1. Introduction
Epithelial ovarian cancer is the fifth leading cause of cancer death for biologically female individuals in the United States [
1]. Efforts to develop screening strategies to prevent ovarian cancer have been unsuccessful [
2]. Potential precursors for high-grade serous ovarian carcinomas (HGSOCs) have been identified in the distal fallopian tubes of patients with BRCA1/2 mutations; salpingectomy may reduce the risk of these lesions progressing to cancer [
3,
4,
5].
Evidence-based recommendations suggest that risk-reducing salpingo-oophorectomy (RRSO) be considered for high-risk patients, once childbearing is complete, or by the age of 35 years [
6,
7]. National professional organizations in the United States [
8,
9,
10], Canada [
11], and regional health authorities encourage salpingectomy at the time of benign gynecologic surgery for those with an average background risk, because it may achieve risk reduction while preserving ovarian function [
8,
9,
10,
11,
12,
13,
14,
15,
16,
17]. Salpingectomy at the time of benign gynecologic surgery as well as during cesarean and following vaginal delivery is safe, feasible, and cost effective [
18,
19,
20,
21,
22,
23].
Data promoting the safety of post-partum salpingectomy derive from studies utilizing costly electrocautery devices, which may only be available in high-resource settings [
21]. Prospective evidence evaluating the safety of post-partum salpingectomy (PPS), particularly in low-resource settings or without using costly equipment, is still lacking. Herein, we describe a standardized protocol for performing PPS as a strategy for the prevention of HGSOCs. We hypothesize that PPS would be feasible, compared to post-partum bilateral tubal ligation (PP-BTL) with similar operative times and estimated blood loss (EBL).
2. Materials and Methods
Permission to conduct this study was obtained from the Institutional Review Boards for Baylor College of Medicine (H-32860) and the Harris Health System (13-06-0471). Gravidae undergoing post-partum tubal permanent contraception at Ben Taub Hospital were identified and approached for possible inclusion between 15 July 2013 and 31 March 2014. Two groups of gravidae were considered eligible: (1) those undergoing post-partum tubal permanent contraception on post-partum days #0–2 following vaginal delivery, or (2) those undergoing post-partum tubal permanent contraception at the time of cesarean. All participants met the state and institutional requirements for post-partum permanent contraception; the state required a minimum age of 21 years and that consent for permanent contraception be obtained a minimum of 30 days and a maximum of 180 days prior to the procedure. There are no criteria related to parity. For the purposes of this study, gravidae under the age of 25 years, or who expressed uncertainty regarding permanent contraception, or who had an impaired decision-making capacity were excluded.
Written informed consent for participation in this study was obtained from all participants. This consent specifically discussed that the performance of PPS for permanent contraception was part of a research study and not the standard of care for permanent contraception. The consent process also involved a discussion that there may theoretically be additional risks to undergoing PPS, compared to the routinely offered modified Pomeroy or Parkland methods for permanent tubal sterilization. The consent discussion indicated that, unlike a partial salpingectomy via the Pomeroy or Parkland methods, the PPS procedure could not be reversed via surgery and that this procedure was absolutely not reversible. Finally, while the consent discussion mentioned that the purpose of removing the whole fallopian tube was to theoretically reduce the risk of ovarian cancer, we specifically stated that this benefit may not benefit the particular participant. Any gravidae who declined to participate in this study received permanent sterilization via the standard of care using either the modified Pomeroy or Parkland method. However, due to potential differences between concurrent groups who were or were not offered the PPS study, a historical cohort was used as the control group.
For the purposes of this study, PPS was defined as the removal of the entire distal fallopian tube starting at a point 1–2 cm lateral to the uterine cornua. Feasibility was defined as a non-doubling of the estimated blood loss (EBL) (i.e., from 12.5 to 25 mL) for procedures performed after vaginal deliveries and an EBL increase of less than 150 mL at the time of cesarean. The target EBL difference was greater for cesareans given the higher EBL and therefore higher range for error. Peri-operative complications, including wound dehiscence, wound infection, intra-operative injury, and need for blood transfusion, were also collected. The reported complication rates following post-partum tubal permanent contraception procedures, including tubal ligation and salpingectomy, are low and range from 0.3–2% [
18,
19,
21], making an adequately powered study to detect meaningful differences in the complication rates between the two procedures unfeasible, especially because, at the time this study was performed, the complication rate of post-partum salpingectomy by this suture-based method was not known. Therefore, operative time was chosen as the primary outcome and EBL as the secondary outcome. Other secondary outcomes included skin incision size, requirement for intra-operative blood transfusion, urinary tract injury, a lost pedicle or bleeding from the mesosalpinx, injury to the surrounding structures, and whether the procedure was aborted. Postoperative secondary outcomes were also evaluated, including superficial wound separation, wound dehiscence, re-admission, cellulitis, blood transfusion, and whether pathology confirmed permanent contraception.
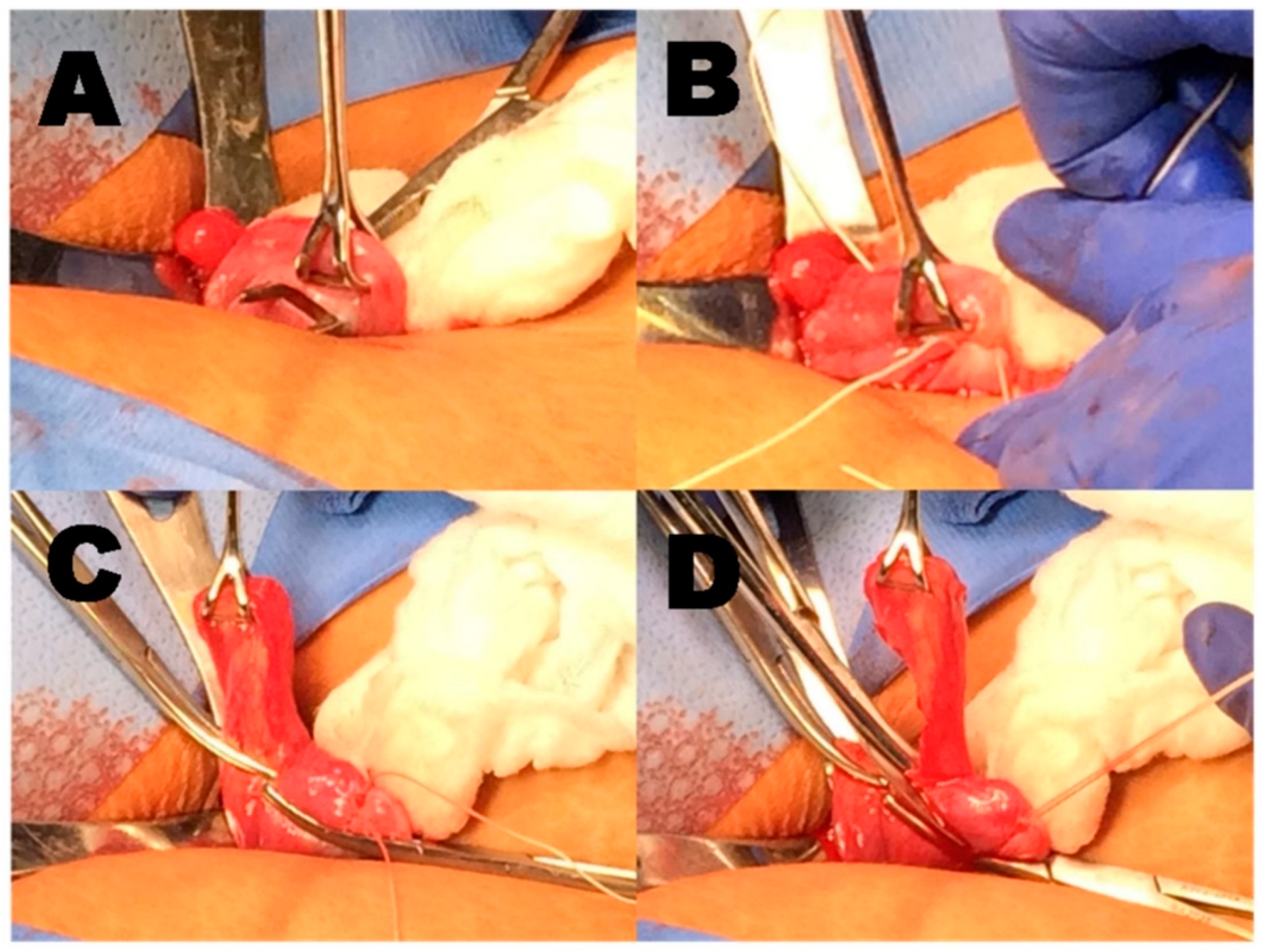
This procedure was designed to remove as much tube as possible while avoiding dilated vasculature along the lateral aspect of the uterus and broad ligament (
Figure 1). After delivering each tube through a 2–3 cm infra-umbilical incision (for PPS following vaginal delivery), a window was made in an avascular area of the mesosalpinx. The proximal end of each tube was doubly suture ligated 1–2 cm lateral to the uterine cornua and transected between the ties. The mesosalpinx underlying the distal tube was then clamped with straight hemostats and the fallopian tube excised and the mesosalpinx tied. Each pedicle created in this fashion was secured with a 2-0 vicryl suture; typically the study site used plain gut for surgical permanent contraception. Vicryl was chosen for the study procedure due to the vascularity and size of the pedicles being secured. Following excision of the tube, the proximal 1 cm of each specimen was trimmed and sent for histologic confirmation of permanent contraception. The remaining portion of the tube was reviewed for serous tubal intraepithelial carcinoma lesions by a pathologist (RM) for research purposes. The procedure for PPS at the time of cesarean delivery was identical. As per standard of care at the institution, the primary surgeon for all study procedures was an intern or second-year resident directly assisted by a fourth-year resident. An attending physician was present for all cases. To ensure study uniformity, all residents and faculty were educated at the start of each clinical block regarding the standardized study procedure. Participating surgeons were asked to document protocol deviations or the difficulties encountered with performing the study procedure per protocol.
Demographic data were abstracted from the electronic health record. The primary outcome was operative time from skin incision to closure obtained from the anesthesia record. The operative note was reviewed for secondary outcomes and feasibility assessment, including estimated blood loss (EBL) as assessed by the surgeon, and any documented complications or protocol deviations. At the time that this study was performed, blood loss for both post-partum permanent contraception procedures and cesarean births were by visually estimated blood loss in accordance with specific didactics on estimating blood loss, wherein the amount of blood on laparotomy sponges was compared to normative standards and added to the blood in suction cannisters [
24]. Regarding the indication for cesarean birth, at this institution during this time period, there were no cesareans performed for the indication of maternal request.
Retrospective data were abstracted for two cohorts of gravidae who underwent post-partum tubal ligations between 1 July 2012 and 1 August 2013 for comparison. Retrospective data were chosen to minimize bias for the comparison group, because those who declined or who were not offered post-partum salpingectomy may have different perceived risks of post-partum salpingectomy than those offered a tubal ligation. The first control group (n = 200) underwent modified Pomeroy tubal ligations following vaginal delivery (SVD-BTL). A Pomeroy tubal ligation is performed by elevating a segment of the fallopian tube and tying an absorbable suture around the base. At the study institution, this was performed with plain gut suture and two sutures were placed for additional hemostasis. Following suture ligation, the tubal segment between the ligatures is cut and removed. A second control group (n = 100) underwent Parkland tubal ligation with cesarean, as per institutional practice (CD-BTL). A Parkland tubal ligation is performed by tying two separate absorbable sutures around the fallopian tube: one at its proximal to middle segment and one a few centimeters away. The tubal segment between the ligatures is then cut and removed. To control for surgeon skill level, control cohorts were assembled by sequentially identifying all post-partum people who underwent tubal ligation at this institution starting 1 July 2012 (the start of the 2012–2013 academic year) until accrual targets for each group were achieved. The month of July was chosen as the starting month to identify controls because the study arm also began accrual in July.
Statistical analyses were performed on an intention-to-treat basis using SPSS software (IBM SPSS, Version 22.0, IBM, Inc., Armonk, NY, USA, 2013). Pearson’s χ2 test or Fisher’s exact test was used to assess categorical variables, and Student’s t-test was used to compare normally distributed continuous variables. The Shapiro–Wilk test was used to determine normality. The Wilcoxon Rank-Sum test was used to compare non-normally distributed continuous variables, including operative time and EBL. A p-value of ≤0.05 was considered significant.
3. Results
A total of 165 gravidae were consented and compared to 300 historical controls. Of the participants who consented, eight were pre-operatively deemed to be ineligible for post-partum tubal permanent contraception by the surgical team (
Figure 2). Thus, 157 participants underwent surgery with the intent to perform PPS. A total of 97 underwent PPS following vaginal delivery (SVD + PPS) and 60 participants underwent PPS following cesarean delivery (CD + PPS). Procedures on 9 participants were converted to traditional SVD-BTL; 3 preoperatively and 6 intra-operatively. Three were converted to SVD-BTL because the upper-level resident felt that the intern was insufficiently familiar with the surgical procedure to perform the PPS. Reasons for intra-operative conversion included difficulties obtaining the entire tube due to adhesions (
n = 4), and the presence of multiple large (≥4 cm) paratubal cysts (
n = 1). All were included in the SVD + PPS group based upon intention to treat. In the control group, five underwent unexpected procedural changes intra-operatively. One SVD-BTL subject did not undergo tubal permanent contraception due to adhesive disease. Of the aborted procedures, in the SVD-BTL group, one tie slipped off, which led to mesosalpinx bleeding, which resulted in an unplanned salpingectomy, and in one case only the left tube was transected due to adhesions. In the CD-PPS group, there was one case where the mesosalpinx was not clamped according to the protocol, which resulted in a broad ligament hematoma and the salpingectomy was not completed; one case where there was a cystotomy related to the cesarean and the surgeon opted to forego the salpingectomy due to operative time; and one related to a perceived increase in operative time and poor visualization due to adhesions. Of the CD-BTL cases that were aborted, three mentioned adhesions as a barrier and were converted to either clip placement or fimbriectomy, and two cited bleeding or dilated blood vessels in the mesosalpinx as reasons to perform a fimbriectomy rather than the planned Parkland tubal ligation. Sixteen participants underwent PPS with surgeon-dependent procedural modifications, which included variations in the methodology of clamping and suture ligation. In each case, changes were made to facilitate the completion of the procedure or to accommodate surgeon comfort. None of these changes prevented the successful removal of the fallopian tube in its entirety. Demographic data are summarized in
Table 1. Participants undergoing PPS at cesarean were slightly older than those undergoing SVD-BTL at cesarean, and the number of prior abdominal surgeries was slightly higher in the SVD-BTL and CD-BTL groups compared to the SVD-PPS and CD-PPS groups, respectively. There were no other demographic differences between PPS participants and controls.
The incidence of intra-operative complications observed in participants undergoing PPS was similar to that observed in controls who underwent standard PP-BTL (
Table 2). Compared to controls, operative time was longer for SVD + PPS. EBL was also greater. Operative time for PPS at cesarean was also longer compared to CD-BTL. No differences were found in the proportion of PPS or controls who received an intra-operative transfusion; experienced bleeding from the mesosalpinx; or a lost surgical pedicle, urinary tract injury, or accidental uterine injury.
The most common intra-operative complication observed with PPS was bleeding due to the loss of a pedicle or bleeding from the mesosalpinx. Three participants in the SVD + PPS group experienced this complication. In one subject, blood loss (EBL 100 mL) required surgeons to extend the skin incision from 3 to 8 cm. In the other two cases, there was no need to extend the skin incision. EBLs for these cases were 50 mL and 150 mL, respectively. For two of these participants, modifications had been made to the recommended protocol for performing PPS by the operating team prior to the complication. Because these modifications potentially contributed to bleeding, modifications to the procedure were discouraged unless indicated for safety. Among CD + PPS participants, one subject developed a broad ligament hematoma following right salpingectomy. After bleeding was controlled, PPS was abandoned and a Parkland tubal ligation was performed on the contralateral tube. EBL for this case (including cesarean delivery) was 1500 mL. No other intra-operative complications were encountered in the SVD + PPS group. Among SVD-BTL controls, one subject experienced an ovarian laceration, which was repaired.
The incidence of postoperative complications was also similar between PPS and control participants (
Table 3). One subject who underwent PPS after vaginal delivery was re-admitted postoperatively with a complicated urinary tract infection. There were no differences in any other complications. PPS had no impact on the ability of pathologists to histologically confirm permanent contraception. Tubal tissue was identified in 100% of participants in the PPS and 99% of the PP-BTL control groups. In the SVD-BTL historical control group, tubal permanent contraception could not be confirmed for two because surgical specimens were lost postoperatively.
4. Discussion
Our study demonstrates that a standardized, low-cost protocol for performing PPS utilizing suture ligation is safe and feasible when compared to PP-BTL. Our data indicate that this protocol can be easily learned and safely performed in resource-limited environments. Furthermore, we demonstrated that this procedure can be performed by trainees with minimal surgical experience without the need for specialized equipment, such as expensive electrothermal bipolar devices. In comparison to historical controls, PPS + SVD resulted in small, but statistically significant, increases in both EBL and operative time, but the EBL remained < 25 mL and operative time < 40 min. These results met our specification of feasibility with a marginal increase in operative time. Our results suggest that the rate of major complications associated with PPS is likely <1%, and that it is sufficiently safe to examine the efficacy of the PPS procedure defined here as part of larger prospective clinical trials. Given that the procedures described were learned and implemented by resident physician surgeons rotating on a monthly basis at an academic teaching facility, our findings suggest that implementation would be feasible in similar clinical settings.
Our findings are similar to a recent publication by Parikh et al., who found that salpingectomy at the time of cesarean and after vaginal delivery may be safe, both using electrocautery methods and a clamp, cut, and tie technique [
25]. Specifically, they found that salpingectomy took approximately 10 min longer [
25]. However, they used a calculated method for assessing blood loss and found no difference in hemoglobin change between salpingectomy and tubal ligation for either cesarean or post-vaginal delivery procedures.
The role of the distal fallopian tube in the development of HGSOC is now well supported by molecular evidence [
4,
5,
22] and the incorporation of salpingectomy into the post-partum period, at the time of cesarean delivery, and at the time of benign of gynecologic surgery has been well documented over the last decade [
9,
15,
23]. A recent meta-analysis evaluating salpingectomy at the time of cesarean demonstrated similar operative times across three randomized controlled trials comparing salpingectomy to bilateral tubal ligation without significant differences in perioperative complications, length of stay, EBL, or post-partum re-admissions [
26]. Additionally, two other studies retrospectively evaluated operative outcomes for the incorporation of salpingectomy in the immediate post-partum period following vaginal delivery [
21,
22]. Danis et al. [
22] compared post-partum salpingectomy to post-partum bilateral tubal ligation in a retrospective consecutive cohort, and found significantly longer operative times for those undergoing post-partum salpingectomy (71.44 min ± 5.81 vs. 59.13 min ± 16 min
p = 0.003) similar to our own findings. Wagar et al. [
21] reported a shorter median operative time for post-partum salpingectomy compared to bilateral tubal ligation immediately following vaginal delivery (30 min [IQR 24–38] vs. 34 min [IQR 26–42],
p = 032). However, 97% of post-partum salpingectomy cases utilized a bipolar electrocautery device [
21]. Our protocol adds evidence to the feasibility of utilizing suture ligation methods for completing this procedure without the need for expensive and possibly cost-prohibitive devices.
The use of post-partum-female permanent contraception varies widely by country [
27]. Descriptions on the use of post-partum tubal ligations for permanent contraception and complication rates are available for at least two low and middle-income countries [
28,
29], and descriptions on how to increase accessibility by alternative approaches to analgesia are also available [
30]. Our procedure described here would allow access not only to contraception, but also potential ovarian cancer risk reduction.
A clear strength of our study is the low cost associated with the implementation of our protocol. At our institution, PPS only required the addition of two straight hemostats to the surgical instrument trays routinely used to perform standard SVD-BTL. The entire surgical tray comprises a 10-blade scalpel, 2 Allis clamps, a needle holder, 2 Babcock clamps, Metzenbaum scissors, and 1–3 straight hemostats. Given the implications of salpingectomy to reduce the risk of HGSOCs, efforts to promote the completion of this procedure in low-resource environments are needed to mitigate potential disparities in access to risk-reduction strategies. Given the uptake of this protocol in our institution with a very high completion rate and comparably low rate of postoperative complications, the generalizability of our findings to other teaching institutions is possible.
Several limitations to our study exist. First, the surgical protocol was not developed using evidence-based studies to decide which technique for salpingectomy is best. We designed PPS for cost efficiency and to resemble the methods for surgical permanent contraception used at the hospital. Second, the study suffered from biases typically associated with the use of historical controls. Although the four groups were demographically similar, two different groups of resident surgeons performed PPS and PP-BTL surgeries based upon advancing academically through the residency program. To minimize the impact of this potential issue, controls were identified from those undergoing standard PP-BTL starting in July of the year preceding study enrollment, so that trainees performing surgical procedures would be at a similar point in their training. Additionally, surgeons were not blinded to this procedure. Thus, there was significant potential for bias in estimating blood loss, particularly because blood loss was estimated visually and not quantified by weighing laparotomy sponges. We are also unable to conclude the effect of salpingectomy on the long-term benefit of reducing the risk of HGSOCs, and prospective long-term data are needed to elucidate an optimal means of preventing this disease. The operative times at this institution were universally longer than other institutions. This is likely related to both the presence of scar tissue at the time of repeat cesarean birth and the fact that these cases are performed by two resident physicians with an attending physician supervising, rather than having the whole case performed by either an attending physician or an attending physician with one resident physician. The estimated blood loss at cesarean was also higher than the median reported in the literature [
31], but here we reported mean blood loss rather than median, which can be skewed by outliers, and it was also an estimate of blood loss, which has its own limitations. Due to hematocrit not being routinely checked after a permanent contraception procedure after SVD, we were also not able to calculate blood loss; a calculated blood loss may have increased or decreased the difference between salpingectomy and tubal ligation groups. Indeed, Parikh et al. demonstrated no difference in blood loss between salpingectomy and tubal ligation when comparing hemoglobin changes [
25].



 ,
, 


{kind=link}
{kind=link}