
Influence of Placement of Ultrashort Implant at Sub-Crestal, Crestal and Supra-Crestal Level with Titanium or Polyetheretherketone Hybrid Abutment: 3D Finite Element Analysis

 ,
, 
 and
and 
Abstract
:1. Introduction
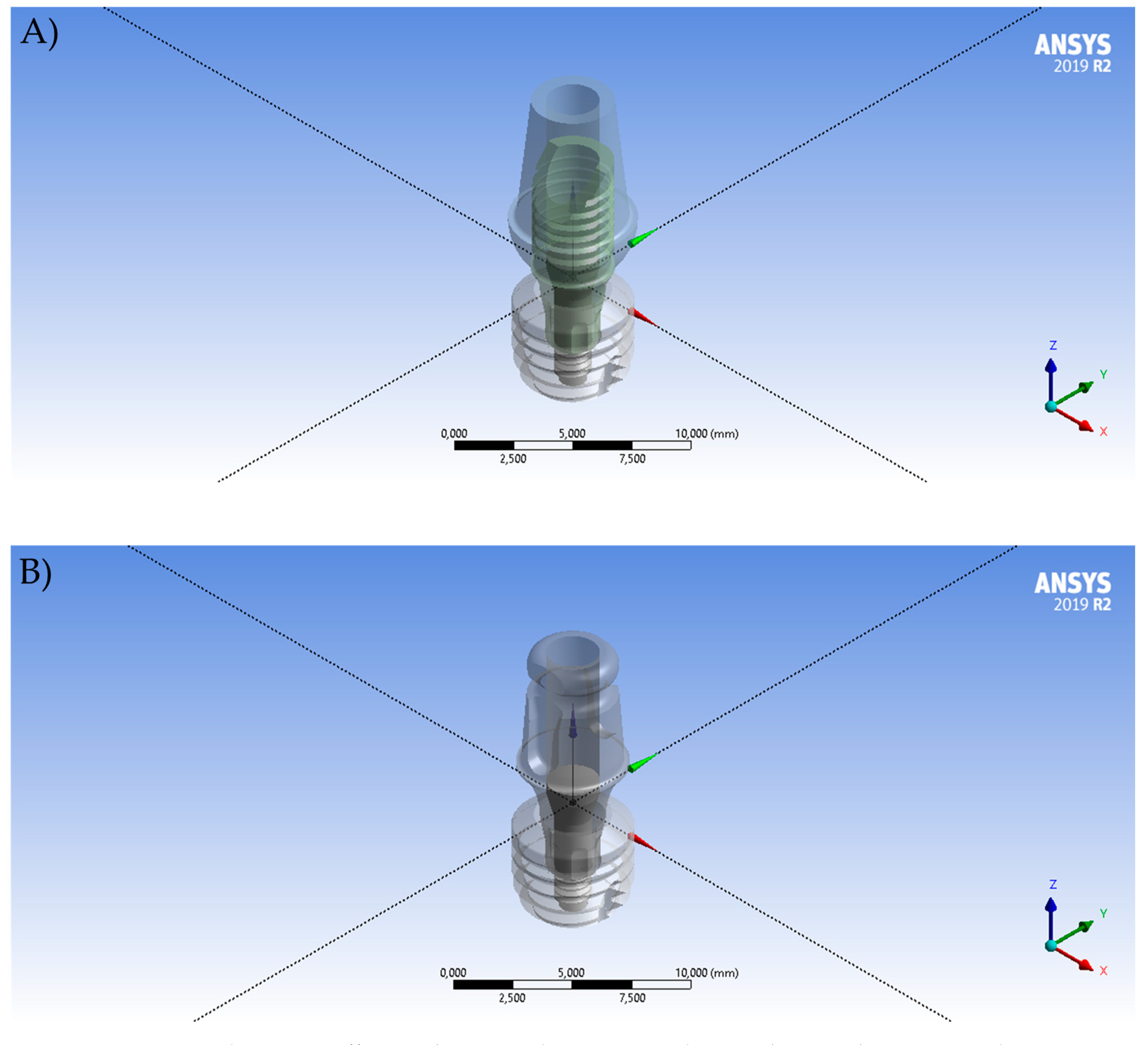
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Morand, M.; Irinakis, T. The Challenge of Implant Therapy in the Posterior Maxilla: Providing a Rationale for the Use of Short Implants. J. Oral Implant. 2007, 33, 257–266. [Google Scholar] [CrossRef]
- Lombardo, G.; Pighi, J.; Marincola, M.; Corrocher, G.; Simancas-Pallares, M.; Nocini, P.F. Cumulative Success Rate of Short and Ultrashort Implants Supporting Single Crowns in the Posterior Maxilla: A 3-Year Retrospective Study. Int. J. Dent. 2017, 2017, 8434281. [Google Scholar] [CrossRef] [Green Version]
- Magdy, M.; Msc, M.A.A.; Alloush, S.; El-Sayed, K.M.F.; Nawwar, A.A.; Shoeib, M.; ElNahass, H.; Msc, M.M.; Msc, S.A. Ultra-short versus standard-length dental implants in conjunction with osteotome-mediated sinus floor elevation: A randomized controlled clinical trial. Clin. Implant. Dent. Relat. Res. 2021, 23, 520–529. [Google Scholar] [CrossRef] [PubMed]
- Heboyan, A.; Giudice, R.L.; Kalman, L.; Zafar, M.S.; Tribst, J.P.M. Stress Distribution Pattern in Zygomatic Implants Supporting Different Superstructure Materials. Materials 2022, 15, 4953. [Google Scholar] [CrossRef]
- Pera, F.; Pesce, P.; Menini, M.; Fanelli, F.; Kim, B.-C.; Zhurakivska, K.; Mayer, Y.; Isola, G.; Cianciotta, G.; Crupi, A.; et al. Immediate loading full-arch rehabilitation using transmucosal tissue-level implants with different variables associated: A one-year observational study. Minerva Dent. Oral Sci. 2023. [Google Scholar] [CrossRef]
- García-Braz, S.H.; Prados-Privado, M.; Zanatta, L.C.S.; Calvo-Guirado, J.L.; Prados-Frutos, J.C.; Gehrke, S.A. A Finite Element Analysis to Compare Stress Distribution on Extra-Short Implants with Two Different Internal Connections. J. Clin. Med. 2019, 8, 1103. [Google Scholar] [CrossRef] [Green Version]
- Fiorillo, L.; Milone, D.; D’andrea, D.; Santonocito, D.; Risitano, G.; Cervino, G.; Cicciù, M. Finite Element Analysis of Zirconia Dental Implant. Prosthesis 2022, 4, 490–499. [Google Scholar] [CrossRef]
- Emam, M.; Arafa, A.M. Stress Distribution and Fracture Resistance of Green Reprocessed Polyetheretherketone (PEEK) Single Implant Crown Restorations Compared to Unreprocessed PEEK and Zirconia: An in-Vitro Study. BMC Oral Health 2023, 23, 275. [Google Scholar] [CrossRef]
- Cicciù, M.; Cervino, G.; Terranova, A.; Risitano, G.; Raffaele, M.; Cucinotta, F.; Santonocito, D.; Fiorillo, L. Prosthetic and Mechanical Parameters of the Facial Bone under the Load of Different Dental Implant Shapes: A Parametric Study. Prosthesis 2019, 1, 41–53. [Google Scholar] [CrossRef] [Green Version]
- De Andrade, G.S.; Kalman, L.; Giudice, R.L.; Adolfi, D.; Feilzer, A.J.; Tribst, J.P.M. Biomechanics of implant-supported restorations. Braz. Dent. Sci. 2023, 26, 1–15. [Google Scholar] [CrossRef]
- Tribst, J.P.M.; Dal Piva, A.M.d.O.; Lo Giudice, R.; Borges, A.L.S.; Bottino, M.A.; Epifania, E.; Ausiello, P. The Influence of Custom-Milled Framework Design for an Implant-Supported Full-Arch Fixed Dental Prosthesis: 3D-FEA Study. Int. J. Environ. Res. Public Health 2020, 17, 4040. [Google Scholar] [CrossRef]
- Ausiello, P.; Tribst, J.P.M.; Ventre, M.; Salvati, E.; di Lauro, A.E.; Martorelli, M.; Lanzotti, A.; Watts, D.C. The role of cortical zone level and prosthetic platform angle in dental implant mechanical response: A 3D finite element analysis. Dent. Mater. 2021, 37, 1688–1697. [Google Scholar] [CrossRef]
- Giudice, R.L.; Sindoni, A.; Tribst, J.P.M.; Piva, A.M.D.O.D.; Giudice, G.L.; Bellezza, U.; Giudice, G.L.; Famà, F. Evaluation of Zirconia and High Performance Polymer Abutment Surface Roughness and Stress Concentration for Implant-Supported Fixed Dental Prostheses. Coatings 2022, 12, 238. [Google Scholar] [CrossRef]
- Paracchini, L.; Barbieri, C.; Redaelli, M.; Di Croce, D.; Vincenzi, C.; Guarnieri, R. Finite Element Analysis of a New Dental Implant Design Optimized for the Desirable Stress Distribution in the Surrounding Bone Region. Prosthesis 2020, 2, 225–236. [Google Scholar] [CrossRef]
- Fiore, D.; Montagner, A.; Sivolella, M.; Stellini, S.; Yilmaz, E.; Brunello, B. Peri-Implant Bone Loss and Overload: A Systematic Review Focusing on Occlusal Analysis through Digital and Analogic Methods. J. Clin. Med. 2022, 11, 4812. [Google Scholar]
- Oliveros-López, L.-G.; Castillo-De-Oyagüe, R.; Serrera-Figallo, M.; Martínez-González, J.; Pérez-Velasco, A.; Torres-Lagares, D.; Gutiérrez-Pérez, J.-L. Bone Loss in Bruxist Patients Wearing Dental Implant Prostheses: A Finite Element Analysis. Metals 2020, 10, 1132. [Google Scholar] [CrossRef]
- D’amico, C.; Bocchieri, S.; Sambataro, S.; Surace, G.; Stumpo, C.; Fiorillo, L. Occlusal Load Considerations in Implant-Supported Fixed Restorations. Prosthesis 2020, 2, 252–265. [Google Scholar] [CrossRef]
- Bambini, F.; Orilisi, G.; Quaranta, A.; Memè, L. Biological Oriented Immediate Loading: A New Mathematical Implant Vertical Insertion Protocol, Five-Year Follow-Up Study. Materials 2021, 14, 387. [Google Scholar] [CrossRef]
- Santonocito, D.; Nicita, F.; Risitano, G. A Parametric Study on a Dental Implant Geometry Influence on Bone Remodelling through a Numerical Algorithm. Prosthesis 2021, 3, 157–172. [Google Scholar] [CrossRef]
- Ellendula, Y.; Sekar, A.C.; Nalla, S.; Basany, R.B.; Sailasri, K.; Thandu, A. Biomechanical Evaluation of Stress Distribution in Equicrestal and Sub-crestally Placed, Platform-Switched Morse Taper Dental Implants in D3 Bone: Finite Element Analysis. Cureus 2022, 2914, e24591. [Google Scholar] [CrossRef]
- Baggi, L.; Cappelloni, I.; Di Girolamo, M.; Maceri, F.; Vairo, G. The influence of implant diameter and length on stress distribution of osseointegrated implants related to crestal bone geometry: A three-dimensional finite element analysis. J. Prosthet. Dent. 2008, 100, 422–431. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chou, H.-Y.; Müftü, S.; Bozkaya, D. Combined effects of implant insertion depth and alveolar bone quality on periimplant bone strain induced by a wide-diameter, short implant and a narrow-diameter, long implant. J. Prosthet. Dent. 2010, 104, 293–300. [Google Scholar] [CrossRef]
- Del Amo, F.S.L.; Yu, S.-H.; Sammartino, G.; Sculean, A.; Zucchelli, G.; Rasperini, G.; Felice, P.; Pagni, G.; Iorio-Siciliano, V.; Grusovin, M.G.; et al. Peri-implant Soft Tissue Management: Cairo Opinion Consensus Conference. Int. J. Environ. Res. Public Heal. 2020, 17, 2281. [Google Scholar] [CrossRef] [Green Version]
- Felice, P.; Bonifazi, L.; Pistilli, R.; Ferri, A.; Gasparro, R.; Barausse, C. Influence of Keratinized Tissue on Short Dental Implants: A Parallel Cohort Retrospective Study on 217 Implants with a Mean Follow-up of 4.1 Years. Int. J. Oral Maxillofac. Implant. 2023, 38, 462–467. [Google Scholar] [CrossRef]
- Aimetti, M.; Ferrarotti, F.; Mariani, G.; Ghelardoni, C.; Romano, F. Soft Tissue and Crestal Bone Changes Around Implants with Platform-Switched Abutments Placed Nonsubmerged at Subcrestal Position: A 2-Year Clinical and Radiographic Evaluation. Int. J. Oral Maxillofac. Implant. 2015, 30, 1369–1377. [Google Scholar] [CrossRef] [Green Version]
- Chan, Y.-H.; Lew, W.-Z.; Lu, E.; Loretz, T.; Lu, L.; Lin, C.-T.; Feng, S.-W. An evaluation of the biocompatibility and osseointegration of novel glass fiber reinforced composite implants: In vitro and in vivo studies. Dent. Mater. 2018, 34, 470–485. [Google Scholar] [CrossRef] [PubMed]
- Çaglar, A.; Bal, B.T.; Karakoca, S.; Aydın, C.; Yılmaz, H.; Sarısoy, S. Three-dimensional finite element analysis of titanium and yttrium-stabilized zirconium dioxide abutments and implants. Int. J. Oral Maxillofac. Implant. 2011, 26, 961–969. [Google Scholar]
- Lee, W.-T.; Koak, J.-Y.; Lim, Y.-J.; Kim, S.-K.; Kwon, H.-B.; Kim, M.-J. Stress shielding and fatigue limits of poly-ether-ether-ketone dental implants. J. Biomed. Mater. Res. Part B Appl. Biomater. 2012, 100B, 1044–1052. [Google Scholar] [CrossRef]
- Najeeb, S.; Zafar, M.S.; Khurshid, Z.; Siddiqui, F. Applications of polyetheretherketone (PEEK) in oral implantology and prosthodontics. J. Prosthodont. Res. 2016, 60, 12–19. [Google Scholar] [CrossRef] [PubMed]
- Barbosa-Júnior, S.A.; Pereira, G.K.R.; DaPieve, K.S.; Machado, P.S.; Valandro, L.F.; Schuh, C.; Consani, R.L.X.; Bacchi, A. Mechanical Fatigue Analysis of PEEK as Alternative to Zirconia for Definitive Hybrid Abutments Supporting All-Ceramic Crowns. Int. J. Oral Maxillofac. Implant. 2020, 35, 1209–1217. [Google Scholar] [CrossRef]
- Mishra, S.; Chowdhary, R. PEEK materials as an alternative to titanium in dental implants: A systematic review. Clin. Implant. Dent. Relat. Res. 2018, 21, 208–222. [Google Scholar] [CrossRef] [Green Version]
- Soares, P.M.; Cadore-Rodrigues, A.C.; Borges, A.L.S.; Valandro, L.F.; Pereira, G.K.R.; Rippe, M.P. Load-bearing capacity under fatigue and FEA analysis of simplified ceramic restorations supported by Peek or zirconia polycrystals as foundation substrate for implant purposes. J. Mech. Behav. Biomed. Mater. 2021, 123, 104760. [Google Scholar] [CrossRef]
- Tretto, P.H.W.; Dos Santos, M.B.F.; Spazzin, A.O.; Pereira, G.K.R.; Bacchi, A. Assessment of stress/strain in dental implants and abutments of alternative materials compared to conventional titanium alloy-3D non-linear finite element analysis. Comput. Methods Biomech. Biomed. Eng. 2020, 23, 372–383. [Google Scholar] [CrossRef] [PubMed]
- Ramos, N.d.C.; Ramos, G.F.; Penteado, M.M.; de Melo, R.M.; Borges, A.L.S.; Bottino, M.A.; Tribst, J.P.M. Comparative Stress Evaluation between Bilayer, Monolithic and Cutback All-Ceramic Crown Designs: 3D Finite Element Study. Prosthesis 2021, 3, 173–180. [Google Scholar] [CrossRef]
- Brånemark, P.-I.; Breine, U.; Adell, R.; Hansson, B.O.; Lindström, J.; Ohlsson, Å. Intra-Osseous Anchorage of Dental Prostheses:I. Experimental Studies. Scand. J. Plast. Reconstr. Surg. 1969, 3, 81–100. [Google Scholar] [CrossRef]
- Geckili, E.; Geckili, O.; Bilhan, H.; Kutay, O.; Bilgin, T. Clinical comparison of screw-retained and screwless Morse taper im-plant-abutment connections: One-year postloading results. Int. J. Oral Maxillofac. Implant. 2017, 32, 1123–1131. [Google Scholar] [CrossRef] [Green Version]
- Fiorillo, L.; Meto, A.; Cicciù, M. Bioengineering Applied to Oral Implantology, a New Protocol: “Digital Guided Surgery”. Prosthesis 2023, 5, 234–250. [Google Scholar] [CrossRef]
- Choi, S.; Kang, Y.S.; Yeo, I.-S.L. Influence of Implant–Abutment Connection Biomechanics on Biological Response: A Literature Review on Interfaces between Implants and Abutments of Titanium and Zirconia. Prosthesis 2023, 5, 527–538. [Google Scholar] [CrossRef]
- Menini, M.; Pesce, P.; Delucchi, F.; Ambrogio, G.; Canepa, C.; Carossa, M.; Pera, F. One-stage versus two-stage technique using two splinted extra-short implants: A multicentric split-mouth study with a one-year follow-up. Clin. Implant. Dent. Relat. Res. 2022, 24, 602–610. [Google Scholar] [CrossRef]
- El-Shabrawy, M.M.; Zaki, A.A.; Elguindy, J.; El Nahass, H.; Bakr, K.A. Patient Satisfaction and Pink Esthetics of PEEK Versus Zirconium Abutments in the Esthetic Zone (A Randomized Controlled Trial). Braz. Dent. Sci. 2021, 24, 1–16. [Google Scholar] [CrossRef]
- Giordano, M.; Ausiello, P.; Martorelli, M. Accuracy evaluation of surgical guides in implant dentistry by non-contact reverse engineering techniques. Dent. Mater. 2012, 28, e178–e185. [Google Scholar] [CrossRef]
- de Kok, P.; Kleverlaan, C.J.; de Jager, N.; Kuijs, R.; Feilzer, A.J. Mechanical performance of implant-supported posterior crowns. J. Prosthet. Dent. 2015, 114, 59–66. [Google Scholar] [CrossRef] [PubMed]
- Van Oers, R.F.M.; Feilzer, A.J. Abutment-to-fixture load transfer and peri-implant bone stress. Am. J. Dent. 2015, 28, 247–250. [Google Scholar] [PubMed]
- Tribst, J.P.M.; Piva, A.M.d.O.D.; Blom, E.J.; Kleverlaan, C.J.; Feilzer, A.J. Dental biomechanics of root-analog implants in different bone types. J. Prosthet. Dent. 2022, 116, 104370. [Google Scholar] [CrossRef] [PubMed]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Structures | Elastic Modulus (GPa) | Poisson Ratio |
|---|---|---|
| Titanium * | 110 | 0.3 |
| BIO-HPP | 3 | 0.3 |
| Cement | 8 | 0.3 |
| Bone tissue | 5.5 | 0.3 |
| Placement | Abutment Design | Microstrain (µ/µ) | Abutment Stress (MPa) | Implant Stress (MPa) | Screw Stress (MPa) |
|---|---|---|---|---|---|
| Sub-crestal | BIO-HPP | 1.08 × 10−2 | 222.67 | 338.63 | 71.10 |
| Titanium | 1.07 × 10−2 | 220.53 | 342.05 | 75.05 | |
| Crestal | BIO-HPP | 1.17 × 10−2 | 248.08 | 287.34 | 71.19 |
| Titanium | 1.17 × 10−2 | 219.88 | 291.94 | 75.61 | |
| Supra-crestal | BIO-HPP | 1.23 × 10−2 | 248.08 | 274.25 | 63.74 |
| Titanium | 1.20 × 10−2 | 221.77 | 276.93 | 61.33 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lo Giudice, R.; Machado, P.S.; Dal Piva, A.M.d.O.; Tribst, J.P.M. Influence of Placement of Ultrashort Implant at Sub-Crestal, Crestal and Supra-Crestal Level with Titanium or Polyetheretherketone Hybrid Abutment: 3D Finite Element Analysis. Prosthesis 2023, 5, 721-732. https://doi.org/10.3390/prosthesis5030051
Lo Giudice R, Machado PS, Dal Piva AMdO, Tribst JPM. Influence of Placement of Ultrashort Implant at Sub-Crestal, Crestal and Supra-Crestal Level with Titanium or Polyetheretherketone Hybrid Abutment: 3D Finite Element Analysis. Prosthesis. 2023; 5(3):721-732. https://doi.org/10.3390/prosthesis5030051
Chicago/Turabian StyleLo Giudice, Roberto, Pablo Soares Machado, Amanda Maria de Oliveira Dal Piva, and João Paulo Mendes Tribst. 2023. "Influence of Placement of Ultrashort Implant at Sub-Crestal, Crestal and Supra-Crestal Level with Titanium or Polyetheretherketone Hybrid Abutment: 3D Finite Element Analysis" Prosthesis 5, no. 3: 721-732. https://doi.org/10.3390/prosthesis5030051