
Percutaneous Vertebroplasty: A Minimally Invasive Procedure for the Management of Vertebral Compression Fractures
 , and
, and
Abstract
:1. Introduction
2. Literature Search Method
3. Results
3.1. Patient Selection
3.2. Preoperative Imaging
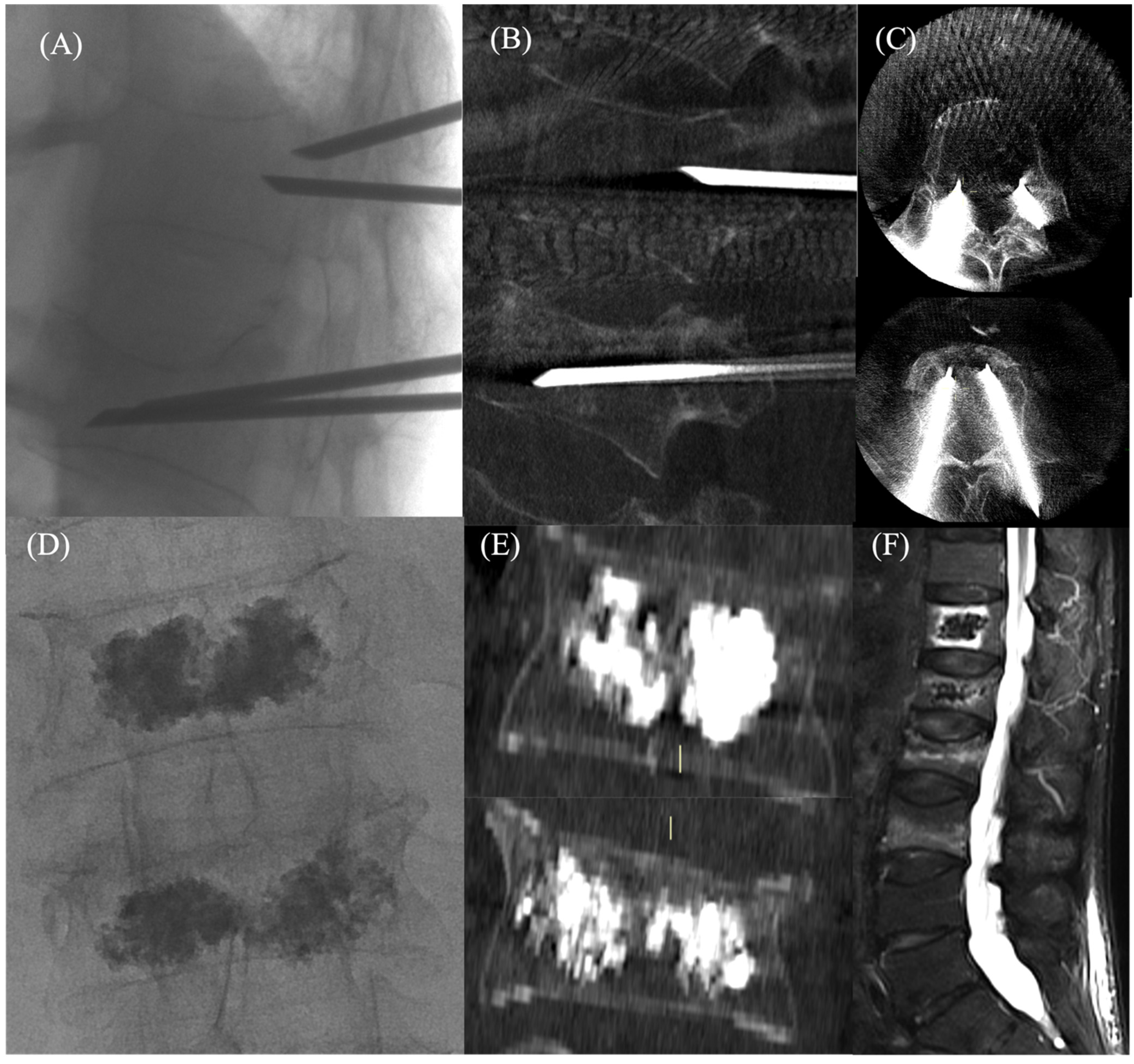
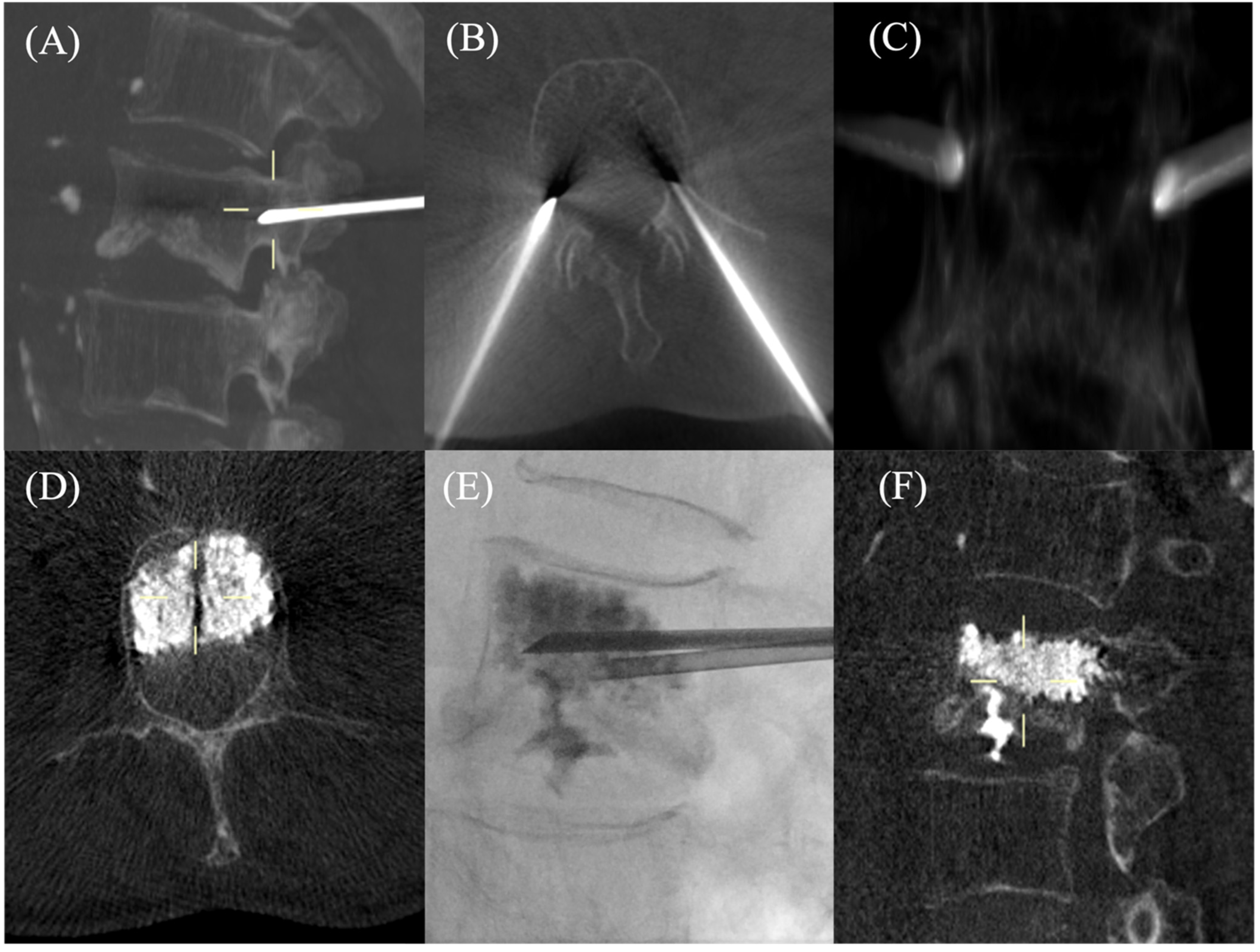
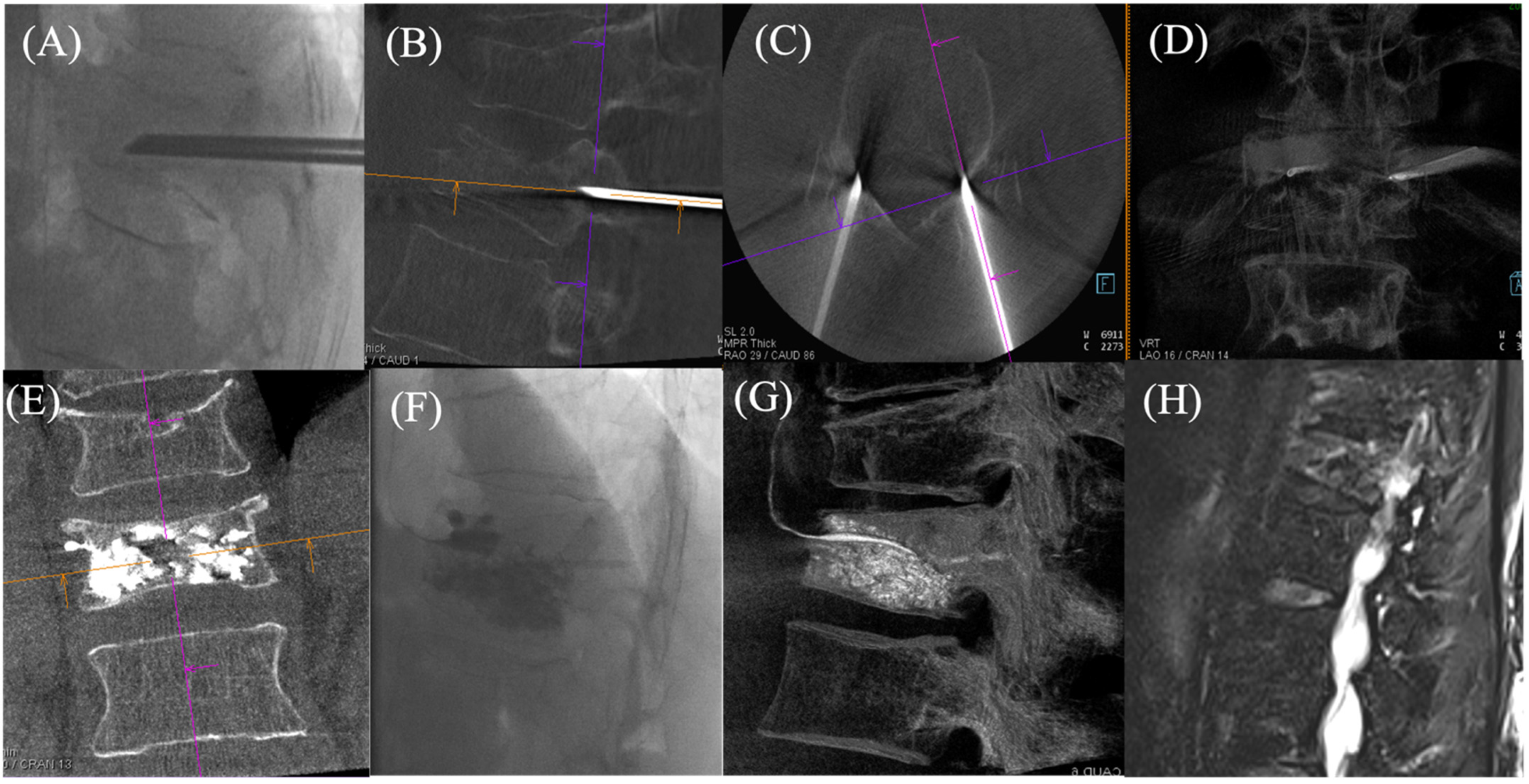
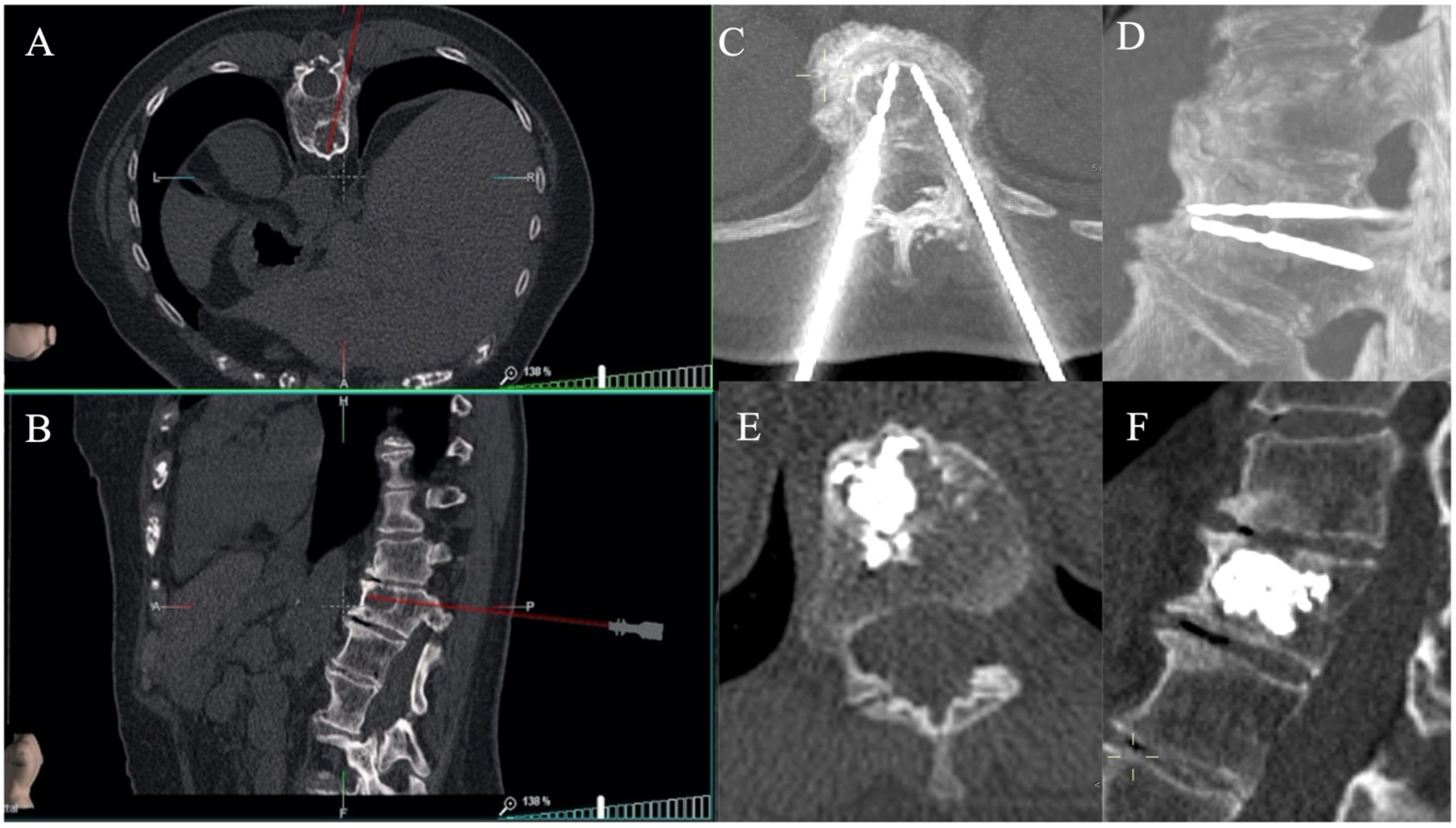
3.3. Procedural Steps
Technique
3.4. Complications
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Conflicts of Interest
References
- Phillips, F. Minimal invasive treatment of osteoporotic vertebral compression fractures. Spine 2003, 28, s45–s53. [Google Scholar] [CrossRef]
- Stallemeyer, M.; Zoarski, G.; Obuchowski, A. Bernadette optimizing patient selection in percutaneous vertebroplasty. Interv. Radiol. 2003, 14, 683–696. [Google Scholar] [CrossRef]
- Wade, S.W.; Strader, C.; Fitzpatrick, L.A.; Anthony, M.S. Sex- and age-specific incidence of non-traumatic fractures in selected industrialized countries. Arch. Osteoporos. 2012, 7, 219–227. [Google Scholar] [CrossRef]
- Johnell, O.; Kanis, J.A. An estimate of the worldwide prevalence and disability associated with osteoporotic fractures. Osteoporos. Int. 2006, 17, 1726–1733. [Google Scholar] [CrossRef] [PubMed]
- Kado, D.M.; Duong, T.; Stone, K.L.; Ensrud, K.E.; Nevitt, M.C.; Greendale, G.A.; Cummings, S.R.; Stone, K.L.; Ensrud, K.E. Incident vertebral fractures and mortality in older women: A prospective study. Osteoporos. Int. 2003, 14, 589–594. [Google Scholar] [CrossRef]
- Lau, E.; Ong, K.; Kurtz, S.; Schmier, J.; Edidin, A. Mortality following the diagnosis of a vertebral compression fracture in the medicare population. J. Bone Joint Surg. Am. 2008, 90, 1479–1486. [Google Scholar] [CrossRef] [Green Version]
- Tsoumakidou, G.; Too, C.W.; Koch, G.; Caudrelier, J.; Cazzato, R.L.; Garnon, J.; Gangi, A. CIRSE Guidelines on Percutaneous Vertebral Augmentation. Cardiovasc. Intervent. Radiol. 2017, 40, 331–342. [Google Scholar] [CrossRef] [PubMed]
- Venmans, A.; Lohle, P.N.M.; van Rooij, W.J. Pain course in conservatively treated patients with back pain and a VCF on the spine radiograph (VERTOS III). Skeletal. Radiol. 2014, 43, 13–18. [Google Scholar] [CrossRef] [PubMed]
- Laredo, J.D.; Chiras, J.; Kemel, S.; Taihi, L.; Hamze, B. Vertebroplasty and interventional radiology procedures for bone metastases. Joint Bone Spine 2018, 85, 191–199. [Google Scholar] [CrossRef] [PubMed]
- Khan, M.; Kushchayev, S.V. Percutaneous Vertebral Body Augmentations: The State of Art. Neuroimaging Clin. N. Am. 2019, 29, 495–513. [Google Scholar] [CrossRef] [PubMed]
- Lieberman, I.H.; Togawa, D.; Kayanja, M.M. Vertebroplasty and kyphoplasty: Filler materials. Spine J. 2005, 5, S305–S316. [Google Scholar] [CrossRef]
- Robinson, Y.; Heyde, C.E.; Fo¨rsth, P.; Olerud, C. Kyphoplasty in osteoporotic vertebral compression fractures—Guidelines and technical considerations. J. Orthop. Surg. Res. 2011, 6, 43. [Google Scholar] [CrossRef] [Green Version]
- Denaro, L.; Longo, U.G.; Denaro, V. Vertebroplasty and kyphoplasty: Reasons for concern? Orthop. Clin. N. Am. 2009, 40, 465–471. [Google Scholar] [CrossRef] [PubMed]
- Galibert, P.; Deramond, H.; Rosat, P.; Le Gars, D. Preliminary note on the treatment of vertebral angioma by percutaneous acrylic vertebroplasty. Neurochirurgie 1987, 33, 166–168. [Google Scholar] [PubMed]
- Buchbinder, R.; Johnston, R.V.; Rischin, K.J.; Homik, J.; Jones, C.A.; Golmohammadi, K.; Kallmes, D.F. Percutaneous vertebroplasty for osteoporotic vertebral compression fracture. Rev. Cochrane Database Syst. Rev. 2018, 4, CD006349. [Google Scholar] [PubMed]
- Kobayashi, K.; Shimoyama, K.; Nakamura, K.; Murata, K. Percutaneous vertebroplasty immediately relieves pain of osteoporotic vertebral compression fractures and prevents prolonged immobilization of patients. Eur. Radiol. 2005, 15, 360–367. [Google Scholar] [CrossRef]
- Masala, S.; Mastrangeli, R.; Petrella, M.C.; Massari, F.; Ursone, A.; Simonetti, G. Percutaneous vertebroplasty in 1,253 levels: Results and long-term effectiveness in a single centre. Eur. Radiol. 2009, 19, 165–171. [Google Scholar] [CrossRef] [PubMed]
- Anselmetti, G.C.; Corrao, G.; Monica, P.D.; Tartaglia, V.; Manca, A.; Eminefendic, H.; Russo, F.; Tosetti, I.; Regge, D. Pain relief following percutaneous vertebroplasty: Results of a series of 283 consecutive patients treated in a single institution. Cardiovasc. Intervent. Radiol. 2007, 30, 441–447. [Google Scholar] [CrossRef]
- Evans, A.J.; Jensen, M.E.; Kip, K.E.; DeNardo, A.J.; Lawler, G.J.; Negin, G.A.; Remley, K.B.; Boutin, S.M.; Dunnagan, S.A. Vertebral compression fractures: Pain reduction and improvement in functional mobility after percutaneous polymethylmethacrylate vertebroplasty retrospective report of 245 cases. Radiology 2003, 226, 366–372. [Google Scholar] [CrossRef] [Green Version]
- Cohen, J.E.; Lylyk, P.; Ceratto, R.; Kaplan, L.; Umansky, F.; Gomori, J.M. Percutaneous vertebroplasty: Technique and results in 192 procedures. Neurol. Res. 2004, 26, 41–49. [Google Scholar] [CrossRef]
- Longo, U.G.; Loppini, M.; Denaro, L.; Maffulli, N.; Denaro, V. Conservative management of patients with an osteoporotic vertebral fracture: A review of the literature. J. Bone Joint Surg. Br. 2012, 94, 152–157. [Google Scholar] [CrossRef] [PubMed]
- Bennell, K.L.; Matthews, B.; Greig, A.; Briggs, A.; Kelly, A.; Sherburn, M.; Larsen, J.; Wark, J. Effects of an exercise and manual therapy program on physical impairments, function and quality-of-life in people with osteoporotic vertebral fracture: A randomised, single-blind controlled pilot trial. BMC Musculoskelet. Disord. 2010, 11, 36. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pfeifer, M.; Begerow, B.; Minne, H.W. Effects of a new spinal orthosis on posture, trunk strength, and quality of life in women with postmenopausal osteoporosis: A randomized trial. Am. J. Phys. Med. Rehabil. 2004, 83, 177–186. [Google Scholar] [CrossRef]
- Longo, U.G.; Denaro, V. Spinal augmentation: What have we learnt? Lancet 2009, 373, 1947. [Google Scholar] [CrossRef]
- Longo, U.G.; Loppini, M.; Denaro, L.; Maffulli, N.; Denaro, V. Osteoporotic vertebral fractures: Current concepts of conservative care. Br. Med. Bull. 2012, 102, 171–189. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Klazen, C.A.; Lohle, P.N.; de Vries, J.; Jansen, F.H.; Tielbeek, A.V.; Blonk, M.C.; Venmans, A.; van Rooij, W.J.J.; Schoemaker, M.C.; Juttmann, J.R.; et al. Vertebroplasty versus conservative treatment in acute osteoporotic vertebral compression fractures (Vertos II): An open-label randomised trial. Lancet 2010, 376, 1085–1092. [Google Scholar] [CrossRef] [Green Version]
- Farrokhi, M.R.; Alibai, E.; Maghami, Z. Randomized controlled trial of percutaneous vertebroplasty versus optimal medical management for the relief of pain and disability in acute osteoporotic vertebral compression fractures. J. Neurosurg. Spine 2011, 14, 561–569. [Google Scholar] [CrossRef] [Green Version]
- Zoarski, G.H.; Snow, P.; Olan, W.J.; Stallmeyer, M.J.B.; Dick, B.W.; Hebel, J.R.; De Deyne, M. Percutaneous vertebroplasty for osteoporotic compression fractures: Quantitative prospective evaluation of long-term outcomes. J. Vasc. Interv. Radiol. 2002, 13, 139–148. [Google Scholar] [CrossRef]
- Mathis, J.M.; Barr, J.D.; Belkoff, S.M.; Barr, M.S.; Jensen, M.E.; Deramond, H. Percutaneous vertebroplasty: A developing standard of care for vertebral compression fractures. AJNR Am. J. Neuroradiol. 2001, 22, 373–381. [Google Scholar]
- Bonnard, E.; Foti, P.; Kastler, A.; Amoretti, N. Percutaneous vertebroplasty under local anaesthesia: Feasibility regarding patients’ experience. Eur. Radiol. 2016, 27, 1512–1516. [Google Scholar] [CrossRef]
- Uppin, A.A.; Hirsch, J.A.; Centenera, L.V.; Pfiefer, B.A.; Pazianos, A.G.; Choi, I.S. Occurrence of new vertebral body fracture after percutaneous vertebroplasty in patients with osteoporosis. Radiology 2003, 226, 119–124. [Google Scholar] [CrossRef] [PubMed]
- White, S.M. Anaesthesia for percutaneous vertebroplasty. Anaesthesia 2002, 57, 1229–1230. [Google Scholar] [PubMed]
- Martin, J.B.; Jean, B.; Sugiu, K.; San Milla´n Ruı´z, D.; Piotin, M.; Murphy, K.; Rüfenacht, B.; Muster, M.; Rüfenacht, D.A. Vertebroplasty: Clinical experience and followup results. Bone 1999, 25, 11S–15S. [Google Scholar] [CrossRef]
- Gangi, A.; Sabharwal, T.; Irani, F.G.; Buy, X.; Morales, J.P.; Adam, A. Standards of Practice Committee of the Society of Interventional Radiology. Quality assurance guidelines for percutaneous vertebroplasty. Cardiovasc. Intervent. Radiol. 2006, 29, 173–178. [Google Scholar] [CrossRef]
- Beall, D.P.; Datir, A.; D’Souza, S.L.; D’Souza, L.S.; Gunda, D.; Morelli, J.; Johnson, M.B.; Nabavizadeh, N. Percutaneous treatment of insufficiency fractures: Principles, technique and review of literature. Skelet. Radiol. 2010, 39, 117–130. [Google Scholar] [CrossRef] [PubMed]
- Jay, B.; Ahn, S.H. Vertebroplasty. Semin. Intervent. Radiol. 2013, 30, 297–306. [Google Scholar]
- Braak, S.J.; Zuurmond, K.; Aerts, H.C.J.; van Leersum, M.; Overtoom, T.T.T.; van Heesewijk, J.P.M.; van Strijen, M.J. Feasibility study of needle placement in percutaneous vertebroplasty: Cone-beam computed tomography guidance versus conventional fluoroscopy. Cardiovasc. Interv. Radiol. 2013, 36, 1120–1126. [Google Scholar] [CrossRef]
- Gangi, A.; Kastler, B.A.; Dietemann, J.L. Percutaneous vertebroplasty guided by a combination of CT and fluoroscopy. AJNR Am. J. Neuroradiol. 1994, 15, 83–86. [Google Scholar] [PubMed]
- RikHargunani, i.; le Corroller, T.; Khashoggi, K.; Liu, D.M.; Marchinkow, L.O.; Mudri, M.J.; Murphy, K.P.; Ouellette, H.A.; Munk, P.L. An overview of vertebroplasty: Current status, controversies, and future directions. Can. Assoc. Radiol. J. 2012, 63, S11–S17. [Google Scholar] [CrossRef] [Green Version]
- Anselmetti, G.C.; Manca, A.; Montemurro, F.; Tutton, S.; Chiara, G.; Battistella, M.; Savojardo, M.; Marcia, S.; Masala, S.; Regge, D. Vertebroplasty using transoral approach in painful malignant involvement of the second cervical vertebra (C2): A single-institution series of 25 patients. Pain Physician 2012, 15, 35–42. [Google Scholar] [CrossRef]
- Murphy, D.T.; Korzan, J.R.; Ouellette, H.A.; Liu, D.M.; Clarkson, P.W.; Munk, P.L. Driven around the bend: Novel use of a curved steerable needle. Cardiovasc. Interv. Radiol. 2013, 36, 531–535. [Google Scholar] [CrossRef]
- AlvBravo, A.E.; Brasuell, J.E.; Favre, A.W.; Koenig, B.M.; Khan, A.A.; Beall, D.P. Treating Vertebral Compression Fractures: Establishing the appropriate diagnosis, preoperative considerations, treatment techniques, postoperative follow-up and general guidelines for the treatment of patients with symptomatic vertebral compression fractures. Tech. Vasc. Interv. Radiol. 2020, 23, 100701. [Google Scholar]
- Clerk-Lamalice, O.; Beall, D.P.; Ong, K.; Lorio, M.P. ISASS Policy 2018-Vertebral Augmentation: Coverage indications, limitations, and/or medical necessity. Int. J. Spine Surg. 2019, 13, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Wang, M.; Zhang, L.; Fu, Z.; Wang, H.; Wu, Y. Selections of Bone Cement Viscosity and Volume in Percutaneous Vertebroplasty: A Retrospective Cohort Study. World Neurosurg. 2021, 150, e218–e227. [Google Scholar]
- McGirt, M.J.; Parker, S.L.; Wolinsky, J.-P.; Witham, T.F.; Bydon, A.; Gokaslan, Z.L. Vertebroplasty and kyphoplasty for the treatment of vertebral compression fractures: An evidenced-based review of the literature. Spine J. 2009, 9, 501–508. [Google Scholar] [CrossRef] [PubMed]
- Saracen, A.; Kotwica, Z. Complications of percutaneous vertebroplasty: An analysis of 1100 procedures performed in 616 patients. Medicine 2016, 95, e3850. [Google Scholar] [CrossRef]
- Chew, C.; Craig, L.; Edwards, R.; Moss, J.; O’Dwyer, P.J. Safety and efficacy of percutaneous vertebroplasty in malignancy: A systematic review. Clin. Radiol. 2011, 66, 63–72. [Google Scholar] [CrossRef]
- Vallejo, R.; Benyamin, R. Vertebral augmentation techniques for the treatment of vertebral compression fractures: A review. Reg. Anesth. Pain Manag. 2010, 14, 133–141. [Google Scholar] [CrossRef]
- Martin, D.J.; Rad, A.E.; Kallmes, D.F. Prevalence of extravertebral cement leakage after vertebroplasty: Procedural documentation versus CT detection. Acta Radiol. 2012, 53, 569–572. [Google Scholar] [CrossRef]
- Krueger, A.; Bliemel, C.; Zettl, R.; Ruchholtz, S. Management of pulmonary cement embolism after percutaneous vertebroplasty and kyphoplasty: A systematic review of the literature. Eur. Spine J. 2009, 18, 1257–1265. [Google Scholar] [CrossRef] [Green Version]
- Scroop, R.; Eskridge, J.; Britz, G.W. Paradoxical cerebral arterial embolization of cement during intraoperative vertebroplasty: Case report. AJNR Am. J. Neuroradiol. 2002, 23, 868–870. [Google Scholar] [PubMed]
- Jensen, M.E.; Evans, A.J.; Mathis, J.M.; Kallmes, D.F.; Cloft, H.J.; Dion, J.E. Percutaneous polymethylmethacrylate vertebroplasty in the treatment of osteoporotic vertebral body compression fractures: Technical aspects. AJNR Am. J. Neuroradiol. 1997, 18, 1897–1904. [Google Scholar] [PubMed]
- Gardos, F.; Depriester, C.; Cayrolle, G. Long term observations of vertebral osteoporotic fractures treated by percutaneous vertebroplasty. Rheumatology 2000, 39, 1410–1414. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nagaraja, S.; Awada, H.K.; Dreher, M.L.; Gupta, S.; Miller, S.W. Vertebroplasty increases compression of adjacent IVDs and vertebrae in osteoporotic spines. Spine J. 2013, 13, 1872–1880. [Google Scholar] [CrossRef]
- Aquarius, R.; van der Zijden, A.M.; Homminga, J.; Verdonschot, N.; Tanck, E. Does bone cement in percutaneous vertebroplasty act as a stress riser? Spine 1976, 2013, 2092–2097. [Google Scholar] [CrossRef]
- Klazen, C.A.H.; Venmans, A.; de Vries, J.; van Rooij, W.J.; Jansen, F.H.; Blonk, M.C.; Lohle, P.; Juttmann, J.; Buskens, E.; Van Everdingen, K.; et al. Percutaneous vertebroplasty is not a risk factor for new osteoporotic compression fractures: Results from VERTOS II. Am. J. Neuroradiol. 2010, 31, 1447–1450. [Google Scholar] [CrossRef] [Green Version]
- Albers, C.E.; Schott, P.M.; Ahmad, S.S.; Benneker, L.M.; Nieuwkamp, N.; Hoppe, S. Vertebral Body Lavage Reduces Hemodynamic Response to Vertebral Body Augmentation With PMMA. Glob. Spine J. 2019, 9, 499–504. [Google Scholar] [CrossRef]
- Berenson, J.; Pflugmacher, R.; Jarzem, P.; Zonder, J.; Schechtman, K.; Tillman, J.B.; Bastian, L.; Ashraf, T.; Vrionis, F. Cancer Patient Fracture Evaluation (CAFE) Investigators. Balloon kyphoplasty versus nonsurgical fracture management for treatment of painful vertebral body compression fractures in patients with cancer: A multicentre, randomised controlled trial. Lancet Oncol. 2011, 12, 225–235. [Google Scholar] [CrossRef]
- Hadjipavlou, A.G.; Tzermiadianos, M.N.; Katonis, P.G.; Szpalski, M. Percutaneous vertebroplasty and balloon kyphoplasty for the treatment of osteoporotic vertebral compression fractures and osteolytic tumours. J. Bone Joint Surg. Br. 2005, 87, 1595–1604. [Google Scholar] [CrossRef] [Green Version]
- Kushchayev, S.V.; Wiener, P.C.; Teytelboym, O.M.; Arrington, J.A.; Khan, M.; Preul, M.C. Percutaneous Vertebroplasty: A history of procedure, technology, culture, specialty, and economics. Rev. Neuroimaging Clin. N. Am. 2019, 29, 481–494. [Google Scholar] [CrossRef]
- Taylor, R.S.; Fritzell, P.; Taylor, R.J. Balloon kyphoplasty in the management of vertebral compression fractures: An updated systematic review and meta-analysis. Eur. Spine J. 2007, 16, 1085–1100. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Key, B.M.; Symanski, J.; Scheidt, M.J.; Tutton, S.M. Vertebroplasty, Kyphoplasty, and Implant-Based Mechanical Vertebral Augmentation. Rev. Semin. Musculoskelet. Radiol. 2021, 25, 785–794. [Google Scholar] [CrossRef] [PubMed]
- Voormolen, M.H.; Mali, W.P.; Lohle, P.N.; Fransen, H.; Lampmann, L.E.H.; Van der Graaf, Y.; Juttmann, J.R.; Jansssens, X.; Verhaar, H.J.J. Percutaneous vertebroplasty compared with optimal pain medication treatment: Short term clinical outcome of patients with subacute or chronic painful osteoporotic vertebral compression fractures. The VERTOS study. AJNR Am. J. Neuroradiol. 2007, 28, 555–560. [Google Scholar] [PubMed]
- Peh, W.C.; Munk, P.L.; Rashid, F.; Gilula, L.A. Percutaneous vertebral augmentation: Vertebroplasty, kyphoplasty and skyphoplasty. Radiol. Clin. North Am. 2008, 46, 611–635. [Google Scholar] [CrossRef]
- Kallmes, D.F.; Comstock, B.A.; Heagerty, P.J.; Turner, J.A.; Wilson, D.J.; Diamond, T.H.; Edwards, R.; Gray, L.A.; Stout, L.; Owen, S.; et al. A randomized trial of vertebroplasty for osteoporotic spinal fractures. N. Engl. J. Med. 2009, 361, 569–579. [Google Scholar] [CrossRef] [Green Version]
- Buchbinder, R.; Osborne, R.H.; Ebeling, P.R.; Wark, J.D.; Mitchell, P.; Wriedt, C.; Graves, S.; Staples, M.P.; Murphy, B. A randomized trial of vertebroplasty for painful osteoporotic vertebral fractures. N. Engl. J. Med. 2009, 361, 557–568. [Google Scholar] [CrossRef] [Green Version]
- Clark, W.; Bird, P.; Gonski, P.; Diamond, T.H.; Smerdely, P.; McNeil, H.P.; Schlaphoff, G.; Bryant, C.; Barnes, E.; Gebski, V. Safety and efficacy of vertebroplasty for acute painful osteoporotic fractures (VAPOUR): A multicentre, randomised, double-blind, placebo-controlled trial. Lancet 2016, 388, 1408–1416. [Google Scholar] [CrossRef]
- Denaro, L.; Longo, U.G.; Papalia, R.; De Salvatore, S.; Ruzzini, L.; Piergentili, I.; Denaro, V. The burden of percutaneous vertebroplasty: An epidemiological nationwide study in Italy from 2009 to 2015. Eur. Spine J. 2021, 30, 3099–3106. [Google Scholar] [CrossRef]
- Hopkins, T.J.; Eggington, S.; Quinn, M.; Nichols-Ricker, C.I. Cost-effectiveness of balloon kyphoplasty and vertebroplasty versus conservative medical management in the USA. Osteoporos Int. 2020, 31, 2461–2471. [Google Scholar] [CrossRef]
- Chew, C.; Ritchie, M.; O’Dwyer, P.J.; Edwards, R. A prospective study of percutaneous vertebroplasty in patients with myeloma and spinal metastases. Clin. Radiol. 2011, 66, 1193–1196. [Google Scholar] [CrossRef]
- Munk, P.L.; Rashid, F.; Heran, M.K.; Papirny, M.; Liu, D.M.; Malfair, D.; Badii, M.; Clarkson, P.W. Combined cementoplasty and radiofrequency ablation in the treatment of painful neoplastic lesions of bone. J. Vasc. Interv. Radiol. 2009, 20, 903–911. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| INDICATIONS | CONTRAINDICATIONS |
| Absolute
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Faiella, E.; Pacella, G.; Altomare, C.; Bernetti, C.; Sarli, M.; Cea, L.; Russo, F.; Vadalà, G.; Beomonte Zobel, B.; Grasso, R.F. Percutaneous Vertebroplasty: A Minimally Invasive Procedure for the Management of Vertebral Compression Fractures. Osteology 2022, 2, 139-151. https://doi.org/10.3390/osteology2040017
Faiella E, Pacella G, Altomare C, Bernetti C, Sarli M, Cea L, Russo F, Vadalà G, Beomonte Zobel B, Grasso RF. Percutaneous Vertebroplasty: A Minimally Invasive Procedure for the Management of Vertebral Compression Fractures. Osteology. 2022; 2(4):139-151. https://doi.org/10.3390/osteology2040017
Chicago/Turabian StyleFaiella, Eliodoro, Giuseppina Pacella, Carlo Altomare, Caterina Bernetti, Marina Sarli, Laura Cea, Fabrizio Russo, Gianluca Vadalà, Bruno Beomonte Zobel, and Rosario Francesco Grasso. 2022. "Percutaneous Vertebroplasty: A Minimally Invasive Procedure for the Management of Vertebral Compression Fractures" Osteology 2, no. 4: 139-151. https://doi.org/10.3390/osteology2040017