Immunological and microRNA Features of Allergic Rhinitis in the Context of United Airway Disease



{kind=link}
Abstract
:1. Introduction
2. Allergic Rhinitis in the Continuum of Airway Inflammation
3. Upper Airway Cough Syndrome
4. Immune Cells Involved in United Airway Inflammation
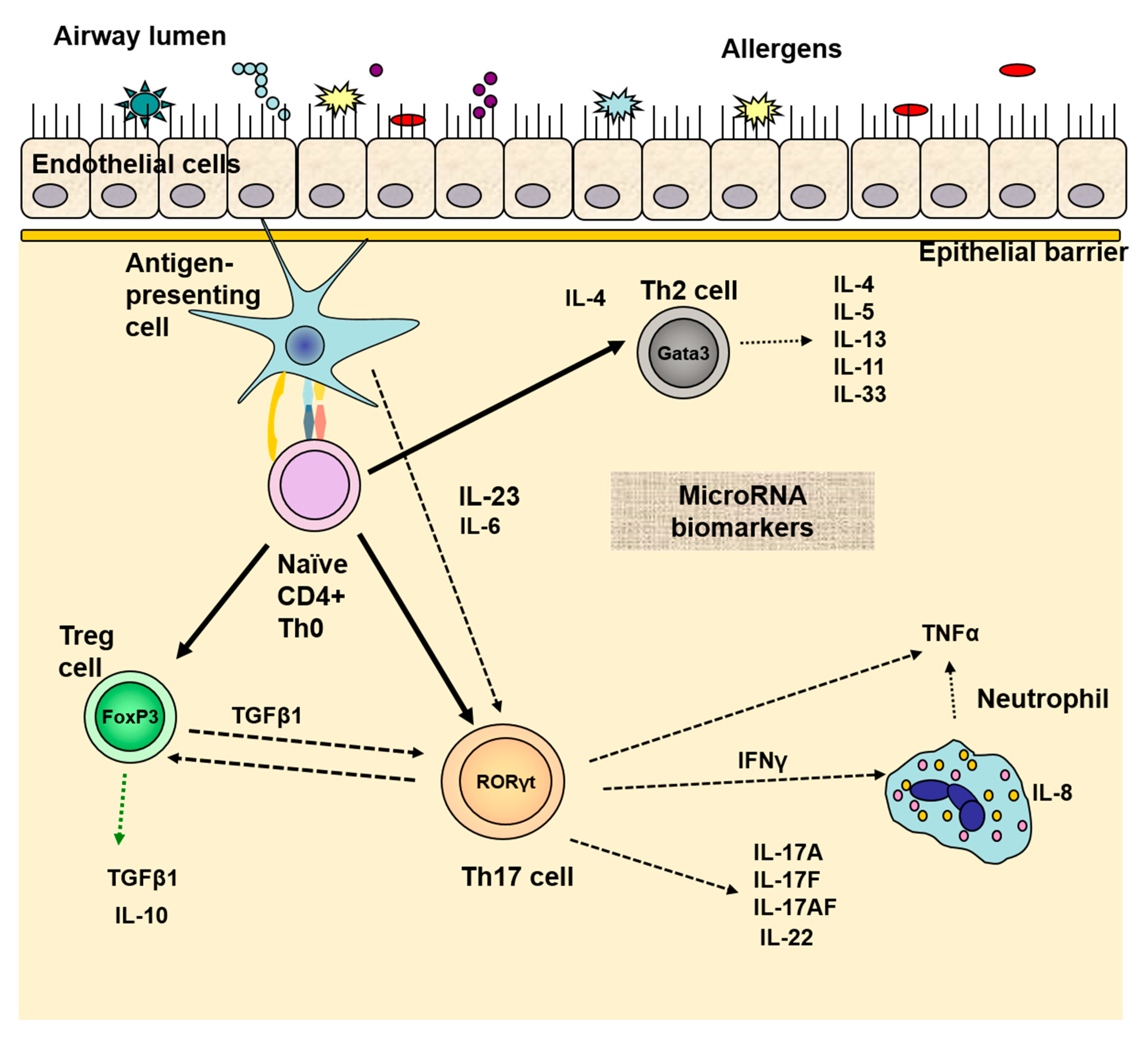
5. Th17 Cells Role in the Common Inflammation of the Airways
6. Diagnostic and Therapeutic Approaches in the Light of the United Airway Pathway
6.1. microRNAs as a Promising Tool in United Airway Disease Diagnosis
6.2. Biological Therapy in the Focus of United Airway Disease
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Caimmi, D.; Marseglia, A.; Pieri, G.; Benzo, S.; Bosa, L.; Caimmi, S. Nose and lungs: One way, one disease. Ital. J. Pediatr. 2012, 38, 60. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Licari, A.; Castagnoli, R.; Denicolò, C.F.; Rossini, L.; Marseglia, A.; Marseglia, G.L. The Nose and the Lung: United Airway Disease? Front. Pediatr. 2017, 5, 44. [Google Scholar] [CrossRef] [Green Version]
- Haccuria, A.; van Muylem, A.; Malinovschi, A.; Doan, V.; Michils, A. Small airways dysfunction: The link between allergic rhinitis and allergic asthma. Eur. Respir. J. 2018, 51, 1701749. [Google Scholar] [CrossRef] [Green Version]
- Compalati, E.; Ridolo, E.; Passalacqua, G.; Braido, F.; Villa, E.; Canonica, G.W. The link between allergic rhinitis and asthma: The united airways disease. Expert Rev. Clin. Immunol. 2010, 6, 413–423. [Google Scholar] [CrossRef]
- Vujnovic, S.D.; Domuz, A. Epidemiological Aspects of Rhinitis and Asthma: Comorbidity or United Airway Disease. In Asthma Diagnosis and Management—Approach Based on Phenotype and Endotype; IntechOpen: London, UK, 2018. [Google Scholar]
- Bousquet, J.; Boushey, H.A.; Busse, W.W.; Canonica, G.W.; Durham, S.R.; Irvin, C.G.; Karpel, J.P.; van Cauwenberge, P.; Chen, R.; Iezzoni, D.G.; et al. Characteristics of patients with seasonal allergic rhinitis and concomitant asthma. Clin. Exp. Allergy 2004, 34, 897–903. [Google Scholar] [CrossRef]
- Small, P.; Keith, P.K.; Kim, H. Allergic rhinitis. Allergy Asthma Clin. Immunol. 2018, 14, 1–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mileva, Z.; Popov, T.; Staneva, M.; Dimitrov, V.; Mateev, V.; Slavov, S. Frequency and characteristics of allergic diseases in Bulgaria. Allergy Asthma 2000, 1, 3–32. [Google Scholar]
- Pawankar, R.; Bunnag, C.; Khaltaev, N.; Bousquet, J. Allergic Rhinitis and Its Impact on Asthma in Asia Pacific and the ARIA Update 2008. World Allergy Organ. J. 2012, 5, S212–S217. [Google Scholar] [CrossRef] [Green Version]
- Dykewicz, M.S. 7. Rhinitis and sinusitis. J. Allergy Clin. Immunol. 2003, 111, S520–S529. [Google Scholar] [CrossRef] [PubMed]
- Bousquet, P.; Schünemann, H.; Samolinski, B.; Demoly, P.; Baena-Cagnani, C.; Bachert, C.; Bonini, S.; Boulet, L.; Brozek, J.; Canonica, G.; et al. Allergic Rhinitis and its Impact on Asthma (ARIA): Achievements in 10 years and future needs. J. Allergy Clin. Immunol. 2012, 130, 1049–1062. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bugten, V.; Nordgård, S.; Romundstad, P.; Steinsvåg, S. Chronic rhinosinusitis and nasal polyposis; indicia of heterogeneity. Rhinol. J. 2008, 46, 40–44. [Google Scholar]
- Ediger, D.; Sin, B.A.; Heper, A.; Anadolu, Y.; Mitoasitoarlitoagil, Z. Airway inflammation in nasal polyposis: Immunopathological aspects of relation to asthma. Clin. Exp. Allergy 2005, 35, 319–326. [Google Scholar] [CrossRef]
- Bousquet, J.; van Cauwenberge, P.; Khaltaev, N. Allergic Rhinitis and Its Impact on Asthma. J. Allergy Clin. Immunol. 2001, 108, S147–S334. [Google Scholar] [CrossRef] [Green Version]
- Millqvist, E.; Bende, M. Role of the upper airways in patients with chronic cough. Curr. Opin. Allergy Clin. Immunol. 2006, 6, 7–11. [Google Scholar] [CrossRef] [PubMed]
- Kogahara, T.; Kanai, K.-I.; Asano, K.; Suzaki, H. Evidence for passing down of postnasal drip into respiratory organs. Vivo 2009, 23, 297–302. [Google Scholar]
- Pratter, M.R. Chronic Upper Airway Cough Syndrome Secondary to Rhinosinus Diseases (Previously Referred to as Postnasal Drip Syndrome). Chest 2006, 129, 63S–71S. [Google Scholar] [CrossRef]
- Forer, M.; Ananda, S. The management of postnasal drip. Aust. Fam. Physician 1999, 28, 223–228. [Google Scholar] [PubMed]
- Meltzer, E.O.; Szwarcberg, J.; Pill, M.W. Allergic Rhinitis, Asthma, and Rhinosinusitis: Diseases of the Integrated Airway. J. Manag. Care Pharm. 2004, 10, 310–317. [Google Scholar] [CrossRef]
- Morice, A.H. The diagnosis and management of chronic cough. Eur. Respir. J. 2004, 24, 481–492. [Google Scholar] [CrossRef] [PubMed]
- Lai, K.; Chen, R.; Lin, J.; Huang, K.; Shen, H.; Kong, L.; Zhou, X.; Luo, Z.; Yang, L.; Wen, F.; et al. A Prospective, Multicenter Survey on Causes of Chronic Cough in China. Chest 2013, 143, 613–620. [Google Scholar] [CrossRef]
- Pecova, R.; Zucha, J.; Pec, M.; Neuschlova, M.; Hanzel, P.; Tatar, M. Cough reflex sensitivity testing in in seasonal allergic rhinitis patients and healthy volunteers. J. Physiol. Pharmacol. 2008, 59, 557–564. [Google Scholar] [PubMed]
- Weinfeld, D.; Ternesten-Hasséus, E.; Löwhagen, O.; Millqvist, E. Capsaicin cough sensitivity in allergic asthmatic patients increases during the birch pollen season. Ann. Allergy Asthma Immunol. 2002, 89, 419–424. [Google Scholar] [CrossRef]
- Lim, K.G.; Rank, M.A.; Kita, H.; Patel, A.; Moore, E. Neuropeptide levels in nasal secretions from patients with and without chronic cough. Ann. Allergy Asthma Immunol. 2011, 107, 360–363. [Google Scholar] [CrossRef] [PubMed]
- Romagnani, S. T-cell subsets (Th1 versus Th2). Ann. Allergy Asthma Immunol. 2000, 85, 9–21. [Google Scholar] [CrossRef]
- Rajan, T. The Gell—Coombs classification of hypersensitivity reactions: A re-interpretation. Trends Immunol. 2003, 24, 376–379. [Google Scholar] [CrossRef]
- Janeway, C.A., Jr.; Travers, P.; Walport, M.; Shlomchik, M.J. Immunobiology: The Immune System in Health and Disease, 5th ed.; Garland Science: New York, NY, USA, 2001. [Google Scholar]
- Larsen, K. The Clinical Relationship of Nasal Polyps to Asthma. Allergy Asthma Proc. 1996, 17, 243–249. [Google Scholar] [CrossRef]
- Muluk, N.B. The united airway disease. Rom. J. Rhinol. 2019, 9, 21–26. [Google Scholar] [CrossRef] [Green Version]
- Ketenci, A.; Kalyoncu, A.F.; del Giacco, S. Upper and Lower Airways Interaction: Is the United Airway Disease Concept a Reflection of Reality? How Important Is It? In Challenges in Rhinology; Cingi, C., Muluk, N.B., Scadding, G.K., Mladina, R., Eds.; Springer International Publishing: Cham, Switzerland, 2020; pp. 405–414. [Google Scholar]
- Gu, Z.W.; Wang, Y.X.; Cao, Z.W. Neutralization of interleukin-17 suppresses allergic rhinitis symptoms by downregulating Th2 and Th17 responses and upregulating the Treg response. Oncotarget 2017, 8, 22361–22369. [Google Scholar] [CrossRef] [Green Version]
- Ciprandi, G.; de Amici, M.; Murdaca, G.; Fenoglio, D.; Ricciardolo, F.L.M.; Marseglia, G.L.; Tosca, M. Serum interleukin-17 levels are related to clinical severity in allergic rhinitis. Allergy 2009, 64, 1375–1378. [Google Scholar] [CrossRef] [PubMed]
- Huang, X.; Chen, Y.; Zhang, F.; Yang, Q.; Zhang, G. Peripheral Th17/Treg cell-mediated immunity imbalance in allergic rhinitis patients. Braz. J. Otorhinolaryngol. 2014, 80, 152–155. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ferretti, E.; di Carlo, E.; Ognio, E.; Guarnotta, C.; Bertoni, F.; Corcione, A.; Prigione, I.; Fraternali-Orcioni, G.; Ribatti, D.; Ravetti, J.L.; et al. Interleukin-17A promotes the growth of human germinal center derived non-Hodgkin B cell lymphoma. OncoImmunology 2015, 4, e1030560. [Google Scholar] [CrossRef]
- Haenuki, Y.; Matsushita, K.; Futatsugi-Yumikura, S.; Ishii, K.J.; Kawagoe, T.; Imoto, Y.; Fujieda, S.; Yasuda, M.; Hisa, Y.; Akira, S.; et al. A critical role of IL-33 in experimental allergic rhinitis. J. Allergy Clin. Immunol. 2012, 130, 184–194.e11. [Google Scholar] [CrossRef] [PubMed]
- Vocca, L.; di Sano, C.; Uasuf, C.G.; Sala, A.; Riccobono, L.; Gangemi, S.; Albano, G.D.; Bonanno, A.; Gagliardo, R.; Profita, M. IL-33/ST2 axis controls Th2/IL-31 and Th17 immune response in allergic airway diseases. Immunobiology 2015, 220, 954–963. [Google Scholar] [CrossRef]
- Ding, W.; Zou, G.-L.; Zhang, W.; Lai, X.-N.; Chen, H.-W.; Xiong, L.-X. Interleukin-33: Its Emerging Role in Allergic Diseases. Molecules 2018, 23, 1665. [Google Scholar] [CrossRef] [Green Version]
- Lloyd, C.M. IL-33 family members and asthma—Bridging innate and adaptive immune responses. Curr. Opin. Immunol. 2010, 22, 800–806. [Google Scholar] [CrossRef] [Green Version]
- Glück, J.; Rymarczyk, B.; Rogala, B. Serum IL-33 but not ST2 level is elevated in intermittent allergic rhinitis and is a marker of the disease severity. Inflamm. Res. 2012, 61, 547–550. [Google Scholar] [CrossRef] [Green Version]
- Degirmenci, P.B.; Aksun, S.; Altin, Z.; Bilgir, F.; Arslan, I.B.; Çolak, H.; Ural, B.; Kahraman, D.S.; Diniz, G.; Ozdemir, B.; et al. Allergic Rhinitis and Its Relationship with IL-10, IL-17, TGF-β, IFN-γ, IL 22, and IL-35. Dis. Markers 2018, 2018, 1–6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, Z.; Zhang, X.-H.; Callejas-Díaz, B.; Mullol, J. MicroRNA in United Airway Diseases. Int. J. Mol. Sci. 2016, 17, 716. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Panganiban, R.P.; Wang, Y.; Howrylak, J.; Chinchilli, V.M.; Craig, T.J.; August, A.; Ishmael, F.T. Circulating microRNAs as biomarkers in patients with allergic rhinitis and asthma. J. Allergy Clin. Immunol. 2016, 137, 1423–1432. [Google Scholar] [CrossRef] [Green Version]
- Suojalehto, H.; Lindström, I.; Majuri, M.-L.; Mitts, C.; Karjalainen, J.; Wolff, H.; Alenius, H. Altered MicroRNA Expression of Nasal Mucosa in Long-Term Asthma and Allergic Rhinitis. Int. Arch. Allergy Immunol. 2014, 163, 168–178. [Google Scholar] [CrossRef]
- Naydenova, K.; Velikova, T.; Dimitrov, V. Interactions of allergic rhinitis and bronchial asthma at mucosal immunology level. AIMS Allergy Immunol. 2019, 3, 1–12. [Google Scholar] [CrossRef]
- Naydenova, K.; Velikova, T.V.; Dimitrov, V. Chapter 5. Allergic Rhinitis, IL-17 and the Concept of a Common Respiratory Pathway. In Th17 Cells in Health and Disease; Nova Publishing: New York, NY, USA, 2020. [Google Scholar]
- Naydenova, K.; Velikova, T.V.; Dimitrov, V. Mucosal Inflammation in Allergic Rhinitis and Bronchial Asthma—Two Sides of a Coin. Clin. Res. Immunol. 2018, 1, 1–2. [Google Scholar]
- Gevaert, P.; Calus, L.; van Zele, T.; Blomme, K.; de Ruyck, N.; Bauters, W.; Hellings, P.; Brusselle, G.; de Bacquer, D.; van Cauwenberge, P.; et al. Omalizumab is effective in allergic and nonallergic patients with nasal polyps and asthma. J. Allergy Clin. Immunol. 2013, 131, 110–116.e1. [Google Scholar] [CrossRef] [PubMed]
- Pavord, I.D.; Korn, S.; Howarth, P.; Bleecker, E.R.; Buhl, R.; Keene, O.N.; Ortega, H.; Chanez, P. Mepolizumab for severe eosinophilic asthma (DREAM): A multicentre, double-blind, placebo-controlled trial. Lancet 2012, 380, 651–659. [Google Scholar] [CrossRef]
- Gevaert, P.; van Bruaene, N.; Cattaert, T.; van Steen, K.; van Zele, T.; Acke, F.; de Ruyck, N.; Blomme, K.; Sousa, A.R.; Marshall, R.P.; et al. Mepolizumab, a humanized anti–IL-5 mAb, as a treatment option for severe nasal polyposis. J. Allergy Clin. Immunol. 2011, 128, 989–995.e8. [Google Scholar] [CrossRef] [Green Version]
- Giavina-Bianchi, P.; Aun, M.V.; Takejima, P.; Kalil, J.; Agondi, R.C. United airway disease: Current perspectives. J. Asthma Allergy 2016, 9, 93–100. [Google Scholar] [CrossRef] [PubMed] [Green Version]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Naydenova, K.; Dimitrov, V.; Velikova, T. Immunological and microRNA Features of Allergic Rhinitis in the Context of United Airway Disease. Sinusitis 2021, 5, 45-52. https://doi.org/10.3390/sinusitis5010005
Naydenova K, Dimitrov V, Velikova T. Immunological and microRNA Features of Allergic Rhinitis in the Context of United Airway Disease. Sinusitis. 2021; 5(1):45-52. https://doi.org/10.3390/sinusitis5010005
Chicago/Turabian StyleNaydenova, Kremena, Vasil Dimitrov, and Tsvetelina Velikova. 2021. "Immunological and microRNA Features of Allergic Rhinitis in the Context of United Airway Disease" Sinusitis 5, no. 1: 45-52. https://doi.org/10.3390/sinusitis5010005