
Dysmetabolic Iron Overload Syndrome: Going beyond the Traditional Risk Factors Associated with Metabolic Syndrome

 ,
,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Information Sources
2.2. Study Selection
2.3. Inclusion Criteria
2.4. Exclusion Criteria
3. Results
4. Discussion
4.1. Ferritin and Hyperferritinemia
4.2. Hepcidin
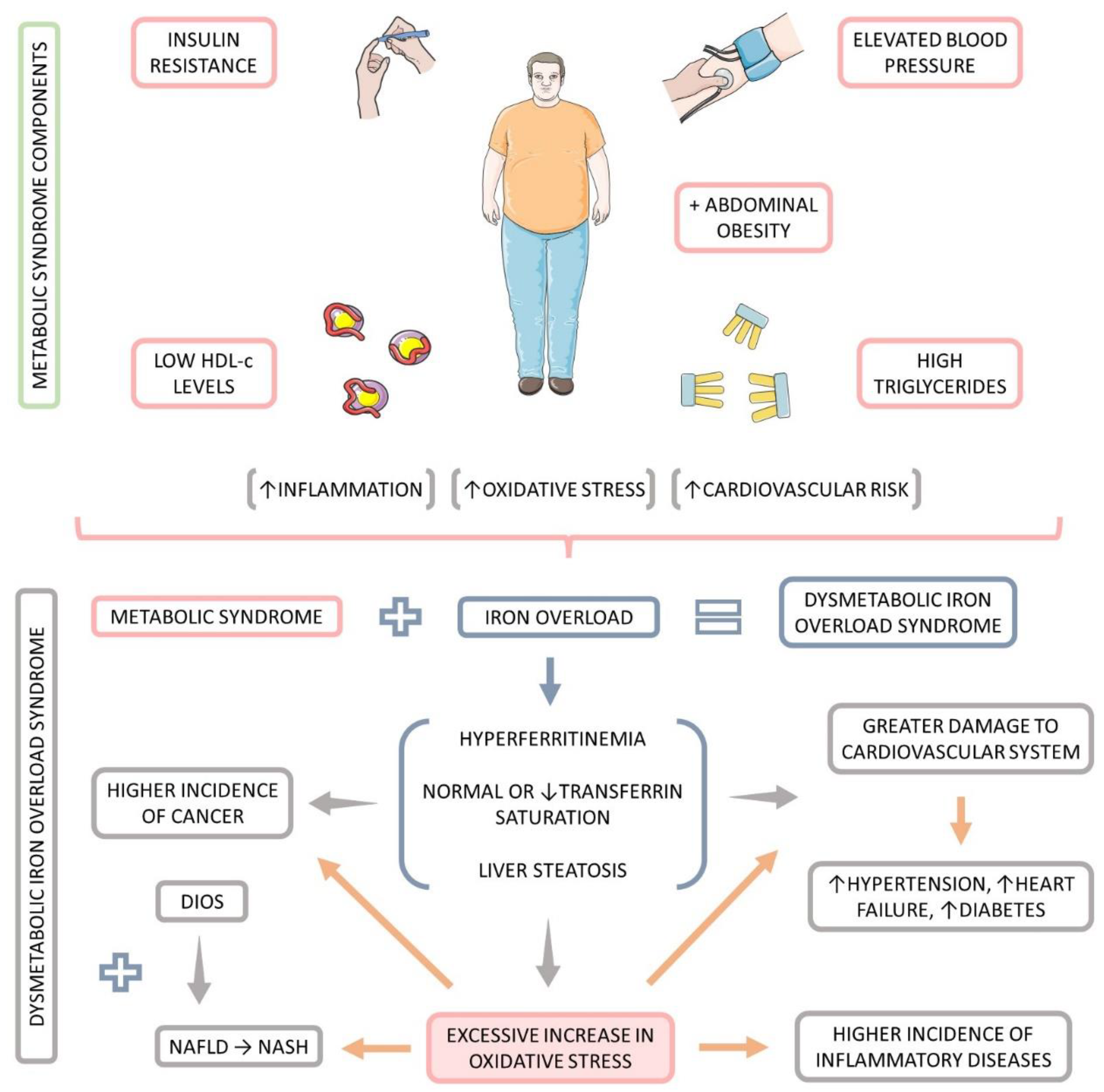
4.3. Metabolic Syndrome
4.4. Oxidative Stress
4.5. Dysmetabolic Iron Overload Syndrome
4.6. Future Directions
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Barbalho, S.M.; Tofano, R.J.; Chagas, E.F.B.; Detregiachi, C.R.P.; Goulart, A.R.; Flato, U.A.P. Benchside to the bedside of frailty and cardiovascular aging: Main shared cellular and molecular mechanisms. Exp. Gerontol. 2021, 148, 111302. [Google Scholar] [CrossRef] [PubMed]
- Liberale, L.; Badimon, L.; Montecucco, F.; Lüscher, T.F.; Libby, P.; Camici, G.G. Inflammation, Aging, and Cardiovascular Disease: JACC Review Topic of the Week. J. Am. Coll. Cardiol. 2022, 79, 837–847. [Google Scholar] [CrossRef] [PubMed]
- Aboonabi, A.; Meyer, R.R.; Singh, I. The association between metabolic syndrome components and the development of atherosclerosis. J. Hum. Hypertens. 2019, 33, 844–855. [Google Scholar] [CrossRef] [PubMed]
- Saedi, S.; Watson, S.E.; Young, J.L.; Tan, Y.; Wintergerst, K.A.; Cai, L. Does maternal low-dose cadmium exposure increase the risk of offspring to develop metabolic syndrome and/or type 2 diabetes? Life Sci. 2023, 9, 121385. [Google Scholar] [CrossRef] [PubMed]
- Silveira Rossi, J.L.; Barbalho, S.M.; Reverete de Araujo, R.; Bechara, M.D.; Sloan, K.P.; Sloan, L.A. Metabolic syndrome and cardiovascular diseases: Going beyond traditional risk factors. Diabetes/Metab. Res. Rev. 2022, 38, e3502. [Google Scholar] [CrossRef]
- Sinatora, R.V.; Chagas, E.F.B.; Mattera, F.O.P.; Mellem, L.J.; Santos, A.; Pereira, L.P.; Aranão, A.L.C.; Guiguer, E.L.; Araújo, A.C.; Haber, J.; et al. Relationship of Inflammatory Markers and Metabolic Syndrome in Postmenopausal Women. Metabolites 2022, 12, 73. [Google Scholar] [CrossRef]
- Dos Santos Vieira, D.A.; Hermes Sales, C.; Galvão Cesar, C.L.; Marchioni, D.M.; Fisberg, R.M. Influence of Haem, Non-Haem, and Total Iron Intake on Metabolic Syndrome and Its Components: A Population-Based Study. Nutrients 2018, 10, 314. [Google Scholar] [CrossRef] [Green Version]
- Li, H.; Lin, L.; Xia, Y.L.; Xie, Y.; Yang, X. Research progress on the role of ferroptosis in cardiovascular disease. Front Cardiovasc Med. 2022, 22, 1077332. [Google Scholar] [CrossRef]
- Lainé, F.; Reymann, J.M.; Morel, F.; Langouët, S.; Perrin, M.; Guillygomarc’h, A.; Brissot, P.; Turmel, V.; Mouchel, C.; Pape, D.; et al. Effects of phlebotomy therapy on cytochrome P450 2e1 activity and oxidative stress markers in dysmetabolic iron overload syndrome: A randomized trial. Aliment. Pharmacol. Ther. 2006, 24, 1207–1213. [Google Scholar] [CrossRef]
- Qiu, R.; Alikhanyan, K.; Volk, N.; Marques, O.; Mertens, C.; Agarvas, A.R.; Singh, S.; Pepperkok, R.; Altamura, S.; Muckenthaler, M.U. Repression of the iron exporter ferroportin may contribute to hepatocyte iron overload in individuals with type 2 diabetes. Mol. Metab. 2022, 66, 101644. [Google Scholar] [CrossRef]
- Sachinidis, A.; Doumas, M.; Imprialos, K.; Stavropoulos, K.; Katsimardou, A.; Athyros, V.G. Dysmetabolic Iron Overload in Metabolic Syndrome. Curr. Pharm. Des. 2020, 26, 1019–1024. [Google Scholar] [CrossRef] [PubMed]
- Castiella, A.; Urreta, I.; Zapata, E.; de Juan, M.; Alústiza, J.M.; Emparanza, J.I. Dysmetabolic iron overload syndrome and its relationship with HFE gene mutations and with liver steatosis. Dig. Liver Dis. 2020, 52, 683–685. [Google Scholar] [CrossRef]
- Fujiwara, S.; Izawa, T.; Mori, M.; Atarashi, M.; Yamate, J.; Kuwamura, M. Dietary iron overload enhances Western diet induced hepatic inflammation and alters lipid metabolism in rats sharing similarity with human DIOS. Sci. Rep. 2022, 12, 21414. [Google Scholar] [CrossRef] [PubMed]
- Méndez-Sánchez, N.; Bugianesi, E.; Gish, R.G.; Lammert, F.; Tilg, H.; Nguyen, M.H.; Sarin, S.K.; Fabrellas, N.; Zelber-Sagi, S.; Fan, J.G.; et al. Global multi-stakeholder endorsement of the MAFLD definition. Lancet Gastroenterol. Hepatol. 2022, 7, 388–390. [Google Scholar] [CrossRef] [PubMed]
- Gattermann, N.; Muckenthaler, M.U.; Kulozik, A.E.; Metzgeroth, G.; Hastka, J. The Evaluation of Iron Deficiency and Iron Overload. Dtsch. Arztebl. Int. 2021, 118, 847–856. [Google Scholar] [CrossRef]
- Moris, W.; Verhaegh, P.; Jonkers, D.; Deursen, C.V.; Koek, G. Hyperferritinemia in Nonalcoholic Fatty Liver Disease: Iron Accumulation or Inflammation? Semin. Liver Dis. 2019, 39, 476–482. [Google Scholar] [CrossRef] [PubMed]
- Crawford, D.H.G.; Ross, D.G.F.; Jaskowski, L.-A.; Burke, L.J.; Britton, L.J.; Musgrave, N.; Briskey, D.; Rishi, G.; Bridle, K.R.; Subramaniam, V.N. Iron depletion attenuates steatosis in a mouse model of non-alcoholic fatty liver disease: Role of iron-dependent pathways. Biochim. Biophys. Acta (BBA)-Mol. Basis Dis. 2021, 1867, 166142. [Google Scholar] [CrossRef] [PubMed]
- Deugnier, Y.; Turlin, B. Iron and hepatocellular carcinoma. J. Gastroenterol. Hepatol. 2001, 16, 491–494. [Google Scholar] [CrossRef]
- Tam, E.; Sung, H.K.; Lam, N.H.; You, S.; Cho, S.; Ahmed, S.M.; Abdul-Sater, A.A.; Sweeney, G. Role of Mitochondrial Iron Overload in Mediating Cell Death in H9c2 Cells. Cells 2022, 28, 118. [Google Scholar] [CrossRef]
- Maliken, B.D.; Nelson, J.E.; Klintworth, H.M.; Beauchamp, M.; Yeh, M.M.; Kowdley, K.V. Hepatic reticuloendothelial system cell iron deposition is associated with increased apoptosis in nonalcoholic fatty liver disease. Hepatology 2013, 57, 1806–1813. [Google Scholar] [CrossRef]
- Nelson, J.E.; Wilson, L.; Brunt, E.M.; Yeh, M.M.; Kleiner, D.E.; Unalp-Arida, A.; Kowdley, K.V. Relationship between the pattern of hepatic iron deposition and histological severity in nonalcoholic fatty liver disease. Hepatology 2011, 53, 448–457. [Google Scholar] [CrossRef] [Green Version]
- Fernandez, M.; Lokan, J.; Leung, C.; Grigg, A. A critical evaluation of the role of iron overload in fatty liver disease. J. Gastroenterol. Hepatol. 2022, 37, 1873–1883. [Google Scholar] [CrossRef] [PubMed]
- Ameka, M.; Hasty, A.H. Paying the Iron Price: Liver Iron Homeostasis and Metabolic Disease. Compr. Physiol. 2022, 12, 3641–3663. [Google Scholar] [CrossRef] [PubMed]
- Wiviott, S.D.; Raz, I.; Bonaca, M.P.; Mosenzon, O.; Kato, E.T.; Cahn, A.; Silverman, M.G.; Zelniker, T.A.; Kuder, J.F.; Murphy, S.A.; et al. Dapagliflozin and Cardiovascular Outcomes in Type 2 Diabetes. N. Engl. J. Med. 2019, 380, 347–357. [Google Scholar] [CrossRef] [PubMed]
- Younossi, Z.; Golabi, P.; Paik, J.; Henry, A.; Van Dongen, C.; Henry, L. The global epidemiology of nonalcoholic fatty liver disease (NAFLD) and non-alcoholic steatohepatitis (NASH): A systematic review. Hepatology. 2023. [Google Scholar] [CrossRef]
- Camaschella, C.; Nai, A.; Silvestri, L. Iron metabolism and iron disorders revisited in the hepcidin era. Haematologica 2020, 105, 260–272. [Google Scholar] [CrossRef] [Green Version]
- Chen, X.; Yu, C.; Kang, R.; Tang, D. Iron Metabolism in Ferroptosis. Front. Cell Dev. Biol. 2020, 8, 590226. [Google Scholar] [CrossRef]
- Xiang, Y.; Fan, X.; Zhao, M.; Guo, Q.; Guo, S. CKIP-1 alleviates oxygen-glucose deprivation/reoxygenation-induced apoptosis and oxidative stress in cultured hippocampal neurons by downregulating Keap1 and activating Nrf2/ARE signaling. Eur. J. Pharmacol. 2019, 848, 140–149. [Google Scholar] [CrossRef]
- Chen, H.; Zhao, W.; Yan, X.; Huang, T.; Yang, A. Overexpression of Hepcidin Alleviates Steatohepatitis and Fibrosis in a Diet-induced Nonalcoholic Steatohepatitis. J. Clin. Transl. Hepatol. 2022, 10, 577–588. [Google Scholar] [CrossRef]
- Kim, C.H.; Leitch, H.A. Iron overload-induced oxidative stress in myelodysplastic syndromes and its cellular sequelae. Crit. Rev. Oncol./Hematol. 2021, 163, 103367. [Google Scholar] [CrossRef]
- Gordan, R.; Fefelova, N.; Gwathmey, J.K.; Xie, L.-H. Iron Overload, Oxidative Stress and Calcium Mishandling in Cardiomyocytes: Role of the Mitochondrial Permeability Transition Pore. Antioxidants 2020, 9, 758. [Google Scholar] [CrossRef] [PubMed]
- Loomba, R.; Sanyal, A.J. The global NAFLD epidemic. Nat. Rev. Gastroenterol. Hepatol. 2013, 10, 686–690. [Google Scholar] [CrossRef] [PubMed]
- Lazo, M.; Hernaez, R.; Eberhardt, M.S.; Bonekamp, S.; Kamel, I.; Guallar, E.; Koteish, A.; Brancati, F.L.; Clark, J.M. Prevalence of nonalcoholic fatty liver disease in the United States: The Third National Health and Nutrition Examination Survey, 1988-1994. Am. J. Epidemiol. 2013, 178, 38–45. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Murali, A.R.; Gupta, A.; Brown, K. Systematic review and meta-analysis to determine the impact of iron depletion in dysmetabolic iron overload syndrome and non-alcoholic fatty liver disease. Hepatol. Res. 2018, 48, E30–E41. [Google Scholar] [CrossRef] [Green Version]
- Satiya, J.; Snyder, H.S.; Singh, S.P.; Satapathy, S.K. Narrative review of current and emerging pharmacological therapies for nonalcoholic steatohepatitis. Transl. Gastroenterol. Hepatol. 2021, 6, 60. [Google Scholar] [CrossRef]
- Huang, D.Q.; El-Serag, H.B.; Loomba, R. Global epidemiology of NAFLD-related HCC: Trends, predictions, risk factors and prevention. Nat. Rev. Gastroenterol. Hepatol. 2021, 18, 223–238. [Google Scholar] [CrossRef]
- Carpi, R.Z.; Barbalho, S.M.; Sloan, K.P.; Laurindo, L.F.; Gonzaga, H.F.; Grippa, P.C.; Zutin, T.L.M.; Girio, R.J.S.; Repetti, C.S.F.; Detregiachi, C.R.P.; et al. The Effects of Probiotics, Prebiotics and Synbiotics in Non-Alcoholic Fat Liver Disease (NAFLD) and Non-Alcoholic Steatohepatitis (NASH): A Systematic Review. Int. J. Mol. Sci. 2022, 23, 8805. [Google Scholar] [CrossRef]
- Chen, H.; Zhan, Y.; Zhang, J.; Cheng, S.; Zhou, Y.; Chen, L.; Zeng, Z. The Global, Regional, and National Burden and Trends of NAFLD in 204 Countries and Territories: An Analysis From Global Burden of Disease 2019. JMIR Public Health Surveill. 2022, 8, e34809. [Google Scholar] [CrossRef]
- Lahaye, C.; Gladine, C.; Pereira, B.; Berger, J.; Chinetti-Gbaguidi, G.; Lainé, F.; Mazur, A.; Ruivard, M. Does iron overload in metabolic syndrome affect macrophage profile? A case control study. J. Trace Elem. Med. Biol. 2021, 67, 126786. [Google Scholar] [CrossRef]
- Vaquero, M.P.; Martínez-Maqueda, D.; Gallego-Narbón, A.; Zapatera, B.; Pérez-Jiménez, J. Relationship between iron status markers and insulin resistance: An exploratory study in subjects with excess body weight. PeerJ 2020, 8, e9528. [Google Scholar] [CrossRef]
- Castiella, A.; Urreta, I.; Zapata, E.; Zubiaurre, L.; Alústiza, J.M.; Otazua, P.; Salvador, E.; Letamendi, G.; Arrizabalaga, B.; Rincón, M.L.; et al. Liver iron concentration in dysmetabolic hyperferritinemia: Results from a prospective cohort of 276 patients. Ann. Hepatol. 2020, 19, 31–35. [Google Scholar] [CrossRef] [PubMed]
- Lobbes, H.; Gladine, C.; Mazur, A.; Pereira, B.; Dualé, C.; Cardot, J.-M.; Ruivard, M. Effect of procyanidin on dietary iron absorption in hereditary hemochromatosis and in dysmetabolic iron overload syndrome: A crossover double-blind randomized controlled trial. Clin. Nutr. 2020, 39, 97–103. [Google Scholar] [CrossRef] [PubMed]
- Rauber, M.R.; Pilger, D.A.; Cecconello, D.K.; Falcetta, F.S.; Marcondes, N.A.; Faulhaber, G.A.M. Hepcidin is a useful biomarker to evaluate hyperferritinemia associated with metabolic syndrome. Acad. Bras. Cienc. 2019, 91, e20180286. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marmur, J.; Beshara, S.; Eggertsen, G.; Onelöv, L.; Albiin, N.; Danielsson, O.; Hultcrantz, R.; Stål, P. Hepcidin levels correlate to liver iron content, but not steatohepatitis, in non-alcoholic fatty liver disease. BMC Gastroenterol. 2018, 18, 78. [Google Scholar] [CrossRef] [PubMed]
- Lainé, F.; Ruivard, M.; Loustaud-Ratti, V.; Bonnet, F.; Calès, P.; Bardou-Jacquet, E.; Sacher-Huvelin, S.; Causse, X.; Beusnel, C.; Renault, A. Metabolic and hepatic effects of bloodletting in dysmetabolic iron overload syndrome: A randomized controlled study in 274 patients. Hepatology 2017, 65, 465–474. [Google Scholar] [CrossRef] [Green Version]
- Stechemesser, L.; Eder, S.K.; Wagner, A.; Patsch, W.; Feldman, A.; Strasser, M.; Auer, S.; Niederseer, D.; Huber-Schönauer, U.; Paulweber, B. Metabolomic profiling identifies potential pathways involved in the interaction of iron homeostasis with glucose metabolism. Mol. Metab. 2017, 6, 38–47. [Google Scholar] [CrossRef]
- Deugnier, Y.; Bardou-Jacquet, É.; Lainé, F. Dysmetabolic iron overload syndrome (DIOS). La Presse Méd. 2017, 46, e306–e311. [Google Scholar] [CrossRef]
- Rametta, R.; Dongiovanni, P.; Pelusi, S.; Francione, P.; Iuculano, F.; Borroni, V.; Fatta, E.; Castagna, A.; Girelli, D.; Fargion, S. Hepcidin resistance in dysmetabolic iron overload. Liver Int. 2016, 36, 1540–1548. [Google Scholar] [CrossRef]
- Jézéquel, C.; Lainé, F.; Laviolle, B.; Kiani, A.; Bardou-Jacquet, E.; Deugnier, Y. Both hepatic and body iron stores are increased in dysmetabolic iron overload syndrome. A case-control study. PLoS ONE 2015, 10, e0128530. [Google Scholar] [CrossRef]
- Dongiovanni, P.; Lanti, C.; Gatti, S.; Rametta, R.; Recalcati, S.; Maggioni, M.; Fracanzani, A.L.; Riso, P.; Cairo, G.; Fargion, S.; et al. High fat diet subverts hepatocellular iron uptake determining dysmetabolic iron overload. PLoS ONE 2015, 10, e0116855. [Google Scholar] [CrossRef]
- Trombini, P.; Paolini, V.; Pelucchi, S.; Mariani, R.; Nemeth, E.; Ganz, T.; Piperno, A. Hepcidin response to acute iron intake and chronic iron loading in dysmetabolic iron overload syndrome. Liver Int. 2011, 31, 994–1000. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ruivard, M.; Lainé, F.; Ganz, T.; Olbina, G.; Westerman, M.; Nemeth, E.; Rambeau, M.; Mazur, A.; Gerbaud, L.; Tournilhac, V. Iron absorption in dysmetabolic iron overload syndrome is decreased and correlates with increased plasma hepcidin. J. Hepatol. 2009, 50, 1219–1225. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.Y.; Chang, S.D.; Sreenivasan, G.M.; Tsang, P.W.; Broady, R.C.; Li, C.H.; Zypchen, L.N. Dysmetabolic hyperferritinemia is associated with normal transferrin saturation, mild hepatic iron overload, and elevated hepcidin. Ann. Hematol. 2011, 90, 139–143. [Google Scholar] [CrossRef]
- Kadoglou, N.P.; Biddulph, J.P.; Rafnsson, S.B.; Trivella, M.; Nihoyannopoulos, P.; Demakakos, P. The association of ferritin with cardiovascular and all-cause mortality in community-dwellers: The English longitudinal study of ageing. PLoS ONE 2017, 12, e0178994. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shander, A.; Goodnough, L.T.; Javidroozi, M.; Auerbach, M.; Carson, J.; Ershler, W.B.; Ghiglione, M.; Glaspy, J.; Lew, I. Iron deficiency anemia—Bridging the knowledge and practice gap. Transfus. Med. Rev. 2014, 28, 156–166. [Google Scholar] [CrossRef]
- Takatoku, M. Japanese National Research Group on Idiopathic Bone Marrow Failure Syndromes. Retrospective nationwide survey of Japanese patients with transfusion-dependent MDS and aplastic anemia highlights the negative impact of iron overload on morbidity/mortality. Eur. J. Haematol. 2007, 78, 487–494. [Google Scholar] [CrossRef] [PubMed]
- Plays, M.; Müller, S.; Rodriguez, R. Chemistry and biology of ferritin. Metallomics 2021, 13, mfab021. [Google Scholar] [CrossRef] [PubMed]
- Lorcerie, B.; Audia, S.; Samson, M.; Millière, A.; Falvo, N.; Leguy-Seguin, V.; Berthier, S.; Bonnotte, B. Diagnosis of hyperferritinemia in routine clinical practice. La Presse Méd. 2017, 46, e329–e338. [Google Scholar] [CrossRef] [PubMed]
- Sandnes, M.; Ulvik, R.J.; Vorland, M.; Reikvam, H. Hyperferritinemia—A Clinical Overview. J. Clin. Med. 2021, 10, 2008. [Google Scholar] [CrossRef] [PubMed]
- Tofano, R.J.; Pescinni-Salzedas, L.M.; Chagas, E.F.B.; Detregiachi, C.R.P.; Guiguer, E.L.; Araujo, A.C.; Bechara, M.D.; Rubira, C.J.; Barbalho, S.M. Association of Metabolic Syndrome and Hyperferritinemia in Patients at Cardiovascular Risk. Diabetes Metab. Syndr. Obes. Targets Ther. 2020, 13, 3239–3248. [Google Scholar] [CrossRef]
- Barreto, B.F.M.; Punaro, G.R.; Elias, M.C.; Parise, E.R. Is homeostasis model assessment for insulin resistance > 2.5 a distinguished criteria for metabolic dysfunction-associated fatty liver disease identification? Arq. Gastroenterol. 2022, 59, 402–407. [Google Scholar] [CrossRef]
- Branisso, P.P.F.; de Oliveira, C.; Filho, H.M.L.; Lima, F.R.; Santos, A.S.; Mancini, M.C.; de Melo, M.E.; Carrilho, F.J.; Rocha, M.S.; Clark, P.; et al. Non-invasive methods for iron overload evaluation in dysmetabolic patients. Ann. Hepatol. 2022, 27, 100707. [Google Scholar] [CrossRef] [PubMed]
- Fan, Y.; Wang, J.; Wei, L.; He, B.; Wang, C.; Wang, B. Iron deficiency activates pro-inflammatory signaling in macrophages and foam cells via the p38 MAPK-NF-κB pathway. Int. J. Cardiol. 2011, 152, 49–55. [Google Scholar] [CrossRef] [PubMed]
- Sung, K.C.; Kang, J.H.; Shin, H.S. Relationship of cardiovascular risk factors and serum ferritin with C-reactive protein. Arch. Med. Res. 2007, 38, 121–125. [Google Scholar] [CrossRef] [PubMed]
- Choi, Y.S.; Jang, H.; Gupta, B.; Jeong, J.H.; Ge, Y.; Yong, C.S.; Kim, J.O.; Bae, J.S.; Song, I.S.; Kim, I.S.; et al. Tie2-mediated vascular remodeling by ferritin-based protein C nanoparticles confers antitumor and anti-metastatic activities. J. Hematol. Oncol. 2020, 13, 123. [Google Scholar] [CrossRef]
- Adamska, A.; Łebkowska, A.; Krentowska, A.; Adamski, M.; Kowalska, I. The Association Between Serum Ferritin Concentration and Visceral Adiposity Estimated by Whole-Body DXA Scan in Women With Polycystic Ovary Syndrome. Front. Endocrinol. 2020, 10, 873. [Google Scholar] [CrossRef] [Green Version]
- Trasolini, R.; Cox, B.; Galts, C.; Yoshida, E.M.; Marquez, V. Elevated serum ferritin in non-alcoholic fatty liver disease is not predictive of fibrosis. Can. Liver J. 2022, 5, 152–159. [Google Scholar] [CrossRef]
- Kanamori, Y.; Murakami, M.; Sugiyama, M.; Hashimoto, O.; Matsui, T.; Funaba, M. Hepcidin and IL-1β. Vitam. Horm. 2019, 110, 143–156. [Google Scholar]
- Kowdley, K.V.; Gochanour, E.M.; Sundaram, V.; Shah, R.A.; Handa, P. Hepcidin Signaling in Health and Disease: Ironing Out the Details. Hepatol. Commun. 2021, 5, 723–735. [Google Scholar] [CrossRef]
- Zhou, W.; Qiu, K. The correlation between lncRNA NEAT1 and serum hepcidin in the peripheral blood of non-alcoholic fatty liver disease patients. Am. J. Transl. Res. 2022, 14, 2593–2599. [Google Scholar]
- Gozzelino, R.; Arosio, P. Iron homeostasis in health and disease. Int. J. Mol. Sci. 2016, 17, 130. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Meynard, D.; Babitt, J.L.; Lin, H.Y. The Journal of the American Society of Hematology. The liver: Conductor of systemic iron balance. Blood J. Am. Soc. Hematol. 2014, 123, 168–176. [Google Scholar]
- Zhu, Y.; He, B.; Xiao, Y.; Chen, Y. Iron metabolism and its association with dyslipidemia risk in children and adolescents: A cross-sectional study. Lipids Health Dis. 2019, 18, 50. [Google Scholar] [CrossRef] [PubMed]
- Datz, C.; Müller, E.; Aigner, E. Iron overload and non-alcoholic fatty liver disease. Minerva Endocrinol. 2016, 42, 173–183. [Google Scholar] [CrossRef]
- Iwasaki, T.; Nakajima, A.; Yoneda, M.; Yamada, Y.; Mukasa, K.; Fujita, K.; Fujisawa, N.; Wada, K.; Terauchi, Y. Serum ferritin is associated with visceral fat area and subcutaneous fat area. Diabetes Care 2005, 28, 2486–2491. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Piperno, A.; Trombini, P.; Gelosa, M.; Mauri, V.; Pecci, V.; Vergani, A.; Salvioni, A.; Mariani, R.; Mancia, G. Increased serum ferritin is common in men with essential hypertension. J. Hypertens. 2002, 20, 1513–1518. [Google Scholar] [CrossRef]
- Kao, T.-W.; Huang, C.-C. Recent Progress in Metabolic Syndrome Research and Therapeutics. Int. J. Mol. Sci. 2021, 22, 6862. [Google Scholar] [CrossRef]
- Lyu, J.; Lin, Q.; Fang, Z.; Xu, Z.; Liu, Z. Complex impacts of gallstone disease on metabolic syndrome and nonalcoholic fatty liver disease. Front. Endocrinol. 2022, 13, 1032557. [Google Scholar] [CrossRef]
- Ellervik, C.; Marott, J.L.; Tybjærg-Hansen, A.; Schnohr, P.; Nordestgaard, B.G. Total and cause-specific mortality by moderately and markedly increased ferritin concentrations: General population study and metaanalysis. Clin. Chem. 2014, 60, 1419–1428. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rametta, R.; Fracanzani, A.L.; Fargion, S.; Dongiovanni, P. Dysmetabolic Hyperferritinemia and Dysmetabolic Iron Overload Syndrome (DIOS): Two Related Conditions or Different Entities? Curr. Pharm. Des. 2020, 26, 1025–1035. [Google Scholar] [CrossRef]
- Li, N.; Liao, Y.; Huang, H.; Fu, S. Co-regulation of hepatic steatosis by ferritinophagy and unsaturated fatty acid supply. Hepatol. Commun. 2022, 6, 2640–2653. [Google Scholar] [CrossRef] [PubMed]
- Mendler, M.-H.; Turlin, B.; Moirand, R.; Jouanolle, A.-M.; Sapey, T.; Guyader, D.; le Gall, J.-Y.; Brissot, P.; David, V.; Deugnier, Y. Insulin resistance–associated hepatic iron overload. Gastroenterology 1999, 117, 1155–1163. [Google Scholar] [CrossRef] [PubMed]
- González-Domínguez, Á.; Visiedo-García, F.M.; Domínguez-Riscart, J.; González-Domínguez, R.; Mateos, R.M.; Lechuga-Sancho, A.M. Iron Metabolism in Obesity and Metabolic Syndrome. Int. J. Mol. Sci. 2020, 21, 5529. [Google Scholar] [CrossRef] [PubMed]
- Martinelli, N.; Traglia, M.; Campostrini, N.; Biino, G.; Corbella, M.; Sala, C.; Busti, F.; Masciullo, C.; Manna, D.; Previtali, S.; et al. Increased serum hepcidin levels in subjects with the metabolic syndrome: A population study. PLoS ONE 2012, 7, e48250. [Google Scholar] [CrossRef]
- Pisoschi, A.M.; Pop, A.; Iordache, F.; Stanca, L.; Predoi, G.; Serban, A.I. Oxidative stress mitigation by antioxidants-An overview on their chemistry and influences on health status. Eur. J. Med. Chem. 2021, 209, 112891. [Google Scholar] [CrossRef] [PubMed]
- Singh, E.; Devasahayam, G. Neurodegeneration by oxidative stress: A review on prospective use of small molecules for neuroprotection. Mol. Biol. Rep. 2020, 47, 3133–3140. [Google Scholar] [CrossRef] [PubMed]
- García-Guede, Á.; Vera, O.; Ibáñez-de-Caceres, I. When Oxidative Stress Meets Epigenetics: Implications in Cancer Development. Antioxidants 2020, 9, 468. [Google Scholar] [CrossRef]
- Ghosh, R.; Alajbegovic, A.; Gomes, A.V. NSAIDs and cardiovascular diseases: Role of reactive oxygen species. Oxidative Med. Cell. Longev. 2015, 2015, 536962. [Google Scholar] [CrossRef] [Green Version]
- Brown, G.C.; Murphy, M.P.; Jastroch, M.; Divakaruni, A.S.; Mookerjee, S.; Treberg, J.R.; Brand, M.D. Mitochondrial proton and electron leaks. Essays Biochem. 2010, 47, 53–67. [Google Scholar] [CrossRef] [Green Version]
- Chen, Q.; Vazquez, E.J.; Moghaddas, S.; Hoppel, C.L.; Lesnefsky, E.J. Production of reactive oxygen species by mitochondria: Central role of complex III. J. Biol. Chem. 2003, 278, 36027–36031. [Google Scholar] [CrossRef] [Green Version]
- Watson, A.J.; Askew, J.N.; Benson, R.S. Poly (adenosine diphosphate ribose) polymerase inhibition prevents necrosis induced by H2O2 but not apoptosis. Gastroenterology 1995, 109, 472–482. [Google Scholar] [CrossRef] [PubMed]
- Hernandez, A.; Sonavane, M.; Smith, K.R.; Seiger, J.; Migaud, M.E.; Gassman, N.R. Dihydroxyacetone suppresses mTOR nutrient signaling and induces mitochondrial stress in liver cells. PLoS ONE 2022, 17, e0278516. [Google Scholar] [CrossRef]
- Maamoun, H.; Benameur, T.; Pintus, G.; Munusamy, S.; Agouni, A. Crosstalk between oxidative stress and endoplasmic reticulum (ER) stress in endothelial dysfunction and aberrant angiogenesis associated with diabetes: A focus on the protective roles of heme oxygenase (HO)-1. Front. Physiol. 2019, 10, 70. [Google Scholar] [CrossRef]
- Shin, G.C.; Lee, H.M.; Kim, N.; Yoo, S.K.; Park, H.S.; Choi, L.S.; Kim, K.P.; Lee, A.R.; Seo, S.U.; Kim, K.H. Paraoxonase-2 contributes to promoting lipid metabolism and mitochondrial function via autophagy activation. Sci. Rep. 2022, 12, 21483. [Google Scholar] [CrossRef]
- Britton, L.J.; Subramaniam, V.N.; Crawford, D.H. Iron and non-alcoholic fatty liver disease. World J. Gastroenterol. 2016, 22, 8112. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hwang, K.A.; Hwang, Y.; Hwang, H.J.; Park, N. Hepatoprotective Effects of Radish (Raphanus sativus L.) on Acetaminophen-Induced Liver Damage via Inhibiting Oxidative Stress and Apoptosis. Nutrients 2022, 14, 5082. [Google Scholar] [CrossRef] [PubMed]
- Ganz, T.; Nemeth, E. Iron homeostasis in host defence and inflammation. Nat. Rev. Immunol. 2015, 15, 500–510. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cabezas, K.G.; Gómez-Fernandez, C.R.; Vazquez-Padron, R. A comprehensive review of oxidative stress as the underlying mechanism in atherosclerosis and the inefficiency of antioxidants to revert this process. Curr. Pharm. Des. 2018, 24, 4705–4710. [Google Scholar] [CrossRef]
- Du, R.; Wu, X.; Peng, K.; Lin, L.; Li, M.; Xu, Y.; Xu, M.; Chen, Y.; Li, D.; Lu, J. Serum apolipoprotein B is associated with increased risk of metabolic syndrome among middle-aged and elderly Chinese: A cross-sectional and prospective cohort study. J. Diabetes 2019, 11, 752–760. [Google Scholar] [CrossRef]
- Barbalho, S.M.; Bueno Ottoboni, A.M.M.; Fiorini, A.M.R.; Guiguer, É.L.; Nicolau, C.C.T.; Goulart, R.d.A.; Flato, U.A.P. Grape juice or wine: Which is the best option? Crit. Rev. Food Sci. Nutr. 2020, 60, 3876–3889. [Google Scholar] [CrossRef]
- Tang, D.; Chen, X.; Kang, R.; Kroemer, G. Ferroptosis: Molecular mechanisms and health implications. Cell Res. 2021, 31, 107–125. [Google Scholar] [CrossRef]
- Zhang, M.W.; Li, X.T.; Zhang, Z.Z.; Liu, Y.; Song, J.W.; Liu, X.M.; Chen, Y.H.; Wang, N.; Guo, Y.; Liang, L.R.; et al. Elabela blunts doxorubicin-induced oxidative stress and ferroptosis in rat aortic adventitial fibroblasts by activating the KLF15/GPX4 signaling. Cell Stress Chaperones 2022, 1–13. [Google Scholar] [CrossRef]
- Bardou-Jacquet, E.; Lainé, F.; Morcet, J.; Perrin, M.; Guyader, D.; Deugnier, Y. Long-term course after initial iron removal of iron excess in patients with dysmetabolic iron overload syndrome. Eur. J. Gastroenterol. Hepatol. 2014, 26, 418–421. [Google Scholar] [CrossRef]
- Dongiovanni, P.; Fracanzani, A.L.; Fargion, S.; Valenti, L. Iron in fatty liver and in the metabolic syndrome: A promising therapeutic target. J. Hepatol. 2011, 55, 920–932. [Google Scholar] [CrossRef]
- Turlin, B.; Mendler, M.H.; Moirand, R.; Guyader, D.; Guillygomarc’h, A.; Deugnier, Y. Histologic features of the liver in insulin resistance–associated iron overload: A study of 139 patients. Am. J. Clin. Pathol. 2001, 116, 263–270. [Google Scholar] [CrossRef] [Green Version]
- Moreno-Navarrete, J.M.; Novelle, M.G.; Catalán, V.; Ortega, F.; Moreno, M.; Gomez-Ambrosi, J.; Xifra, G.; Serrano, M.; Guerra, E.; Ricart, W. Insulin resistance modulates iron-related proteins in adipose tissue. Diabetes Care 2014, 37, 1092–1100. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yamamoto, K.; Kuragano, T.; Kimura, T.; Nanami, M.; Hasuike, Y.; Nakanishi, T. Interplay of adipocyte and hepatocyte: Leptin upregulates hepcidin. Biochem. Biophys. Res. Commun. 2018, 495, 1548–1554. [Google Scholar] [CrossRef]
- Orr, J.S.; Kennedy, A.; Anderson-Baucum, E.K.; Webb, C.D.; Fordahl, S.C.; Erikson, K.M.; Zhang, Y.; Etzerodt, A.; Moestrup, S.K.; Hasty, A.H. Obesity alters adipose tissue macrophage iron content and tissue iron distribution. Diabetes 2014, 63, 421–432. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dongiovanni, P.; Ruscica, M.; Rametta, R.; Recalcati, S.; Steffani, L.; Gatti, S.; Girelli, D.; Cairo, G.; Magni, P.; Fargion, S. Dietary iron overload induces visceral adipose tissue insulin resistance. Am. J. Pathol. 2013, 182, 2254–2263. [Google Scholar] [CrossRef]
- Nazari, M.; Ho, K.W.; Langley, N.; Cha, K.M.; Kodsi, R.; Wang, M.; Laybutt, D.R.; Cheng, K.; Stokes, R.A.; Swarbrick, M.M.; et al. Iron chelation increases beige fat differentiation and metabolic activity, preventing and treating obesity. Sci. Rep. 2022, 12, 776. [Google Scholar] [CrossRef] [PubMed]
- Khan, M.J.; Gerasimidis, K.; Edwards, C.A.; Shaikh, M.G. Role of gut microbiota in the aetiology of obesity: Proposed mechanisms and review of the literature. J. Obes. 2016, 2016, 7353642. [Google Scholar] [CrossRef] [Green Version]
- Zhang, J.; Cao, J.; Xu, H.; Dong, G.; Huang, K.; Wu, W.; Ye, J.; Fu, J. Ferritin as a key risk factor for nonalcoholic fatty liver disease in children with obesity. J. Clin. Lab. Anal. 2020, 35, e23602. [Google Scholar] [CrossRef] [PubMed]
- Zhao, L.; Zhang, X.; Shen, Y.; Fang, X.; Wang, Y.; Wang, F. Obesity and iron deficiency: A quantitative meta-analysis. Obes. Rev. 2015, 16, 1081–1093. [Google Scholar] [CrossRef] [PubMed]
- Chen, P.K.; Yeo, K.J.; Huang, P.H.; Chang, S.H.; Chang, C.K.; Lan, J.L.; Chen, D.Y. Increased Lipid Peroxidation May Be Linked to Ferritin Levels Elevation in Adult-Onset Still’s Disease. Biomedicines 2021, 9, 1508. [Google Scholar] [CrossRef]
- Ruivard, M.; Laine, F.; Deugnier, Y. Iron absorption in nonalcoholic steatohepatitis and dysmetabolic iron overload syndrome. Hepatology 2016, 63, 1737–1738. [Google Scholar] [CrossRef] [Green Version]
- Deugnier, Y.; Turlin, B. Pathology of hepatic iron overload. Semin. Liver Dis. 2011, 31, 260–271. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Riva, A.; Trombini, P.; Mariani, R.; Salvioni, A.; Coletti, S.; Bonfadini, S.; Paolini, V.; Pozzi, M.; Facchetti, R.; Bovo, G.; et al. Revaluation of clinical and histological criteria for diagnosis of dysmetabolic iron overload syndrome. World J. Gastroenterol. 2008, 14, 4745–4752. [Google Scholar] [CrossRef]
- Deugnier, Y.; Turlin, B. Pathology of hepatic iron overload. World J. Gastroenterol. 2007, 13, 4755–4760. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Reference | Study Design | Sample | Evaluations | Results |
|---|---|---|---|---|
| [39] | Case-control study. | 60 participants (20 with MtS without iron overload, 20 with DIOS, and 20 healthy controls). | Monocytes of the included participants were phenotyped and differenced in inflammatory (M2) through the presence of response for IL-4. 38 genes related to inflammation were also assessed, additionally to genes related to iron metabolism. | No differences between the monocytes phenotypes were assessed. Inflammatory genes related to IL-4 M2 response were activated in DIOS monocytes and in MtS, which correlates with impaired M2 polarization. Iron metabolism genes were higher expressed in DIOS monocytes than in MtS. |
| [40] | Cross-sectional analytical study. | 50 overweight participants and with at least one more MtS risk factor. | Anthropometric parameters, body composition, lipids, Glycemia, BP, insulin, leptin, CRP, ferritin, transferrin, transferrin saturation, and soluble transferrin receptor were evaluated. | Iron transport and iron storage were altered in individuals affected by overweight/obesity that at the same showed IR. |
| [41] | Prospective study. | 276 participants with hyperferritinemia (135 with MS, and 141 without MtS). | In all participants, magnetic resonance images were made to determine liver iron concentration. | No significant differences were found for liver iron concentrations of both MtS and non-MtS groups. Therefore, participants with hyperferritinemia and MtS presented increased liver iron concentrations. |
| [42] | Experimental double-blind, randomized controlled trial. | 40 patients (20 with HH and 20 with DIOS). | Basal levels of serum iron were evaluated (overnight fast). Patients consumed a standardized test iron-rich meal with 43 mg of iron and placebo capsules or Proanthocyanidin supplement every three days. | The iron-rich meal showed a significant increase of serum iron compared with baseline at 120, 180, and 240 min in DIOS (8–9.1%) and HH (15.8–25.7%). The use of procyanidin did not significantly interfere in iron absorption in DIOS or HH. |
| [43] | Cross-sectional study. | 94 participants diagnosed with MtS. | All participants had weight, waist circumference, and height measures, additionally to dosages of ferritin, iron, transferrin saturation, hepcidin, lipids, and glycemia. | Hyperferritinemia prevalence was 27.7% among the participants and was associated with transferrin saturation and serum hepcidin. Hepcidin is helpful to assess ferritin increases. |
| [44] | Observational Case -Control study. | 84 patients with liver disease, 26♀, 58♂/62 with elevated ferritin levels and 22 with normal levels (54 with iron overload, 38 with NAFLD, 29 with chronic liver disease (no NAFLD), and 17 had untreated HH. | Serum hepcidin was measured in all patients. HAMP mRNA was determined in liver tissue with PCR in 36 patients. | Serum hepcidin was higher in NAFLD with DIOS and other chronic liver diseases with iron overload (but not with genetic hemochromatosis). HAMP mRNA (liver tissue) and serum hepcidin were correlated to the liver iron content in NAFLD patients but not to BMI, NAFLD activity score, and serum lipids. There was a correlation between HAMP mRNA in liver tissue and serum hepcidin. |
| [45] | Experimental Multicenter Randomized, controlled trial. | 274 patients (adult subjects with nondiabetic DIOS and with hepatic iron >50 μmol/g). | 146 patients received Phlebotomy lifestyle(LFDA) and diet advice and 128 with LFDA only. 1st phase consisted of bi-monthly phlebotomies (to reach serum ferritin <50 μg/L with hemoglobin levels >11 g/dL). 2nd phase: maintenance phase with bi-monthly phlebotomy by serum levels of ferritin. | Comparison of iron-depleted patients and the control group showed a significant reduction of ferritin levels after blood-letting as well as a significant reduction of body weight and HOMA. In patients with DIOS, iron depletion by bloodletting is not related to the improvement of metabolic and hepatic features. |
| [46] | Observational Cross-sectional study. | 163 patients divided in lean and healthy controls (n = 53); MtS without hyperferritinemia (n = 54) and MtS with hyperferritinemia (n = 56); group with 29 patients with biopsy showing iron overload before and after iron removal. | Patients were submitted to phlebotomies bi-weekly until ferritin concentrations were between 50 and 100 mg/L. Clinical and metabolic parameters before and after iron removal therapy were performed. | Patients with MtS and elevated ferritin showed significantly higher glycemia, HbA1c, and oral glucose tolerance tests compared with MtS without iron overload. Results suggested that high serum ferritin is linked to impaired glucose homeostasis in patients with MtS. |
| [47] | Observational Cohort Study. | 58 DIOS patients underwent venesection for a median follow-up of 5.75 years. | Patients received dietetic counseling. Venesection was performed fortnightly until reaching body iron stores of less than 100 ng/L. | After initial removal of this element, iron loading does not support systematic maintenance therapy but requires periodical follow-up of patients with iron overload recurrence. |
| [48] | Quasi-experimental. | 18 individuals with DIOS, 18 with NAFLD, 23 healthy controls, and 10 with hereditary HH. | Patients were compared after a 24-h oral iron tolerance test (hepcidin evaluations and iron metabolism modeling). | DIOS patients presented higher transferrin saturation (and higher hepcidin levels) than patients with normal iron status and lower values than HH patients. Hepcidin resistance index was correlated with ferritin. |
| [49] | Observational Case-control Study. | 24 individuals: 12 with DIOS and 12 overweight controls and normal serum ferritin levels. | All patients were submitted to venesection program (phlebotomies of 7 mL/kg/14 days until serum ferritin dropped < 50 μg/L). | All patients were comparable regarding the metabolic abnormalities but differed according to serum ferritin levels. The amount of mobilized iron was higher, and serum transferrin was lower in DIOS patients. The authors concluded that total iron stores of the body are highly increased in DIOS. |
| [50] | Pre-clinical study (animal). | 46 patients with NAFLD (23 with uncomplicated steatosis and 23 with NASH; ten individuals with suspicious NAFLD (without histological abnormalities) were considered as controls. | Patients were subjected to percutaneous liver biopsy. | The levels of hepatic TfR-1 mRNA were upregulated in subjects with fatty liver and DIOS. Augmented exposition to fatty acids interferes with hepatic iron metabolism, stimulating iron uptake despite iron accumulation in hepatocytes. |
| [51] | Observational Case -Control study. | 24 adult Italian patients (21 men and three women) with DIOS. | Evaluation of glycemia, insulin, hemoglobin, C-reactive protein, TS, SF, cholesterol, HDL-c, triglycerides, AST, ALT, and γ-glutamyl-transferase, BMI, abdominal waist and iron depletion. | In the beginning, hepcidin levels were significantly higher than in controls. After iron depletion, hepcidin decreased to normal values. In iron-depleted subjects, urinary hepcidin increased after the oral iron test suggesting that in DIOS patients, the progression of iron accumulation is related to the increase in hepcidin release and progressive reduction of iron absorption. |
| [52] | Observational Case-control study. | Six men with DIOS (53 ± 11 years) and age-matched controls with normal iron stores (lean and overweight subjects). | Administration of a single dose of a stable iron isotope. Ferritin and hepcidin were evaluated. | Intestinal absorption of iron was lower in DIOS compared to controls. Intestinal absorption of iron was inversely correlated with plasma hepcidin and CRP. Overweight subjects with normal stores of iron show decreased absorption through hepcidin upregulation, and in DIOS subjects, this reduction is more important due to an extra effect of iron excess on circulating hepcidin levels. |
| [53] | Observational Case-control study. | 10 cases with dysmetabolic Hyperferritinemia. | Comparison of serum iron levels and urine hepcidin levels to healthy controls. Other evaluations were: glycemia, creatinine, AST, ALT, lipids, CRP, SF, and TS. | Patients showed higher serum ferritin than controls, but the median transferrin saturation was not different. Urinary hepcidin was augmented in dysmetabolic hyperferritinemia. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Barbalho, S.M.; Laurindo, L.F.; Tofano, R.J.; Flato, U.A.P.; Mendes, C.G.; de Alvares Goulart, R.; Briguezi, A.M.G.M.; Bechara, M.D. Dysmetabolic Iron Overload Syndrome: Going beyond the Traditional Risk Factors Associated with Metabolic Syndrome. Endocrines 2023, 4, 18-37. https://doi.org/10.3390/endocrines4010002
Barbalho SM, Laurindo LF, Tofano RJ, Flato UAP, Mendes CG, de Alvares Goulart R, Briguezi AMGM, Bechara MD. Dysmetabolic Iron Overload Syndrome: Going beyond the Traditional Risk Factors Associated with Metabolic Syndrome. Endocrines. 2023; 4(1):18-37. https://doi.org/10.3390/endocrines4010002
Chicago/Turabian StyleBarbalho, Sandra Maria, Lucas Fornari Laurindo, Ricardo José Tofano, Uri Adrian Prync Flato, Claudemir G. Mendes, Ricardo de Alvares Goulart, Ana Maria Gonçalves Milla Briguezi, and Marcelo Dib Bechara. 2023. "Dysmetabolic Iron Overload Syndrome: Going beyond the Traditional Risk Factors Associated with Metabolic Syndrome" Endocrines 4, no. 1: 18-37. https://doi.org/10.3390/endocrines4010002