


Facial Scanners in Dentistry: An Overview

Abstract
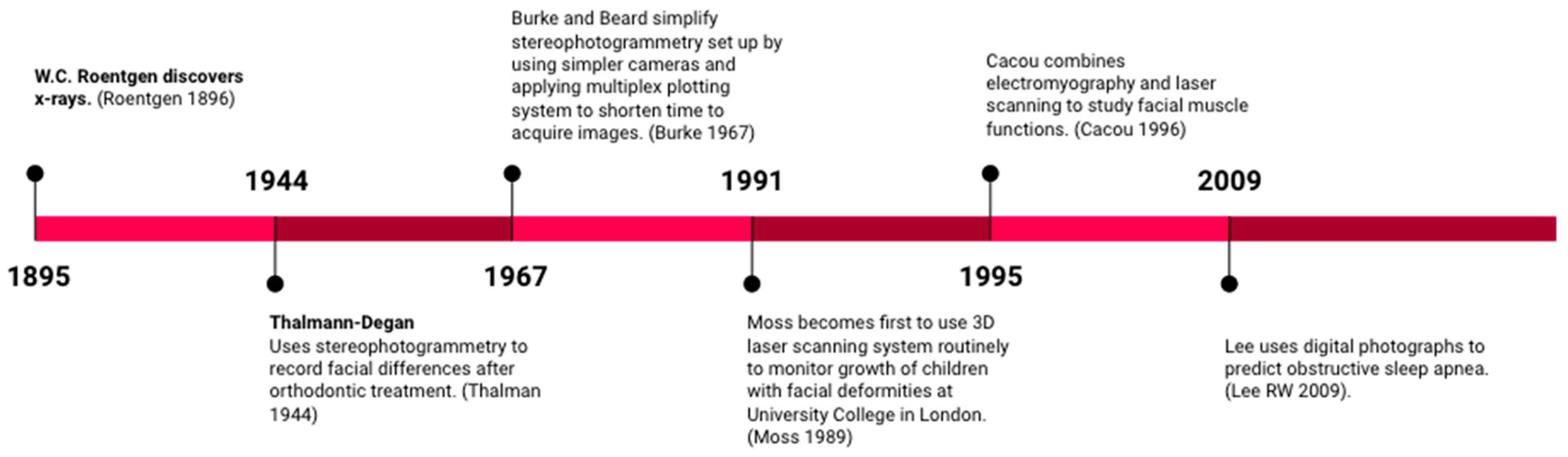
:1. Introduction: Significance of Facial Scanners in Dentistry
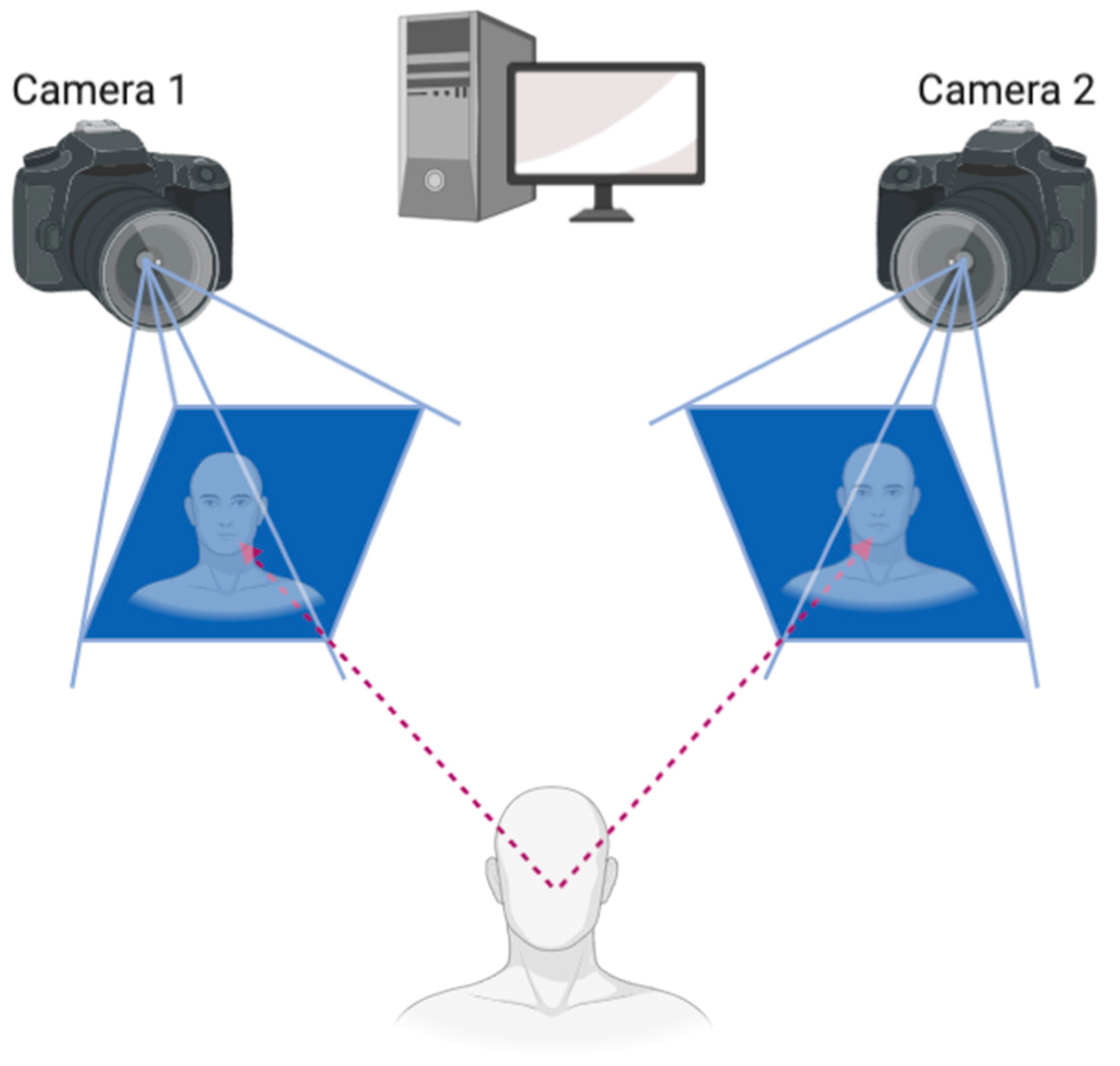
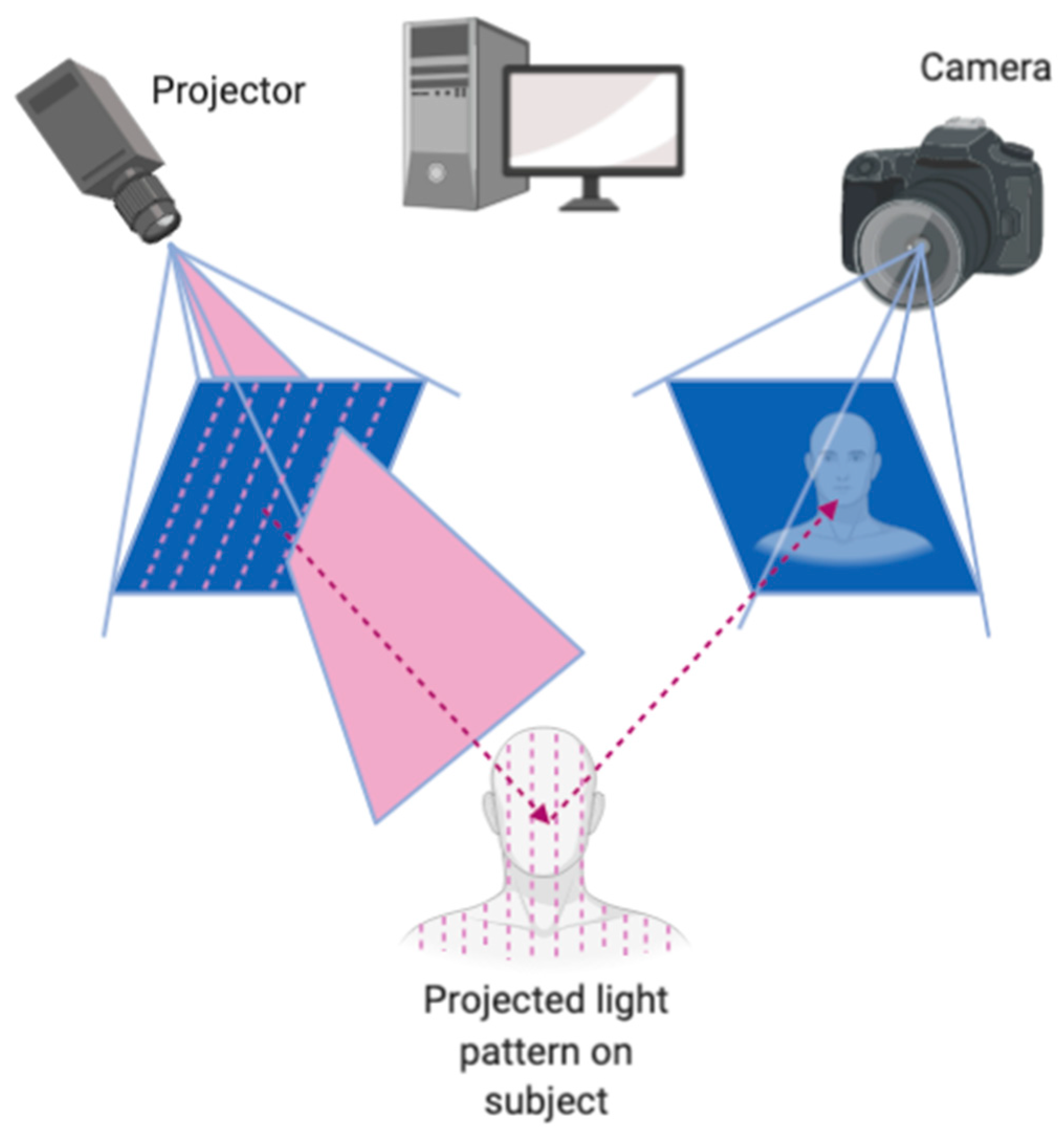
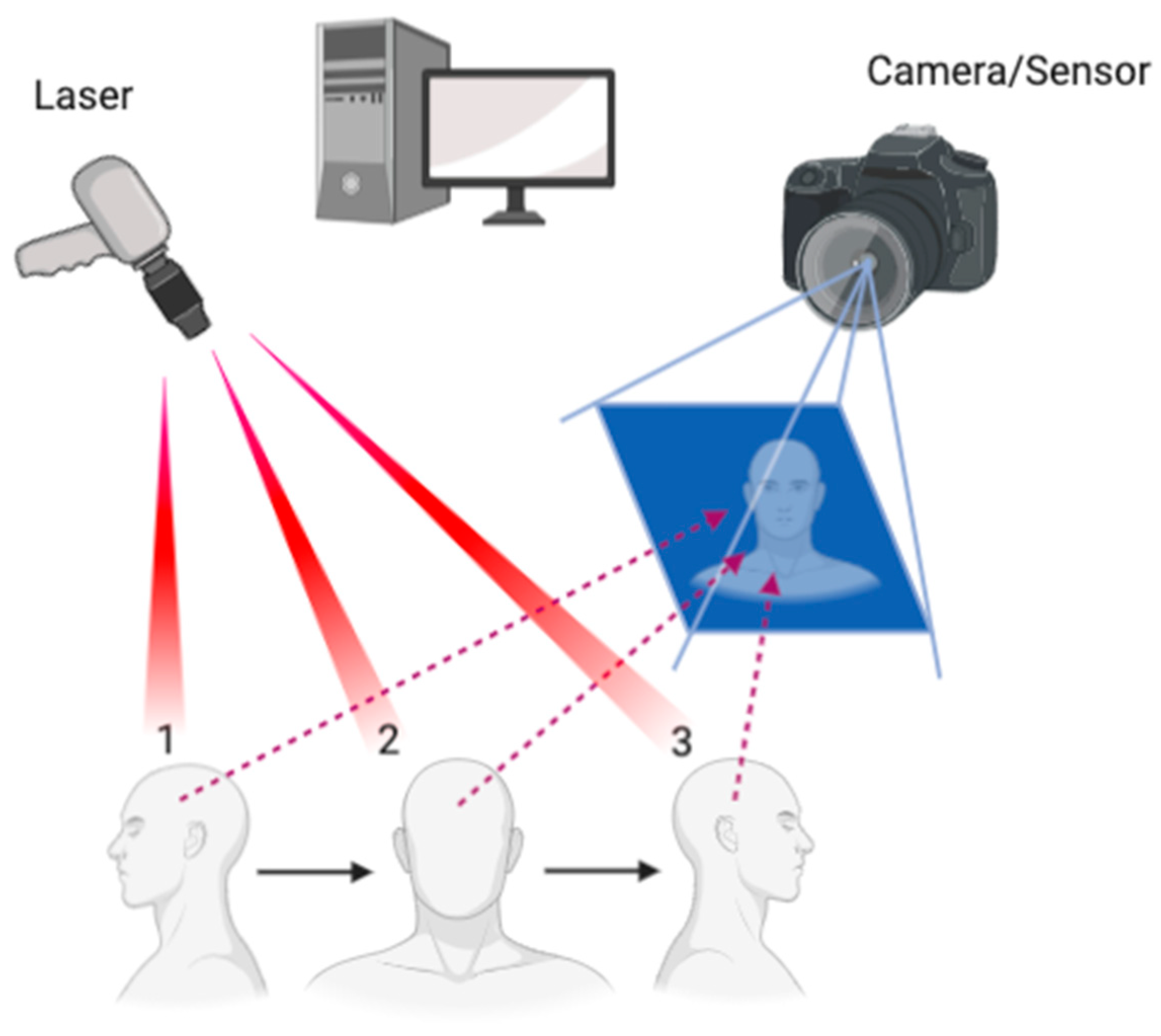
1.1. Scanning Mechanisms
1.2. Accuracy of Facial Scanners
2. Applications of Facial Scanners in Dentistry
2.1. Diagnostic Records and the Virtual Patient
2.2. Smile Design
2.3. Obstructive Sleep Apnea (OSA)
3. Future Applications
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Moss, J.P.; Coombes, A.M.; Linney, A.D.; Campos, J. Methods of three dimensional analysis of patients with asymmetry of the face. Proc. Finn. Dent. Soc. Suom. Hammaslaak. Toim. 1991, 87, 139–149. [Google Scholar]
- Karatas, O.H.; Toy, E. Three-dimensional imaging techniques: A literature review. Eur. J. Dent. 2014, 8, 132–140. [Google Scholar] [CrossRef] [PubMed]
- Mangano, F.; Gandolfi, A.; Luongo, G.; Logozzo, S. Intraoral scanners in dentistry: A review of the current literature. BMC Oral Health 2017, 17, 149. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hassan, B.; Greven, M.; Wismeijer, D. Integrating 3D facial scanning in a digital workflow to CAD/CAM design and fabricate complete dentures for immediate total mouth rehabilitation. J. Adv. Prosthodont. 2017, 9, 381–386. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Piedra-Cascón, W.; Meyer, M.J.; Methani, M.M.; Revilla-León, M. Accuracy (trueness and precision) of a dual-structured light facial scanner and interexaminer reliability. J. Prosthet. Dent. 2020, 124, 567–574. [Google Scholar] [CrossRef] [PubMed]
- Hong, C.; Choi, K.; Kachroo, Y.; Kwon, T.; Nguyen, A.; McComb, R.; Moon, W. Evaluation of the 3dMDface system as a tool for soft tissue analysis. Orthod. Craniofac. Res. 2017, 20 (Suppl. S1), 119–124. [Google Scholar] [CrossRef]
- Heike, C.L.; Upson, K.; Stuhaug, E.; Weinberg, S.M. 3D digital stereophotogrammetry: A practical guide to facial image acquisition. Head Face Med. 2010, 6, 18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tzou, C.-H.J.; Artner, N.M.; Pona, I.; Hold, A.; Placheta, E.; Kropatsch, W.G.; Frey, M. Comparison of three-dimensional surface-imaging systems. J. Plast. Reconstr. Aesthetic Surg. JPRAS 2014, 67, 489–497. [Google Scholar] [CrossRef]
- Gibelli, D.; Pucciarelli, V.; Poppa, P.; Cummaudo, M.; Dolci, C.; Cattaneo, C.; Sforza, C. Three-dimensional facial anatomy evaluation: Reliability of laser scanner consecutive scans procedure in comparison with stereophotogrammetry. J. Cranio-Maxillofac. Surg. Off. Publ. Eur. Assoc. Cranio-Maxillofac. Surg. 2018, 46, 1807–1813. [Google Scholar] [CrossRef]
- Amornvit, P.; Sanohkan, S. The Accuracy of Digital Face Scans Obtained from 3D Scanners: An In Vitro Study. Int. J. Environ. Res. Public Health 2019, 16, 5061. [Google Scholar] [CrossRef] [Green Version]
- Bohner, L.; Gamba, D.D.; Hanisch, M.; Marcio, B.S.; Neto, P.T.; Laganá, D.C.; Sesma, N. Accuracy of digital technologies for the scanning of facial, skeletal, and intraoral tissues: A systematic review. J. Prosthet. Dent. 2019, 121, 246–251. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Y.J.; Xiong, Y.X.; Wang, Y. Three-Dimensional Accuracy of Facial Scan for Facial Deformities in Clinics: A New Evaluation Method for Facial Scanner Accuracy. PLoS ONE 2017, 12, e0169402. [Google Scholar] [CrossRef] [Green Version]
- Artopoulos, A.; Buytaert, J.; Dirckx, J.; Coward, T. Comparison of the accuracy of digital stereophotogrammetry and projection moiré profilometry for three-dimensional imaging of the face. Int. J. Oral Maxillofac. Surg. 2014, 43, 654–662. [Google Scholar] [CrossRef] [PubMed]
- Knoops, P.G.; Beaumont, C.A.A.; Borghi, A.; Rodriguez-Florez, N.; Breakey, R.W.; Rodgers, W.; Angullia, F.; Jeelani, N.O.; Schievano, S.; Dunaway, D.J. Comparison of three-dimensional scanner systems for craniomaxillofacial imaging. J. Plast. Reconstr. Aesthetic Surg. JPRAS 2017, 70, 441–449. [Google Scholar] [CrossRef] [PubMed]
- Joda, T.; Gallucci, G.O. The virtual patient in dental medicine. Clin. Oral Implants. Res. 2015, 26, 725–726. [Google Scholar] [CrossRef]
- Mangano, C.; Luongo, F.; Migliario, M.; Mortellaro, C.; Mangano, F.G. Combining Intraoral Scans, Cone Beam Computed Tomography and Face Scans: The Virtual Patient. J. Craniofac. Surg. 2018, 29, 2241–2246. [Google Scholar] [CrossRef]
- Ayoub, A.F.; Xiao, Y.; Khambay, B.; Siebert, J.P.; Hadley, D. Towards building a photo-realistic virtual human face for craniomaxillofacial diagnosis and treatment planning. Int. J. Oral Maxillofac. Surg. 2007, 36, 423–428. [Google Scholar] [CrossRef]
- Lepidi, L.; Galli, M.; Mastrangelo, F.; Venezia, P.; Joda, T.; Wang, H.; Li, J. Virtual Articulators and Virtual Mounting Procedures: Where Do We Stand? J. Prosthodont. Off. J. Am. Coll. Prosthodont. 2020, 30, 24–35. [Google Scholar] [CrossRef]
- Lam, W.Y.H.; Hsung, R.T.C.; Choi, W.W.S.; Luk, H.W.K.; Pow, E.H.N. A 2-part facebow for CAD-CAM dentistry. J. Prosthet. Dent. 2016, 116, 843–847. [Google Scholar] [CrossRef]
- Schweiger, J. 3D Facial Scanning. Published December 2018. Available online: https://www.zirkonzahn.com/assets/files/publications/EN-Dental-Dialogue-2018-12-web.pdf (accessed on 29 December 2020).
- Solaberrieta, E.; Garmendia, A.; Minguez, R.; Brizuela, A.; Pradies, G. Virtual facebow technique. J. Prosthet. Dent. 2015, 114, 751–755. [Google Scholar] [CrossRef]
- Solaberrieta, E.; Mínguez, R.; Barrenetxea, L.; Otegi, J.R.; Szentpétery, A. Comparison of the accuracy of a 3-dimensional virtual method and the conventional method for transferring the maxillary cast to a virtual articulator. J. Prosthet. Dent. 2015, 113, 191–197. [Google Scholar] [CrossRef] [PubMed]
- Inoue, N.; Scialabba, R.; Lee, J.D. A comparison of virtually mounted dental casts from traditional facebow records, average values, and 3D facial scans. J. Prosthet. Dent. 2022. [Google Scholar] [CrossRef]
- Hong, S.J.; Noh, K. Setting the sagittal condylar inclination on a virtual articulator by using a facial and intraoral scan of the protrusive interocclusal position: A dental technique. J. Prosthet. Dent. 2021, 125, 392–395. [Google Scholar] [CrossRef]
- Kwon, J.H.; Im, S.; Chang, M.; Kim, J.E.; Shim, J.S. A digital approach to dynamic jaw tracking using a target tracking system and a structured-light three-dimensional scanner. J. Prosthodont. Res. 2019, 63, 115–119. [Google Scholar] [CrossRef]
- Kim, J.E.; Park, J.H.; Moon, H.S.; Shim, J.S. Complete assessment of occlusal dynamics and establishment of a digital workflow by using target tracking with a three-dimensional facial scanner. J. Prosthodont. Res. 2019, 63, 120–124. [Google Scholar] [CrossRef]
- Stavness, I.K.; Hannam, A.G.; Tobias, D.L.; Zhang, X. Simulation of dental collisions and occlusal dynamics in the virtual environment. J. Oral Rehabil. 2016, 43, 269–278. [Google Scholar] [CrossRef] [PubMed]
- Antolín, A.; Rodríguez, N.A.; Crespo, J.A. Digital Flow in Implantology Using Facial Scanner. Published 2018. Available online: https://www.semanticscholar.org/paper/Digital-Flow-in-Implantology-Using-Facial-Scanner-Antol%C3%ADn-Rodr%C3%ADguez/0397531202d32a61f18337de99e4b3acf546206b (accessed on 23 December 2020).
- Lin, W.S.; Harris, B.T.; Phasuk, K.; Llop, D.R.; Morton, D. Integrating a facial scan, virtual smile design, and 3D virtual patient for treatment with CAD-CAM ceramic veneers: A clinical report. J. Prosthet. Dent. 2018, 119, 200–205. [Google Scholar] [CrossRef]
- Jamieson, A.; Guilleminault, C.; Partinen, M.; Quera-Salva, M.A. Obstructive sleep apneic patients have craniomandibular abnormalities. Sleep 1986, 9, 469–477. [Google Scholar] [CrossRef]
- Ferguson, K.A.; Ono, T.; Lowe, A.A.; Ryan, C.F.; Fleetham, J.A. The relationship between obesity and craniofacial structure in obstructive sleep apnea. Chest 1995, 108, 375–381. [Google Scholar] [CrossRef]
- Kushida, C.A.; Efron, B.; Guilleminault, C. A predictive morphometric model for the obstructive sleep apnea syndrome. Ann. Intern. Med. 1997, 127 8 Pt 1, 581–587. [Google Scholar] [CrossRef]
- Lee, R.W.W.; Vasudavan, S.; Hui, D.; Prvan, T.; Petocz, P.; Darendeliler, M.A.; Cistulli, P.A. Differences in Craniofacial Structures and Obesity in Caucasian and Chinese Patients with Obstructive Sleep Apnea. Sleep 2010, 33, 1075–1080. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2910536/ (accessed on 29 December 2020). [PubMed]
- Lee, C.H.; Kim, J.-W.; Lee, H.J.; Yun, P.-Y.; Kim, D.-Y.; Seo, B.S.; Yoon, I.-Y.; Mo, J.-H. An investigation of upper airway changes associated with mandibular advancement device using sleep videofluoroscopy in patients with obstructive sleep apnea. Arch. Otolaryngol. Head Neck Surg. 2009, 135, 910–914. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Espinoza-Cuadros, F.; Fernández-Pozo, R.; Toledano, D.T.; Alcázar-Ramírez, J.D.; López-Gonzalo, E.; Hernández-Gómez, L.A. Speech Signal and Facial Image Processing for Obstructive Sleep Apnea Assessment. Comput. Math. Methods Med. 2015, 2015, 489761. [Google Scholar] [CrossRef] [PubMed]
- Balaei, A.T.; Sutherland, K.; Cistulli, P.A.; de Chazal, P. Automatic detection of obstructive sleep apnea using facial images. In Proceedings of the 2017 IEEE 14th International Symposium on Biomedical Imaging (ISBI 2017), Melbourne, Australia, 18–21 April 2017; pp. 215–218. [Google Scholar] [CrossRef]
- Islam, S.M.S.; Mahmood, H.; Al-Jumaily, A.A.; Claxton, S. Deep Learning of Facial Depth Maps for Obstructive Sleep Apnea Prediction. In Proceedings of the 2018 International Conference on Machine Learning and Data Engineering (ICMLDE), Sydney, Australia, 3–7 December 2018; pp. 154–157. [Google Scholar] [CrossRef]
- Eastwood, P.; Gilani, S.Z.; McArdle, N.; Hillman, D.; Walsh, J.; Maddison, K.; Goonewardene, B.M.; Mian, A. Predicting sleep apnea from three-dimensional face photography. J. Clin. Sleep Med. 2020, 16, 493–502. [Google Scholar] [CrossRef] [PubMed]
- Duong, K.; Glover, J.; Perry, A.; Olmstead, D.; Colarusso, P.; Ungrin, M.; MacLean, J.; Martin, A. Customized Facemasks for Continuous Positive Airway Pressure: Feasibility Study in Healthy Adults Volunteers. Am. J. Respir. Crit. Care Med. 2020, 201, A2432. [Google Scholar] [CrossRef]
- Luyster, F.S.; Buysse, D.J.; Strollo, P.J. Comorbid insomnia and obstructive sleep apnea: Challenges for clinical practice and research. J. Clin. Sleep Med. JCSM Off. Publ. Am. Acad. Sleep Med. 2010, 6, 196–204. [Google Scholar]
- Liu, W.; Li, M.; Yi, L. Identifying children with autism spectrum disorder based on their face processing abnormality: A machine learning framework. Autism Res. Off. J. Int. Soc. Autism Res. 2016, 9, 888–898. [Google Scholar] [CrossRef]
- Knoops, P.G.M.; Papaioannou, A.; Borghi, A.; Breakey, R.W.F.; Wilson, A.T.; Jeelani, O.; Zafeiriou, S.; Steinbacher, D.; Padwa, B.L.; Dunaway, D.J.; et al. A machine learning framework for automated diagnosis and computer-assisted planning in plastic and reconstructive surgery. Sci. Rep. 2019, 9, 13597. [Google Scholar] [CrossRef] [Green Version]
- Jiang, J.G.; Zhang, Y.D. Motion planning and synchronized control of the dental arch generator of the tooth-arrangement robot. Int. J. Med. Robot. Comput. Assist. Surg. MRCAS 2013, 9, 94–102. [Google Scholar] [CrossRef]
- Burgert, O.; Seifert, S.; Salb, T.; Gockel, T.; Dillmann, R.; Hassfeld, S.; Mühling, J. A VR-system supporting symmetry related cranio-maxillofacial surgery. Stud. Health Technol. Inform. 2003, 94, 33–35. [Google Scholar]
- Gulati, M.; Anand, V.; Salaria, S.K.; Jain, N.; Gupta, S. Computerized implant-dentistry: Advances toward automation. J. Indian Soc. Periodontol. 2015, 19, 5–10. [Google Scholar] [CrossRef] [PubMed]
- Azari, A.; Nikzad, S. Computer-assisted implantology: Historical background and potential outcomes-a review. Int. J. Med. Robot. Comput. Assist. Surg. MRCAS 2008, 4, 95–104. [Google Scholar] [CrossRef] [PubMed]
- Du, Y.F.; Chen, N.; Li, D.Q. Application of robot-assisted surgery in the surgical treatment of head and neck cancer. Zhonghua Kou Qiang Yi Xue Za Zhi Zhonghua Kouqiang Yixue Zazhi Chin. J. Stomatol. 2019, 54, 58–61. [Google Scholar] [CrossRef]
- Grischke, J.; Johannsmeier, L.; Eich, L.; Griga, L.; Haddadin, S. Dentronics: Towards robotics and artificial intelligence in dentistry. Dent. Mater. Off. Publ. Acad. Dent. Mater. 2020, 36, 765–778. [Google Scholar] [CrossRef] [PubMed]
- Maikuma, Y.; Usui, K.; Araki, K.; Mataki, S.; Kurosaki, N.; Furuya, N. Evaluation of an articulated measuring apparatus for use in the oral cavity. Dent. Mater. J. 2003, 22, 168–179. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Woo, S.-Y.; Lee, S.-J.; Yoo, J.-Y.; Han, J.-J.; Hwang, S.-J.; Huh, K.-H.; Lee, S.-S.; Heo, M.-S.; Choi, S.-C.; Yi, W.-J. Autonomous bone reposition around anatomical landmark for robot-assisted orthognathic surgery. J. Cranio-Maxillofac. Surg. Off. Public Eur. Assoc. Cranio-Maxillofac. Surg. 2017, 45, 1980–1988. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Scanner Type and Name | Applications | Features | |
|---|---|---|---|
| Photogrammetry /Stereophotogrammetry | 3dMD Face system (3dMD, Atlanta, GA, USA) | Medical and dental field. | 4D records of facial expressions, function, smile and speech. Anatomically precise 3D surface images for surgical intervention assessment and measurement of long-term morphological changes outcomes, such as cleft lip and palate. No manual registration is required. |
| iPhone X (Apple, Cupertino, CA, USA) using Bellus3D Face Application (Bellus3D, Inc. Campbell, CA, USA) | Face ID authentication. Facial recognition to unlock the phone and authorize purchases. | The dot projector in the TrueDepth camera projected over 30,000 IR dots and captured the infrared image. The neural engine of Bionic Chip transformed the mathematical model to build a facial map and compared to the enrolled data. | |
| Di4D (Dimensional Imaging, Glasgow, Scotland) | Video games and movies. Crosses into the entertainment sector to provide high density facial scans. | Bring digital humans to life. Capture an actor’s high fidelity motion data and translate to a virtual character. | |
| Planmeca ProMax 3D Mid (PM) (Planmeca USA, Inc., Hoffman Estates, IL, USA) | Dental and ENT imaging. | Handles a wide range of diagnostic tasks including CBCT, orthodontic planning, CADCAM, implant planning, and maxillofacial surgeries. With anatomical presets for ears, nose and throat. | |
| Structured light scanner | Facehunter (Zirconzahn, South Tyrol, Italy) | Designed for dentists and dental technicians. | Efficient patient consultation. Planning reliability for the patient, the dentist and the dental technicians. Well-integrated with digital workflow. |
| FaceScan system (Isravision, Darmstadt, Germany) | Designed for dental field. | Has a double-mirror structure that captures three angles of 3D images and combines them into 3D models. | |
| EinScan Pro (Shining 3D Tech. Co., Ltd., Hangzhou, China) | Handheld. Designed for engineers, designers, art and heritage, custom orthotics. | Multifunctional. Utilizing infrared light instead of visible light during face scan mode, comfortable for eyes. | |
| EinScan Pro 2X Plus (Shining 3D Tech. Co., Ltd. Hangzhou, China) using Shining Software | Handheld. Not specific to dental workflow. | Multifunctional. Manually or markers align mode. Not recommended for moving or hairy objects. | |
| Priti mirror scanner and priti image software (Isravision, Polymetric, Germany) | Digital models of face and teeth merged together with image software. | Take pictures at different angles. An open 3D software with CAD construction programs. (ExoCAD Dental CAD, 3Shape dental designer) | |
| ATOS Compact Scan 5M (GOM mbH, Braunschweig, Germany) | For reverse engineering and dimension inspection. | Precise optical measuring system. Has a probing feature that can digitize deep pockets and areas that are not optically accessible. | |
| Laser scanner | ObiScanner (ObiScanner, Milano, Italy) | Dental field. | Scan lasts 15 s to produce a 3D model. Requires no training. An open software compatible with CAD systems. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, J.D.; Nguyen, O.; Lin, Y.-C.; Luu, D.; Kim, S.; Amini, A.; Lee, S.J. Facial Scanners in Dentistry: An Overview. Prosthesis 2022, 4, 664-678. https://doi.org/10.3390/prosthesis4040053
Lee JD, Nguyen O, Lin Y-C, Luu D, Kim S, Amini A, Lee SJ. Facial Scanners in Dentistry: An Overview. Prosthesis. 2022; 4(4):664-678. https://doi.org/10.3390/prosthesis4040053
Chicago/Turabian StyleLee, Jason D., Olivia Nguyen, Yu-Chun Lin, Dianne Luu, Susie Kim, Ashley Amini, and Sang J. Lee. 2022. "Facial Scanners in Dentistry: An Overview" Prosthesis 4, no. 4: 664-678. https://doi.org/10.3390/prosthesis4040053