
Ileocolic Anastomosis Dehiscence in Colorectal Cancer Surgery
 ,
,
Abstract
:1. Introduction
2. Results
2.1. Baseline Clinical and Preoperative Data
2.2. Surgical Procedure
2.3. Postoperative Findings
2.4. Association with AL
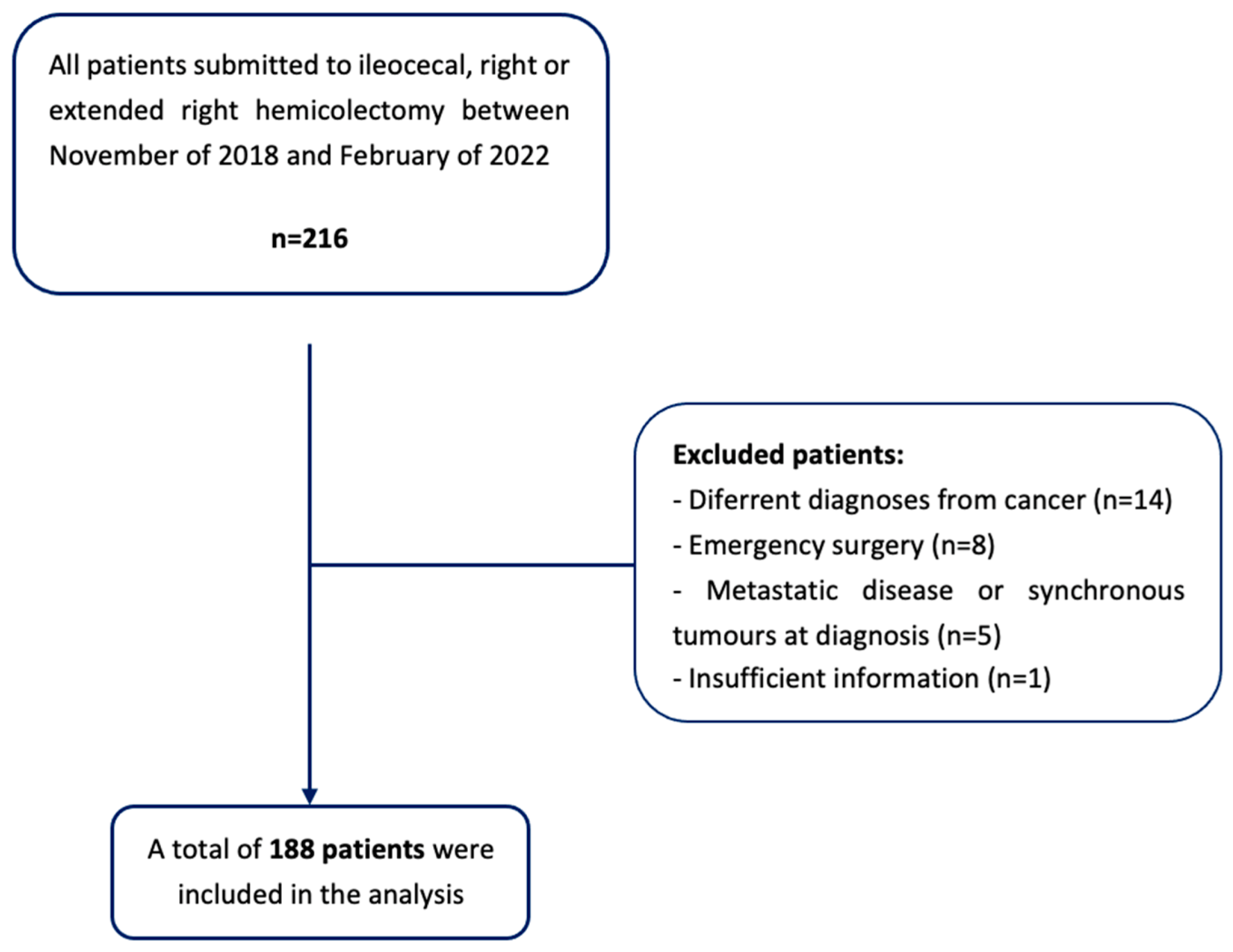
3. Materials and Methods
- Patients undergoing to emergency surgery or surgical re-intervention;
- Patients with a non-cancer diagnosis (i.e., inflammatory bowel disease or diverticular disease);
- The presence of metastatic disease at diagnosis, or synchronous tumors in other locations;
- The presence of a diverting stoma or a tumor resection surgery, with no ileocolic anastomosis;
- Insufficient information in the clinical process to determine the variables used in the study.
3.1. Data Collection
3.2. Definitions
- Grade A: Corresponds to the definition of a ‘‘radiologic leakage’’, used by several authors. This grade of AL is not associated with clinical symptoms or abnormal laboratory tests, and no active therapeutic intervention is required.
- Grade B: Patient’s clinical condition requires an active therapeutic intervention, such as the administration of antibiotics and/or radiologically guided drainage, that can be managed without operative reintervention.
- Grade C: Patients are often quite ill and require operative re-laparotomy.
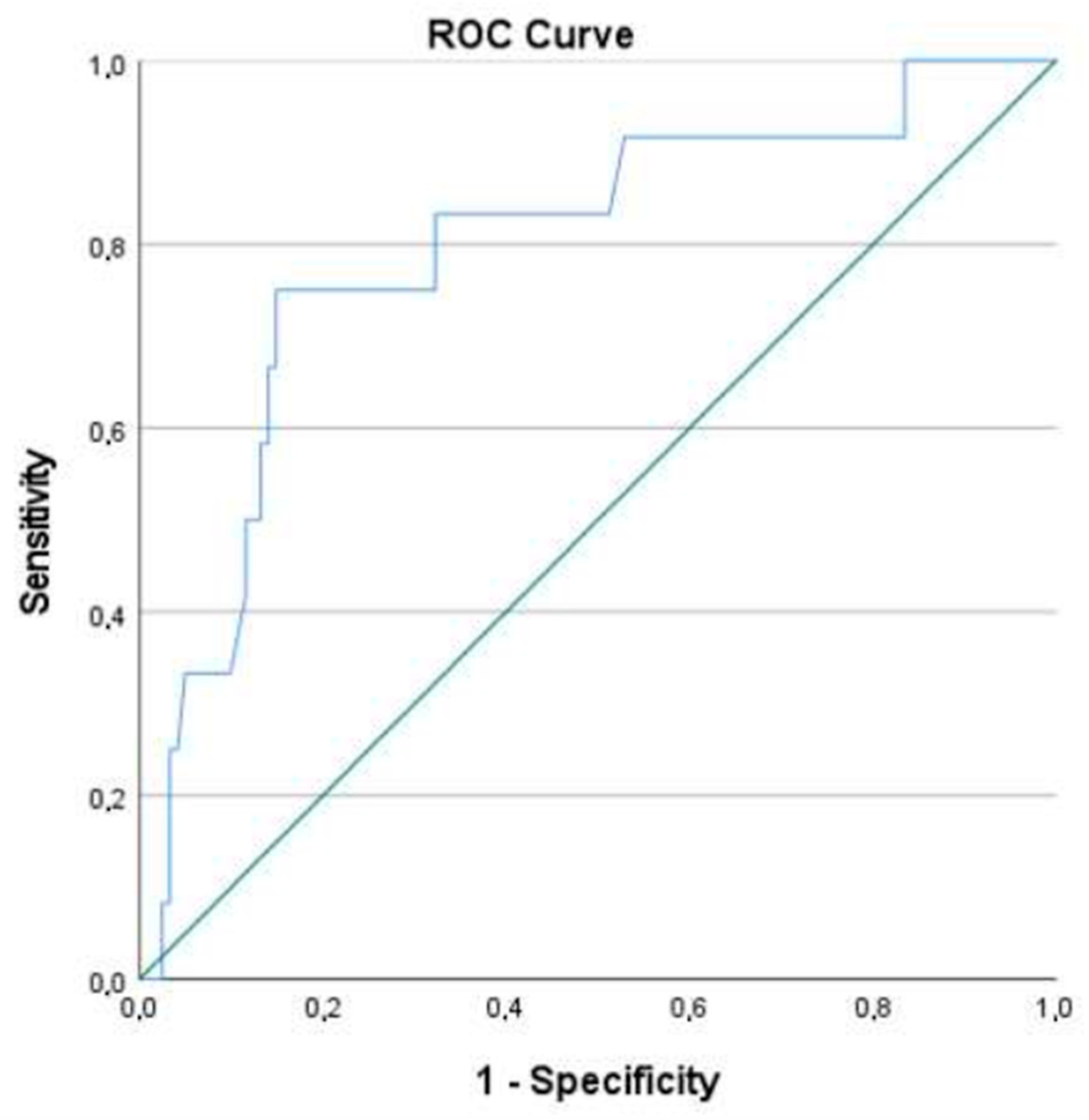
3.3. Statistical Analysis
3.4. Ethical Considerations
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Salibasic, M.; Pusina, S.; Bicakcic, E.; Pasic, A.; Gavric, I.; Kulovic, E.; Rovcanin, A.; Beslija, S. Colorectal Cancer Surgical Treatment, our Experience. Med. Arch. 2019, 73, 412–414. [Google Scholar] [CrossRef]
- Rentsch, M.; Schiergens, T.; Khandoga, A.; Werner, J. Surgery for Colorectal Cancer-Trends, Developments, and Future Perspectives. Visc. Med. 2016, 32, 184–1891. [Google Scholar] [CrossRef] [Green Version]
- Golub, R.W.; Cantu, R.; Stein, H.D. A multivariate analysis of factors contributing to leakage of intestinal anastomoses. J. Am. Coll. Surg. 1997, 184, 364–372. [Google Scholar]
- Alves, A.; Panis, Y.; Trancart, D.; Regimbeau, J.M.; Pocard, M.; Valleur, P. Factors associated with clinically significant anastomotic leakage after large bowel resection: Multivariate analysis of 707 patients. World J. Surg. 2002, 26, 499–502. [Google Scholar]
- Branagan, G.; Finnis, D. Prognosis After Anastomotic Leakage in Colorectal Surgery. Dis. Colon Rectum 2005, 48, 1021–1026. [Google Scholar] [CrossRef]
- Kube, R.; Mroczkowski, P.; Granowski, D.; Benedix, F.; Sahm, M.; Schmidt, U.; Gastinger, I.; Lippert, H. Anastomotic leakage after colon cancer surgery: A predictor of significant morbidity and hospital mortality, and diminished tumour-free survival. Eur. J. Surg. Oncol. EJSO 2010, 36, 120–124. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Buchs, N.C.; Gervaz, P.; Secic, M.; Bucher, P.; Mugnier-Konrad, B.; Morel, P. Incidence, consequences, and risk factors for anastomotic dehiscence after colorectal surgery: A prospective monocentric study. Int. J. Color. Dis. 2007, 23, 265–270. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Golda, T.; Lazzara, C.; Zerpa, C.; Sobrino, L.; Fico, V.; Kreisler, E.; Biondo, S. Risk factors for ileocolic anastomosis dehiscence; a cohort study. Am. J. Surg. 2019, 220, 170–177. [Google Scholar] [CrossRef] [PubMed]
- Sørensen, L.T.; Jørgensen, T.; Kirkeby, L.T.; Skovdal, J.; Vennits, B.; Wille-Jørgensen, P. Smoking and alcohol abuse are major risk factors for anastomotic leakage in colorectal surgery. Br. J. Surg. 1999, 86, 927–931. [Google Scholar] [CrossRef] [PubMed]
- Bruce, J.; Krukowski, Z.H.; Al-Khairy, G.; Russell, E.M.; Park, K.G.M. Systematic review of the definition and measurement of anastomotic leak after gastrointestinal surgery. Br. J. Surg. 2001, 88, 1157–1168. [Google Scholar] [CrossRef]
- Frasson, M.; ANACO Study Group; Granero-Castro, P.; Rodríguez, J.L.R.; Flor-Lorente, B.; Braithwaite, M.; Martínez, E.M.; Pérez, J.A.Á.; Cazador, A.C.; Espí, A. Risk factors for anastomotic leak and postoperative morbidity and mortality after elective right colectomy for cancer: Results from a prospective, multicentric study of 1102 patients. Eur. Soc. Coloproctol. Meet. 2014, 31, 105–114. [Google Scholar] [CrossRef]
- Choy, P.Y.G.; Bissett, I.P.; Docherty, J.G.; Parry, B.R.; Merrie, A.; Fitzgerald, A. Stapled versus handsewn methods for ileocolic anastomoses. Cochrane Database Syst. Rev. 2011, 9, CD004320. [Google Scholar] [CrossRef]
- European Society of Coloproctology Collaborating Group; Battersby, N.; Bhangu, A.; Chaudhri, S.; El-Hussuna, A.; Frasson, M.; Nepogodiev, D.; Singh, B.; Vennix, S.; Zmora, O.; et al. Relationship between method of anastomosis and anastomotic failure after right hemicolectomy and ileo-caecal resection: An international snapshot audit. Color. Dis. 2017, 19, e296–e311. [Google Scholar] [CrossRef] [Green Version]
- Jessen, M.; Nerstrøm, M.; Wilbek, T.E.; Roepstorff, S.; Rasmussen, M.S.; Krarup, P.-M. Risk factors for clinical anastomotic leakage after right hemicolectomy. Int. J. Color. Dis. 2016, 31, 1619–1624. [Google Scholar] [CrossRef] [PubMed]
- Gustafsson, P.; Jestin, P.; Gunnarsson, U.; Lindforss, U. Higher Frequency of Anastomotic Leakage with Stapled Compared to Hand-Sewn Ileocolic Anastomosis in a Large Population-Based Study. World J. Surg. 2015, 39, 1834–1839. [Google Scholar] [CrossRef]
- Jurowich, C.; Lichthardt, S.; Matthes, N.; Kastner, C.; Haubitz, I.; Prock, A.; Filser, J.; Germer, C.-T.; Wiegering, A. Effects of anastomotic technique on early postoperative outcome in open right-sided hemicolectomy. BJS Open 2018, 3, 203–209. [Google Scholar] [CrossRef]
- Sánchez-Guillén, L.; Frasson, M.; García-Granero, A.; Pellino, G.; Flor-Lorente, B.; Álvarez-Sarrado, E. Risk factors for leak, complications and mortality after ileocolic anastomosis: Comparison of two anastomotic techniques. Ann. R. Coll. Surg. Engl. 2019, 101, 571–578. [Google Scholar] [CrossRef]
- Kwak, H.D.; Kim, S.-H.; Kang, D.W.; Baek, S.-J.; Kwak, J.M.; Kim, J. Risk Factors and Oncologic Outcomes of Anastomosis Leakage After Laparoscopic Right Colectomy. Surg. Laparosc. Endosc. Percutaneous Tech. 2017, 27, 440–444. [Google Scholar] [CrossRef]
- Ellis, C.T.; Maykel, J.A.; Surgery, C.; Polk, H.C. Defining Anastomotic Leak and the Clinical Relevance of Leaks Definition of Large Bowel Anastomotic Leak Definition. Clin. Colon Rectal Surg. 2021, 34, 359–365. [Google Scholar] [PubMed]
- Kulu, Y.; Ulrich, A.; Bruckner, T.; Contin, P.; Welsch, T.; Rahbari, N.N.; Büchler, M.W.; Weitz, J. Validation of the International Study Group of Rectal Cancer definition and severity grading of anastomotic leakage. Surgery 2013, 153, 753–761. [Google Scholar] [CrossRef] [PubMed]
- Rahbari, N.N.; Weitz, J.; Hohenberger, W.; Heald, R.J.; Moran, B.; Ulrich, A.; Holm, T.; Wong, W.D.; Tiret, E.; Moriya, Y.; et al. Definition and grading of anastomotic leakage following anterior resection of the rectum: A proposal by the International Study Group of Rectal Cancer. Surgery 2010, 147, 339–351. [Google Scholar] [CrossRef]
- Clavien, P.A.; Barkun, J.; de Oliveira, M.L.; Vauthey, J.N.; Dindo, D.; Schulick, R.D.; Graf, R.; Cameron, J.; Padbury, R.; Masatoshi, M.D.; et al. The Clavien- Dindo classification of surgical complications: Five-year experience. Ann. Surg. 2009, 250, 187–196. [Google Scholar] [CrossRef] [Green Version]
- Field, A.P. Discovering Statistics Using IBM SPSS Statistics, 5th ed.; Sage: London, UK, 2017. [Google Scholar]
- Bursac, Z.; Gauss, C.H.; Williams, D.K.; Hosmer, D.W. Purposeful selection of variables in logistic regression. Source Code Biol. Med. 2008, 3, 17. [Google Scholar] [CrossRef] [Green Version]
- Bracale, U.; Melillo, P.; Lazzara, F.; Andreuccetti, J.; Stabilini, C.; Corcione, F.; Pignata, G. Single-Access Laparoscopic Rectal Resection Versus the Multiport Technique. Surg. Innov. 2014, 22, 46–53. [Google Scholar] [CrossRef] [Green Version]
- Sciuto, A.; Merola, G.; De Palma, G.D.; Sodo, M.; Pirozzi, F.; Bracale, U. Predictive factors for anastomotic leakage after laparoscopic colorectal surgery. World J. Gastroenterol. 2018, 24, 2247–2260. [Google Scholar] [CrossRef]
- Guillou, P.J.; Quirke, P.; Thorpe, H.; Walker, J.; Jayne, D.G.; Smith, A.M.; Heath, R.M.; Brown, J.M. Short-term endpoints of conventional versus laparoscopic-assisted surgery in patients with colorectal cancer (MRC CLASICC trial): Multicentre, randomised controlled trial. Lancet 2005, 365, 1718–1726. [Google Scholar] [CrossRef]
- Dubose, A.C.; Kuy, S. A Comparison of Laparoscopically Assisted and Open Colectomy for Colon Cancer. In 50 Studies Every Surgeon Should Know; Oxford Medicine Online: Oxford, UK, 2017. [Google Scholar]
- Lacy, A.M.; Delgado, S.; García-Valdecasas, J.C.; Castells, A.; Piqué, J.M.; Grande, L.; Fuster, J.; Targarona, E.M.; Pera, M.; Visa, J. Port site metastases and recurrence after laparoscopic colectomy. Surg. Endosc. 1998, 12, 1039–1042. [Google Scholar] [CrossRef]
- Arezzo, A.; Passera, R.; Scozzari, G.; Verra, M.; Morino, M. Laparoscopy for rectal cancer reduces short-term mortality and morbidity: Results of a systematic review and meta-analysis. Surg. Endosc. 2012, 27, 1485–1502. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abraham, N.S.; Young, J.M.; Solomon, M. Meta-analysis of short-term outcomes after laparoscopic resection for colorectal cancer. Br. J. Surg. 2004, 91, 1111–1124. [Google Scholar] [CrossRef] [PubMed]
- Mungo, B.; Papageorge, C.M.; Stem, M.; Molena, D.; Lidor, A.O. The Impact of Operative Approach on Postoperative Complications Following Colectomy for Colon Cancer. World J. Surg. 2017, 41, 2143–2152. [Google Scholar] [CrossRef] [PubMed]
- Milone, M.; Elmore, U.; Allaix, M.E.; Bianchi, P.P.; Biondi, A.; Boni, L.; Bracale, U.; Cassinotti, E.; Ceccarelli, G.; Corcione, F.; et al. Fashioning enterotomy closure after totally laparoscopic ileocolic anastomosis for right colon cancer: A multicenter experience. Surg. Endosc. 2019, 34, 557–563. [Google Scholar] [CrossRef]
- Carnuccio, P.; Jimeno, J.; Parés, D. Laparoscopic right colectomy: A systematic review and meta-analysis of observational studies comparing two types of anastomosis. Tech. Coloproctol. 2013, 18, 5–12. [Google Scholar] [CrossRef] [PubMed]
- Nors, J.; Sommer, T.; Wara, P. Leakage Rate After Laparoscopic Ileocolic Intracorporeal Anastomosis. J. Laparoendosc. Adv. Surg. Tech. 2018, 28, 1287–1293. [Google Scholar] [CrossRef] [PubMed]
- Kornmann, V.N.N.; Hagendoorn, J.; Van Koeverden, S.; Van Ramshorst, B.; Smits, A.B. Totally Laparoscopic Right Hemicolectomy with Intracorporeal Anastomosis is a Technically and Oncologically Safe Procedure. Acta Chir. Belg. 2013, 113, 439–443. [Google Scholar] [CrossRef]
- Biondi, A.; Santocchi, P.; Pennestrì, F.; Santullo, F.; D’ugo, D.; Persiani, R. Totally laparoscopic right colectomy versus laparoscopically assisted right colectomy: A propensity score analysis. Surg. Endosc. 2017, 31, 5275–5282. [Google Scholar] [CrossRef] [PubMed]
- Magistro, C.; Di Lernia, S.; Ferrari, G.; Zullino, A.; Mazzola, M.; De Martini, P.; De Carli, S.; Forgione, A.; Bertoglio, C.L.; Pugliese, R. Totally laparoscopic versus laparoscopic-assisted right colectomy for colon cancer: Is there any advantage in short-term outcomes? A prospective comparative assessment in our center. Surg. Endosc. 2013, 27, 2613–2618. [Google Scholar] [CrossRef] [PubMed]
- Ibáñez, N.; Abrisqueta, J.; Luján, J.; Hernández, Q.; Rufete, M.D.; Parrilla, P. Isoperistaltic versus antiperistaltic ileocolic anastomosis. Does it really matter? Results from a randomised clinical trial (ISOVANTI). Surg. Endosc. 2018, 33, 2850–2857. [Google Scholar] [CrossRef]
- 2015 European Society of Coloproctology Collaborating Group; Glasbey, J.C.; Nepogodiev, D.; Battersby, N.; Bhangu, A.; El-Hussuna, A.; Frasson, M.; Singh, B.; Vennix, S.; Zmora, O.; et al. The impact of stapling technique and surgeon specialism on anastomotic failure after right- sided colorectal resection: An international multicentre, prospective audit. Color. Dis. 2018, 20, 1028–1040. [Google Scholar]
- Fleetwood, V.A.; Gross, K.; Alex, G.C.; Cortina, C.S.; Smolevitz, J.B.; Sarvepalli, S.; Bakhsh, S.R.; Myers, J.A.; Singer, M.A.; Orkin, B.A. Common side closure type but not stapler brand or oversewing influences side-to-side anastomotic leak rates. J. Am. Coll. Surg. 2015, 221, 590–595. [Google Scholar] [CrossRef]
- Vasiliu, E.C.Z.; Zarnescu, N.O.; Costea, R.; Neagu, S. Review of Risk Factors for Anastomotic Leakage in Colorectal Surgery. Chirurgia 2015, 110, 319–326. [Google Scholar]
- Ozben, V.; Stocchi, L.; Ashburn, J.; Liu, X.; Gorgun, E. Impact of a restrictive vs liberal transfusion strategy on anastomotic leakage and infectious complications after restorative surgery for rectal cancer. Color. Dis. 2017, 19, 772–780. [Google Scholar] [CrossRef]
- Park, J.S.; Choi, G.-S.; Kim, S.H.; Kim, H.R.; Kim, N.K.; Lee, K.Y.; Kang, S.B.; Kim, J.Y.; Lee, K.Y.; Kim, B.C.; et al. Multicenter Analysis of Risk Factors for Anastomotic Leakage After Laparoscopic Rectal Cancer Excision. Ann. Surg. 2013, 257, 665–671. [Google Scholar] [CrossRef]
- Tartter, P.I.; Quintero, S.; Barron, D.M. Perioperative blood transfusion associated with infectious complications after colorectal cancer operations. Am. J. Surg. 1986, 152, 479–482. [Google Scholar] [CrossRef]
- Tang, R.; Chen, H.H.; Wang, Y.L.; Changchien, C.R.; Chen, J.-S.; Hsu, K.-C.; Chiang, J.-M.; Wang, J.-Y. Risk Factors for Surgical Site Infection After Elective Resection of the Colon and Rectum: A Single-Center Prospective Study of 2,809 Consecutive Patients. Ann. Surg. 2001, 234, 181–189. [Google Scholar] [CrossRef] [Green Version]
- Ydy, L.R.A.; Slhessarenko, N.; de Aguilar-Nascimento, J.E. Effect of Perioperative Allogeneic Red Blood Cell Transfusion on the Immune-Inflammatory Response After Colorectal Cancer Resection. World J. Surg. 2007, 31, 2044–2051. [Google Scholar] [CrossRef] [PubMed]
- Ford, C.D.; Vanmoorleghem, G.; Menlove, R.L. Blood transfusions and postoperative wound infection. Surgery 1993, 113, 603–607. [Google Scholar] [PubMed]
- Gibbs, J.; Cull, W.; Henderson, W.; Daley, J.; Hur, K.; Khuri, S.F. Preoperative Serum Albumin Level as a Predictor of Operative Mortality and Morbidity Results from the National VA Surgical Risk Study. Arch Surg. 1999, 134, 36–42. [Google Scholar] [CrossRef] [Green Version]
- Fuhrman, M.P.; Charney, P.; Mueller, C.M. Hepatic proteins and nutrition assessment. J. Am. Diet. Assoc. 2004, 104, 1258–1264. [Google Scholar] [CrossRef]
- Kudsk, K.; Tolley, E.; DeWitt, R.; Janu, P.; Blackwell, A.; Yeary, S.; King, B. Preoperative albumin and surgical site identify surgical risk for major postoperative complications. J. Parenter. Enter. Nutr. 2003, 27, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Kuzu, M.A.; Terzioğlu, H.; Genç, V.; Erkek, A.B.; Özban, M.; Sonyürek, P.; Elhan, A.H.; Torun, N. Preoperative Nutritional Risk Assessment in Predicting Postoperative Outcome in Patients Undergoing Major Surgery. World J. Surg. 2006, 30, 378–390. [Google Scholar] [CrossRef] [PubMed]
- Garth, A.K.; Newsome, C.M.; Simmance, N.; Crowe, T.C. Nutritional status, nutrition practices and post-operative complications in patients with gastrointestinal cancer. J. Hum. Nutr. Diet. 2010, 23, 393–401. [Google Scholar] [CrossRef]
- Lohsiriwat, V.; Lohsiriwat, D.; Boonnuch, W.; Chinswangwatanakul, V.; Akaraviputh, T.; Lert-Akayamanee, N. Pre-operative hypoalbuminemia is a major risk factor for postoperative complications following rectal cancer surgery. World J. Gastroenterol. 2008, 14, 1248–1251. [Google Scholar] [CrossRef] [PubMed]
- Lai, C.-C.; You, J.-F.; Yeh, C.-Y.; Chen, J.-S.; Tang, R.; Wang, J.-Y.; Chin, C.-C. Low preoperative serum albumin in colon cancer: A risk factor for poor outcome. Int. J. Color. Dis. 2010, 26, 473–481. [Google Scholar] [CrossRef] [PubMed]
- Irvin, T.T.; Hunt, T.K. Effect of Malnutrition on Colonic Healing. Ann. Surg. 1974, 180, 765–772. [Google Scholar] [CrossRef]
- Gonçalves, C.G.; Groth, A.K.; Ferreira, M.; Matias, J.E.F.; Coelho, J.C.U.; Campos, A.C.L. Influence of Preoperative Feeding on the Healing of Colonic Anastomoses in Malnourished Rats. J. Parenter. Enter. Nutr. 2008, 33, 83–89. [Google Scholar] [CrossRef]
- Ward, M.W.N.; Danzi, M.; Lewin, M.R.; Rennie, M.J.; Clark, C.G. The effects of subclinical malnutrition and refeeding on the healing of experimental colonic anastomoses. Br. J. Surg. 1982, 69, 308–310. [Google Scholar] [CrossRef] [PubMed]
- Shimura, T.; Toiyama, Y.; Hiro, J.; Imaoka, H.; Fujikawa, H.; Kobayashi, M.; Ohi, M.; Inoue, Y.; Mohri, Y.; Kusunoki, M. Monitoring perioperative serum albumin can identify anastomotic leakage in colorectal cancer patients with curative intent. Asian J. Surg. 2018, 41, 30–38. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| [Total] N = 188 | ||
|---|---|---|
| Age (years) (Mdn, IQR) | 73 (17) | |
| Gender (n, %) | Female | 68 (36.2) |
| Male | 120 (63.8) | |
| ASA score (n, %) | I | 5 (2.7) |
| II | 109 (58) | |
| III | 64 (34) | |
| IV | 10 (5.3) | |
| COPD (n, %) | No | 178 (94.7) |
| Yes | 10 (5.3) | |
| DM (n, %) | No | 136 (72.3) |
| Yes | 52 (27.7) | |
| HTN (n, %) | No | 61 (32.4) |
| Yes | 127 (67.6) | |
| Smoking Habits (n, %) | Non Smoker | 163 (86.7) |
| Previous Smoker | 9 (4.8) | |
| Active Smoker | 16 (8.5) | |
| BMI (Mdn, IQR) | 32.5 (72.8) | |
| Obesity (body mass index ≥ 30) (n, %) | No Yes | 125 (77.6) 36 (22.4) |
| NO AL | AL | Statistics Test | p-Value | |
|---|---|---|---|---|
| Gender (n, %) | Fisher’s exact test | >0.990 | ||
| Female | 63 (36.0) | 5 (38.5) | ||
| Male | 112 (64.0) | 8 (61.5) | ||
| Age, years (Mdn, IQR) | 73 (17) | 77 (9) | Mann–Whitney test | 0.107 |
| ASA score (n, %) | Fisher’s exact test | 0.046 | ||
| I–II | 107 (61.1) | 7 (53.8) | ||
| III | 61 (34.9) | 3 (23.1) | ||
| ≥IV | 7 (4.0) | 3 (23.1) | ||
| DM (n, %) | Fisher’s exact test | 0.009 | ||
| No | 131 (74.9) | 5 (38.5) | ||
| Yes | 44 (25.1) | 8 (61.5) | ||
| COPD (n, %) | Fisher’s exact test | 0.520 | ||
| No | 166 (94.9) | 12 (92.3) | ||
| Yes | 9 (5.1) | 1 (7.7) | ||
| Smoking habits (n, %) | Fisher’s exact test | 0.685 | ||
| Non Smoker | 152 (86.9) | 11 (84.6) | ||
| Active Smoker/Previous Smoker | 23 (13.1) | 2 (15.4) | ||
| HTN (n, %) | Fisher’s exact test | 0.553 | ||
| No | 58 (33.1) | 3 (23.1) | ||
| Yes | 117 (66.9) | 10 (76.9) | ||
| Obesity (n, %) | Fisher’s exact test | 0.685 | ||
| No | 117 (77.0) | 8 (88.9) | ||
| Yes | 35 (23.0) | 1 (11.1) | ||
| Ca 19.9 (Mdn, IQR) | 6.80 (14.40) | 5.16 (6.74) | Mann–Whitney test | 0.655 |
| CEA (Mdn, IQR) | 1.70 (2.20) | 2.30 (2.80) | Mann–Whitney test | 0.402 |
| Albumin | 4.20 (0.77) | 4.0 (0.92) | Mann–Whitney test | 0.504 |
| (g/dL) (Mdn, IQR) | ||||
| Total proteins (g/dL) (Mdn, IQR) | 7.1 (0.7) | 7.1 (1.45) | Mann–Whitney test | 0.413 |
| Haemoglobin (g/dL) (Mdn, IQR) | 12.6 (3.5) | 10.9 (2.8) | Mann–Whitney test | 0.066 |
| Glucose (g/dL) (Mdn, IQR) | 105.5 (35) | 117 (31) | Mann–Whitney test | 0.992 |
| Blood transfusion (n, %) | Fisher’s exact test | >0.990 | ||
| No | 159 (90.9) | 12 (92.3) | ||
| Yes | 16 (9.1) | 1 (7.7) |
| NO AL | AL | Statistics Test | p-Value | |
|---|---|---|---|---|
| Operating time (min) (Mdn, IQR) | 140 (60) | 120 (75) | Mann–Whitney test | 0.050 |
| Surgical approach (n, %) | Fisher’s exact test | 0.001 | ||
| Laparoscopic | 151 (86.3) | 6 (46.2) | ||
| Laparotomy/Converted to laparotomy | 24 (13.7) | 7 (53.8) | ||
| Suture Reinforcement (n, %) | Fisher’s exact test | 0.553 | ||
| No | 58 (33.1) | 3 (23.1) | ||
| Yes | 117 (66.9) | 10 (76.9) |
| NO AL | AL | Statistics Test | p-Value | |
|---|---|---|---|---|
| Length of stay (days) (Mdn, IQR) | 4.00 (2) | 11.00 (8) | Mann–Whitney test | <0.001 |
| Blood transfusion (n, %) | Fisher’s exact test | 0.005 | ||
| No | 172 (98.3) | 10 (76.9) | ||
| Yes | 3 (1.7) | 3 (23.1) | ||
| Haemoglobin (g/dL) (M, SD) | 10.38 (1.91) | 9.80 (2.17) | t-test | 0.294 |
| Albumin (g/dL) (M, SD) | 3.34 (0.57) | 2.96 (0.54) | t-test | 0.026 |
| Total proteins (g/dL) (M, SD) | 5.67 (0.57) | 5.51 (0.58) | t-test | 0.455 |
| CRP (Mdn, IQR) | 140.7 (107.8) | 171 (111.30) | Mann–Whitney test | 0.07 |
| Mortality (n, %) | Fisher’s exact test | 0.024 | ||
| No | 168 (96.0) | 10 (76.9) | ||
| Yes | 7 (4.0) | 3 (23.1) |
| Multivariate | |||||
|---|---|---|---|---|---|
| B | S.E | p-Value | OR | IC 95% | |
| Operating time (min) (Mdn, AIQ) | −0.015 | 0.007 | 0.038 | 0.985 | 0.972; 0.999 |
| Postop albumin (g/L) (M, SD) | −1.268 | 0.537 | 0.018 | 0.281 | 0.098; 0.806 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gomes, S.L.; Santos, P.M.D.d.; Costa Pereira, J.; Martins, S.F. Ileocolic Anastomosis Dehiscence in Colorectal Cancer Surgery. Gastrointest. Disord. 2023, 5, 273-286. https://doi.org/10.3390/gidisord5020022
Gomes SL, Santos PMDd, Costa Pereira J, Martins SF. Ileocolic Anastomosis Dehiscence in Colorectal Cancer Surgery. Gastrointestinal Disorders. 2023; 5(2):273-286. https://doi.org/10.3390/gidisord5020022
Chicago/Turabian StyleGomes, Sara Lima, Pedro Miguel Dias dos Santos, Joaquim Costa Pereira, and Sandra F. Martins. 2023. "Ileocolic Anastomosis Dehiscence in Colorectal Cancer Surgery" Gastrointestinal Disorders 5, no. 2: 273-286. https://doi.org/10.3390/gidisord5020022