Impacts of Australian Firefighters’ On-Call Work Arrangements on the Sleep of Partners

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Procedures
2.2. Participants and Recruitment
2.3. Measures
2.4. Demographic Questions
2.5. Sleep Quantity and Quality
2.6. On-Call Sleep Disturbances
2.7. Relationship Happiness
2.8. Statistical Analysis
- Partner’s firefighting role (‘very much like’/’somewhat want’ my partner to give up role/’neutral’, and ‘somewhat’/’very much like my partner to continue’);
- Rating of sleep when partner is (a) not called and (b) is called (‘very poor’/’rather poor’ and ‘neither poor nor good’/’rather good’/’very good’);
- Ease of returning to sleep a) following a call and b) when partner returns from callout (‘strongly agree’/’agree’/’neither agree nor disagree’ and ‘disagree’/’strongly disagree’);
- Time taken to fall asleep (<30 min or >30 min) and;
- Hours of sleep (<7 h and >7 h).
3. Results
3.1. Demographics
3.2. Sleep Related to Calls
3.3. Habitual Sleep
3.4. Research Questions
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| DAS-7 | Dyadic Adjustment Scale |
| DOAJ | Directory of open access journals |
| MDPI | Multidisciplinary Digital Publishing Institute |
| PSQI | Pittsburgh Sleep Quality Index |
| QFES | Queensland Fire and Emergency Services |
| RQ | Research question |
References
- Australian Bureau of Statistics. Characteristics of Employment (cat. no. 6333.0). 2016. Available online: https://www.abs.gov.au/AUSSTATS/abs@.nsf/DetailsPage/6333.0August%202016?OpenDocument (accessed on 29 January 2020).
- Golden, L. Irregular work scheduling and its consequences. EPI Briefing Paper #394. 2015. Available online: https://www.epi.org/publication/irregular-work-scheduling-and-its-consequences/ (accessed on 29 January 2020).
- Parent-Thirion, A.; Vermeylen, G.; Van Houten, G.; Lyly-Yrjänäinen, M.; Biletta, I.; Cabrita, J.; Niedhammer, I. Fifth European Working Conditions Survey. Publications Office of the European Union, Luxembourg. 2012. Available online: https://www.eurofound.europa.eu/publications/report/2012/working-conditions/fifth-european-working-conditions-survey-overview-report (accessed on 29 January 2020).
- Nicol, A.M.; Botterill, J.S. On-call work and health: A review. Environ. Health 2004, 3, 15. [Google Scholar] [CrossRef] [Green Version]
- Vincent, G.E.; Jay, S.M.; Preece, H.; Hall, S.J.; Aisbett, B.; Baumert, M.; Sprajcer, M.; Lack, L.; Ferguson, S.A. Overnight heart rate variability and next day cortisol response during simulated on-call conditions. Psychoneuroendocrinology 2019, 109, 104406. [Google Scholar] [CrossRef]
- Kovac, K.; Vincent, G.E.; Jay, S.M.; Sprajcer, M.; Aisbett, B.; Lack, L.; Ferguson, S.A. The impact of anticipating a stressful task on sleep inertia when on-call. Appl. Ergon. 2020, 82, 102942. [Google Scholar] [CrossRef]
- Perrin, S.; Jay, S.; Vincent, G.; Sprajcer, M.; Lack, L.; Ferguson, S.; Vakulin, A. Waking qEEG to assess psychophysiological stress and alertness during simulated on-call conditions. Int. J. Psychophysiol. 2019, 141, 93–100. [Google Scholar] [CrossRef] [PubMed]
- Sprajcer, M.; Jay, S.M.; Vincent, G.E.; Vakulin, A.; Lack, L.; Ferguson, S.A. The effects of anticipating a high-stress task on sleep and performance during simulated on-call work. J. Sleep Res. 2018, e12691. [Google Scholar] [CrossRef] [Green Version]
- Hall, S.J.; Ferguson, S.A.; Turner, A.I.; Robertson, S.J.; Vincent, G.E.; Aisbett, B. The effect of working on-call on stress physiology and sleep: A systematic review. Sleep Med. Rev. 2017, 33, 79–87. [Google Scholar] [CrossRef] [Green Version]
- van de Ven, H.A.; Bültmann, U.; de Looze, M.P.; Koolhaas, W.; Kantermann, T.; Brouwer, S.; van der Klink, J.J.L. Need for recovery among male technical distal on-call workers. Ergonomics 2015, 58, 1927–1938. [Google Scholar] [CrossRef] [PubMed]
- Torsvall, L.; Åkerstedt, T. Disturbed sleep while being on-call: An EEG study of ships’ engineers. Sleep 1988, 11, 35–38. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sprajcer, M.; Jay, S.M.; Vincent, G.E.; Vakulin, A.; Lack, L.; Ferguson, S.A. How the chance of missing the alarm during an on-call shift affects pre-bed anxiety, sleep and next day cognitive performance. Biol. Psychol. 2018, 137, 133–139. [Google Scholar] [CrossRef]
- Sprajcer, M.; Jay, S.M.; Vincent, G.E.; Vakulin, A.; Lack, L.; Ferguson, S.A. Uncertain call likelihood negatively affects sleep and next-day cognitive performance while on-call in a laboratory environment. Chronobiol. Int. 2018, 35, 838–848. [Google Scholar] [CrossRef]
- Vincent, G.E.; Kinchin, I.; Ferguson, S.A.; Jay, S.M. The Cost of Inadequate Sleep among On-Call Workers in Australia: A Workplace Perspective. Int. J. Environ. Res. Public Health 2018, 15, 398. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Troxel, W.M. It’s more than sex: Exploring the dyadic nature of sleep and implications for health. Psychosom. Med. 2010, 72, 578. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Adams, R.J.; Appleton, S.L.; Taylor, A.W.; Gill, T.K.; Lang, C.; McEvoy, R.D.; Antic, N.A. Sleep health of Australian adults in 2016: Results of the 2016 Sleep Health Foundation national survey. Sleep Health. 2017, 3, 35–42. [Google Scholar] [CrossRef] [PubMed]
- Fillo, J.; Holliday, S.B.; DeSantis, A.; Germain, A.; Buysse, D.J.; Matthews, K.A.; Troxel, W.M. Observed relationship behaviors and sleep in military veterans and their partners. Ann. Behav. Med. 2017, 51, 879–889. [Google Scholar] [CrossRef] [PubMed]
- Troxel, W.M.; Robles, T.F.; Hall, M.; Buysse, D.J. Marital quality and the marital bed: Examining the covariation between relationship quality and sleep. Sleep Med. Rev. 2007, 11, 389–404. [Google Scholar] [CrossRef] [Green Version]
- Yang, H.-C.; Suh, S.; Kim, H.; Cho, E.R.; Lee, S.K.; Shin, C. Testing bidirectional relationships between marital quality and sleep disturbances: A 4-year follow-up study in a Korean cohort. J. Psychosom. Res. 2013, 74, 401–406. [Google Scholar] [CrossRef]
- Karan, S.M.; Vincent, G.E.; Ferguson, S.A.; Jay, S.M. The Impact of on-Call Work for Partners’ Sleep, Relationship Quality and Daytime Functioning. Clocks & Sleep 2019, 1, 185–192. [Google Scholar]
- Banks, S.; Dinges, D.F. Behavioral and physiological consequences of sleep restriction. J. Clin. Sleep Med. 2007, 3, 519–528. [Google Scholar] [CrossRef] [Green Version]
- Kecklund, G.; Axelsson, J. Health consequences of shift work and insufficient sleep. BMJ 2016, 355, i5210. [Google Scholar] [CrossRef]
- Larsen, B.; Snow, R.; Vincent, G.; Tran, J.; Wolkow, A.; Aisbett, B. Multiple days of heat exposure on firefighters’ work performance and physiology. PLoS ONE 2015, 10, e0136413. [Google Scholar] [CrossRef] [Green Version]
- Vincent, G.E.; Ridgers, N.D.; Ferguson, S.A.; Aisbett, B.J.E. Associations between firefighters’ physical activity across multiple shifts of wildfire suppression. Ergonomics 2016, 59, 924–931. [Google Scholar] [CrossRef] [PubMed]
- Wolkow, A.; Ferguson, S.A.; Vincent, G.E.; Larsen, B.; Aisbett, B.; Main, L.C. The impact of sleep restriction and simulated physical firefighting work on acute inflammatory stress responses. PLoS ONE 2015, 10, e0138128. [Google Scholar] [CrossRef] [PubMed]
- Vincent, G.E.; Aisbett, B.; Hall, S.J.; Ferguson, S.A. Sleep quantity and quality is not compromised during planned burn shifts of less than 12 h. Chronobiol. Int. 2016, 33, 657–666. [Google Scholar] [CrossRef] [PubMed]
- Vincent, G.E.; Aisbett, B.; Wolkow, A.; Jay, S.M.; Ridgers, N.D.; Ferguson, S.A. Sleep in wildland firefighters: What do we know and why does it matter? Int. J. Wildland Fire 2018, 27, 73–84. [Google Scholar] [CrossRef]
- Vincent, G.; Aisbett, B.; Larsen, B.; Ridgers, N.; Snow, R.; Ferguson, S. The impact of heat exposure and sleep restriction on firefighters’ work performance and physiology during simulated wildfire suppression. Int. J. Environ. Res. Public Health. 2017, 14, 180. [Google Scholar] [CrossRef] [Green Version]
- Vincent, G.E.; Ferguson, S.; Larsen, B.; Ridgers, N.D.; Snow, R.; Aisbett, B. Adding sleep restriction to the equation: Impact on wildland firefighters’ work performance and physiology in hot conditions. Int. Arch. Occup. Environ. Health. 2018, 91, 601–611. [Google Scholar] [CrossRef]
- Cvirn, M.A.; Dorrian, J.; Smith, B.P.; Jay, S.M.; Vincent, G.E.; Ferguson, S.A. The sleep architecture of Australian volunteer firefighters during a multi-day simulated wildfire suppression: Impact of sleep restriction and temperature. Accid. Anal. Prev. 2017, 99, 389–394. [Google Scholar]
- Paterson, J.L.; Aisbett, B.; Ferguson, S.A. Sound the alarm: Health and safety risks associated with alarm response for salaried and retained metropolitan firefighters. Saf. Sci. 2016, 82, 174–181. [Google Scholar] [CrossRef]
- Cowlishaw, S.; Evans, L.; McLennan, J. Work–family conflict and crossover in volunteer emergency service workers. Work. Stress 2010, 24, 342–358. [Google Scholar] [CrossRef]
- Kelly, W.E.; Forbes, A. Temporal stability of the Sleep Disturbance Ascribed to Worry Scale. Percept. Mot. Ski. 2004, 99, 628. [Google Scholar] [CrossRef]
- Åkerstedt, T.; Kecklund, G.; Axelsson, J. Impaired sleep after bedtime stress and worries. Biol. Psychol. 2007, 76, 170–173. [Google Scholar] [CrossRef] [PubMed]
- Jay, S.M.; Paterson, J.L.; Aisbett, B.; Ferguson, S.A. No rest for the women: Understanding the impact of on-call work for women in the emergency services. Chronobiol. Int. 2018, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Roberts, B.; Vincent, G.E.; Ferguson, S.A.; Reynolds, A.C.; Jay, S.M. Understanding the differing impacts of on-call work for males and females: Results from an online survey. Int. J. Environ. Res. Public Health 2019, 16, 370. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Evans, J.R.; Mathur, A. The value of online surveys. Internet Res. 2005, 15, 195–219. [Google Scholar] [CrossRef]
- Buysse, D.J.; Reynolds, C.F., 3rd; Monk, T.H.; Berman, S.R.; Kupfer, D.J. The Pittsburgh Sleep Quality Index: A new instrument for psychiatric practice and research. Psychiatry Res. 1989, 28, 193–213. [Google Scholar] [CrossRef]
- Schlarb, A.; Claßen, M.; Schuster, E.-S.; Neuner, F.; Hautzinger, M.J.H. Did You Sleep Well, Darling?—Link between Sleep Quality and Relationship Quality. Health 2015, 7, 1747–1756. [Google Scholar] [CrossRef] [Green Version]
- Smith, M.T.; Wegener, S.T. Measures of sleep: The insomnia severity index, medical outcomes study (MOS) sleep scale, Pittsburgh sleep diary (PSD), and Pittsburgh sleep quality index (PSQI). Arthritis Care & Res. 2003, 49, S184–S196. [Google Scholar]
- Sharpley, C.F.; Rogers, H.J. Preliminary validation of the Abbreviated Spanier Dyadic Adjustment Scale: Some psychometric data regarding a screening test of marital adjustment. Educ. Psychol. Meas. 1984, 44, 1045–1049. [Google Scholar] [CrossRef]
- R Development Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2008. [Google Scholar]
- Rout, U. Stress among general practitioners and their spouses: A qualitative study. Br. J. Gen. Pract. 1996, 46, 157–160. [Google Scholar]
- Knutson, K.L. Sleep duration and cardiometabolic risk: A review of the epidemiologic evidence. Best Pract. Res. Clin. Endocrinol. Metab. 2010, 24, 731–743. [Google Scholar] [CrossRef] [Green Version]
- Schmid, S.M.; Hallschmid, M.; Schultes, B. The metabolic burden of sleep loss. Lancet Diabetes Endocrinol. 2015, 3, 52–62. [Google Scholar] [CrossRef]
- Cappuccio, F.P.; D’Elia, L.; Strazzullo, P.; Miller, M.A. Sleep duration and all-cause mortality: A systematic review and meta-analysis of prospective studies. Sleep 2010, 33, 585–592. [Google Scholar] [CrossRef] [PubMed]
- Qu, L.; Knight, K.; Higgins, D. Same-sex couples families in Australia. Available online: https://aifs.gov.au/publications/same-sex-couple-families-Australia (accessed on 2 July 2019).
- Ward, T.C.S. Reasons for mother–infant bed-sharing: A systematic narrative synthesis of the literature and implications for future research. Matern. Child Health J. 2015, 19, 675–690. [Google Scholar] [CrossRef] [PubMed]
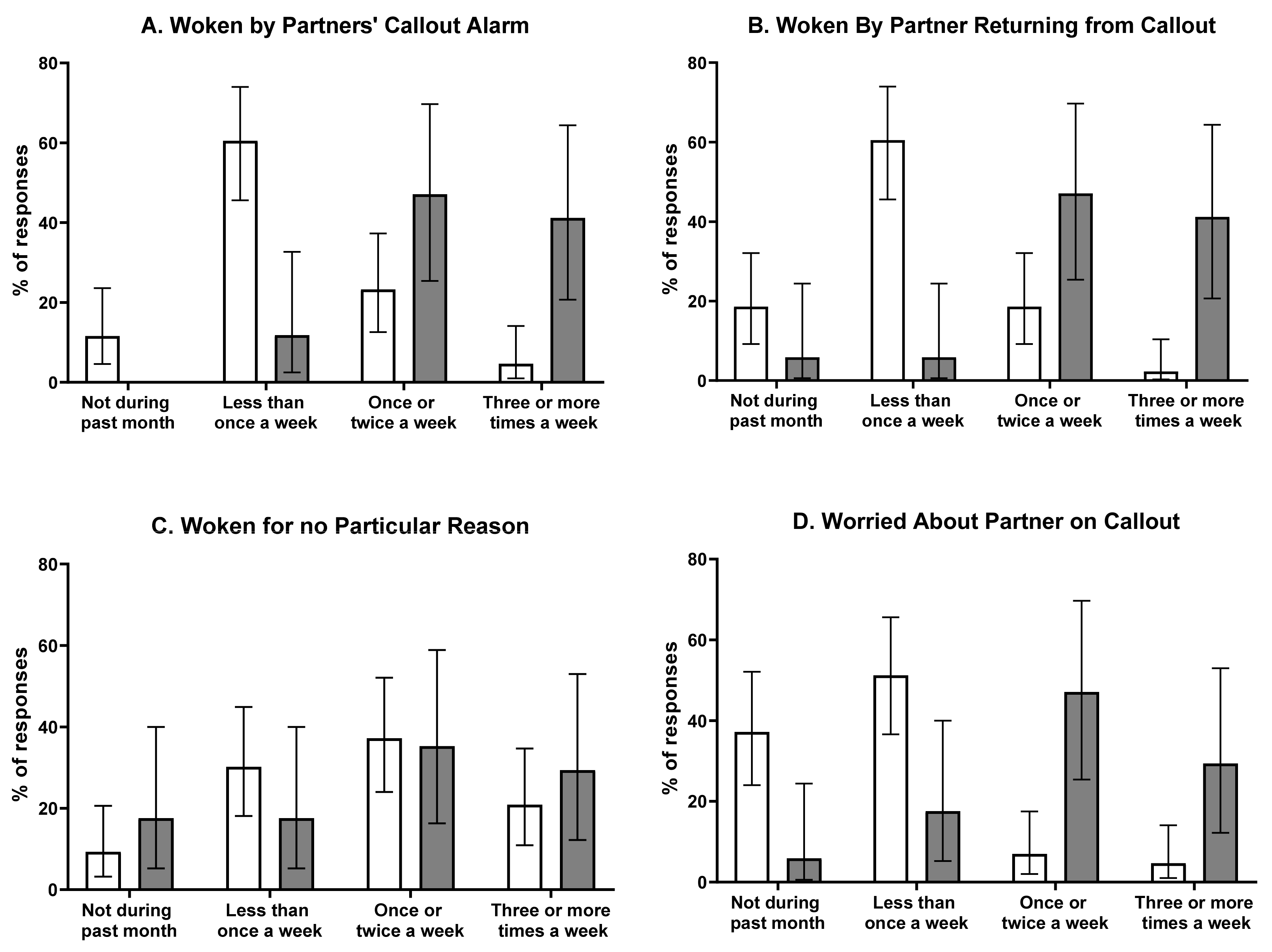
 = participants whose partners received ≤ 5 calls per month;
= participants whose partners received ≤ 5 calls per month;  = participants whose partners received >5 calls per month. Please note: n = 1 “other” response not shown due to low frequency.
= participants whose partners received ≤ 5 calls per month; = participants whose partners received >5 calls per month. Please note: n = 1 “other” response not shown due to low frequency.
= participants whose partners received >5 calls per month. Please note: n = 1 “other” response not shown due to low frequency.
= participants whose partners received ≤ 5 calls per month; = participants whose partners received >5 calls per month. Please note: n = 1 “other” response not shown due to low frequency.

{kind=link}
| Total | ||
|---|---|---|
| Participant Characteristic | n | % |
| n | 60 | 100 |
| Sex | ||
| Female | 56 | 93.3 |
| Male | 4 | 6.7 |
| How old are you? Age group (y) | ||
| 18–24 years | 5 | 8.3 |
| 25–34 years | 17 | 28.4 |
| 35–44 years | 20 | 33.3 |
| 45–54 years | 13 | 21.7 |
| >55 years | 5 | 8.3 |
| How long (in years) have you and your partner been a couple, while your partner has been on-call as a firefighter? | ||
| 0–5 years | 29 | 48.3 |
| 6–10 years | 12 | 20.0 |
| 11–15 years | 7 | 11.7 |
| 16–20 years | 6 | 10.0 |
| Over 20 years | 6 | 10.0 |
| Approximately how many overnight firefighter calls did your partner receive over the past month? | ||
| 0–5 | 43 | 71.7 |
| 6–10 | 13 | 21.7 |
| 11–15 | 2 | 3.3 |
| 16–20 | 2 | 3.3 |
| The following represent different degrees of happiness in your relationship. The middle point, “happy”, represents the degree of happiness of most relationships. Please select the degree of happiness, all things considered, in your relationship. | ||
| Extremely/Fairly/A Little Unhappy | 5 | 8.3 |
| Happy/Very/Extremely Happy or Perfect | 55 | 91.7 |
| With regard to your partner’s auxiliary firefighter role, how do you feel about their participation? | ||
| I would like/very much like my partner to give up role | 5 | 8.3 |
| Neutral | 10 | 16.7 |
| I would like/very much like my partner to continue role | 45 | 75.0 |
| Total | ||
|---|---|---|
| Question | n | % |
| Do you have any of the following diagnosed sleep-related disorders or conditions that impact your sleep? (select all that apply) | ||
| No, I do not currently have a diagnosed sleep disorder or condition impacting sleep | 41 | 68.3 |
| Snoring | 7 | 11.7 |
| Insomnia | 5 | 8.3 |
| Restless Legs | 4 | 6.7 |
| Sleep Apnoea | 0 | 0.0 |
| Depression | 5 | 8.3 |
| Anxiety | 5 | 8.3 |
| PTSD | 0 | 0.0 |
| Other | 4 | 6.7 |
| In general, how would you rate your sleep on a night when your partner is not called? | ||
| Very Poor/Rather Poor | 3 | 5.0 |
| Neither Poor Nor Good | 9 | 15.0 |
| Very Good/Rather Good | 48 | 80.0 |
| In general, how would you rate your sleep on a night when your partner is called? | ||
| Very Poor/Rather Poor | 37 | 61.7 |
| Neither Poor Nor Good | 7 | 11.7 |
| Very Good/Rather Good | 16 | 26.6 |
| In general, when I am woken by my partner’s call I can easily go back to sleep. | ||
| Strongly Disagree/Disagree | 38 | 63.3 |
| Neither Agree nor Disagree | 9 | 15.0 |
| Strongly Agree/Agree | 13 | 21.7 |
| In general, when my partner returns from a call, I can easily go back to sleep if I have the opportunity to do so. | ||
| Strongly Disagree/Disagree | 14 | 23.3 |
| Neither Agree nor Disagree | 14 | 23.3 |
| Strongly Agree/Agree | 32 | 53.4 |
| During the past month, with regard to sleeping arrangements with your partner, did you usually? | ||
| Sleep with partner in same bed | 54 | 90.0 |
| Sleep in another room | 6 | 10.0 |
| During the past month, what time have you usually gone to bed on a weekday? | ||
| 08:00 pm–08:59 pm | 8 | 13.4 |
| 09:00 pm–09:59 pm | 26 | 43.3 |
| 10:00 pm–10:59 pm | 21 | 35.0 |
| 11:00 pm–11:59 pm | 4 | 6.6 |
| 12:00 am–12:59 am | 1 | 1.7 |
| During the past month, what time have you usually gone to bed on the weekend? | ||
| 07:00 pm–07:59 pm | 1 | 1.7 |
| 08:00 pm–08:59 pm | 2 | 3.3 |
| 09:00 pm–09:59 pm | 15 | 25.0 |
| 10:00 pm–10:59 pm | 31 | 51.7 |
| 11:00 pm–11:59 pm | 8 | 13.3 |
| 12:00 am–12:59 am | 2 | 3.3 |
| 01:00 am–01:59 am | 1 | 1.7 |
| During the past month, how long (in minutes) has it usually taken you to fall asleep when you go to bed? | ||
| 1–15 min | 24 | 40.0 |
| 16–30 min | 23 | 38.3 |
| 31–45 min | 10 | 16.7 |
| >45 min | 3 | 5.0 |
| During the past month, what time have you usually gotten up in the morning on a weekday? | ||
| 04:00 am–04:59 am | 2 | 3.3 |
| 05:00 am–05:59 am | 17 | 28.4 |
| 06:00 am–06:59 am | 26 | 43.3 |
| 07:00 am–07:59 am | 13 | 21.7 |
| 08:00 am–08:59 am | 2 | 3.3 |
| During the past month, what time have you usually gotten up in the morning on the weekend? | ||
| 05:00 am–05:59 am | 1 | 1.7 |
| 06:00 am–06:59 am | 17 | 28.3 |
| 07:00 am–07:59 am | 20 | 33.3 |
| 08:00 am–08:59 am | 12 | 20.0 |
| 09:00 am–09:59 am | 7 | 11.7 |
| 10:00 am–10:59 am | 2 | 3.3 |
| 11:00 am–11:59 am | 1 | 1.7 |
| During the past month, how many hours of actual sleep did you get at night, on average? | ||
| 5–5.5 h | 7 | 11.7 |
| 6–6.5 h | 7 | 11.7 |
| 7–7.5 h | 26 | 43.3 |
| 8–8.5 h | 16 | 26.7 |
| 9–9.5 h | 4 | 6.6 |
| During the past month, how would you rate your sleep quality overall? | ||
| Very bad | 1 | 1.7 |
| Fairly bad | 15 | 25.0 |
| Fairly good | 38 | 63.3 |
| Very good | 6 | 10.0 |
| During the past month, how often have you taken medicine (prescribed or “over the counter”) to help you sleep? | ||
| Not during the past month | 50 | 83.4 |
| Less than once a week | 2 | 3.3 |
| Once or twice a week | 2 | 3.3 |
| Three or more times a week | 6 | 10.0 |
| During the past month, how often have you had trouble staying awake while driving, eating meals, or engaging in social activity? | ||
| Not during the past month | 48 | 80.0 |
| Less than once a week | 9 | 15.0 |
| Once or twice a week | 3 | 5.0 |
| Three or more times a week | 0 | 0.0 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vincent, G.E.; Karan, S.; Paterson, J.; Reynolds, A.C.; Dominiak, M.; Ferguson, S.A. Impacts of Australian Firefighters’ On-Call Work Arrangements on the Sleep of Partners. Clocks & Sleep 2020, 2, 39-51. https://doi.org/10.3390/clockssleep2010005
Vincent GE, Karan S, Paterson J, Reynolds AC, Dominiak M, Ferguson SA. Impacts of Australian Firefighters’ On-Call Work Arrangements on the Sleep of Partners. Clocks & Sleep. 2020; 2(1):39-51. https://doi.org/10.3390/clockssleep2010005
Chicago/Turabian StyleVincent, Grace E., Simone Karan, Jessica Paterson, Amy C. Reynolds, Michelle Dominiak, and Sally A. Ferguson. 2020. "Impacts of Australian Firefighters’ On-Call Work Arrangements on the Sleep of Partners" Clocks & Sleep 2, no. 1: 39-51. https://doi.org/10.3390/clockssleep2010005