
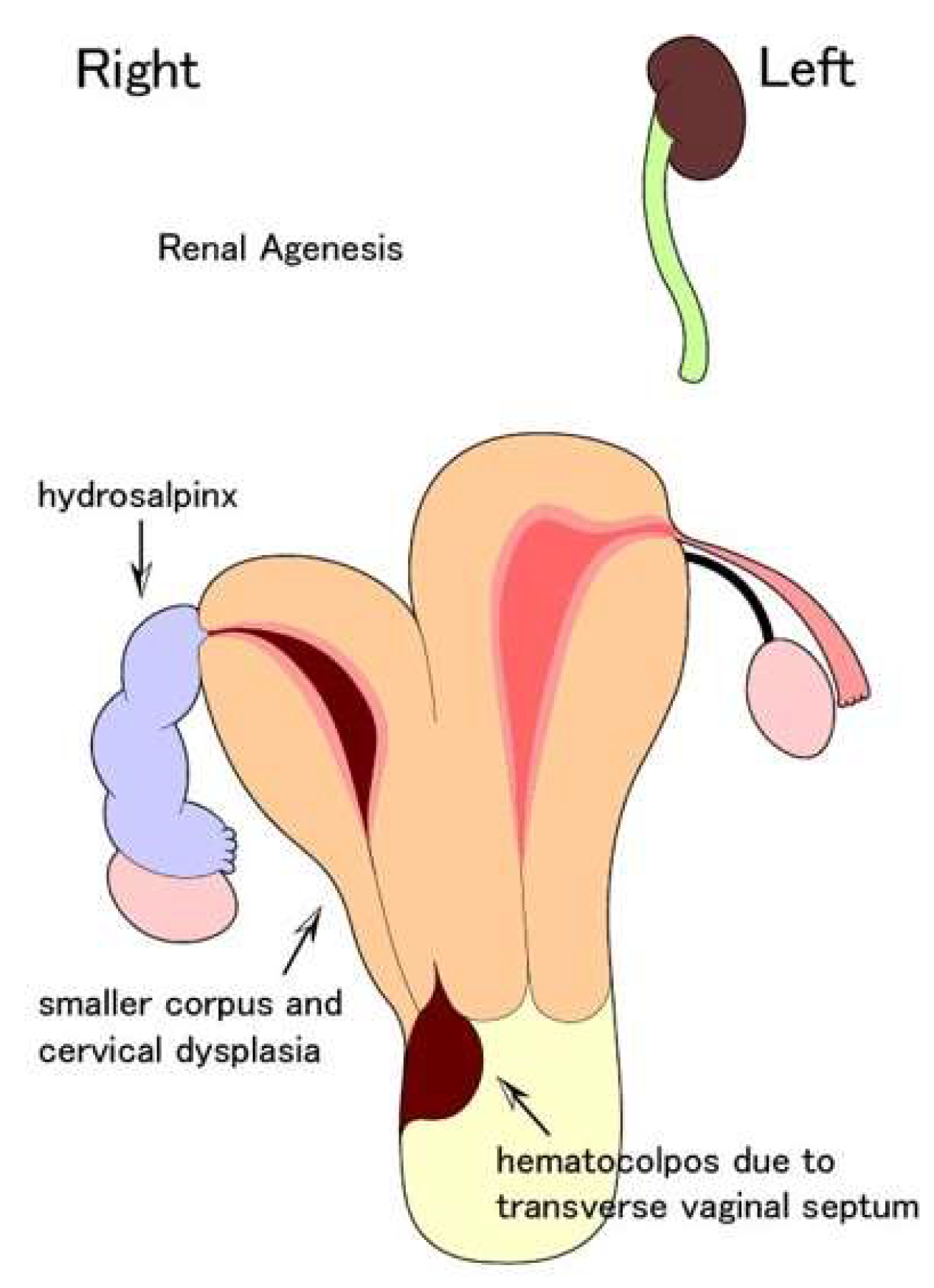
Effects of Hydrosalpinx on Endometrial Receptivity and Uterine Microbiome: An Interesting Case of Double Uterus with Unilateral Hydrosalpinx
 , and
, and
Abstract
:1. Introduction
2. Case Presentation
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Díaz-Gimeno, P.; Horcajadas, J.A.; Martinez-Conejero, J.A.; Esteban, F.J.; Alama, P.; Pellicer, A.; Simon, C. A genomic diagnostic tool for human endometrial receptivity based on the transcriptomic signature. Fertil. Steril. 2011, 95, 50–60. [Google Scholar] [CrossRef] [PubMed]
- Díaz-Gimeno, P.; Ruiz-Alonso, M.; Blesa, D.; Bosch, N.; Martínez-Conejero, J.A.; Alamá, P.; Garrido, N.; Pellicer, A.; Simón, C. The accuracy and reproducibility of the endometrial receptivity array is superior to histology as a diagnostic method for endometrial receptivity. Fertil. Steril. 2013, 99, 508–517. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.; Song, X.; Wei, W.; Zhong, H.; Dai, J.; Lan, Z.; Li, F.; Yu, X.; Feng, Q.; Wang, Z.; et al. The microbiota continuum along the female reproductive tract and its relation to uterine-related diseases. Nat. Commun. 2017, 8, 875. [Google Scholar] [CrossRef] [Green Version]
- Franasiak, J.M.; Scott, R.T., Jr. Reproductive tract microbiome in assisted reproductive technologies. Fertil. Steril. 2015, 104, 1364–1371. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koedooder, R.; Singer, M.; Schoenmakers, S.; Savelkoul, P.H.M.; Morré, S.A.; De Jonge, J.D.; Poort, L.; Cuypers, W.J.S.S.; Beckers, N.G.M.; Broekmans, F.J.M.; et al. The vaginal microbiome as a predictor for outcome of in vitro fertilization with or without intracytoplasmic sperm injection: A prospective study. Hum. Reprod. 2019, 34, 1042–1054. [Google Scholar] [CrossRef] [PubMed]
- Carranza, F.; González-Ravina, A.; Blasco, V.; Fernández-Sánchez, M. Different endometrial receptivity in each hemiuterus of a woman with uterus didelphys and previous failed embryo transfers. J. Hum. Reprod. Sci. 2018, 11, 297–299. [Google Scholar] [CrossRef]
- Grimbizis, G.F.; Gordts, S.; Sardo, A.D.S.; Brucker, S.; De Angelis, C.; Gergolet, M.; Li, T.-C.; Tanos, V.; Brölmann, H.; Gianaroli, L.; et al. The ESHRE/ESGE consensus on the classification of female genital tract congenital anomalies. Hum. Reprod. 2013, 28, 2032–2044. [Google Scholar] [CrossRef] [Green Version]
- McQueen, D.B.; Perfetto, C.O.; Hazard, F.K.; Lathi, R.B. Pregnancy outcomes in women with chronic endometritis and recurrent pregnancy loss. Fertil. Steril. 2015, 104, 927–931. [Google Scholar] [CrossRef] [Green Version]
- Gardner, D.K.; Lane, M.; Stevens, J.; Schlenker, T.; Schoolcraft, W.B. Blastocyst score affects implantation and pregnancy outcome: Towards a single blastocyst transfer. Fertil. Steril. 2000, 73, 1155–1158. [Google Scholar] [CrossRef]
- Tong, J.; Zhu, L.; Chen, N.; Lang, J. Endometriosis in association with Herlyn-Werner-Wunderlich syndrome. Fertil. Steril. 2014, 102, 790–794. [Google Scholar] [CrossRef]
- American Society for Reproductive Medicine. The Practice Committee. Role of tubal surgery in the era of assisted reproductive technology: A committee opinion. Fertil. Steril. 2021, 115, 1143–1150. [Google Scholar] [CrossRef] [PubMed]
- Strandell, A.; Lindhard, A.; Waldenström, U.; Thorburn, J.; Janson, P.O.; Hamberger, L. Hydrosalpinx and IVF outcome: A prospective, randomized multicentre trial in Scandinavia on salpingectomy prior to IVF *. Hum. Reprod. 1999, 14, 2762–2769. [Google Scholar] [CrossRef] [PubMed]
- de Wit, W.; Gowrising, C.J.; Kuik, D.J.; Lens, J.W.; Schats, R. Only hydrosalpinges visible on ultrasound are associated with reduced implantation and pregnancy rates after in-vitro fertilization. Hum. Reprod. 1998, 13, 1696–1701. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kassabji, M.; Sims, J.A.; Butler, L.; Muasher, S.J. Reduced pregnancy outcome in patients with unilateral or bilateral hy-drosalpinx after in vitro fertilization. Eur. J. Obstet. Gynecol. Reprod. Biol. 1994, 56, 129–132. [Google Scholar] [CrossRef] [PubMed]
- Shelton, K.E.; Butler, L.; Toner, J.P.; Oehninger, S.; Muasher, S.J. Salpingectomy improves the pregnancy rate in in-vitro fertilization patients with hydrosalpinx. Hum. Reprod. 1996, 11, 523–525. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- American Society for Reproductive Medicine. Practice Committee of the American Society for Reproductive Medicine in collaboration with The Society of Reproductive Surgeons. Salpingectomy for hydrosalpinx prior to in vitro fertilization. Fertil. Steril. 2008, 90, S66–S68. [Google Scholar] [CrossRef]
- Meyer, W.R.; Castelbaum, A.J.; Somkuti, S.; Sagoskin, A.W.; Doyle, M.; Harris, J.E.; Lessey, B.A. Hydrosalpinges adversely affect markers of endometrial receptivity. Hum. Reprod. 1997, 12, 1393–1398. [Google Scholar] [CrossRef] [Green Version]
- Daftary, G.S.; Kayisli, U.; Seli, E.; Bukulmez, O.; Arici, A.; Taylor, H.S. Salpingectomy increases peri-implantation endometrial HOXA10 expression in women with hydrosalpinx. Fertil. Steril. 2007, 87, 367–372. [Google Scholar] [CrossRef]
- Copperman, A.B.; Wells, V.; Luna, M.; Kalir, T.; Sandler, B.; Mukherjee, T. Presence of hydrosalpinx correlated to endometrial inflammatory response in vivo. Fertil. Steril. 2006, 86, 972–976. [Google Scholar] [CrossRef]
- Strandell, A.; Sjögren, A.; Bentin-Ley, U.; Thorburn, J.; Hamberger, L.; Brännström, M. Hydrosalpinx fluid does not adversely affect the normal development of human embryos and implantation in vitro. Hum. Reprod. 1998, 13, 2921–2925. [Google Scholar] [CrossRef]
- Moreno, I.; Codoñer, F.M.; Vilella, F.; Valbuena, D.; Martinez-Blanch, J.F.; Jimenez-Almazán, J.; Alonso, R.; Alamá, P.; Remohí, J.; Pellicer, A.; et al. Evidence that the endometrial microbiota has an effect on implantation success or failure. Am. J. Obstet. Gynecol. 2016, 215, 684–703. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Strandell, A.; Lindhard, A.; Fernandez-Sanchez, M. Why does hydrosalpinx reduce fertility? The importance of hydrosalpinx fluid. Hum. Reprod. 2002, 17, 1141–1145. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hurni, Y.; Bonollo, M.; Ferrero, L.; Taraschi, G.; Canonica, C.; Lozano, S.V.R. Pyosalpinx complicating chronic hydrosalpinx in a 50-year old virgo woman: A case report. BMC Women’s Health 2018, 18, 90. [Google Scholar] [CrossRef]
- Laufer, N.; Simon, A.; Schenker, J.G.; Sekeles, E.; Cohen, R. Fallopian Tubal Mucosal Damage Induced Experimentally by Escherichia coli in the Rabbit: A Scanning Electron Microscopic Study. Pathol.-Res. Pract. 1984, 178, 605–610. [Google Scholar] [CrossRef] [PubMed]
- Cicinelli, E.; Matteo, M.; Tinelli, R.; Pinto, V.; Marinaccio, M.; Indraccolo, U.; De Ziegler, D.; Resta, L. Chronic Endometritis due to Common Bacteria Is Prevalent in Women with Recurrent Miscarriage as Confirmed by Improved Pregnancy Outcome after Antibiotic Treatment. Reprod. Sci. 2014, 21, 640–647. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Benner, M.; Ferwerda, G.; Joosten, I.; Van Der Molen, R.G. How uterine microbiota might be responsible for a receptive, fertile endometrium. Hum. Reprod. Updat. 2018, 24, 393–415. [Google Scholar] [CrossRef] [Green Version]
- Cicinelli, E.; Matteo, M.; Tinelli, R.; Lepera, A.; Alfonso, R.; Indraccolo, U.; Marrocchella, S.; Greco, P.; Resta, L. Prevalence of chronic endometritis in repeated unexplained implantation failure and the IVF success rate after antibiotic therapy. Hum. Reprod. 2015, 30, 323–330. [Google Scholar] [CrossRef] [Green Version]
- Kitaya, K.; Takeuchi, T.; Mizuta, S.; Matsubayashi, H.; Ishikawa, T. Endometritis: New time, new concepts. Fertil. Steril. 2018, 110, 344–350. [Google Scholar] [CrossRef]
- Moreno, I.; Garcia-Grau, I.; Perez-Villaroya, D.; Gonzalez-Monfort, M.; Bahçeci, M.; Barrionuevo, M.J.; Taguchi, S.; Puente, E.; Dimattina, M.; Lim, M.W.; et al. Endometrial microbiota composition is associated with reproductive outcome in infertile patients. Microbiome 2022, 10, 1. [Google Scholar] [CrossRef]
- Kuroda, K.; Horikawa, T.; Moriyama, A.; Nakao, K.; Juen, H.; Takamizawa, S.; Ojiro, Y.; Nakagawa, K.; Sugiyama, R. Impact of chronic endometritis on endometrial receptivity analysis results and pregnancy outcomes. Immun. Inflamm. Dis. 2020, 8, 650–658. [Google Scholar] [CrossRef]
- Puttemans, P.J.; Brosens, I.A. Preventive salpingectomy of hydrosalpinx prior to IVF: Salpingectomy improves in-vitro fertilization outcome in patients with a hydrosalpinx: Blind victimization of the Fallopian tube? Hum. Reprod. 1996, 11, 2079–2081. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Soper, D.E.; Brockwell, N.J.; Dalton, H.P.; Johnson, D. Observations concerning the microbial etiology of acute salpingitis. Am. J. Obstet. Gynecol. 1994, 170, 1008–1017. [Google Scholar] [CrossRef]
- Sweet, R.L.; Draper, D.L.; Hadley, W.K. Etiology of acute salpingitis: Influence of episode number and duration of symptoms. Obstet. Gynecol. 1981, 58, 62–68. [Google Scholar] [PubMed]
- Cohen, C.R.; Sinei, S.; Reilly, M.; Bukusi, E.; Eschenbach, D.; Holmes, K.K.; Ndinya-Achola, J.O.; Bwayo, J.; Grieco, V.; Stamm, W.; et al. Effect of Human Immunodeficiency Virus Type 1 Infection upon Acute Salpingitis: A Laparoscopic Study. J. Infect. Dis. 1998, 178, 1352–1358. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hebb, J.K.; Cohen, C.R.; Astete, S.G.; Bukusi, E.A.; Totten, P.A. Detection of Novel Organisms Associated with Salpingitis, by Use of 16S rDNA Polymerase Chain Reaction. J. Infect. Dis. 2004, 190, 2109–2120. [Google Scholar] [CrossRef]
- Hillier, S.L.; Kiviat, N.B.; Hawes, S.E.; Hasselquist, M.B.; Hanssen, P.W.; Eschenbach, D.A.; Holmes, K.K. Role of bacterial vaginosis–associated microorganisms in endometritis. Am. J. Obstet. Gynecol. 1996, 175, 435–441. [Google Scholar] [CrossRef]
- Nikolic, B.; Nguyen, K.; Martin, L.G.; Redd, D.C.; Best, I.; Silverstein, M.I. Pyosalpinx Developing from a Preexisting Hydrosalpinx after Uterine Artery Embolization. J. Vasc. Interv. Radiol. 2004, 15, 297–301. [Google Scholar] [CrossRef]
- Chan, C.C.; Ng, E.H.; Li, C.F.; Ho, P.C. Impaired ovarian blood flow and reduced antral follicle count following laparoscopic salpingectomy for ectopic pregnancy. Hum. Reprod. 2003, 18, 2175–2180. [Google Scholar] [CrossRef] [Green Version]
- Strandell, A.; Lindhard, A.; Waldenström, U.; Thorburn, J. Prophylactic salpingectomy does not impair the ovarian response in IVF treatment. Hum. Reprod. 2001, 16, 1135–1139. [Google Scholar] [CrossRef] [Green Version]
- Song, X.-M.; Jiang, H.; Zhang, W.-X.; Zhou, Y.; Ni, F.; Wang, X.-M. Ultrasound sclerotherapy pretreatment could obtain a similar effect to surgical intervention on improving the outcomes of in vitro fertilization for patients with hydrosalpinx. J. Obstet. Gynaecol. Res. 2017, 43, 122–127. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Results | ||
|---|---|---|
| Right Uterus | Left Uterus | |
| ERA (endometrial receptivity array) | Receptive 126+/−3 h | Receptive 126+/−3 h |
| EMMA (endometrial microbiome metagenomic analysis) | Abnormal endometrial microbiome Lactobacillus 0% Escherichia 46.78% Trabulsiella 31.69% Microbacterium 5.54% Others 15.99% | Abnormal endometrial microbiome Lactobacillus 0% Escherichia 49.91% Trabulsiella 30.67% Microbacterium 5.99% Streptococcus 5.84% Others 7.59% |
| ALICE (analysis of infectious chronic endometritis) | Escherichia 46.78% | Escherichia 49.91% |
| Immunostaining with CD138 McQueen’s classification | None Score 0 | None Score 0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mitsui, J.; Kawai, K.; Tajima, M.; Hiraoka, K.; Casaroli, V.; Sato, Y.; Furusawa, Y.; Ishikawa, T.; Miyasaka, N. Effects of Hydrosalpinx on Endometrial Receptivity and Uterine Microbiome: An Interesting Case of Double Uterus with Unilateral Hydrosalpinx. Endocrines 2022, 3, 821-830. https://doi.org/10.3390/endocrines3040068
Mitsui J, Kawai K, Tajima M, Hiraoka K, Casaroli V, Sato Y, Furusawa Y, Ishikawa T, Miyasaka N. Effects of Hydrosalpinx on Endometrial Receptivity and Uterine Microbiome: An Interesting Case of Double Uterus with Unilateral Hydrosalpinx. Endocrines. 2022; 3(4):821-830. https://doi.org/10.3390/endocrines3040068
Chicago/Turabian StyleMitsui, Junichiro, Kiyotaka Kawai, Makiko Tajima, Kenichiro Hiraoka, Viviane Casaroli, Yoshimi Sato, Yoshiaki Furusawa, Tomonori Ishikawa, and Naoyuki Miyasaka. 2022. "Effects of Hydrosalpinx on Endometrial Receptivity and Uterine Microbiome: An Interesting Case of Double Uterus with Unilateral Hydrosalpinx" Endocrines 3, no. 4: 821-830. https://doi.org/10.3390/endocrines3040068