
The Efficacy of a Multimodal Bedroom-Based ‘Smart’ Alarm System on Mitigating the Effects of Sleep Inertia
 , ,
, ,
Abstract
:1. Introduction
2. Results
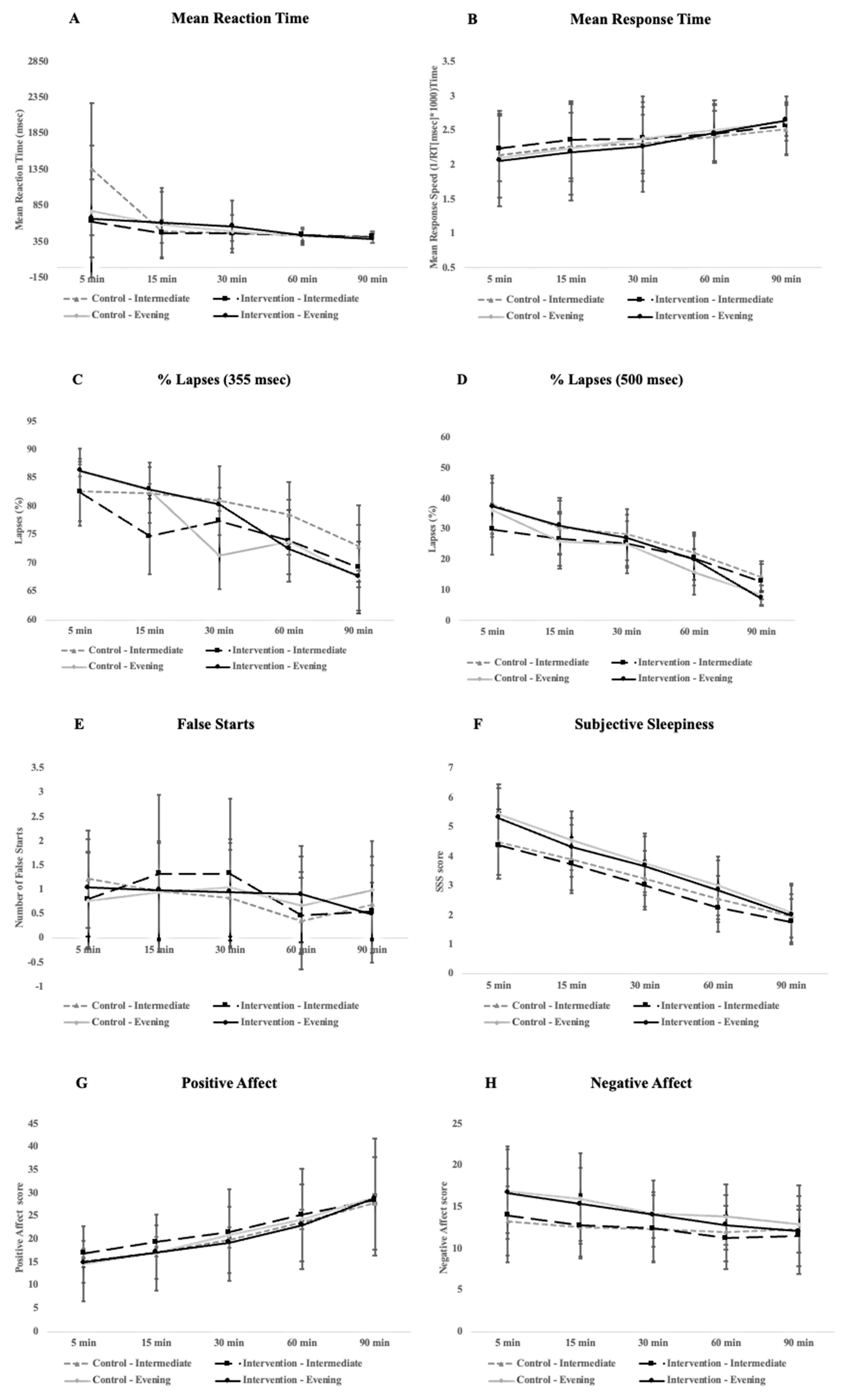
2.1. Impact of Intervention on Sleep Inertia Symptoms
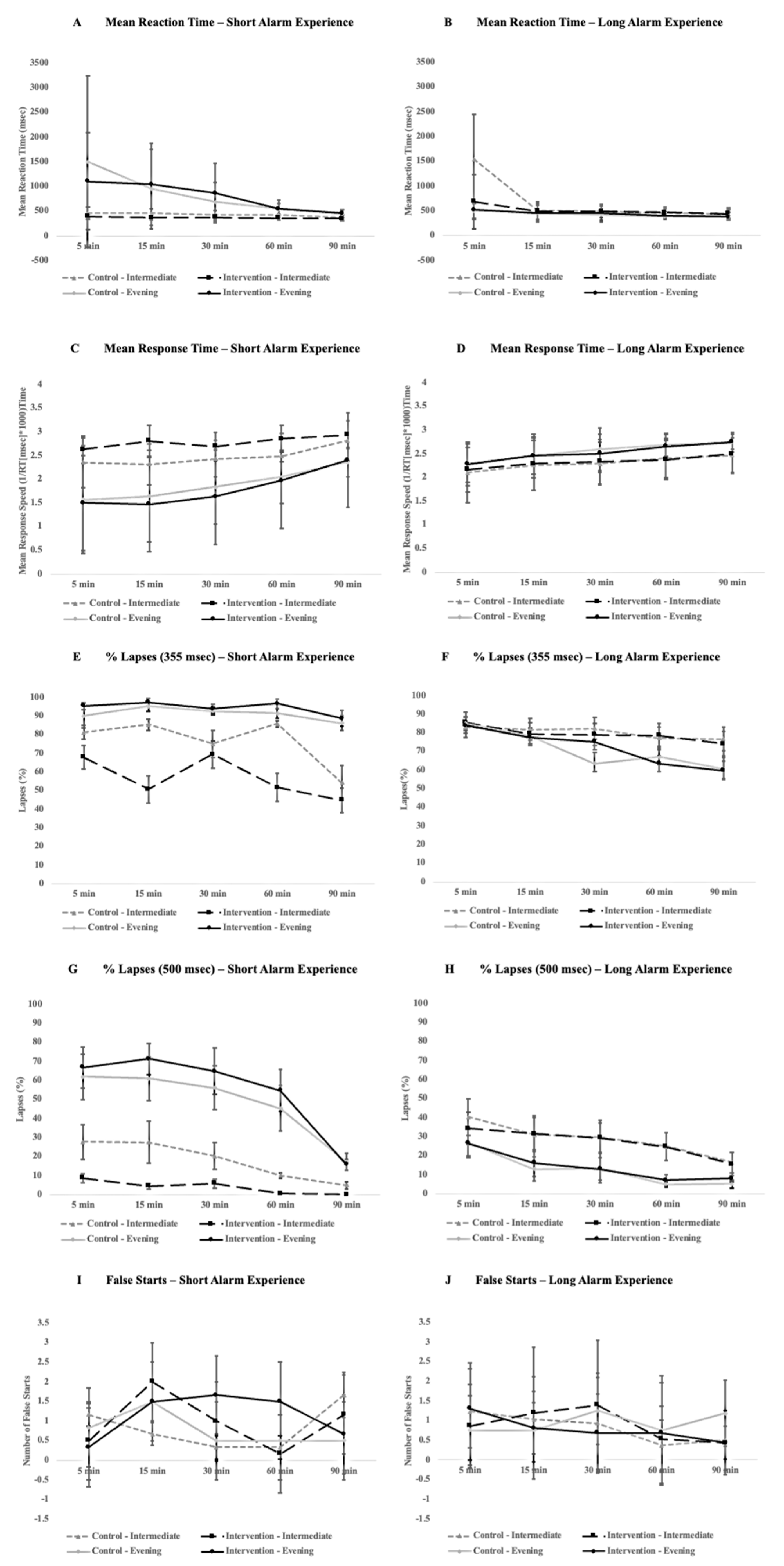
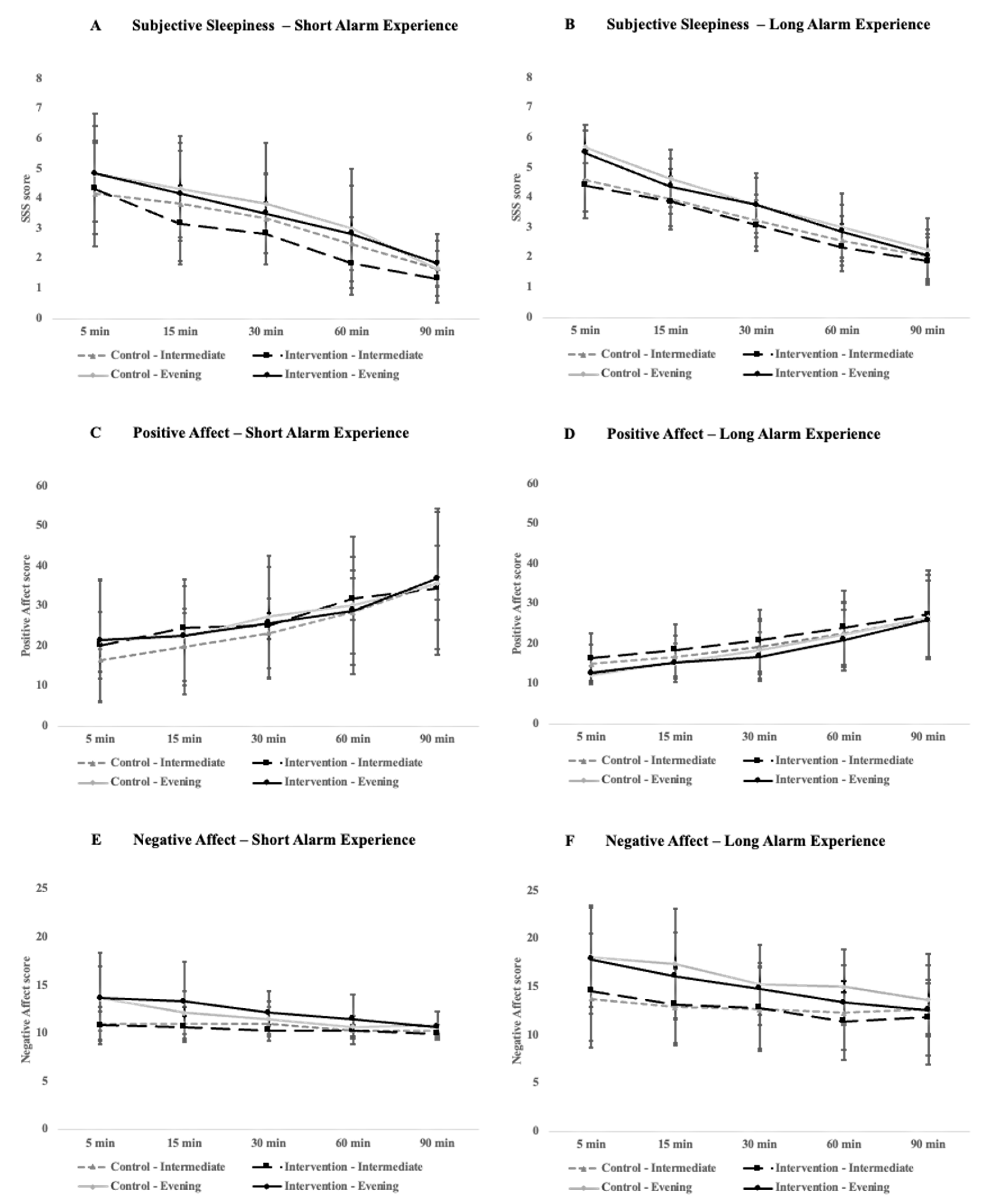
2.2. ‘Short’ vs. ‘Long’ Alarm Experience
2.3. Differences in Sleep during Each Condition
3. Discussion
4. Materials and Methods
4.1. Study Population
4.2. Overview of Study Design
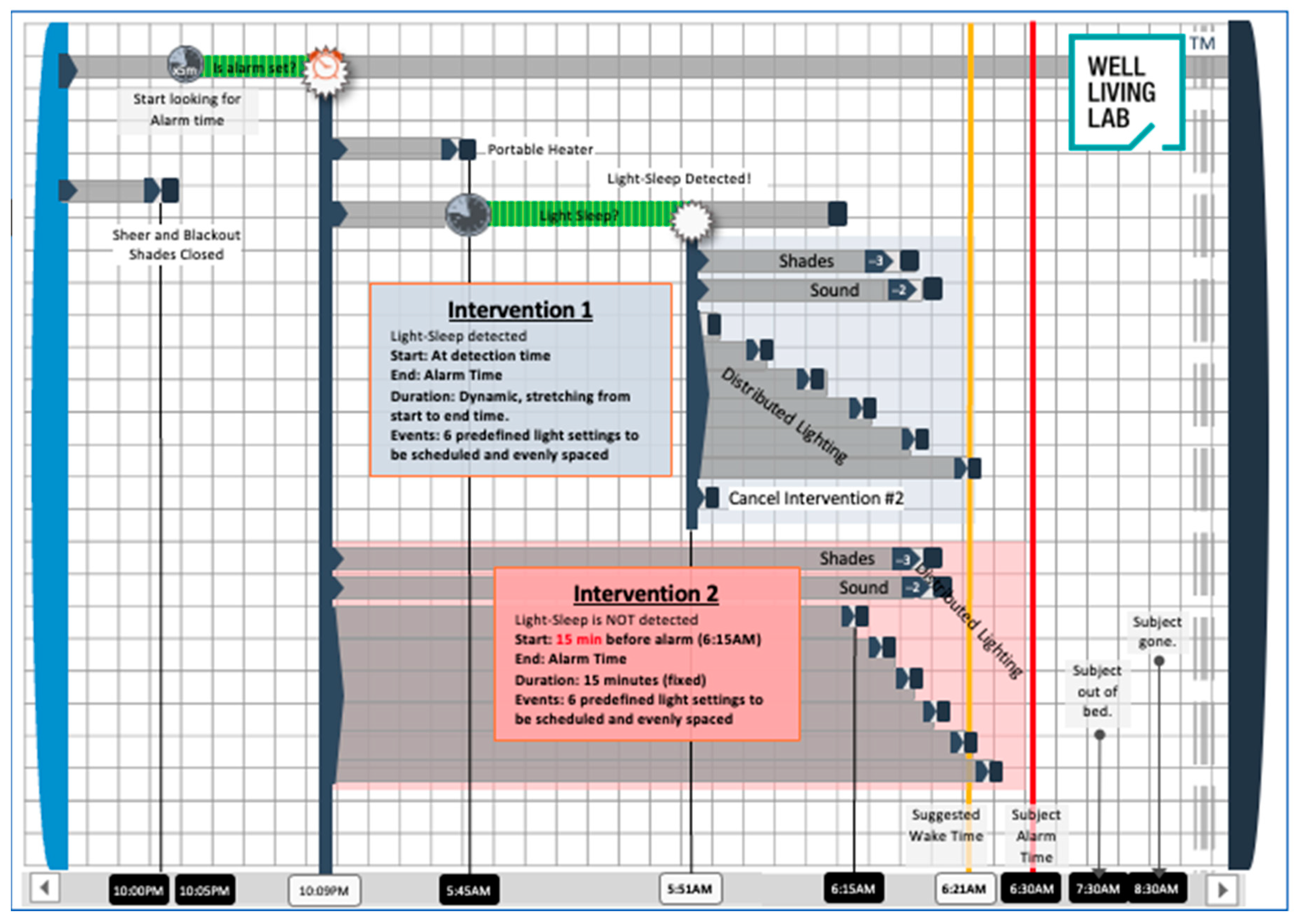
4.3. Multimodal Bedroom-Based Alarm Intervention
4.4. Cognitive Performance, Alertness, and Mood
4.5. Sleep Behaviors
4.6. Statistical Analyses
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Jeanneret, P.R.; Webb, W.B. Strength of Grip on Arousal from Full Night’s Sleep. Percept. Mot. Skills 1963, 17, 759–761. [Google Scholar] [CrossRef] [PubMed]
- Tassi, P.; Muzet, A. Sleep inertia. Sleep Med. Rev. 2000, 4, 341–353. [Google Scholar] [CrossRef]
- Signal, T.L.; van den Berg, M.J.; Mulrine, H.M.; Gander, P.H. Duration of Sleep Inertia after Napping during Simulated Night Work and in Extended Operations. Chronobiol. Int. 2012, 29, 769–779. [Google Scholar] [CrossRef]
- Dinges, D.F.; Orne, M.T.; Orne, E.C. Assessing performance upon abrupt awakening from naps during quasi-continuous operations. Behav. Res. Methods Instrum. Comput. 1985, 17, 37–45. [Google Scholar] [CrossRef]
- Dinges, D.F.; Orne, M.T.; Whitehouse, W.G.; Orne, E.C. Temporal Placement of a Nap for Alertness: Contributions of Circadian Phase and Prior Wakefulness. Sleep 1987, 10, 313–329. [Google Scholar] [CrossRef]
- Naitoh, P.; Kelly, T.; Babkoff, H. Sleep Inertia: Best Time Not to Wake Up? Chronobiol. Int. 1993, 10, 109–118. [Google Scholar] [CrossRef]
- Bruck, D.; Pisani, D.L. The effects of sleep inertia on decision-making performance. J. Sleep Res. 1999, 8, 95–103. [Google Scholar] [CrossRef]
- Brooks, A.; Lack, L. A brief afternoon nap following nocturnal sleep restriction: Which nap duration is most recuperative? Sleep 2006, 29, 831–840. [Google Scholar] [CrossRef]
- Hilditch, C.J.; Centofanti, S.A.; Dorrian, J.; Banks, S. A 30-Minute, but Not a 10-Minute Nighttime Nap is Associated with Sleep Inertia. Sleep 2016, 39, 675–685. [Google Scholar] [CrossRef]
- Rosa, R.R.; Bonnet, M.H.; Warm, J.S. Recovery of performance during sleep following sleep deprivation. Psychophysiology 1983, 20, 152–159. [Google Scholar] [CrossRef]
- Balkin, T.J.; Badia, P. Relationship between sleep inertia and sleepiness: Cumulative effects of four nights of sleep disruption/restriction on performance following abrupt nocturnal awakening. Biol. Psychol. 1988, 27, 245–258. [Google Scholar] [CrossRef]
- Miccoli, L.; Versace, F.; Koterle, S.; Cavallero, C. Comparing Sleep-Loss Sleepiness and Sleep Inertia: Lapses Make the Difference. Chronobiol. Int. 2008, 25, 725–744. [Google Scholar] [CrossRef]
- Jewett, M.E.; Wyatt, J.K.; Ritz-De Cecco, A.; Khalsa, S.B.; Dijk, D.J.; Czeisler, C.A. Time course of sleep inertia dissipation in human performance and alertness. J. Sleep Res. 1999, 8, 1–8. [Google Scholar] [CrossRef]
- Cajochen, C.; Zeitzer, J.M.; Czeisler, C.A.; Dijk, D.-J. Dose-response relationship for light intensity and ocular and electroencephalographic correlates of human alertness. Behav. Brain Res. 2000, 115, 75–83. [Google Scholar] [CrossRef] [PubMed]
- Campbell, S.S.; Dijk, D.-J.; Boulos, Z.; Eastman, C.I.; Lewy, A.J.; Terman, M. Light Treatment for Sleep Disorders: Consensus Report: III. Alerting and Activating Effects. J. Biol. Rhythms 1995, 10, 129–132. [Google Scholar] [CrossRef] [PubMed]
- Rüger, M.; Gordijn, M.C.M.; Beersma, D.G.M.; de Vries, B.; Daan, S. Acute and Phase-Shifting Effects of Ocular and Extraocular Light in Human Circadian Physiology. J. Biol. Rhythms 2003, 18, 409–419. [Google Scholar] [CrossRef] [PubMed]
- Rüger, M.; Gordijn, M.C.M.; Beersma, D.G.M.; de Vries, B.; Daan, S. Time-of-day-dependent effects of bright light exposure on human psychophysiology: Comparison of daytime and nighttime exposure. Am. J. Physiol.-Regul. Integr. Comp. Physiol. 2006, 290, R1413–R1420. [Google Scholar] [CrossRef] [PubMed]
- Gordijn, M.C.M.; Beersma, D.G.M.; Korte, H.J.; Hoofdakker, R.H.V.D. Effects of light exposure and sleep displacement on dim light melatonin onset. J. Sleep Res. 1999, 8, 163–174. [Google Scholar] [CrossRef] [PubMed]
- Honma, K.; Honma, S. Circabidian rhythm: Its appearance and disappearance in association with a bright light pulse. Experientia 1988, 44, 981–983. [Google Scholar] [CrossRef] [PubMed]
- Khalsa, S.B.S.; Jewett, M.E.; Cajochen, C.; Czeisler, C.A. A Phase Response Curve to Single Bright Light Pulses in Human Subjects. J. Physiol. 2003, 549, 945–952. [Google Scholar] [CrossRef]
- Minors, D.S.; Waterhouse, J.M.; Wirz-Justice, A. A human phase-response curve to light. Neurosci. Lett. 1991, 133, 36–40. [Google Scholar] [CrossRef]
- Duffy, J.F.; Zitting, K.-M.; Czeisler, C.A. The Case for Addressing Operator Fatigue. Rev. Hum. Factors Ergon. 2015, 10, 29–78. [Google Scholar] [CrossRef]
- Horne, J.; Moseley, R. Sudden early-morning awakening impairs immediate tactical planning in a changing ‘emergency’ scenario. J. Sleep Res. 2011, 20, 275–278. [Google Scholar] [CrossRef]
- Rosekind, M.R.; Smith, R.M.; Miller, D.L.; Co, E.L.; Gregory, K.B.; Webbon, L.L.; Gander, P.H.; Lebacqz, J.V. Alertness management: Strategic naps in operational settings. J. Sleep Res. 1995, 4, 62–66. [Google Scholar] [CrossRef]
- Smith-Coggins, R.; Howard, S.K.; Mac, D.T.; Wang, C.; Kwan, S.; Rosekind, M.R.; Sowb, Y.; Balise, R.; Levis, J.; Gaba, D.M. Improving Alertness and Performance in Emergency Department Physicians and Nurses: The Use of Planned Naps. Ann. Emerg. Med. 2006, 48, 596–604.e3. [Google Scholar] [CrossRef]
- Reyner, L.A.; Horne, J.A. Suppression of sleepiness in drivers: Combination of caffeine with a short nap. Psychophysiology 1997, 34, 721–725. [Google Scholar] [CrossRef]
- Van Dongen, H.P.; Price, N.J.; Mullington, J.M.; Szuba, M.P.; Kapoor, S.C.; Dinges, D.F. Caffeine eliminates psychomotor vigilance deficits from sleep inertia. Sleep 2001, 24, 813–819. [Google Scholar] [CrossRef]
- Newman, R.A.; Kamimori, G.H.; Wesensten, N.J.; Picchioni, D.; Balkin, T.J. Caffeine Gum Minimizes Sleep Inertia. Percept. Mot. Skills 2013, 116, 280–293. [Google Scholar] [CrossRef]
- Hayashi, M.; Masuda, A.; Hori, T. The alerting effects of caffeine, bright light and face washing after a short daytime nap. Clin. Neurophysiol. Off. J. Int. Fed. Clin. Neurophysiol. 2003, 114, 2268–2278. [Google Scholar] [CrossRef]
- Figueiro, M.G.; Sahin, L.; Roohan, C.; Kalsher, M.; Plitnick, B.; Rea, M.S. Effects of red light on sleep inertia. Nat. Sci. Sleep 2019, 11, 45–57. [Google Scholar] [CrossRef]
- Giménez, M.C.; Hessels, M.; van de Werken, M.; de Vries, B.; Beersma, D.G.M.; Gordijn, M.C.M. Effects of Artificial Dawn on Subjective Ratings of Sleep Inertia and Dim Light Melatonin Onset. Chronobiol. Int. 2010, 27, 1219–1241. [Google Scholar] [CrossRef]
- Hilditch, C.J.; Wong, L.R.; Bathurst, N.G.; Feick, N.H.; Pradhan, S.; Santamaria, A.; Shattuck, N.L.; Flynn-Evans, E.E. Rise and shine: The use of polychromatic short-wavelength-enriched light to mitigate sleep inertia at night following awakening from slow-wave sleep. J. Sleep Res. 2022, 31, e13558. [Google Scholar] [CrossRef]
- Hilditch, C.J.; Pradhan, S.; Costedoat, G.; Bathurst, N.G.; Glaros, Z.; Gregory, K.B.; Shattuck, N.L.; Flynn-Evans, E.E. An at-home evaluation of a light intervention to mitigate sleep inertia symptoms. Sleep Health 2023, in press. [Google Scholar] [CrossRef]
- Hayashi, M.; Uchida, C.; Shoji, T.; Hori, T. The effects of the preference for music on sleep inertia after a short daytime nap. Sleep Biol. Rhythms 2004, 2, 184–191. [Google Scholar] [CrossRef]
- McFarlane, S.J.; Garcia, J.E.; Verhagen, D.S.; Dyer, A.G. Alarm tones, music and their elements: Analysis of reported waking sounds to counteract sleep inertia. PLoS ONE 2020, 15, e0215788. [Google Scholar] [CrossRef]
- Tassi, P.; Nicolas, A.; Dewasmes, G.; Eschenlauer, R.; Ehrhart, J.; Salame, P.; Muzet, A.; Libert, J.P. Effects of noise on sleep inertia as a function of circadian placement of a one-hour nap. Percept. Mot. Skills 1992, 75, 291–302. [Google Scholar] [CrossRef]
- Kräuchi, K.; Cajochen, C.; Wirz-Justice, A. Waking up properly: Is there a role of thermoregulation in sleep inertia? J. Sleep Res. 2004, 13, 121–127. [Google Scholar] [CrossRef]
- Kräuchi, K.; Knoblauch, V.; Wirz-Justice, A.; Cajochen, C. Challenging the sleep homeostat does not influence the thermoregulatory system in men: Evidence from a nap vs. sleep-deprivation study. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2006, 290, R1052–R1061. [Google Scholar] [CrossRef]
- Lewy, A.; Wehr, T.; Goodwin, F.; Newsome, D.; Markey, S. Light suppresses melatonin secretion in humans. Science 1981, 210, 1267–1269. [Google Scholar] [CrossRef]
- Wahnschaffe, A.; Haedel, S.; Rodenbeck, A.; Stoll, C.; Rudolph, H.; Kozakov, R.; Schoepp, H.; Kunz, D. Out of the Lab and into the Bathroom: Evening Short-Term Exposure to Conventional Light Suppresses Melatonin and Increases Alertness Perception. Int. J. Mol. Sci. 2013, 14, 2573–2589. [Google Scholar] [CrossRef]
- Werken, M.V.D.; Giménez, M.C.; Vries, B.D.; Beersma, D.G.M.; Someren, E.J.W.V.; Gordijn, M.C.M. Effects of artificial dawn on sleep inertia, skin temperature, and the awakening cortisol response. J. Sleep Res. 2010, 19, 425–435. [Google Scholar] [CrossRef]
- Wilkinson, R.T.; Stretton, M. Performance after awakening at different times of night. Psychon. Sci. 1971, 23, 283–285. [Google Scholar] [CrossRef]
- Dinges, D.F. Are you awake? Cognitive performance and reverie during the hypnopompic state. In Sleep and Cognition; American Psychological Association: Washington, DC, USA, 1990; pp. 159–175. ISBN 978-1-55798-083-0. [Google Scholar]
- Hilditch, C.J.; McHill, A.W. Sleep inertia: Current insights. Nat. Sci. Sleep 2019, 11, 155–165. [Google Scholar] [CrossRef]
- Lok, R.; Smolders, K.C.H.J.; Beersma, D.G.M.; de Kort, Y.A.W. Light, Alertness, and Alerting Effects of White Light: A Literature Overview. J. Biol. Rhythms 2018, 33, 589–601. [Google Scholar] [CrossRef]
- Souman, J.L.; Tinga, A.M.; Te Pas, S.F.; Van Ee, R.; Vlaskamp, B.N.S. Acute alerting effects of light: A systematic literature review. Behav. Brain Res. 2018, 337, 228–239. [Google Scholar] [CrossRef]
- Hirose, A.; Nagasaka, A. The Effects of the Level of Alertness during the Rest Period on Subsequent Performance. Int. J. Occup. Saf. Ergon. 2003, 9, 479–490. [Google Scholar] [CrossRef]
- Ritchie, H.K.; Burke, T.M.; Dear, T.B.; Mchill, A.W.; Axelsson, J.; Wright, K.P. Impact of sleep inertia on visual selective attention for rare targets and the influence of chronotype. J. Sleep Res. 2017, 26, 551–558. [Google Scholar] [CrossRef]
- Terman, M.; Schlager, D.; Fairhurst, S.; Perlman, B. Dawn and dusk simulation as a therapeutic intervention. Biol. Psychiatry 1989, 25, 966–970. [Google Scholar] [CrossRef]
- Noguchi, H.; Sakaguchi, T.; Shirakawa, S.; Komada, Y. Effects of Simulated Dawn Lighting on Awakening. J. Illum. Eng. Soc. 2001, 30, 49–56. [Google Scholar] [CrossRef]
- Thompson, A.; Jones, H.; Gregson, W.; Atkinson, G. Effects of dawn simulation on markers of sleep inertia and post-waking performance in humans. Eur. J. Appl. Physiol. 2014, 114, 1049–1056. [Google Scholar] [CrossRef]
- Thorn, L.; Hucklebridge, F.; Esgate, A.; Evans, P.; Clow, A. The effect of dawn simulation on the cortisol response to awakening in healthy participants. Psychoneuroendocrinology 2004, 29, 925–930. [Google Scholar] [CrossRef] [PubMed]
- Ko, P.-R.T.; Kientz, J.A.; Choe, E.K.; Kay, M.; Landis, C.A.; Watson, N.F. Consumer Sleep Technologies: A Review of the Landscape. J. Clin. Sleep Med. JCSM Off. Publ. Am. Acad. Sleep Med. 2015, 11, 1455–1461. [Google Scholar] [CrossRef]
- Viola, A.U.; Gabel, V.; Chellappa, S.L.; Schmidt, C.; Hommes, V.; Tobaldini, E.; Montano, N.; Cajochen, C. Dawn simulation light: A potential cardiac events protector. Sleep Med. 2015, 16, 457–461. [Google Scholar] [CrossRef]
- Santhi, N.; Groeger, J.A.; Archer, S.N.; Gimenez, M.; Schlangen, L.J.M.; Dijk, D.-J. Morning Sleep Inertia in Alertness and Performance: Effect of Cognitive Domain and White Light Conditions. PLoS ONE 2013, 8, e79688. [Google Scholar] [CrossRef]
- Kakitsuba, N.; White, M.D. Effect of change in ambient temperature on core temperature during the daytime. Int. J. Biometeorol. 2014, 58, 901–907. [Google Scholar] [CrossRef]
- Basner, M.; Dinges, D.F. Maximizing Sensitivity of the Psychomotor Vigilance Test (PVT) to Sleep Loss. Sleep 2011, 34, 581–591. [Google Scholar] [CrossRef]
- Kanady, J.; Harvey, A. Development and Validation of the Sleep Inertia Questionnaire (SIQ) and Assessment of Sleep Inertia in Analogue and Clinical Depression. Cogn. Ther. Res. 2015, 39. [Google Scholar] [CrossRef]
- Dinges, D.F.; Pack, F.; Williams, K.; Gillen, K.A.; Powell, J.W.; Ott, G.E.; Aptowicz, C.; Pack, A.I. Cumulative Sleepiness, Mood Disturbance, and Psychomotor Vigilance Performance Decrements during a Week of Sleep Restricted to 4–5 Hours per Night. Sleep 1997, 20, 267–277. [Google Scholar] [CrossRef]
- Drummond, S.P.A.; Bischoff-Grethe, A.; Dinges, D.F.; Ayalon, L.; Mednick, S.C.; Meloy, M.J. The neural basis of the psychomotor vigilance task. Sleep 2005, 28, 1059–1068. [Google Scholar]
- Jung, C.M.; Ronda, J.M.; Czeisler, C.A.; Wright, K.P., Jr. Comparison of sustained attention assessed by auditory and visual psychomotor vigilance tasks prior to and during sleep deprivation. J. Sleep Res. 2011, 20, 348–355. [Google Scholar] [CrossRef]
- Basner, M.; Rubinstein, J. Fitness for duty: A 3 minute version of the Psychomotor Vigilance Test predicts fatigue related declines in luggage screening performance. J. Occup. Environ. Med. Am. Coll. Occup. Environ. Med. 2011, 53, 1146–1154. [Google Scholar] [CrossRef]
- Grant, D.A.; Honn, K.A.; Layton, M.E.; Riedy, S.M.; Van Dongen, H.P.A. 3-minute smartphone-based and tablet-based psychomotor vigilance tests for the assessment of reduced alertness due to sleep deprivation. Behav. Res. Methods 2017, 49, 1020–1029. [Google Scholar] [CrossRef] [PubMed]
- Matsangas, P.; Shattuck, N.L.; Mortimore, K.; Paghasian, C.; Greene, F. The 3-minute Psychomotor Vigilance Task (PVT) Embedded in a Wrist-worn Device: Time of Day Effects. Proc. Hum. Factors Ergon. Soc. Annu. Meet. 2019, 63, 797–801. [Google Scholar] [CrossRef]
- Matsangas, P.; Shattuck, N.L. Agreement between the 3-minute Psychomotor Vigilance Task (PVT) Embedded in a Wrist-worn Device and the Laptop-based PVT. Proc. Hum. Factors Ergon. Soc. Annu. Meet. 2018, 62, 666–670. [Google Scholar] [CrossRef]
- Watson, D.; Anna, L.; Tellegen, A. Development and Validation of Brief Measures of Positive and Negative Affect: The PANAS Scales. J. Pers. Soc. Psychol. 1988, 54, 81063–81070. [Google Scholar] [CrossRef]
- Hoddes, E.; Zarcone, V.; Smythe, H.; Phillips, R.; Dement, W.C. Quantification of Sleepiness: A New Approach. Psychophysiology 1973, 10, 431–436. [Google Scholar] [CrossRef]
- Horne, J.A.; Östberg, O. A self-assessment questionnaire to determine morningness-eveningness in human circadian rhythms. Int. J. Chronobiol. 1976, 4, 97–110. [Google Scholar]
- Buysse, D.J.; Reynolds III, C.F.; Monk, T.H.; Hoch, C.C.; Yeager, A.L.; Kupfer, D.J. Quantification of subjective sleep quality in healthy elderly men and women using the Pittsburgh Sleep Quality Index (PSQI). Sleep 1991, 14, 331–338. [Google Scholar]
- Chinoy, E.D.; Cuellar, J.A.; Huwa, K.E.; Jameson, J.T.; Watson, C.H.; Bessman, S.C.; Hirsch, D.A.; Cooper, A.D.; Drummond, S.P.A.; Markwald, R.R. Performance of seven consumer sleep-tracking devices compared with polysomnography. Sleep 2020, 44, zsaa291. [Google Scholar] [CrossRef]
- Tal, A.; Shinar, Z.; Shaki, D.; Codish, S.; Goldbart, A. Validation of Contact-Free Sleep Monitoring Device with Comparison to Polysomnography. J. Clin. Sleep Med. JCSM Off. Publ. Am. Acad. Sleep Med. 2017, 13, 517–522. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Control | Intervention | p-Value | |
|---|---|---|---|
| Sleep Duration (min) | 396.41 (47.37) | 402.45 (73.67) | 0.642 |
| Time in Bed (min) | 459.19 (67.42) | 478.44 (75.44) | 0.258 |
| Sleep Onset | 22:38 (76.55 min) | 22:29 (90.54 min) | 0.541 |
| Sleep Onset Latency (min) | 29.78 (16.43) | 34.77 (22.18) | 0.287 |
| Wake Time | 6:18 (80.89 min) | 6:19 (79.59 min) | 0.909 |
| WASO (min) | 52.42 (41.98) | 64.79 (60.76) | 0.065 |
| Sleep Efficiency (%) | 86.65 (5.93) | 83.97 (10.18) | 0.042 * |
| All Recruited Participants | |
|---|---|
| N = 37 | Mean (SD) |
| Age | 27.13 (3.97) |
| Gender Chronotype | 19 females |
| Intermediate | 24 |
| Moderate evening | 13 |
| PSQI | 6.87 (2.65) |
| Usable participants after excluding for technical malfunctions | |
| N = 29 | Mean (SD) |
| Age | 27.00 (3.24) |
| Gender Chronotype | 14 females |
| Intermediate | 18 |
| Moderate evening | 11 |
| PSQI | 6.90 (2.68) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Campanella, C.; Byun, K.; Senerat, A.; Li, L.; Zhang, R.; Aristizabal, S.; Porter, P.; Bauer, B. The Efficacy of a Multimodal Bedroom-Based ‘Smart’ Alarm System on Mitigating the Effects of Sleep Inertia. Clocks & Sleep 2024, 6, 183-199. https://doi.org/10.3390/clockssleep6010013
Campanella C, Byun K, Senerat A, Li L, Zhang R, Aristizabal S, Porter P, Bauer B. The Efficacy of a Multimodal Bedroom-Based ‘Smart’ Alarm System on Mitigating the Effects of Sleep Inertia. Clocks & Sleep. 2024; 6(1):183-199. https://doi.org/10.3390/clockssleep6010013
Chicago/Turabian StyleCampanella, Carolina, Kunjoon Byun, Araliya Senerat, Linhao Li, Rongpeng Zhang, Sara Aristizabal, Paige Porter, and Brent Bauer. 2024. "The Efficacy of a Multimodal Bedroom-Based ‘Smart’ Alarm System on Mitigating the Effects of Sleep Inertia" Clocks & Sleep 6, no. 1: 183-199. https://doi.org/10.3390/clockssleep6010013