.M.; Saag, K.G.; Singer, A.J.; Siris, E.S. The clinician’s guide to prevention and treatment of osteoporosis. Osteoporos. Int. 2022, 33, 2049–2102. [Google Scholar] [CrossRef]
- Bryce, G.; Bomfim, D.I.; Bassi, G.S. Pre- and post-operative management of dental implant placement. Part 2: Management of early-presenting complications. Br. Dent. J. 2014, 217, 171–176. [Google Scholar] [CrossRef]
- Bryce, G.; Bomfim, D.I.; Bassi, G.S. Pre- and post-operative management of dental implant placement. Part 1: Management of post-operative pain. Br. Dent. J. 2014, 217, 123–127. [Google Scholar] [CrossRef] [PubMed]
- Marenzana, M.; Arnett, T.R. The Key Role of the Blood Supply to Bone. Bone Res. 2013, 1, 203–215. [Google Scholar] [CrossRef] [PubMed]
- Ma, H.T.; Griffith, J.F.; Zhao, X.; Lv, H.; Yeung, D.K.; Leung, P.C. Relationship between marrow perfusion and bone mineral density: A pharmacokinetic study of DCE-MRI. In Proceedings of the 2012 Annual International Conference of the IEEE Engineering in Medicine and Biology Society, San Diego, CA, USA, 28 August–1 September 2012. [Google Scholar] [CrossRef]
- Dergin, G.; Emes, Y.; Aybar, B. Evaluation and Management of Mandibular Fracture. IntechOpen 2019, 83024. [Google Scholar] [CrossRef]
- Von Wowern, N. General and oral aspects of osteoporosis: A review. Clin. Oral Investig. 2001, 5, 71–82. [Google Scholar] [CrossRef] [PubMed]
- Oliveira, L.S.A.F.; Neves, F.S.; Torres, M.G.G.; Rabello, I.M.C.R.; Campos, P.S.F. Características radiográficas dos portadores de osteoporose e o papel do cirurgião-dentista no diagnóstico. Rev. Ciências Médicas Biol. 2009, 8, 85–90. [Google Scholar] [CrossRef]
- Wical, K.E.; Swoope, C.C. Studies of residual ridge resorption. Part I. Use of panoramic radiographs for evaluation and classification of mandibular resorption. J. Prosthet. Dent. 1974, 32, 7–12. [Google Scholar] [CrossRef] [PubMed]
- Taguchi, A.; Tsuda, M.; Ohtsuka, M.; Kodama, I.; Sanada, M.; Nakamoto, T.; Inagaki, K.; Noguchi, T.; Kudo, Y.; Suei, Y.; et al. Use of dental panoramic radiographs in identifying younger postmenopausal women with osteoporosis. Osteoporos. Int. 2006, 17, 387–394. [Google Scholar] [CrossRef] [PubMed]
| Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}







