
Digital Workflow in Full Mouth Rehabilitation with Immediate Loading, Intraoral Welding and 3D-Printed Reconstructions in a Periodontal Patient: A Case Report


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Case Report Section
2.1. Patient Information and Clinical Findings
- The extraction of remaining teeth and immediately give removable 3D printed dentures inserted on the temporary implants to the patient;
- Implantation after the healing time and the immediate loading of temporaries;
- Final restoration after another six months.
2.2. Therapeutic Intervention and Outcomes
2.2.1. Stage I
2.2.2. Stage II
2.2.3. Stage III
- Intraoral scan and CBCT;
- Meshmixer design of removable dentures;
- Three-dimensional manufacturing of removable dentures;
- Extraction of remaining teeth, immediate temporary implant placement, and removable denture delivery.
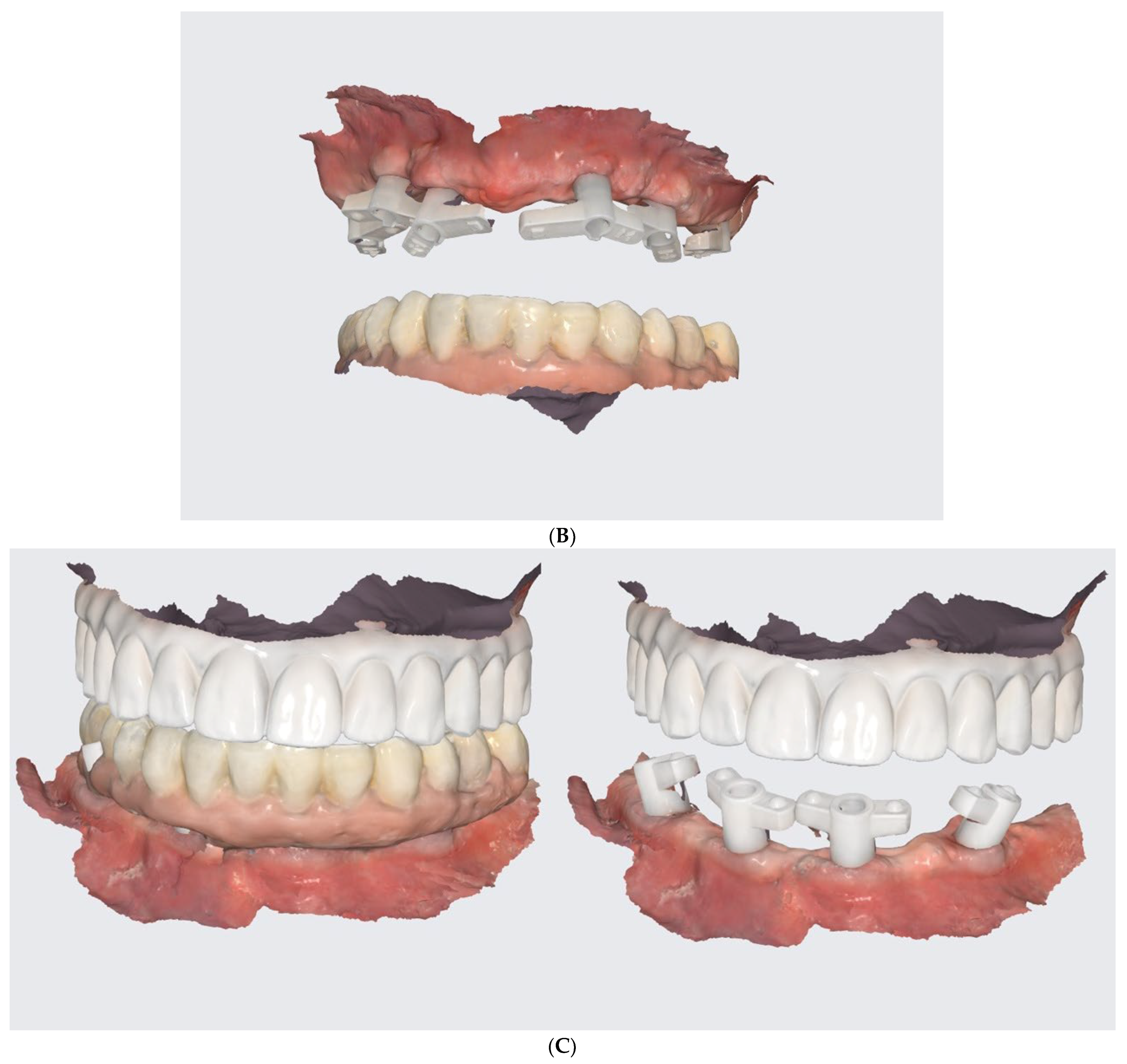
- Conduction of DSD, an I.O. scan, a 360° scan of removals, and CBCT after the healing phrase.
- The merging of the abovementioned examination data and design of the prosthetically driven implant positions.
- The development of the surgical guide and the 3D-printing of the teeth shells.
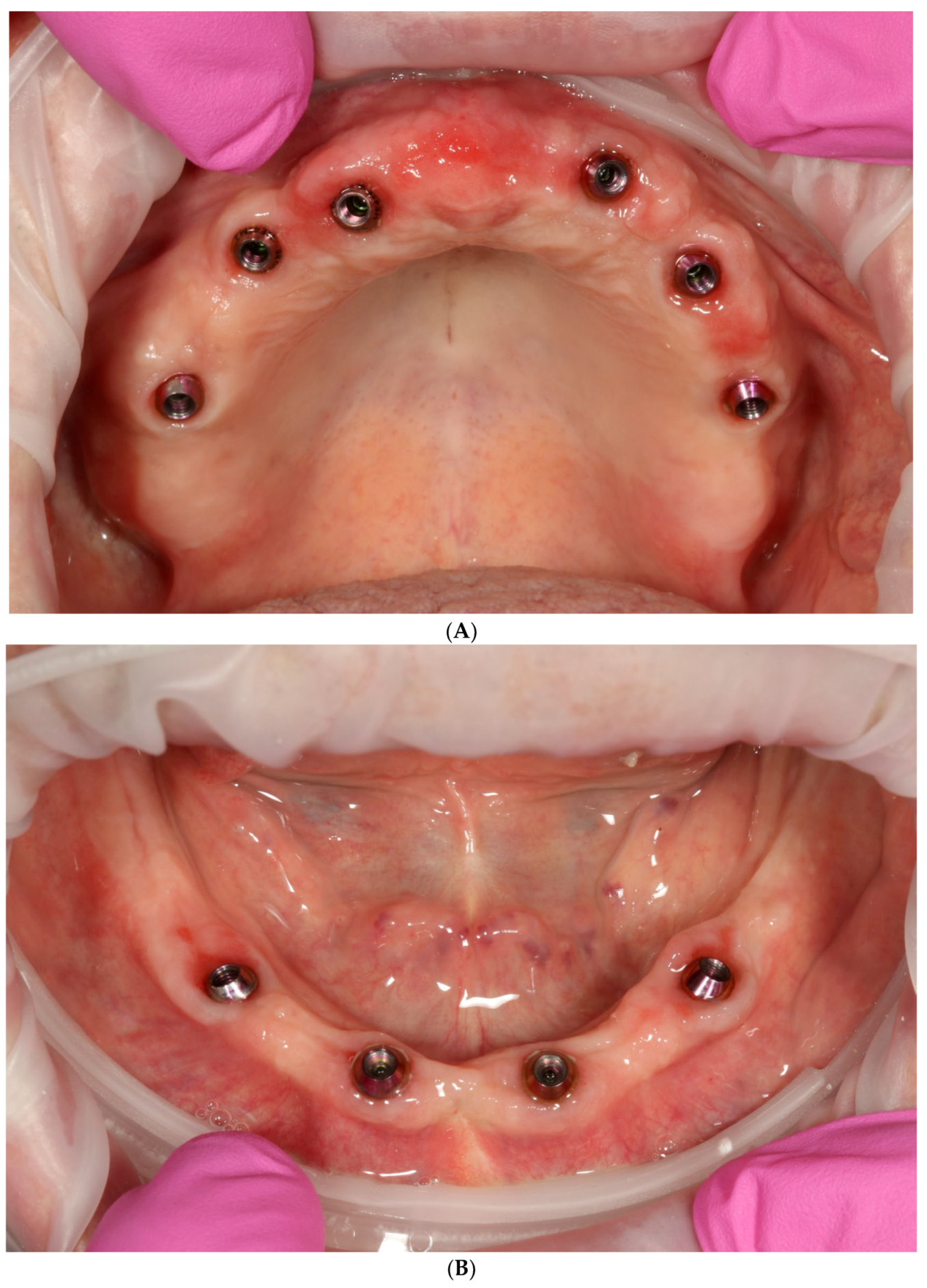
- One-day surgery with implant placement, MUA, and intraoral welding to obtain immediately loaded long-lasting temporaries.
- The conduction of an analogue impression, an I.O. scan, a removable 360° scan, and a scanflag scan.
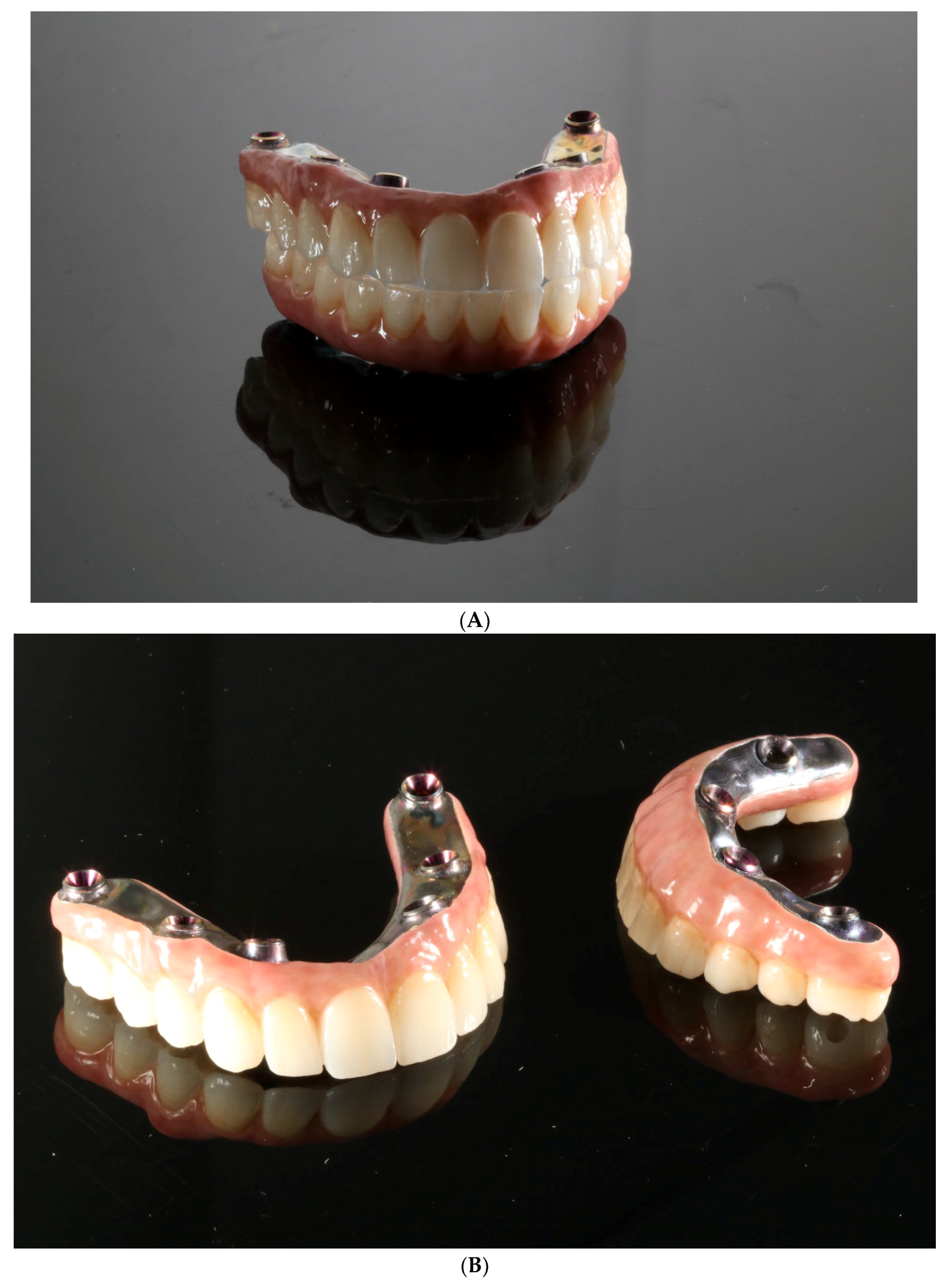
- The conduction of a Sheffield passive fit test of 3D-printed try-ins on a milled titanium bar.
- Final restoration delivery with occlusal equilibration.
3. Discussion
- Those printed on a desktop 3D printer (Phrozen mini 4k, Phrozen Tech. Co., Ltd., Hsinchu City, Taiwan) [6];
- Those printed and fixed with a rigid welded bar, as a reinforced overdenture shows a lower risk of fracture, when compared to that associated with nonreinforced dentures [25];
- Those created with a full-porcelain and milled titanium bar (also reinforced).
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Yussif, N.; Rahman, A.R.A. Is immediate implant placement advantageous for the management of aggressive periodontitis patients in maxillary esthetic zone? An update of systematic reviews. J. Osseointegr. 2020, 12. [Google Scholar] [CrossRef]
- Tonetti, M.S.; Greenwell, H.; Kornman, K.S. Staging and grading of periodontitis: Framework and proposal of a new classification and case definition. J. Periodontol. 2018, 89 (Suppl. 1), S159–S172. [Google Scholar] [CrossRef] [PubMed]
- Del Fabbro, M.; Testori, T.; Kekovic, V.; Goker, F.; Tumedei, M.; Wang, H.-L. A systematic review of survival rates of osseointegrated implants in fully and partially edentulous patients following immediate loading. J. Clin. Med. 2019, 8, 2142. [Google Scholar] [CrossRef]
- Venezia, P.; Torsello, F.; Santomauro, V.; Dibello, V.; Cavalcanti, R. Full Digital Workflow for the Treatment of an Edentulous Patient with Guided Surgery, Immediate Loading and 3D-Printed Hybrid Prosthesis: The BARI Technique 2.0. A Case Report. Int. J. Environ. Res. Public Health 2019, 16, 5160. [Google Scholar] [CrossRef] [PubMed]
- Cortellini, P.; Stalpers, G.; Mollo, A.; Tonetti, M.S. Periodontal regeneration versus extraction and dental implant or prosthetic replacement of teeth severely compromised by attachment loss to the apex: A randomized controlled clinical trial reporting 10-year outcomes, survival analysis and mean cumulative cost of recurrence. J. Clin. Periodontol. 2020, 47, 768–776. [Google Scholar] [CrossRef]
- D’haese, R.; Vrombaut, T.; Hommez, G.; De Bruyn, H.; Vandeweghe, S. Accuracy of Guided Implant Surgery Using an Intraoral Scanner and Desktop 3D-Printed Tooth-Supported Guides. Int. J. Oral Maxillofac. Implant. 2022, 37, 479–484. [Google Scholar] [CrossRef]
- Slutzkey, G.S.; Cohen, O.; Chaushu, L.; Rahmanov, A.; Mijiritsky, E.; Beitlitum, I.; Kolerman, R. Immediate Maxillary Full-Arch Rehabilitation of Periodontal Patients with Terminal Dentition Using Tilted Implants and Bone Augmentation: A 5-Year Retrospective Cohort Study. J. Clin. Med. 2022, 11, 2902. [Google Scholar] [CrossRef] [PubMed]
- Marconcini, S.; Giammarinaro, E.; Covani, U.; Mascolo, A.; Caso, G.; Del Corso, M. Immediate restoration of fixed full-arch prostheses placed on implants in both fresh and healed sockets using the flat one-bridge technique: A 7-year retrospective study. BMC Oral Health 2021, 21, 617. [Google Scholar] [CrossRef]
- Degidi, M.M.; Nardi, D.D.; Piattelli, A.M. A six-year follow-up of full-arch immediate restorations fabricated with an intraoral welding technique. Implant. Dent. 2013, 22, 224–231. [Google Scholar] [CrossRef]
- Albiero, A.; Benato, R.; Benato, A.; Degidi, M. Use of Intraoral Welding to Increase the Predictability of Immediately Loaded Computer-Guided Implants. Int. J. Periodontics Restor. Dent. 2017, 37, 591–598. [Google Scholar] [CrossRef] [PubMed]
- Mazurek-Popczyk, J.; Nowicki, A.; Arkusz, K.; Pałka, Ł.; Zimoch-Korzycka, A.; Baldy-Chudzik, K. Evaluation of biofilm formation on acrylic resins used to fabricate dental temporary restorations with the use of 3D printing technology. BMC Oral Health 2022, 22, 442. [Google Scholar] [CrossRef] [PubMed]
- Buzayan, M.M.; Yunus, N.B. Passive Fit in Screw Retained Multi-unit Implant Prosthesis Understanding and Achieving: A Review of the Literature. J. Indian Prosthodont. Soc. 2014, 14, 16–23. [Google Scholar] [CrossRef] [PubMed]
- Scarano, A.; Stoppaccioli, M.; Casolino, T. Zirconia crowns cemented on titanium bars using CAD/CAM: A five-year follow-up prospective clinical study of 9 patients. BMC Oral Health 2019, 19, 286. [Google Scholar] [CrossRef] [PubMed]
- Hobo, S.; Ichida, E.; García, L.T. Osseointegration and Occlusal Rehabilitation, 1st ed.; Quintessence Publishing Company: New York, NY, USA, 1989; pp. 315–328. [Google Scholar]
- Wismeijer, D.; van Waas, M.A.; Kalk, W. Factors to consider in selecting an occlusal concept for patients with implants in the edentulous mandible. J. Prosthet. Dent. 1995, 74, 380–384. [Google Scholar] [CrossRef] [PubMed]
- Darby, I. Risk factors for periodontitis & peri-implantitis. Periodontology 2022, 90, 9–12. [Google Scholar] [CrossRef]
- Pimkhaokham, A.; Jiaranuchart, S.; Kaboosaya, B.; Arunjaroensuk, S.; Subbalekha, K.; Mattheos, N. Can computer-assisted implant surgery improve clinical outcomes and reduce the frequency and intensity of complications in implant dentistry? A critical review. Periodontology 2022, 90, 197–223. [Google Scholar] [CrossRef]
- Massuda, C.K.M.; de Carvalho, M.R.; de Moraes, J.B.; Pallos, D.; Kim, Y.J. Accuracy of guided dental implant surgery using a fully digital workflow: A case series. J. Prosthet. Dent. 2022, 128. [Google Scholar] [CrossRef]
- Tatakis, D.N.; Chien, H.-H.; Parashis, A.O. Guided implant surgery risks and their prevention. Periodontology 2019, 81, 194–208. [Google Scholar] [CrossRef]
- Chackartchi, T.; Romanos, G.E.; Parkanyi, L.; Schwarz, F.; Sculean, A. Reducing errors in guided implant surgery to optimize treatment outcomes. Periodontology 2022, 88, 64–72. [Google Scholar] [CrossRef]
- Cattoni, F.; Chirico, L.; Merlone, A.; Manacorda, M.; Vinci, R.; Gherlone, E.F. Digital Smile Designed Computer-Aided Surgery versus Traditional Workflow in “All on Four” Rehabilitations: A Randomized Clinical Trial with 4-Years Follow-Up. Int. J. Environ. Res. Public Health 2021, 18, 3449. [Google Scholar] [CrossRef]
- Degidi, M.; Nardi, D.; Piattelli, A. Immediate loading of the edentulous maxilla with a final restoration supported by an intraoral welded titanium bar: A case series of 20 consecutive cases. J. Periodontol. 2008, 79, 2207–2213. [Google Scholar] [CrossRef]
- Albiero, A.M.; Benato, R. Computer-assisted surgery and intraoral welding technique for immediate implant-supported rehabilitation of the edentulous maxilla: Case report and technical description. Int. J. Med. Robot. 2015, 12, 453–460. [Google Scholar] [CrossRef]
- Avvanzo, P.; Fabrocini, L.A.; Ciavarella, D.; Avvanzo, A.; Muzio, L.L.; De Maio, R.A. Use of intraoral welding to stabilize dental implants in augmented sites for immediate provisionalization: A case report. J. Oral Implant. 2012, 38, 33–41. [Google Scholar] [CrossRef] [PubMed]
- Sailer, I.; Karasan, D.; Todorovic, A.; Ligoutsikou, M.; Pjetursson, B.E. Prosthetic failures in dental implant therapy. Periodontology 2022, 88, 130–144. [Google Scholar] [CrossRef]
- Anadioti, E.; Musharbash, L.; Blatz, M.B.; Papavasiliou, G.; Kamposiora, P. 3D printed complete removable dental prostheses: A narrative review. BMC Oral Health 2020, 20, 343. [Google Scholar] [CrossRef] [PubMed]
- Ferguson, R. Simplifying Full-Arch Treatment with In-House 3D-Printed Surgical Guides and Immediate Fixed Provisional Prostheses Using Only CBCT Data. Compend. Contin. Educ. Dent. 2020, 41, 521–526. [Google Scholar] [PubMed]



















Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nowicki, A.; Osypko, K. Digital Workflow in Full Mouth Rehabilitation with Immediate Loading, Intraoral Welding and 3D-Printed Reconstructions in a Periodontal Patient: A Case Report. Reports 2023, 6, 52. https://doi.org/10.3390/reports6040052
Nowicki A, Osypko K. Digital Workflow in Full Mouth Rehabilitation with Immediate Loading, Intraoral Welding and 3D-Printed Reconstructions in a Periodontal Patient: A Case Report. Reports. 2023; 6(4):52. https://doi.org/10.3390/reports6040052
Chicago/Turabian StyleNowicki, Adam, and Karolina Osypko. 2023. "Digital Workflow in Full Mouth Rehabilitation with Immediate Loading, Intraoral Welding and 3D-Printed Reconstructions in a Periodontal Patient: A Case Report" Reports 6, no. 4: 52. https://doi.org/10.3390/reports6040052