
The Glenoid Track Concept: On-Track and Off-Track—A Narrative Review


 and
and 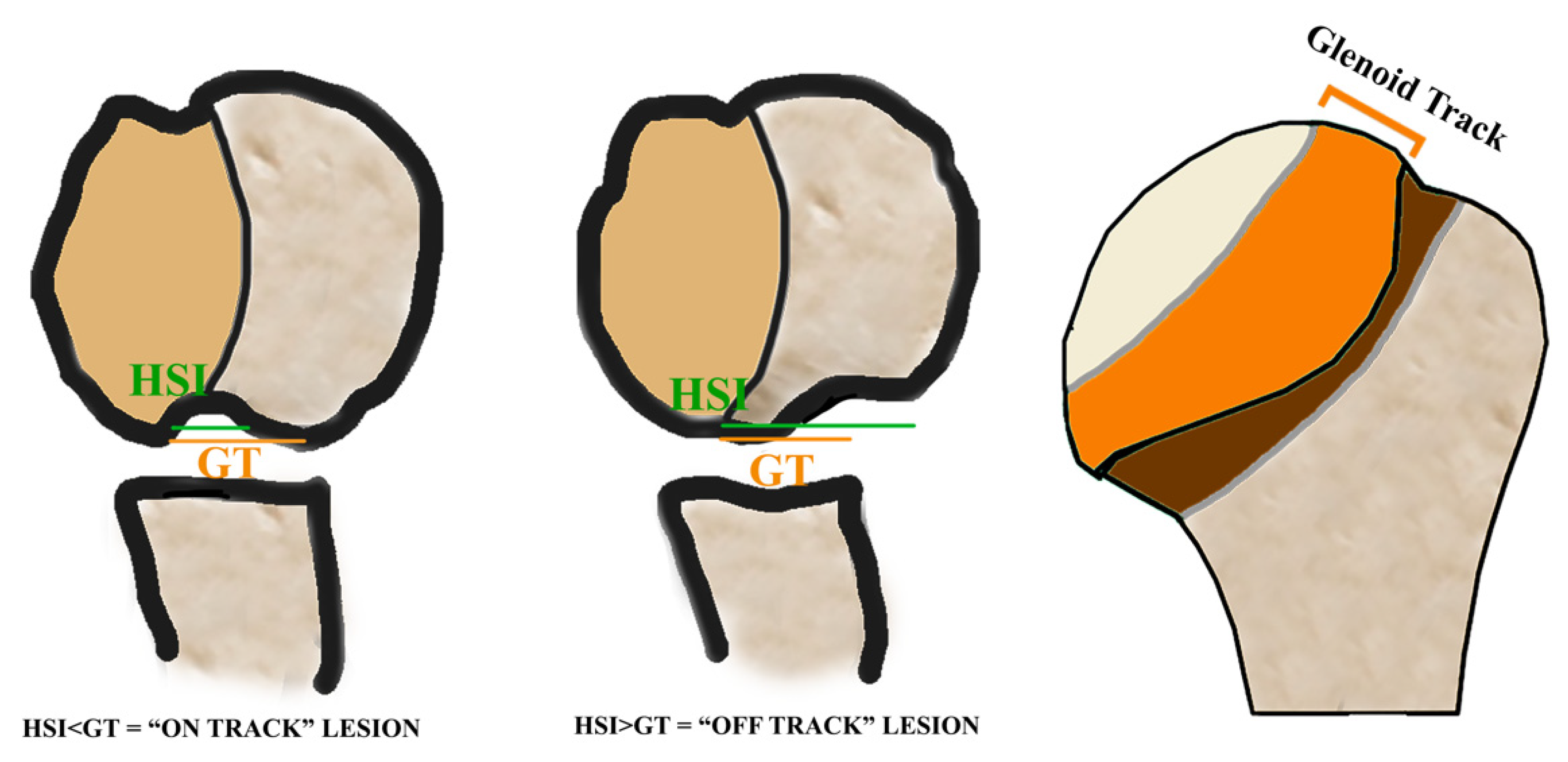{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
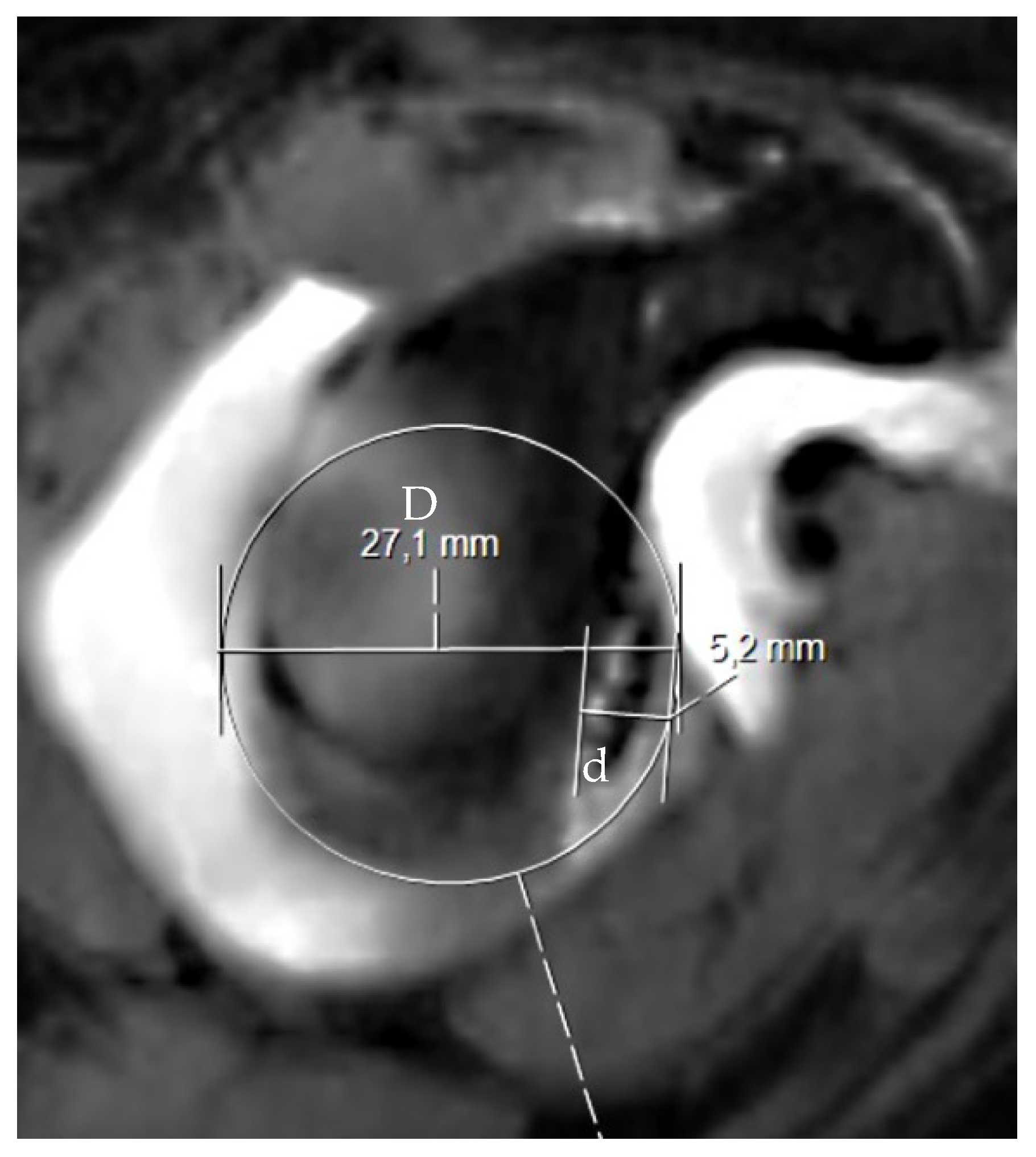
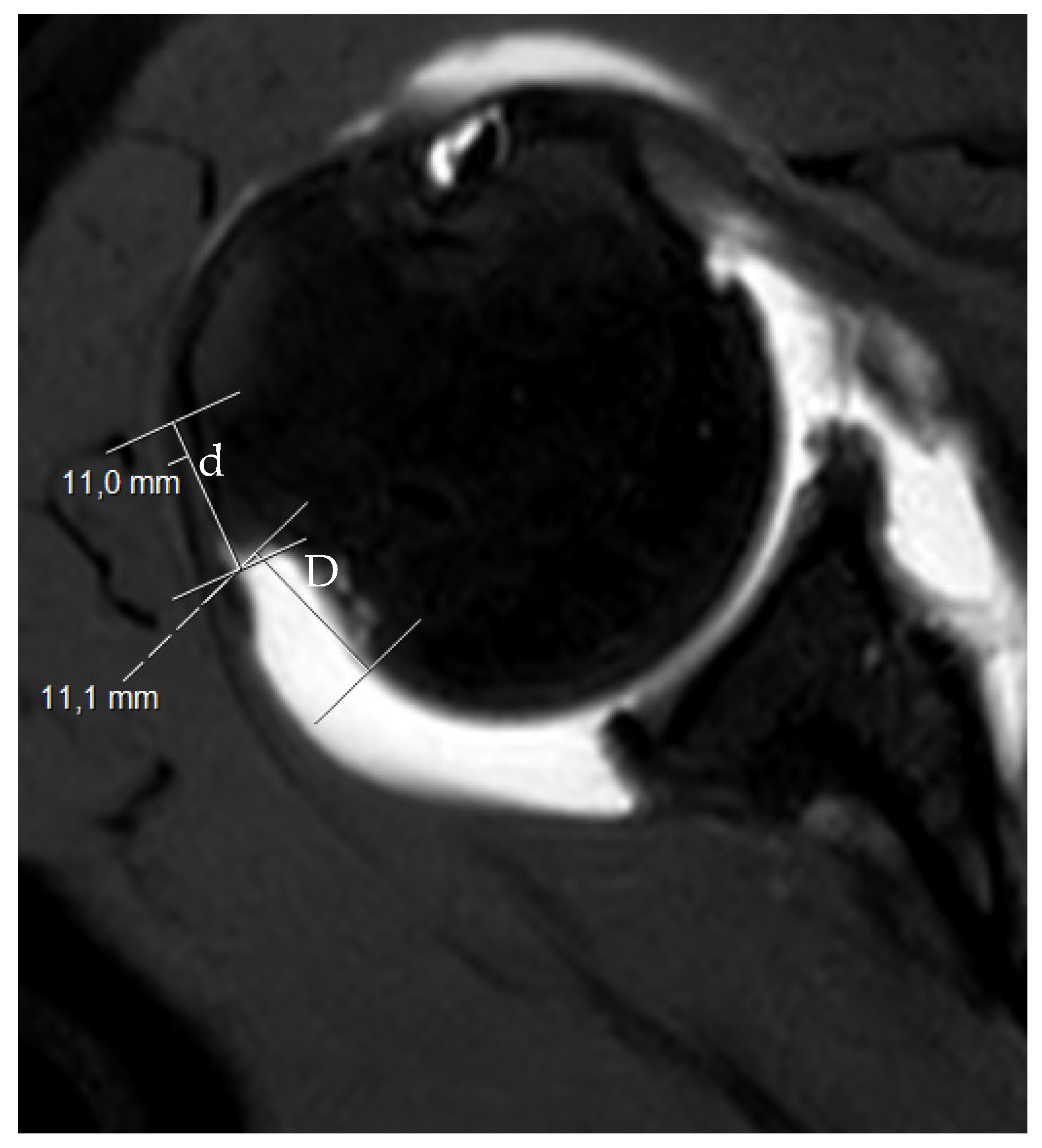
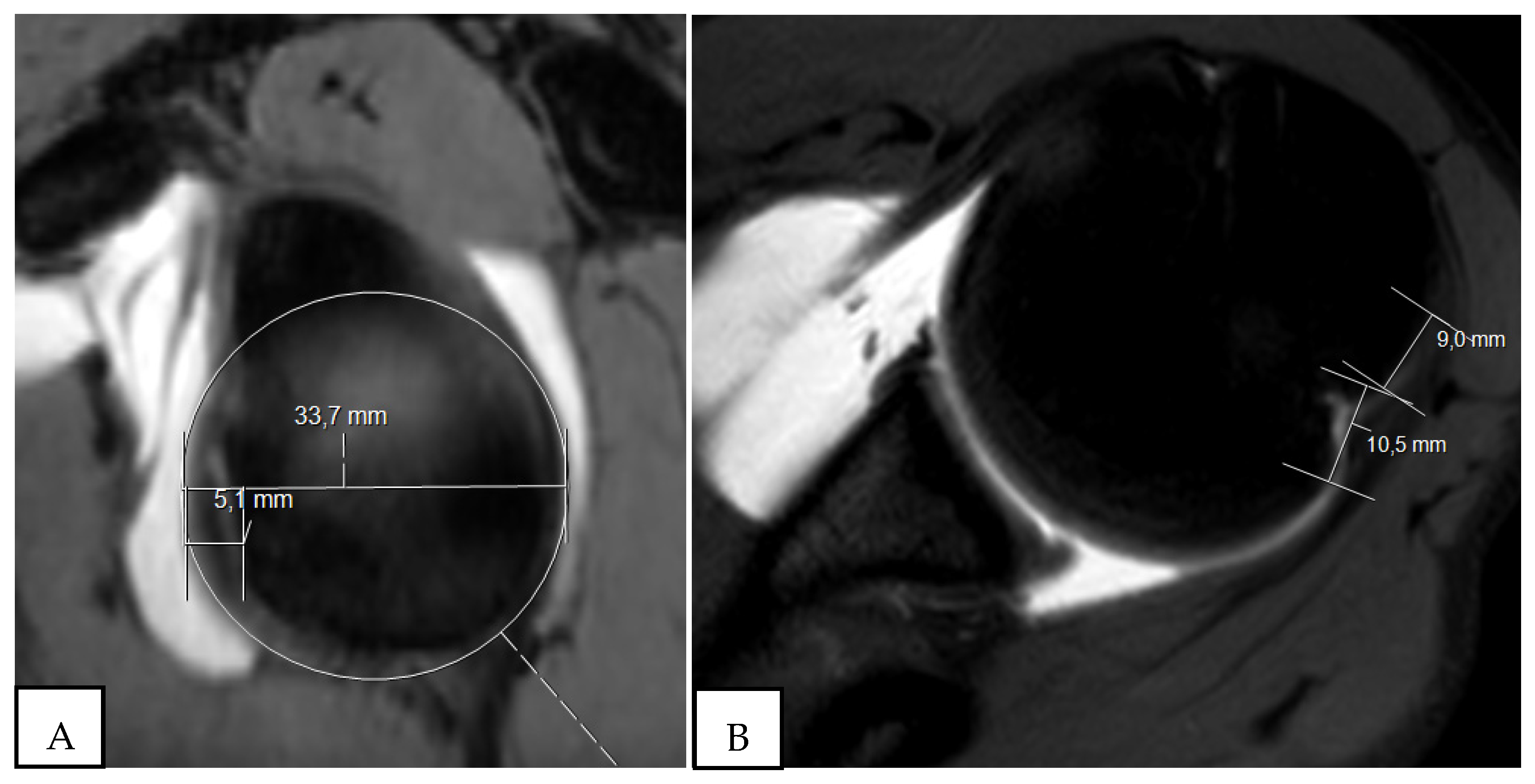
2. The Glenoid Track and Hill–Sachs Lesions: On-Track and Off-Track
3. Clinical Implications of the Glenoid Track Method
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
Abbreviations
| Abduction and external rotation | ABER |
| Glenohumeral Instability | GI |
| Glenoid track | GT |
| Hill–Sachs index | HSI |
| Hill–Sachs lesions | HSL |
| Magnetic Resonance Imaging | MRI |
References
- Gulati, A.; Dessouky, R.; Wadhwa, V.; Sanders, D.; Chhabra, A. New concepts of radiologic preoperative evaluation of anterior shoulder instability: On-track and off-track lesions. Acta Radiol. 2018, 59, 966–972. [Google Scholar] [CrossRef] [PubMed]
- Dumont, G.D.; Russell, R.D.; Robertson, W.J. Anterior shoulder instability: A review of pathoanatomy, diagnosis and treatment. Curr. Rev. Musculoskelet. Med. 2011, 4, 200–207. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Itoi, E.; Lee, S.B.; Amrami, K.K.; Wenger, D.E.; An, K.N. Quantitative assessment of classic anteroinferior bony Bankart lesions by radiography and computed tomography. Am. J. Sports Med. 2003, 31, 112–118. [Google Scholar] [CrossRef] [PubMed]
- Longo, U.G.; Rizzello, G.; Loppini, M.; Locher, J.; Buchmann, S.; Maffulli, N.; Denaro, V. Multidirectional Instability of the Shoulder: A Systematic Review. Arthroscopy 2015, 31, 2431–2443. [Google Scholar] [CrossRef]
- Longo, U.G.; Huijsmans, P.E.; Maffulli, N.; Denaro, V.; De Beer, J.F. Video analysis of the mechanisms of shoulder dislocation in four elite rugby players. J. Orthop. Sci. 2011, 16, 389–397. [Google Scholar] [CrossRef]
- Longo, U.G.; Papalia, R.; Ciapini, G.; De Salvatore, S.; Casciaro, C.; Ferrari, E.; Cosseddu, F.; Novi, M.; Piergentili, I.; Parchi, P.; et al. Instability Severity Index Score Does Not Predict the Risk of Shoulder Dislocation after a First Episode Treated Conservatively. Int. J. Environ. Res. Public Health 2021, 18, 12026. [Google Scholar] [CrossRef]
- Fritch, J.; Parekh, A.; Labbe, A.; Courseault, J.; Savoie, F.; Longo, U.G.; De Salvatore, S.; Candela, V.; Di Naro, C.; Casciaro, C.; et al. Orthopaedic Biomechanics of the Throwing Shoulder; Springer: Cham, Switzerland, 2021. [Google Scholar]
- Longo, U.G.; Candela, V.; Berton, A.; Naro, C.D.; Migliorini, F.; Schena, E.; Denaro, V. Epidemiology of shoulder instability in Italy: A 14-years nationwide registry study. Injury 2021, 52, 862–868. [Google Scholar] [CrossRef]
- Provencher, M.T.; Frank, R.M.; Leclere, L.E.; Metzger, P.D.; Ryu, J.J.; Bernhardson, A.; Romeo, A.A. The Hill-Sachs lesion: Diagnosis, classification, and management. J. Am. Acad. Orthop. Surg. 2012, 20, 242–252. [Google Scholar] [CrossRef] [Green Version]
- Fox, J.A.; Sanchez, A.; Zajac, T.J.; Provencher, M.T. Understanding the Hill-Sachs Lesion in Its Role in Patients with Recurrent Anterior Shoulder Instability. Curr. Rev. Musculoskelet. Med. 2017, 10, 469–479. [Google Scholar] [CrossRef] [Green Version]
- Itoi, E. Editorial Commentary: It Is Not the Size, But the Location of Hill-Sachs Lesion That Matters. Arthroscopy 2021, 37, 3262–3265. [Google Scholar] [CrossRef]
- Itoi, E. ‘On-track’ and ‘off-track’ shoulder lesions. EFORT Open Rev. 2017, 2, 343–351. [Google Scholar] [CrossRef] [PubMed]
- Saito, H.; Itoi, E.; Sugaya, H.; Minagawa, H.; Yamamoto, N.; Tuoheti, Y. Location of the glenoid defect in shoulders with recurrent anterior dislocation. Am. J. Sports Med. 2005, 33, 889–893. [Google Scholar] [CrossRef] [PubMed]
- Di Giacomo, G.; Itoi, E.; Burkhart, S.S. Evolving concept of bipolar bone loss and the Hill-Sachs lesion: From “engaging/non-engaging” lesion to “on-track/off-track” lesion. Arthroscopy 2014, 30, 90–98. [Google Scholar] [CrossRef] [PubMed]
- Younan, Y.; Wong, P.K.; Karas, S.; Umpierrez, M.; Gonzalez, F.; Jose, J.; Singer, A.D. The glenoid track: A review of the clinical relevance, method of calculation and current evidence behind this method. Skeletal Radiol. 2017, 46, 1625–1634. [Google Scholar] [CrossRef]
- Locher, J.; Wilken, F.; Beitzel, K.; Buchmann, S.; Longo, U.G.; Denaro, V.; Imhoff, A.B. Hill-Sachs Off-track Lesions as Risk Factor for Recurrence of Instability After Arthroscopic Bankart Repair. Arthroscopy 2016, 32, 1993–1999. [Google Scholar] [CrossRef] [PubMed]
- Longo, U.G.; Loppini, M.; Rizzello, G.; Romeo, G.; Huijsmans, P.E.; Denaro, V. Glenoid and humeral head bone loss in traumatic anterior glenohumeral instability: A systematic review. Knee Surg. Sports Traumatol. Arthrosc. 2014, 22, 392–414. [Google Scholar] [CrossRef] [PubMed]
- Longo, U.G.; Loppini, M.; Rizzello, G.; Ciuffreda, M.; Berton, A.; Maffulli, N.; Denaro, V. Remplissage, humeral osteochondral grafts, weber osteotomy, and shoulder arthroplasty for the management of humeral bone defects in shoulder instability: Systematic review and quantitative synthesis of the literature. Arthroscopy 2014, 30, 1650–1666. [Google Scholar] [CrossRef]
- Trivedi, S.; Pomerantz, M.L.; Gross, D.; Golijanan, P.; Provencher, M.T. Shoulder instability in the setting of bipolar (glenoid and humeral head) bone loss: The glenoid track concept. Clin. Orthop. Relat. Res. 2014, 472, 2352–2362. [Google Scholar] [CrossRef] [Green Version]
- Godinho, A.C.; Godinho, P.C.; França, F.O.; Ribeiro, E.J.S.; de Toledo, D.C.; Franco, G.H. Evaluation of the Glenoid Track Tomographic Method in Magnetic Resonance Imaging/Arthro-MRI. Rev. Bras. Ortop. 2021, 56, 733–740. [Google Scholar] [CrossRef]
- Vopat, M.L.; Peebles, L.A.; McBride, T.; Cirone, I.; Rider, D.; Provencher, C.M.T. Accuracy and Reliability of Imaging Modalities for the Diagnosis and Quantification of Hill-Sachs Lesions: A Systematic Review. Arthroscopy 2021, 37, 391–401. [Google Scholar] [CrossRef]
- Itoi, E.; Lee, S.B.; Berglund, L.J.; Berge, L.L.; An, K.N. The effect of a glenoid defect on anteroinferior stability of the shoulder after Bankart repair: A cadaveric study. J. Bone Jt. Surg. Am. 2000, 82, 35–46. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, N.; Itoi, E.; Abe, H.; Minagawa, H.; Seki, N.; Shimada, Y.; Okada, K. Contact between the glenoid and the humeral head in abduction, external rotation, and horizontal extension: A new concept of glenoid track. J. Shoulder Elbow Surg. 2007, 16, 649–656. [Google Scholar] [CrossRef] [PubMed]
- Burkhart, S.S.; Danaceau, S.M. Articular arc length mismatch as a cause of failed bankart repair. Arthroscopy 2000, 16, 740–744. [Google Scholar] [CrossRef]
- Burkhart, S.S.; De Beer, J.F. Traumatic glenohumeral bone defects and their relationship to failure of arthroscopic Bankart repairs: Significance of the inverted-pear glenoid and the humeral engaging Hill-Sachs lesion. Arthroscopy 2000, 16, 677–694. [Google Scholar] [CrossRef] [Green Version]
- Longo, U.G.; Berton, A.; Khan, W.S.; Maffulli, N.; Denaro, V. Histopathology of rotator cuff tears. Sports Med. Arthrosc. 2011, 19, 227–236. [Google Scholar] [CrossRef] [PubMed]
- Omori, Y.; Yamamoto, N.; Koishi, H.; Futai, K.; Goto, A.; Sugamoto, K.; Itoi, E. Measurement of the Glenoid Track In Vivo as Investigated by 3-Dimensional Motion Analysis Using Open MRI. Am. J. Sports Med. 2014, 42, 1290–1295. [Google Scholar] [CrossRef]
- Gyftopoulos, S.; Beltran, L.S.; Bookman, J.; Rokito, A. MRI Evaluation of Bipolar Bone Loss Using the On-Track Off-Track Method: A Feasibility Study. AJR Am. J. Roentgenol. 2015, 205, 848–852. [Google Scholar] [CrossRef]
- Sugaya, H.; Moriishi, J.; Dohi, M.; Kon, Y.; Tsuchiya, A. Glenoid rim morphology in recurrent anterior glenohumeral instability. J. Bone Jt. Surg. Am. 2003, 85, 878–884. [Google Scholar] [CrossRef]
- Franceschi, F.; Longo, U.G.; Ruzzini, L.; Rizzello, G.; Maffulli, N.; Denaro, V. The Roman Bridge: A “double pulley-suture bridges” technique for rotator cuff repair. BMC Musculoskelet. Disord. 2007, 8, 123. [Google Scholar] [CrossRef] [Green Version]
- Shaha, J.S.; Cook, J.B.; Rowles, D.J.; Bottoni, C.R.; Shaha, S.H.; Tokish, J.M. Clinical Validation of the Glenoid Track Concept in Anterior Glenohumeral Instability. J. Bone Jt. Surg. Am. 2016, 98, 1918–1923. [Google Scholar] [CrossRef]
- Park, I.; Oh, M.J.; Shin, S.J. Effects of Glenoid and Humeral Bone Defects on Recurrent Anterior Instability of the Shoulder. Clin. Orthop. Surg. 2020, 12, 145–150. [Google Scholar] [CrossRef] [PubMed]
- Kurokawa, D.; Yamamoto, N.; Nagamoto, H.; Omori, Y.; Tanaka, M.; Sano, H.; Itoi, E. The prevalence of a large Hill-Sachs lesion that needs to be treated. J. Shoulder Elbow Surg. 2013, 22, 1285–1289. [Google Scholar] [CrossRef] [PubMed]





Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ventura, A.; Smiraglio, C.; Viscomi, A.; De Salvatore, S.; Bertucci, B. The Glenoid Track Concept: On-Track and Off-Track—A Narrative Review. Osteology 2022, 2, 129-136. https://doi.org/10.3390/osteology2030015
Ventura A, Smiraglio C, Viscomi A, De Salvatore S, Bertucci B. The Glenoid Track Concept: On-Track and Off-Track—A Narrative Review. Osteology. 2022; 2(3):129-136. https://doi.org/10.3390/osteology2030015
Chicago/Turabian StyleVentura, Antonio, Claudia Smiraglio, Antonio Viscomi, Sergio De Salvatore, and Bernardo Bertucci. 2022. "The Glenoid Track Concept: On-Track and Off-Track—A Narrative Review" Osteology 2, no. 3: 129-136. https://doi.org/10.3390/osteology2030015