
Complications in Acute Myocardial Infarction: Navigating Challenges in Diagnosis and Management
 , , , , and
, , , , and
Abstract
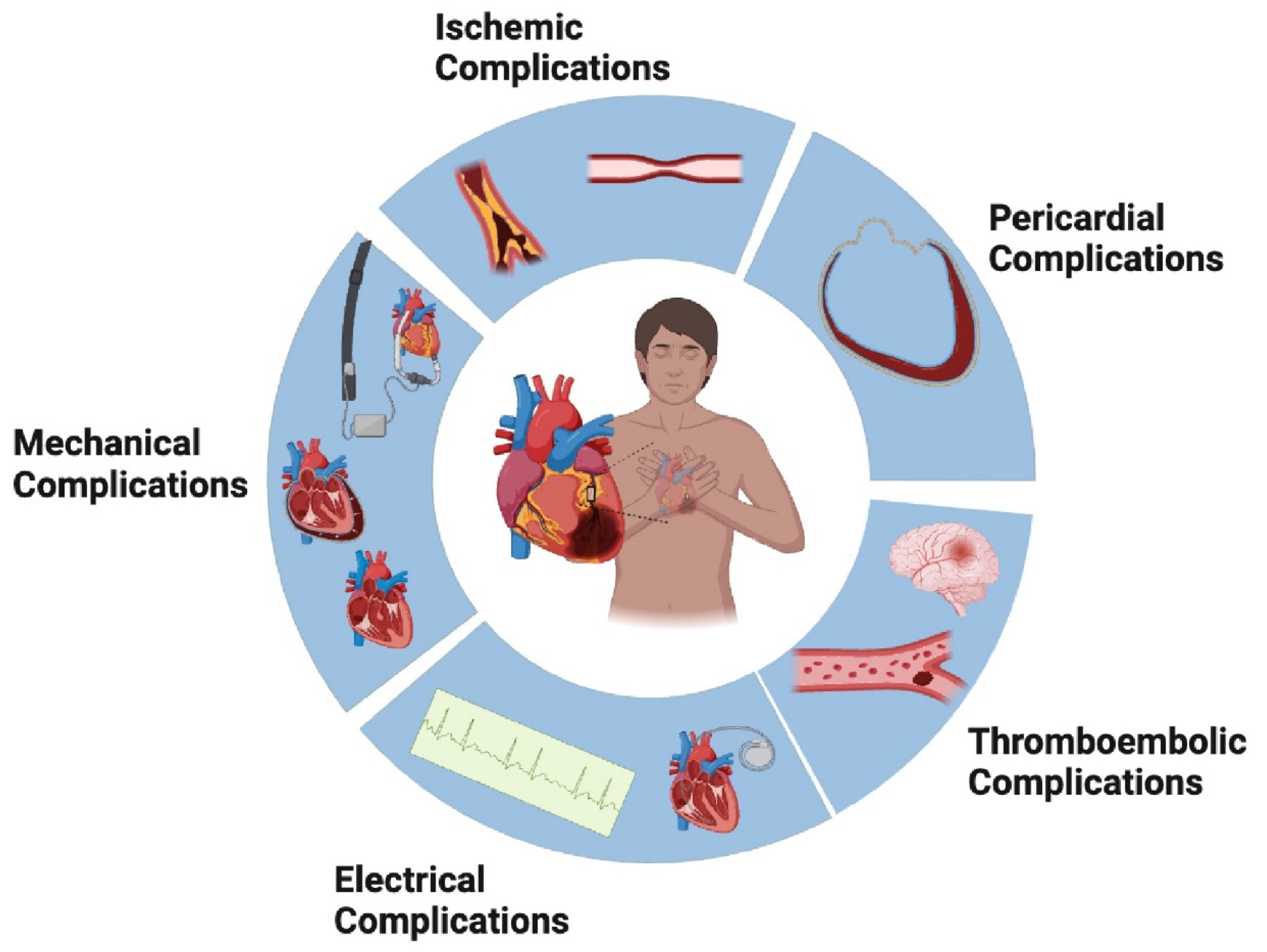
:1. Introduction
2. Mechanical Complications
2.1. Papillary Muscle Rupture and Ischemic Mitral Regurgitation
2.2. Ventricular Septal Rupture
2.3. Free Wall Rupture
2.4. True and Pseudoaneurysms
2.5. Left Ventricular Failure and Cardiogenic Shock
2.6. Right Ventricular Myocardial Infarction
2.7. Dynamic Left Ventricular Outflow Tract Obstruction
3. Electrical Complications
3.1. Atrial Tachyarrhythmias
3.2. Ventricular Tachyarrhythmias
3.3. Bradyarrhythmia’s
4. Ischemic Complications
5. Pericardial Complications
6. Thromboembolic Complications
7. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Thygesen, K.; Alpert, J.S.; Jaffe, A.S.; Chaitman, B.R.; Bax, J.J.; Morrow, D.A.; White, H.D.; ESC Scientific Document Group. Fourth universal definition of myocardial infarction (2018). Eur. Heart J. 2019, 40, 237–269. [Google Scholar] [CrossRef]
- Dyrbuś, K.; Gąsior, M.; Desperak, P.; Osadnik, T.; Nowak, J.; Banach, M. The prevalence and management of familial hypercholesterolemia in patients with acute coronary syndrome in the Polish tertiary centre: Results from the TERCET registry with 19,781 individuals. Atherosclerosis 2019, 288, 33–41. [Google Scholar] [CrossRef] [PubMed]
- Kwok, C.S.; Abbas, K.S.; Qureshi, A.I.; Lip, G.Y.H. Outcomes for patients hospitalized with acute myocardial infarction and cerebral infarction in the United States: Insights from the National Inpatient Sample. Intern. Emerg. Med. 2023, 18, 375–383. [Google Scholar] [CrossRef] [PubMed]
- Gerber, Y.; Weston, S.A.; Jiang, R.; Roger, V.L. The changing epidemiology of myocardial infarction in Olmsted County, Minnesota, 1995–2012. Am. J. Med. 2015, 128, 144–151. [Google Scholar] [CrossRef] [PubMed]
- Rogers, W.J.; Frederick, P.D.; Stoehr, E.; Canto, J.G.; Ornato, J.P.; Gibson, C.M.; Pollack, C.V.; Gore, J.M.; Chandra-Strobos, N.; Peterson, E.D.; et al. Trends in presenting characteristics and hospital mortality among patients with ST elevation and non-ST elevation myocardial infarction in the National Registry of Myocardial Infarction from 1990 to 2006. Am. Heart J. 2008, 156, 1026–1034. [Google Scholar] [CrossRef] [PubMed]
- French, J.K.; Hellkamp, A.S.; Armstrong, P.W.; Cohen, E.; Kleiman, N.S.; O’Connor, C.M.; Holmes, D.R.; Hochman, J.S.; Granger, C.B.; Mahaffey, K.W. Mechanical Complications After Percutaneous Coronary Intervention in ST-Elevation Myocardial Infarction (from APEX-AMI). Am. J. Cardiol. 2010, 105, 59–63. [Google Scholar] [CrossRef] [PubMed]
- Bueno, H.; Martínez-Sellés, M.; Pérez-David, E.; López-Palop, R. Effect of thrombolytic therapy on the risk of cardiac rupture and mortality in older patients with first acute myocardial infarction†. Eur. Heart J. 2005, 26, 1705–1711. [Google Scholar] [CrossRef]
- Salari, N.; Morddarvanjoghi, F.; Abdolmaleki, A.; Rasoulpoor, S.; Khaleghi, A.A.; Hezarkhani, L.A.; Shohaimi, S.; Mohammadi, M. The global prevalence of myocardial infarction: A systematic review and meta-analysis. BMC Cardiovasc. Disord. 2023, 23, 206. [Google Scholar] [CrossRef]
- Chevalier, P.; Burri, H.; Fahrat, F.; Cucherat, M.; Jegaden, O.; Obadia, J.-F.; Kirkorian, G.; Touboul, P. Perioperative outcome and long-term survival of surgery for acute post-infarction mitral regurgitation. Eur. J. Cardiothorac. Surg. 2004, 26, 330–335. [Google Scholar] [CrossRef]
- Calvo, F.E.; Figueras, J.; Cortadellas, J.; Soler-Soler, J. Severe mitral regurgitation complicating acute myocardial infarction: Clinical and angiographic differences between patients with and without papillary muscle rupture. Eur. Heart J. 1997, 18, 1606–1610. [Google Scholar] [CrossRef]
- Thompson, C.R.; Buller, C.E.; Sleeper, L.A.; Antonelli, T.A.; Webb, J.G.; Jaber, W.A.; Abel, J.G.; Hochman, J.S. Cardiogenic shock due to acute severe mitral regurgitation complicating acute myocardial infarction: A report from the SHOCK Trial Registry. SHould we use emergently revascularize Occluded Coronaries in cardiogenic shocK? J. Am. Coll. Cardiol. 2000, 36, 1104–1109. [Google Scholar] [CrossRef] [PubMed]
- Durko, A.P.; Budde, R.P.J.; Geleijnse, M.L.; Kappetein, A.P. Recognition, assessment and management of the mechanical complications of acute myocardial infarction. Heart 2018, 104, 1216–1223. [Google Scholar] [CrossRef] [PubMed]
- Vahanian, A.; Beyersdorf, F.; Praz, F.; Milojevic, M.; Baldus, S.; Bauersachs, J.; Capodanno, D.; Conradi, L.; De Bonis, M.; De Paulis, R.; et al. 2021 ESC/EACTS Guidelines for the management of valvular heart disease: Developed by the Task Force for the management of valvular heart disease of the European Society of Cardiology (ESC) and the European Association for Cardio-Thoracic Surgery (EACTS). Eur. Heart J. 2022, 43, 561–632. [Google Scholar] [CrossRef] [PubMed]
- Hennessey, B.; Sabatovicz, N.; Del Trigo, M. Acute Ischaemic Mitral Valve Regurgitation. J. Clin. Med. 2022, 11, 5526. [Google Scholar] [CrossRef]
- Whiting, P.C.; Morgan-Hughes, N.J. Transesophageal echocardiographic findings in papillary muscle rupture. Anesth. Analg. 2005, 101, 1292–1293. [Google Scholar] [CrossRef] [PubMed]
- Bouma, W.; Wijdh-den Hamer, I.J.; Koene, B.M.; Kuijpers, M.; Natour, E.; Erasmus, M.E.; Jainandunsing, J.S.; van der Horst, I.C.C.; Gorman, J.H.; Gorman, R.C.; et al. Long-term survival after mitral valve surgery for post-myocardial infarction papillary muscle rupture. J. Cardiothorac. Surg. 2015, 10, 11. [Google Scholar] [CrossRef]
- Russo, A.; Suri, R.M.; Grigioni, F.; Roger, V.L.; Oh, J.K.; Mahoney, D.W.; Schaff, H.V.; Enriquez-Sarano, M. Clinical outcome after surgical correction of mitral regurgitation due to papillary muscle rupture. Circulation 2008, 118, 1528–1534. [Google Scholar] [CrossRef]
- Adamo, M.; Curello, S.; Chiari, E.; Fiorina, C.; Chizzola, G.; Magatelli, M.; Locantore, E.; Cuminetti, G.; Lombardi, C.; Manzato, A.; et al. Percutaneous edge-to-edge mitral valve repair for the treatment of acute mitral regurgitation complicating myocardial infarction: A single centre experience. Int. J. Cardiol. 2017, 234, 53–57. [Google Scholar] [CrossRef]
- Estévez-Loureiro, R.; Arzamendi, D.; Freixa, X.; Cardenal, R.; Carrasco-Chinchilla, F.; Serrador-Frutos, A.; Pan, M.; Sabaté, M.; Diaz, J.; Hernández, J.M.; et al. Percutaneous Mitral Valve Repair for Acute Mitral Regurgitation After an Acute Myocardial Infarction. J. Am. Coll. Cardiol. 2015, 66, 91–92. [Google Scholar] [CrossRef]
- Birnbaum, Y.; Fishbein, M.C.; Blanche, C.; Siegel, R.J. Ventricular septal rupture after acute myocardial infarction. N. Engl. J. Med. 2002, 347, 1426–1432. [Google Scholar] [CrossRef]
- Menon, V.; Webb, J.G.; Hillis, L.D.; Sleeper, L.A.; Abboud, R.; Dzavik, V.; Slater, J.N.; Forman, R.; Monrad, E.S.; Talley, J.D.; et al. Outcome and profile of ventricular septal rupture with cardiogenic shock after myocardial infarction: A report from the SHOCK Trial Registry. SHould we emergently revascularize Occluded Coronaries in cardiogenic shocK? J. Am. Coll. Cardiol. 2000, 36, 1110–1116. [Google Scholar] [CrossRef]
- Crenshaw, B.S.; Granger, C.B.; Birnbaum, Y.; Pieper, K.S.; Morris, D.C.; Kleiman, N.S.; Vahanian, A.; Califf, R.M.; Topol, E.J. Risk factors, angiographic patterns, and outcomes in patients with ventricular septal defect complicating acute myocardial infarction. GUSTO-I (Global Utilization of Streptokinase and TPA for Occluded Coronary Arteries) Trial Investigators. Circulation 2000, 101, 27–32. [Google Scholar] [CrossRef] [PubMed]
- Honda, S.; Asaumi, Y.; Yamane, T.; Nagai, T.; Miyagi, T.; Noguchi, T.; Anzai, T.; Goto, Y.; Ishihara, M.; Nishimura, K.; et al. Trends in the clinical and pathological characteristics of cardiac rupture in patients with acute myocardial infarction over 35 years. J. Am. Heart Assoc. 2014, 3, e000984. [Google Scholar] [CrossRef] [PubMed]
- Jones, B.M.; Kapadia, S.R.; Smedira, N.G.; Robich, M.; Tuzcu, E.M.; Menon, V.; Krishnaswamy, A. Ventricular septal rupture complicating acute myocardial infarction: A contemporary review. Eur. Heart J. 2014, 35, 2060–2068. [Google Scholar] [CrossRef] [PubMed]
- Moreyra, A.E.; Huang, M.S.; Wilson, A.C.; Deng, Y.; Cosgrove, N.M.; Kostis, J.B. MIDAS Study Group (MIDAS 13) Trends in incidence and mortality rates of ventricular septal rupture during acute myocardial infarction. Am. J. Cardiol. 2010, 106, 1095–1100. [Google Scholar] [CrossRef] [PubMed]
- Delmas, C.; Barbosa, H.; David, C.-H.; Bouisset, F.; Piriou, P.-G.; Roubille, F.; Leick, J.; Pavlov, M.; Leurent, G.; Potapov, E.V.; et al. Impella for the Management of Ventricular Septal Defect Complicating Acute Myocardial Infarction: A European Multicenter Registry. ASAIO J. 2023, 69, e491. [Google Scholar] [CrossRef] [PubMed]
- Daggett, W.M.; Guyton, R.A.; Mundth, E.D.; Buckley, M.J.; McEnany, M.T.; Gold, H.K.; Leinbach, R.C.; Austen, W.G. Surgery for post-myocardial infarct ventricular septal defect. Ann. Surg. 1977, 186, 260–271. [Google Scholar] [CrossRef]
- David, T.E.; Dale, L.; Sun, Z. Postinfarction ventricular septal rupture: Repair by endocardial patch with infarct exclusion. J. Thorac. Cardiovasc. Surg. 1995, 110, 1315–1322. [Google Scholar] [CrossRef]
- Singh, V.; Rodriguez, A.P.; Bhatt, P.; Alfonso, C.E.; Sakhuja, R.; Palacios, I.F.; Inglessis-Azuaje, I.; Cohen, M.G.; Elmariah, S.; O’Neill, W.W. Ventricular Septal Defect Complicating ST-Elevation Myocardial Infarctions: A Call for Action. Am. J. Med. 2017, 130, 863.e1–863.e12. [Google Scholar] [CrossRef]
- Ibanez, B.; James, S.; Agewall, S.; Antunes, M.J.; Bucciarelli-Ducci, C.; Bueno, H.; Caforio, A.L.P.; Crea, F.; Goudevenos, J.A.; Halvorsen, S.; et al. 2017 ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation: The Task Force for the management of acute myocardial infarction in patients presenting with ST-segment elevation of the European Society of Cardiology (ESC). Eur. Heart J. 2018, 39, 119–177. [Google Scholar] [CrossRef]
- Ronco, D.; Matteucci, M.; Kowalewski, M.; De Bonis, M.; Formica, F.; Jiritano, F.; Fina, D.; Folliguet, T.; Bonaros, N.; Russo, C.F.; et al. Surgical Treatment of Postinfarction Ventricular Septal Rupture. JAMA Netw. Open 2021, 4, e2128309. [Google Scholar] [CrossRef] [PubMed]
- Faccini, A.; Butera, G. Techniques, Timing, and Prognosis of Transcatheter Post Myocardial Infarction Ventricular Septal Defect Repair. Curr. Cardiol. Rep. 2019, 21, 59. [Google Scholar] [CrossRef] [PubMed]
- Calvert, P.A.; Cockburn, J.; Wynne, D.; Ludman, P.; Rana, B.S.; Northridge, D.; Mullen, M.J.; Malik, I.; Turner, M.; Khogali, S.; et al. Percutaneous closure of postinfarction ventricular septal defect: In-hospital outcomes and long-term follow-up of UK experience. Circulation 2014, 129, 2395–2402. [Google Scholar] [CrossRef] [PubMed]
- Becker, A.E.; van Mantgem, J.P. Cardiac tamponade. A study of 50 hearts. Eur. J. Cardiol. 1975, 3, 349–358. [Google Scholar] [PubMed]
- Slater, J.; Brown, R.J.; Antonelli, T.A.; Menon, V.; Boland, J.; Col, J.; Dzavik, V.; Greenberg, M.; Menegus, M.; Connery, C.; et al. Cardiogenic shock due to cardiac free-wall rupture or tamponade after acute myocardial infarction: A report from the SHOCK Trial Registry. Should we emergently revascularize occluded coronaries for cardiogenic shock? J. Am. Coll. Cardiol. 2000, 36, 1117–1122. [Google Scholar] [CrossRef] [PubMed]
- Reardon, M.J.; Carr, C.L.; Diamond, A.; Letsou, G.V.; Safi, H.J.; Espada, R.; Baldwin, J.C. Ischemic left ventricular free wall rupture: Prediction, diagnosis, and treatment. Ann. Thorac. Surg. 1997, 64, 1509–1513. [Google Scholar] [CrossRef] [PubMed]
- Formica, F.; Mariani, S.; Singh, G.; D’Alessandro, S.; Messina, L.A.; Jones, N.; Bamodu, O.A.; Sangalli, F.; Paolini, G. Postinfarction left ventricular free wall rupture: A 17-year single-centre experience. Eur. J. Cardiothorac. Surg. 2018, 53, 150–156. [Google Scholar] [CrossRef]
- Matteucci, M.; Fina, D.; Jiritano, F.; Meani, P.; Blankesteijn, W.M.; Raffa, G.M.; Kowaleski, M.; Heuts, S.; Beghi, C.; Maessen, J.; et al. Treatment strategies for post-infarction left ventricular free-wall rupture. Eur. Heart J. Acute Cardiovasc. Care 2019, 8, 379–387. [Google Scholar] [CrossRef]
- Yeo, T.C.; Malouf, J.F.; Oh, J.K.; Seward, J.B. Clinical profile and outcome in 52 patients with cardiac pseudoaneurysm. Ann. Intern. Med. 1998, 128, 299–305. [Google Scholar] [CrossRef]
- Meizlish, J.L.; Berger, H.J.; Plankey, M.; Errico, D.; Levy, W.; Zaret, B.L. Functional left ventricular aneurysm formation after acute anterior transmural myocardial infarction. Incidence, natural history, and prognostic implications. N. Engl. J. Med. 1984, 311, 1001–1006. [Google Scholar] [CrossRef]
- Tikiz, H.; Balbay, Y.; Atak, R.; Terzi, T.; Genç, Y.; Kütük, E. The effect of thrombolytic therapy on left ventricular aneurysm formation in acute myocardial infarction: Relationship to successful reperfusion and vessel patency. Clin. Cardiol. 2001, 24, 656–662. [Google Scholar] [CrossRef]
- Konen, E.; Merchant, N.; Gutierrez, C.; Provost, Y.; Mickleborough, L.; Paul, N.S.; Butany, J. True versus False Left Ventricular Aneurysm: Differentiation with MR Imaging—Initial Experience. Radiology 2005, 236, 65–75. [Google Scholar] [CrossRef] [PubMed]
- Tuan, J.; Kaivani, F.; Fewins, H. Left ventricular pseudoaneurysm. Eur. J. Echocardiogr. 2008, 9, 107–109. [Google Scholar] [CrossRef]
- Atik, F.A.; Navia, J.L.; Vega, P.R.; Gonzalez-Stawinski, G.V.; Alster, J.M.; Gillinov, A.M.; Svensson, L.G.; Pettersson, B.G.; Lytle, B.W.; Blackstone, E.H. Surgical treatment of postinfarction left ventricular pseudoaneurysm. Ann. Thorac. Surg. 2007, 83, 526–531. [Google Scholar] [CrossRef] [PubMed]
- Faxon, D.P.; Ryan, T.J.; Davis, K.B.; McCabe, C.H.; Myers, W.; Lesperance, J.; Shaw, R.; Tong, T.G. Prognostic significance of angiographically documented left ventricular aneurysm from the Coronary Artery Surgery Study (CASS). Am. J. Cardiol. 1982, 50, 157–164. [Google Scholar] [CrossRef] [PubMed]
- Authors/Task Force members; Windecker, S.; Kolh, P.; Alfonso, F.; Collet, J.-P.; Cremer, J.; Falk, V.; Filippatos, G.; Hamm, C.; Head, S.J.; et al. 2014 ESC/EACTS Guidelines on myocardial revascularization: The Task Force on Myocardial Revascularization of the European Society of Cardiology (ESC) and the European Association for Cardio-Thoracic Surgery (EACTS)Developed with the special contribution of the European Association of Percutaneous Cardiovascular Interventions (EAPCI). Eur. Heart J. 2014, 35, 2541–2619. [Google Scholar] [CrossRef] [PubMed]
- Hochman, J.S.; Buller, C.E.; Sleeper, L.A.; Boland, J.; Dzavik, V.; Sanborn, T.A.; Godfrey, E.; White, H.D.; Lim, J.; LeJemtel, T. Cardiogenic shock complicating acute myocardial infarction–etiologies, management and outcome: A report from the SHOCK Trial Registry. SHould we emergently revascularize Occluded Coronaries for cardiogenic shocK? J. Am. Coll. Cardiol. 2000, 36, 1063–1070. [Google Scholar] [CrossRef]
- Thiele, H.; Zeymer, U.; Neumann, F.-J.; Ferenc, M.; Olbrich, H.-G.; Hausleiter, J.; Richardt, G.; Hennersdorf, M.; Empen, K.; Fuernau, G.; et al. Intraaortic Balloon Support for Myocardial Infarction with Cardiogenic Shock. N. Engl. J. Med. 2012, 367, 1287–1296. [Google Scholar] [CrossRef]
- Bernhardt, A.M.; Copeland, H.; Deswal, A.; Gluck, J.; Givertz, M.M.; Bernhardt, A.M.; Gluck, J.; Garan, A.R.; Hall, S.; Hayanga, A.; et al. The International Society for Heart and Lung Transplantation/Heart Failure Society of America Guideline on Acute Mechanical Circulatory Support. J. Heart Lung Transplant. 2023, 42, e1–e64. [Google Scholar] [CrossRef]
- Members, A.F.; McDonagh, T.A.; Metra, M.; Adamo, M.; Gardner, R.S.; Baumbach, A.; Böhm, M.; Burri, H.; Butler, J.; Čelutkienė, J.; et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur. J. Heart Fail. 2022, 24, 4–131. [Google Scholar] [CrossRef]
- Thiele, H.; Zeymer, U.; Akin, I.; Behnes, M.; Rassaf, T.; Mahabadi, A.A.; Lehmann, R.; Eitel, I.; Graf, T.; Seidler, T.; et al. Extracorporeal Life Support in Infarct-Related Cardiogenic Shock. N. Engl. J. Med. 2023, 389, 1286–1297. [Google Scholar] [CrossRef] [PubMed]
- Taleb, I.; Koliopoulou, A.G.; Tandar, A.; McKellar, S.H.; Tonna, J.E.; Nativi-Nicolau, J.; Alvarez Villela, M.; Welt, F.; Stehlik, J.; Gilbert, E.M.; et al. Shock Team Approach in Refractory Cardiogenic Shock Requiring Short-Term Mechanical Circulatory Support: A Proof of Concept. Circulation 2019, 140, 98–100. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.H. Mechanical Circulatory Support in Cardiogenic Shock: Shock Team or Bust? Can. J. Cardiol. 2020, 36, 197–204. [Google Scholar] [CrossRef] [PubMed]
- Wilson-Smith, A.R.; Bogdanova, Y.; Roydhouse, S.; Phan, K.; Tian, D.H.; Yan, T.D.; Loforte, A. Outcomes of venoarterial extracorporeal membrane oxygenation for refractory cardiogenic shock: Systematic review and meta-analysis. Ann. Cardiothorac. Surg. 2019, 8, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Delmas, C.; Vandenbriele, C.; Pappalardo, F.; Roubille, F. What about current recommendations for extracorporeal life support in acute myocardial infarction-associated cardiogenic shock: Stay or go? or time to revise? Eur. J. Heart Fail. 2023, 25, 2102–2104. [Google Scholar] [CrossRef]
- O’Rourke, R.A.; Dell’italia, L.J. Diagnosis and management of right ventricular myocardial infarction. Curr. Probl. Cardiol. 2004, 29, 6–47. [Google Scholar] [CrossRef]
- Antman, E.M.; Anbe, D.T.; Armstrong, P.W.; Bates, E.R.; Green, L.A.; Hand, M.; Hochman, J.S.; Krumholz, H.M.; Kushner, F.G.; Lamas, G.A.; et al. ACC/AHA guidelines for the management of patients with ST-elevation myocardial infarction–executive summary: A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise the 1999 Guidelines for the Management of Patients with Acute Myocardial Infarction). Circulation 2004, 110, 588–636. [Google Scholar] [CrossRef]
- Grothoff, M.; Elpert, C.; Hoffmann, J.; Zachrau, J.; Lehmkuhl, L.; de Waha, S.; Desch, S.; Eitel, I.; Mende, M.; Thiele, H.; et al. Right ventricular injury in ST-elevation myocardial infarction: Risk stratification by visualization of wall motion, edema, and delayed-enhancement cardiac magnetic resonance. Circ. Cardiovasc. Imaging 2012, 5, 60–68. [Google Scholar] [CrossRef]
- Hrovatin, E.; Piazza, R.; Pavan, D.; Mimo, R.; Macor, F.; Dall’Aglio, V.; Burelli, C.; Cassin, M.; Canterin, F.A.; Brieda, M.; et al. Dynamic Left Ventricular Outflow Tract Obstruction in the Setting of Acute Anterior Myocardial Infarction: A Serious and Potentially Fatal Complication? Echocardiography 2002, 19, 449–455. [Google Scholar] [CrossRef]
- Dynamic Left Ventricular Outflow Tract Obstruction in Acute Myocardial Infarction with Shock. Available online: https://www.ahajournals.org/doi/epub/10.1161/CIRCULATIONAHA.107.711697 (accessed on 17 November 2023).
- Brown, M.L.; Abel, M.D.; Click, R.L.; Morford, R.G.; Dearani, J.A.; Sundt, T.M.; Orszulak, T.A.; Schaff, H.V. Systolic anterior motion after mitral valve repair: Is surgical intervention necessary? J. Thorac. Cardiovasc. Surg. 2007, 133, 136–143. [Google Scholar] [CrossRef]
- Cohen, R.; Rivagorda, J.; Elhadad, S. Asymmetric septal hypertrophy complicated by dynamic left ventricular obstruction after intra-aortic balloon counterpulsation placement in the setting of anterior myocardial infarction. J. Invasive Cardiol. 2006, 18, E207–E208. [Google Scholar] [PubMed]
- Lee, T.H.; Goldman, L. The Coronary Care Unit Turns 25: Historical Trends and Future Directions. Ann. Intern. Med. 1988, 108, 887–894. [Google Scholar] [CrossRef] [PubMed]
- Huizar, J.F.; Ellenbogen, K.A.; Tan, A.Y.; Kaszala, K. Arrhythmia-Induced Cardiomyopathy: JACC State-of-the-Art Review. J. Am. Coll. Cardiol. 2019, 73, 2328–2344. [Google Scholar] [CrossRef] [PubMed]
- Mayuga, K.A.; Fedorowski, A.; Ricci, F.; Gopinathannair, R.; Dukes, J.W.; Gibbons, C.; Hanna, P.; Sorajja, D.; Chung, M.; Benditt, D.; et al. Sinus Tachycardia: A Multidisciplinary Expert Focused Review. Circ. Arrhythmia Electrophysiol. 2022, 15, e007960. [Google Scholar] [CrossRef] [PubMed]
- Benjamin, E.J.; Wolf, P.A.; D’Agostino, R.B.; Silbershatz, H.; Kannel, W.B.; Levy, D. Impact of atrial fibrillation on the risk of death: The Framingham Heart Study. Circulation 1998, 98, 946–952. [Google Scholar] [CrossRef]
- Kannel, W.B.; Benjamin, E.J. Status of the epidemiology of atrial fibrillation. Med. Clin. N. Am. 2008, 92, 17–40, ix. [Google Scholar] [CrossRef] [PubMed]
- Lavie, C.J.; Gersh, B.J. Acute Myocardial Infarction: Initial Manifestations, Management, and Prognosis. Mayo Clin. Proc. 1990, 65, 531–548. [Google Scholar] [CrossRef]
- 2023 ACC/AHA/ACCP/HRS Guideline for the Diagnosis and Management of Atrial Fibrillation: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines|Journal of the American College of Cardiology. Available online: https://www.jacc.org/doi/abs/10.1016/j.jacc.2023.08.017 (accessed on 12 January 2024).
- Ding, W.Y.; Blomström-Lundqvist, C.; Fauchier, L.; Marin, F.; Potpara, T.S.; Boriani, G.; Lip, G.Y.H.; The ESC-EHRA EORP-AF Long-Term General Registry Investigators. Contemporary management of atrial fibrillation and the predicted vs. absolute risk of ischaemic stroke despite treatment: A report from ESC-EHRA EORP-AF Long-Term General Registry. EP Eur. 2023, 25, 277–282. [Google Scholar] [CrossRef]
- Bhar-Amato, J.; Davies, W.; Agarwal, S. Ventricular Arrhythmia after Acute Myocardial Infarction: ‘The Perfect Storm’. Arrhythm. Electrophysiol. Rev. 2017, 6, 134–139. [Google Scholar] [CrossRef]
- Mont, L.; Cinca, J.; Blanch, P.; Blanco, J.; Figueras, J.; Brotons, C.; Soler-Soler, J. Predisposing Factors and Prognostic Value of Sustained Monomorphic Ventricular Tachycardia in the Early Phase of Acute Myocardial Infarction. J. Am. Coll. Cardiol. 1996, 28, 1670–1676. [Google Scholar] [CrossRef]
- Zwerling, H.K. Does exogenous magnesium suppress myocardial irritability and tachyarrhythmias in the nondigitalized patient? Am. Heart J. 1987, 113, 1046–1053. [Google Scholar] [CrossRef] [PubMed]
- Al-Khatib, S.M.; Stevenson, W.G.; Ackerman, M.J.; Bryant, W.J.; Callans, D.J.; Curtis, A.B.; Deal, B.J.; Dickfeld, T.; Field, M.E.; Fonarow, G.C.; et al. 2017 AHA/ACC/HRS Guideline for Management of Patients with Ventricular Arrhythmias and the Prevention of Sudden Cardiac Death. Circulation 2018, 138, e272–e391. [Google Scholar] [CrossRef]
- Kusumoto, F.M.; Calkins, H.; Boehmer, J.; Buxton, A.E.; Chung, M.K.; Gold, M.R.; Hohnloser, S.H.; Indik, J.; Lee, R.; Mehra, M.R.; et al. HRS/ACC/AHA Expert Consensus Statement on the Use of Implantable Cardioverter-Defibrillator Therapy in Patients Who Are Not Included or Not Well Represented in Clinical Trials. Circulation 2014, 130, 94–125. [Google Scholar] [CrossRef] [PubMed]
- Meine, T.J.; Al-Khatib, S.M.; Alexander, J.H.; Granger, C.B.; White, H.D.; Kilaru, R.; Williams, K.; Ohman, E.M.; Topol, E.; Califf, R.M. Incidence, predictors, and outcomes of high-degree atrioventricular block complicating acute myocardial infarction treated with thrombolytic therapy. Am. Heart J. 2005, 149, 670–674. [Google Scholar] [CrossRef] [PubMed]
- Onodera, S.; Ito, M.; Odakura, H.; Yagi, T.; Namekawa, A.; Sato, T.; Nagashima, M.; Shinoda, S.; Suzuki, H. Atrioventricular block in acute inferior myocardial infarction. Kokyu Junkan 1992, 40, 255–260. [Google Scholar]
- Alnsasra, H.; Ben-Avraham, B.; Gottlieb, S.; Ben-avraham, M.; Kronowski, R.; Iakobishvili, Z.; Goldenberg, I.; Strasberg, B.; Haim, M. High-grade atrioventricular block in patients with acute myocardial infarction. Insights from a contemporary multi-center survey. J. Electrocardiol. 2018, 51, 386–391. [Google Scholar] [CrossRef]
- Harikrishnan, P.; Gupta, T.; Palaniswamy, C.; Kolte, D.; Khera, S.; Mujib, M.; Aronow, W.S.; Ahn, C.; Sule, S.; Jain, D.; et al. Complete Heart Block Complicating ST-Segment Elevation Myocardial Infarction. JACC Clin. Electrophysiol. 2015, 1, 529–538. [Google Scholar] [CrossRef]
- Hauer, R.N.W.; Lie, K.I.; Liem, K.L.; Durrer, D. Long-term prognosis in patients with bundle branch block complicating acute anteroseptal infarction. Am. J. Cardiol. 1982, 49, 1581–1585. [Google Scholar] [CrossRef]
- Scheinman, M.M.; Thorburn, D.; Abbott, J.A. Use of atropine in patients with acute myocardial infarction and sinus bradycardia. Circulation 1975, 52, 627–633. [Google Scholar] [CrossRef]
- Brady, W.J.; Swart, G.; DeBehnke, D.J.; Ma, O.J.; Aufderheide, T.P. The efficacy of atropine in the treatment of hemodynamically unstable bradycardia and atrioventricular block: Prehospital and emergency department considerations. Resuscitation 1999, 41, 47–55. [Google Scholar] [CrossRef]
- Yaqub, Y.; Perez-Verdia, A.; Jenkins, L.A.; Sehli, S.; Paige, R.L.; Nugent, K.M. Temporary Transvenous Cardiac Pacing in Patients with Acute Myocardial Infarction Predicts Increased Mortality. Cardiol. Res. 2012, 3, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Kusumoto, F.M.; Schoenfeld, M.H.; Barrett, C.; Edgerton, J.R.; Ellenbogen, K.A.; Gold, M.R.; Goldschlager, N.F.; Hamilton, R.M.; Joglar, J.A.; Kim, R.J.; et al. 2018 ACC/AHA/HRS Guideline on the Evaluation and Management of Patients with Bradycardia and Cardiac Conduction Delay: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society. Circulation 2019, 140, e382–e482. [Google Scholar] [CrossRef] [PubMed]
- Waltenberger, J.; Gelissen, M.; Bekkers, S.C.; Vainer, J.; van Ommen, V.; Eerens, F.; Ruiters, A.; Holthuijsen, A.; Cuesta, P.; Strauven, R.; et al. Clinical Pacing Post-Conditioning During Revascularization After AMI. JACC Cardiovasc. Imaging 2014, 7, 620–626. [Google Scholar] [CrossRef] [PubMed]
- Fioretti, P.; Brower, R.W.; Balakumaran, K. Early Post-Infarction Angina. Incidence and Prognostic Relevance. Eur. Heart J. 1986, 7, 73–77. [Google Scholar] [CrossRef] [PubMed]
- Hutchins, G.M.; Bulkley, B.H. Infarct expansion versus extension: Two different complications of acute myocardial infarction. Am. J. Cardiol. 1978, 41, 1127–1132. [Google Scholar] [CrossRef]
- Reid, P.R.; Taylor, D.R.; Kelly, D.T.; Weisfeldt, M.L.; Humphries, J.O.; Ross, R.S.; Pitt, B. Myocardial-infarct extension detected by precordial ST-segment mapping. N. Engl. J. Med. 1974, 290, 123–128. [Google Scholar] [CrossRef] [PubMed]
- Williams, D.B.; Ivey, T.D.; Bailey, W.W.; Irey, S.J.; Rideout, J.T.; Stewart, D. Postinfarction angina: Results of early revascularization. J. Am. Coll. Cardiol. 1983, 2, 859–864. [Google Scholar] [CrossRef]
- Dorfman, T.A.; Aqel, R. Regional Pericarditis: A Review of the Pericardial Manifestations of Acute Myocardial Infarction. Clin. Cardiol. 2009, 32, 115–120. [Google Scholar] [CrossRef]
- Tofler, G.H.; Muller, J.E.; Stone, P.H.; Willich, S.N.; Davis, V.G.; Poole, W.K.; Robertson, T.; Braunwald, E. Pericarditis in acute myocardial infarction: Characterization and clinical significance. Am. Heart J. 1989, 117, 86–92. [Google Scholar] [CrossRef]
- Indik, J.H.; Alpert, J.S. Post-myocardial infarction pericarditis. Curr. Treat. Options Cardio Med. 2000, 2, 351–355. [Google Scholar] [CrossRef]
- Verma, B.R.; Montane, B.; Chetrit, M.; Khayata, M.; Furqan, M.M.; Ayoub, C.; Klein, A.L. Pericarditis and Post-cardiac Injury Syndrome as a Sequelae of Acute Myocardial Infarction. Curr. Cardiol. Rep. 2020, 22, 127. [Google Scholar] [CrossRef] [PubMed]
- Doulaptsis, C.; Goetschalckx, K.; Masci, P.G.; Florian, A.; Janssens, S.; Bogaert, J. Assessment of Early Post-Infarction Pericardial Injury by CMR. JACC Cardiovasc. Imaging 2013, 6, 411–413. [Google Scholar] [CrossRef]
- Hirsh, J.; Fuster, V.; Ansell, J.; Halperin, J.L. American Heart Association/American College of Cardiology Foundation Guide to Warfarin Therapy. Circulation 2003, 107, 1692–1711. [Google Scholar] [CrossRef] [PubMed]
- Asinger, R.W.; Mikell, F.L.; Elsperger, J.; Hodges, M. Incidence of Left-Ventricular Thrombosis after Acute Transmural Myocardial Infarction. N. Engl. J. Med. 1981, 305, 297–302. [Google Scholar] [CrossRef]
- Jugdutt, B.I.; Sivaram, C.A.; Wortman, C.; Trudell, C.; Penner, P. Prospective two-dimensional echocardiographic evaluation of left ventricular thrombus and embolism after acute myocardial infarction. J. Am. Coll. Cardiol. 1989, 13, 554–564. [Google Scholar] [CrossRef] [PubMed]
- Glueck, H.I.; Ryder, H.W.; Wasserman, P. The Prevention of Thromboembolic Complications in Myocardial Infarction by Anticoagulant Therapy. Circulation 1956, 13, 884–895. [Google Scholar] [CrossRef] [PubMed]
- Lattuca, B.; Bouziri, N.; Kerneis, M.; Portal, J.-J.; Zhou, J.; Hauguel-Moreau, M.; Mameri, A.; Zeitouni, M.; Guedeney, P.; Hammoudi, N.; et al. Antithrombotic Therapy for Patients with Left Ventricular Mural Thrombus. J. Am. Coll. Cardiol. 2020, 75, 1676–1685. [Google Scholar] [CrossRef]
- Chen, M.; Liu, D.; Weidemann, F.; Lengenfelder, B.D.; Ertl, G.; Hu, K.; Frantz, S.; Nordbeck, P. Echocardiographic risk factors of left ventricular thrombus in patients with acute anterior myocardial infarction. ESC Heart Fail. 2021, 8, 5248–5258. [Google Scholar] [CrossRef]
- Shibata, T.; Kawakami, S.; Noguchi, T.; Tanaka, T.; Asaumi, Y.; Kanaya, T.; Nagai, T.; Nakao, K.; Fujino, M.; Nagatsuka, K.; et al. Prevalence, Clinical Features, and Prognosis of Acute Myocardial Infarction Attributable to Coronary Artery Embolism. Circulation 2015, 132, 241–250. [Google Scholar] [CrossRef]
- Delewi, R.; Zijlstra, F.; Piek, J.J. Left ventricular thrombus formation after acute myocardial infarction. Heart 2012, 98, 1743–1749. [Google Scholar] [CrossRef]


{kind=link}
| Complication | Presentation | Diagnosis | Management |
|---|---|---|---|
| Mechanical Complications | |||
| Papillary Muscle Rupture Ischemic Mitral Regurgitation | Typically, 7 days post-MI. Most common clinical presentation: acute pulmonary edema. Most commonly involved territory: RCA. | CXR: acute pulmonary edema. TTE, TEE: ruptured papillary muscle, flail leaflets, and regurgitant jet. | Management of acute pulmonary edema. Surgical intervention: mitral valve replacement. |
| Ventricular Septal Rupture | Heightened risk in the initial 24 h. Secondary peak at 3 to 5 days. Symptoms: chest pain, dyspnea, and signs of cardiogenic shock. | TTE, TEE: presence, location, and size of the rupture. Coronary angiogram: confirm VSR suspicion via left ventriculogram. | Medical therapy: inotropes/diuretics. Unstable patients: IABP/ECMO. Surgical intervention: trimming and suturing the infarcted myocardium using a larger patch. Percutaneous techniques: for high-risk surgery patients, guided by TEE and fluoroscopy. |
| Free Wall Rupture | Type 1: Sudden tear within 24 h. Type 2: gradual tear with localized erosion. Type 3: perforation of a thin-walled aneurysm after 7 days. Symptoms: chest pain, restlessness, hemodynamic instability, and cardiac tamponade. | TTE: pericardial effusion, tamponade physiology, or hemopericardium. | Addressing acute tamponade: pericardiocentesis. If hypotensive: IABP/ECMO. Definitive: surgical management. |
| True and Pseudoaneurysms | Usually within 2 weeks post-MI. Pseudoaneurysm symptoms: chest pain, dyspnea, or cardiac tamponade. True aneurysms manifest as angina, heart failure, ventricular tachycardia, or a visible apical impulse. | TTE: pseudoaneurysms show narrow neck and posterior/lateral location and true aneurysms seen as wider neck and anterior/apical location. Cardiac CT or MRI. | Pseudoaneurysm: surgical direct closure. True aneurysms: anticoagulation Large aneurysm: surgical resection during CABG. |
| LV Failure and Cardiogenic Shock | Symptoms: new chest pain, a cold and wet physiological state, hypotension, tachycardia, dyspnea, jugular venous distension, rales, and the emergence of a new murmur. | TTE: cardiac function, structural abnormalities. PAC. | Medical: diuretics. Refractory shock: IABP/Impella/ECMO. |
| Right Ventricular Myocardial Infarction | Symptoms: hypotension, elevated jugular venous pressure, clear lung fields, indications of inferior wall infarction. | ECG: ST-elevation in lead V4R. Angiogram: blockage of the proximal right coronary artery. | STEMI management: DAPT, statin, anticoagulation, primary PCI. |
| Dynamic Left Ventricular Outflow Tract Obstruction | Historically associated with hypertrophic obstructive cardiomyopathy. Other symptoms: hemodynamic instability, potential STEMI, and signs such as sustained apical heave and an ejection murmur. | TTE. | Intravenous fluids. Coronary revascularization. Inotropic agents. BB, CCB. Phenylephrine, IABP. |
| Electrical Complications | |||
| Atrial Tachyarrhythmia | AFib and Aflutter are common. | ECG. | Rate control: BB. Unstable: cardioversion. Anticoagulation. |
| Ventricular Tachyarrhythmia | NSVT—tolerable. VT, VFib—significant short-term and long-term mortality risks. | Unstable Vt/VFib: rapid unsynchronized electrical countershock. Electrolyte replenishment. Recurrent or refractory ventricular tachycardia: CD. | |
| Bradyarrhythmia | Commonly seen in infer posterior wall MI. | ECG: sinus bradycardia and AV blocks. | 1st degree AVB: no intervention. 2nd degree AVB: atropine for symptomatic patients. Complete AVB: temporary pacing, PPM. |
| Ischemic Complications | |||
| Post-infarction Angina | Suspicion of recurrent infarction within the initial 18 to 24 h post-AMI. Symptoms: chest pain, congestive heart failure, hypotension. | ECG: ST-T wave changes, new Q waves. Lab: cardiac biomarker elevation. | Urgent PCI. If PCI unavailable—fibrinolysis can be considered. Medical: BB, nitroglycerine. |
| Pericardial Complications | |||
| Post-infarction Pericarditis | Early infarct-associated pericarditis: initial 4 days after AMI. Dressler syndrome/late pericarditis: 1–2 weeks post-AMI. Symptoms: pleuritic chest pain, pericardial friction rub. | ECG: upright T waves and new-onset positive T waves. Lab: troponin, inflammatory markers. | Early post-infarction pericarditis: aspirin every 8–12 h. Late pericarditis: aspirin until symptomatic improvement. |
| Thromboembolic Complications | |||
| Systemic Embolism and LV thrombus | Most frequently within the initial 10 days post-AMI. Signs: strokes, limb ischemia, renal infarction, and mesenteric ischemia | TTE. Cardiac MRI. | Anticoagulation. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Moras, E.; Yakkali, S.; Gandhi, K.D.; Virk, H.U.H.; Alam, M.; Zaid, S.; Barman, N.; Jneid, H.; Vallabhajosyula, S.; Sharma, S.K.; et al. Complications in Acute Myocardial Infarction: Navigating Challenges in Diagnosis and Management. Hearts 2024, 5, 122-141. https://doi.org/10.3390/hearts5010009
Moras E, Yakkali S, Gandhi KD, Virk HUH, Alam M, Zaid S, Barman N, Jneid H, Vallabhajosyula S, Sharma SK, et al. Complications in Acute Myocardial Infarction: Navigating Challenges in Diagnosis and Management. Hearts. 2024; 5(1):122-141. https://doi.org/10.3390/hearts5010009
Chicago/Turabian StyleMoras, Errol, Shreyas Yakkali, Kruti D. Gandhi, Hafeez Ul Hassan Virk, Mahboob Alam, Syed Zaid, Nitin Barman, Hani Jneid, Saraschandra Vallabhajosyula, Samin K. Sharma, and et al. 2024. "Complications in Acute Myocardial Infarction: Navigating Challenges in Diagnosis and Management" Hearts 5, no. 1: 122-141. https://doi.org/10.3390/hearts5010009