
Nurses’ Beliefs and Barriers of Delivering Cardiopulmonary Rehabilitation for Heart Failure Patients in Saudi Arabia: A Cross-Sectional Study
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population and Sampling Strategy
2.2. Statistical Analysis
3. Results
3.1. Opinions on Referring Patients with Heart Failure to Cardiopulmonary Rehabilitation
3.2. Mode of Delivery and Component of Cardiopulmonary Rehabilitation
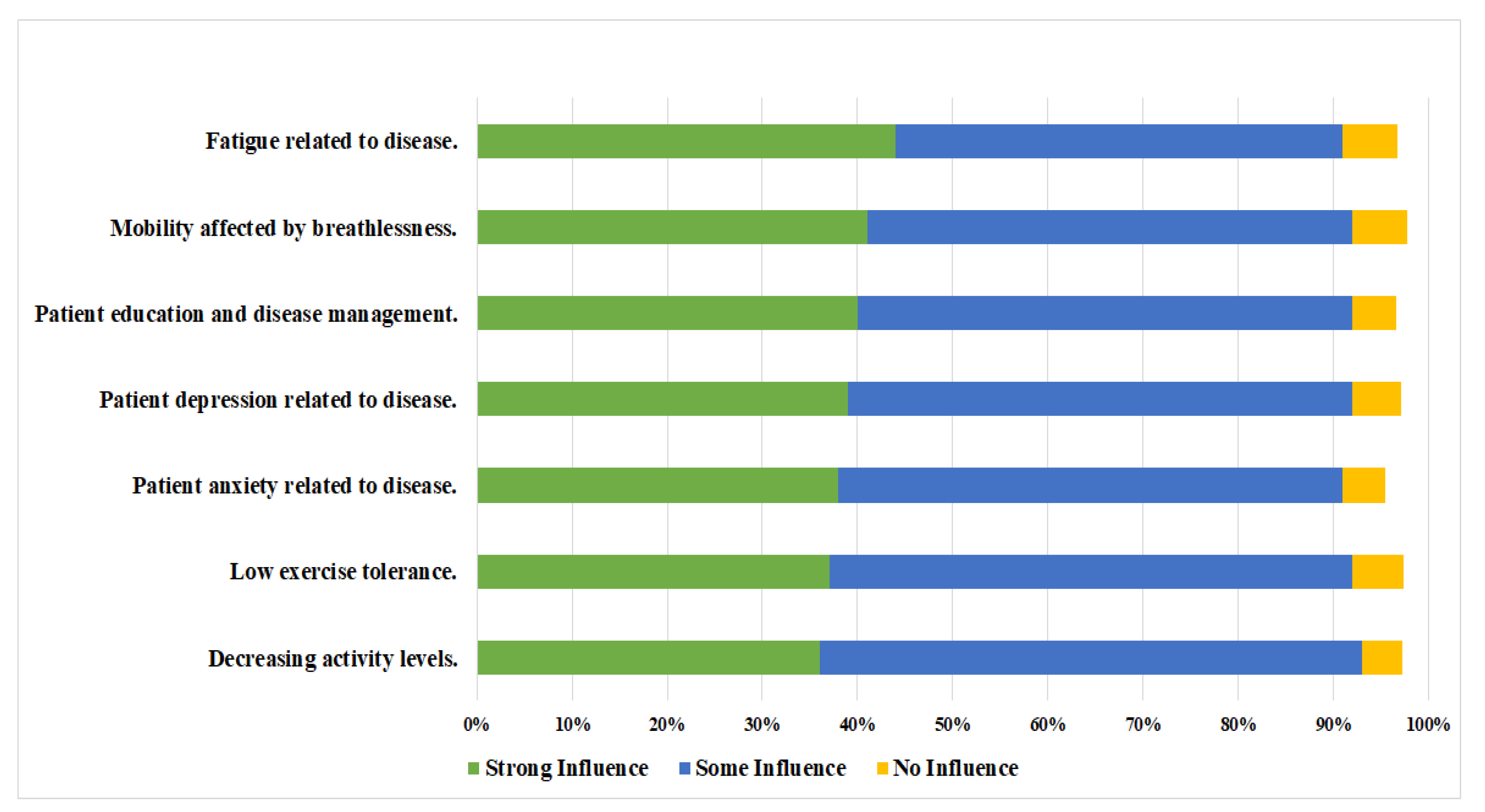
3.3. Patient-Related Factors That Influence Referral Decision to Cardiopulmonary Rehabilitation
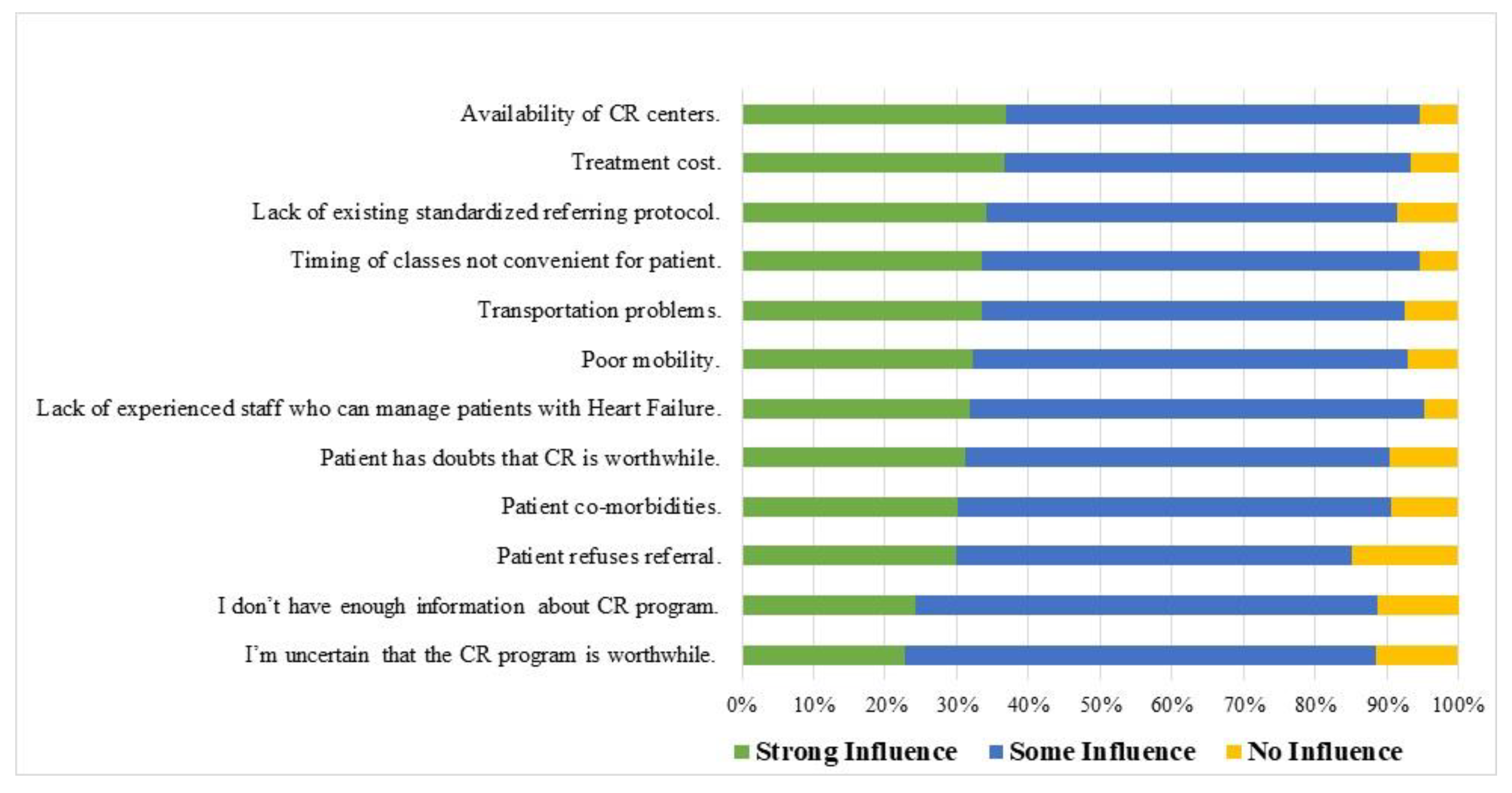
3.4. CR Referral Barriers
4. Discussion
5. Study Limitations
6. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Roth, G.A.; Mensah, G.A.; Johnson, C.O.; Addolorato, G.; Ammirati, E.; Baddour, L.M.; Barengo, N.C.; Beaton, A.Z.; Benjamin, E.J.; Benziger, C.P.; et al. Global Burden of Cardiovascular Diseases and Risk Factors, 1990–2019: Update from the GBD 2019 Study. J. Am. Coll. Cardiol. 2020, 76, 2982–3021. [Google Scholar] [CrossRef] [PubMed]
- Kim, K.H.; Jahan, S.A.; Kabir, E. A review of diseases associated with household air pollution due to the use of biomass fuels. J. Hazard. Mater. 2011, 192, 425–431. [Google Scholar] [CrossRef] [PubMed]
- Khot, U.N.; Khot, M.B.; Bajzer, C.T.; Sapp, S.K.; Ohman, E.M.; Brener, S.J.; Ellis, S.G.; Lincoff, A.M.; Topol, E.J. Prevalence of conventional risk factors in patients with coronary heart disease. JAMA 2003, 290, 898–904. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roger, V.L. Epidemiology of Heart Failure. Circ. Res. 2013, 113, 646–659. [Google Scholar] [CrossRef] [PubMed]
- Bragazzi, N.L.; Zhong, W.; Shu, J.; Abu, M.A.; Lotan, D.; Grupper, A.; Younis, A.; Dai, H. Burden of heart failure and underlying causes in 195 countries and territories from 1990 to 2017. Eur. J. Prev. Cardiol. 2021, 28, 1682–1690. [Google Scholar] [CrossRef]
- Britz, J.A.; Dunn, K.S. Self-care and quality of life among patients with heart failure. J. Am. Acad. Nurse Pract. 2010, 22, 480–487. [Google Scholar] [CrossRef]
- Macchia, A.; Monte, S.; Romero, M.; D’Ettorre, A.; Tognoni, G. The prognostic influence of chronic obstructive pulmonary disease in patients hospitalised for chronic heart failure. Eur. J. Heart Fail. 2007, 9, 942–948. [Google Scholar] [CrossRef] [Green Version]
- AbuRuz, M.E.; Alaloul, F.; Saifan, A.; Masa’deh, R.; Abusalem, S. Quality of Life for Saudi Patients With Heart Failure: A Cross-Sectional Correlational Study. Glob. J. Health Sci. 2016, 8, 49. [Google Scholar] [CrossRef] [Green Version]
- Alqahtani, J.S. Prevalence, incidence, morbidity and mortality rates of COPD in Saudi Arabia: Trends in burden of COPD from 1990 to 2019. PLoS ONE 2022, 17, e0268772. [Google Scholar] [CrossRef]
- Heo, S.; Lennie, T.A.; Okoli, C.; Moser, D.K. Quality of life in patients with heart failure: Ask the patients. Heart Lung 2009, 38, 100–108. [Google Scholar] [CrossRef]
- Redeker, N.S.; Conley, S.; Anderson, G.; Cline, J.; Andrews, L.; Mohsenin, V.; Jacoby, D.; Jeon, S. Effects of Cognitive Behavioral Therapy for Insomnia on Sleep, Symptoms, Stress, and Autonomic Function Among Patients With Heart Failure. Behav. Sleep Med. 2018, 18, 190–202. [Google Scholar] [CrossRef]
- Rice, H.; Say, R.; Betihavas, V. The effect of nurse-led education on hospitalisation, readmission, quality of life and cost in adults with heart failure. A systematic review. Patient Educ. Couns. 2018, 101, 363–374. [Google Scholar] [CrossRef]
- Bozkurt, B.; Fonarow, G.C.; Goldberg, L.R.; Guglin, M.; Josephson, R.A.; Forman, D.E.; Lin, G.; Lindenfeld, J.; O’Connor, C.; Panjrath, G.; et al. Cardiac Rehabilitation for Patients with Heart Failure. J. Am. Coll. Cardiol. 2021, 77, 1454–1469. [Google Scholar] [CrossRef]
- Heran, B.S.; Chen, J.M.; Ebrahim, S.; Moxham, T.; Oldridge, N.; Rees, K.; Thompson, D.R.; Taylor, R.S. Exercise-based cardiac rehabilitation for coronary heart disease. Cochrane Database Syst. Rev. 2011, Cd001800. [Google Scholar] [CrossRef]
- Piepoli, M.F.; Davos, C.; Francis, D.P.; Coats, A.J. Exercise training meta-analysis of trials in patients with chronic heart failure (ExTraMATCH). BMJ 2004, 328, 189. [Google Scholar] [CrossRef] [Green Version]
- Forman, D.E.; Sanderson, B.K.; Josephson, R.A.; Raikhelkar, J.; Bittner, V. American College of Cardiology’s Prevention of Cardiovascular Disease Section. Heart Failure as a Newly Approved Diagnosis for Cardiac Rehabilitation: Challenges and Opportunities. J. Am. Coll. Cardiol. 2015, 65, 2652–2659. [Google Scholar] [CrossRef] [Green Version]
- Piña, I.L.; Apstein, C.S.; Balady, G.J.; Belardinelli, R.; Chaitman, B.R.; Duscha, B.D.; Fletcher, B.J.; Fleg, J.L.; Myers, J.N.; Sullivan, M.J. American Heart Association Committee on exercise, rehabilitation, and prevention. Exercise and heart failure: A statement from the American Heart Association Committee on exercise, rehabilitation, and prevention. Circulation. Circulation 2003, 107, 1210–1225. [Google Scholar] [CrossRef]
- Shanks, L.C.; Moore, S.M.; Zeller, R.A. Predictors of cardiac rehabilitation initiation. Rehabil. Nurs. 2007, 32, 152–157. [Google Scholar] [CrossRef]
- Arena, R.; Williams, M.; Forman, D.E.; Cahalin, L.P.; Coke, L.; Myers, J.; Hamm, L.; Kris-Etherton, P.; Humphrey, R.; Bittner, V.; et al. Increasing referral and participation rates to outpatient cardiac rehabilitation: The valuable role of healthcare professionals in the inpatient and home health settings: A science advisory from the American Heart Association. Circulation 2012, 125, 1321–1329. [Google Scholar] [CrossRef]
- Rashed, M.; Theruvan, N.; Gad, A.; Shaheen, H. Cardiac Rehabilitation: Future of Heart Health in Saudi Arabia, a Perceptual View. World J. Cardiovasc. Dis. 2020, 10, 666–677. [Google Scholar] [CrossRef]
- Aldhahir, A.M.; Alqahtani, J.S.; Alghamdi, S.M.; Alqarni, A.A.; Khormi, S.K.; Alwafi, H.; Samannodi, M.; Siraj, R.A.; Alhotye, M.; Naser, A.Y.; et al. Physicians’ Attitudes, Beliefs and Barriers to a Pulmonary Rehabilitation for COPD Patients in Saudi Arabia: A Cross-Sectional Study. Healthcare 2022, 10, 904. [Google Scholar] [CrossRef] [PubMed]
- McDonagh, T.A.; Metra, M.; Adamo, M.; Gardner, R.S.; Baumbach, A.; Böhm, M.; Burri, H.; Butler, J.; Čelutkienė, J.; Chioncel, O.; et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: Developed by the Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC) With the special contribution of the Heart Failure Association (HFA) of the ESC. Eur. Heart J. 2021, 42, 3599–3726. [Google Scholar] [PubMed]
- Yancy, C.W.; Jessup, M.; Bozkurt, B.; Butler, J.; Casey, D.E.; Drazner, M.H.; Fonarow, G.C.; Geraci, S.A.; Horwich, T.; Januzzi, J.L.; et al. 2013 ACCF/AHA guideline for the management of heart failure: A report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. J. Am. Coll. Cardiol. 2013, 62, e147–e239. [Google Scholar] [CrossRef] [Green Version]
- Long, L.; Mordi, I.R.; Bridges, C.; Sagar, V.A.; Davies, E.J.; Coats, A.J.; Dalal, H.; Rees, K.; Singh, S.J.; Taylor, R.S. Exercise-based cardiac rehabilitation for adults with heart failure. Cochrane Database Syst. Rev. 2019, 2019, CD003331. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Taylor, R.S.; Long, L.; Mordi, I.R.; Madsen, M.T.; Davies, E.J.; Dalal, H.; Rees, K.; Singh, S.J.; Gluud, C.; Zwisler, A.D. Exercise-based rehabilitation for heart failure: Cochrane systematic review, meta-analysis, and trial sequential analysis. JACC Heart Fail. 2019, 7, 691–705. [Google Scholar] [CrossRef]
- Cao, Y.; Davidson, P.M.; DiGiacomo, M. Cardiovascular disease in China: An urgent need to enhance the nursing role to improve health outcomes. J. Clin. Nurs. 2009, 18, 687–693. [Google Scholar] [CrossRef]
- Fernandez, R.S.; Salamonson, Y.; Griffiths, R.; Juergens, C.; Davidson, P. Sociodemographic predictors and reasons for participation in an outpatient cardiac rehabilitation programme following percutaneous coronary intervention. Int. J. Nurs. Pract. 2008, 14, 237–242. [Google Scholar] [CrossRef]
- Kellar, G.; Hickey, G.W.; Goss, F.; Fertman, C.; Forman, D.E. Cardiac Rehabilitation Knowledge and Attitudes of Cardiology Fellows. J. Cardiopulm. Rehabil. Prev. 2021, 41, 30–34. [Google Scholar] [CrossRef]
- Krantz, M.J.; Havranek, E.P.; Mehler, P.S.; Haynes, D.K.; Long, C.S. Impact of a cardiac risk reduction program in vulnerable patients hospitalized with coronary artery disease. Pharmacother. J. Hum. Pharmacol. Drug Ther. 2004, 24, 768–775. [Google Scholar] [CrossRef]
- Rassin, M. Nurses’ professional and personal values. Nurs. Ethics 2008, 15, 614–630. [Google Scholar] [CrossRef]
- McBride, C.M.; Emmons, K.M.; Lipkus, I.M. Understanding the potential of teachable moments: The case of smoking cessation. Health Educ. Res. 2003, 18, 156–170. [Google Scholar] [CrossRef]
- Gravely-Witte, S.; Leung, Y.W.; Nariani, R.; Tamim, H.; Oh, P.; Chan, V.M.; Grace, S.L. Effects of cardiac rehabilitation referral strategies on referral and enrollment rates. Nat. Rev. Cardiol. 2010, 7, 87–96. [Google Scholar] [CrossRef] [Green Version]
- Buttery, A.K.; Carr-White, G.; Martin, F.C.; Glaser, K.; Lowton, K. Limited availability of cardiac rehabilitation for heart failure patients in the United Kingdom: Findings from a national survey. Eur. J. Prev. Cardiol. 2014, 21, 928–940. [Google Scholar] [CrossRef]
- Taylor, R.S.; Dalal, H.M.; McDonagh, S.T.J. The role of cardiac rehabilitation in improving cardiovascular outcomes. Nat. Rev. Cardiol. 2022, 19, 180–194. [Google Scholar] [CrossRef]
- Strens, D.; Colle, A.; Vrijens, F.; Paulus, D.; Eyssen, M.; Van Brabandt, H.; Van Vlaenderen, I. Multidisciplinary outpatient rehabilitation following cardiac revascularization or valve surgery: Patient-related factors for uptake. Eur. J. Prev. Cardiol. 2013, 20, 422–430. [Google Scholar] [CrossRef]
- Elsakr, C.; Bulger, D.A.; Roman, S.; Kirolos, I.; Khouzam, R.N. Barriers physicians face when referring patients to cardiac rehabilitation: A narrative review. Ann. Transl. Med. 2019, 7, 414. [Google Scholar] [CrossRef]
- Turk-Adawi, K.I.; Terzic, C.; Bjarnason-Wehrens, B.; Grace, S.L. Cardiac rehabilitation in Canada and Arab countries: Comparing availability and program characteristics. BMC Health Serv. Res. 2015, 15, 521. [Google Scholar] [CrossRef] [Green Version]
- Turk-Adawi, K.; Sarrafzadegan, N.; Grace, S.L. Global availability of cardiac rehabilitation. Nat. Rev. Cardiol. 2014, 11, 586–596. [Google Scholar] [CrossRef] [Green Version]
- Zhu, H.; Ye, Z.; Ning, L.; Han, X.; Wu, Y. Knowledge and Attitude of the Medical Staff Concerning Cardiac Rehabilitation in Zhejiang Province, China: A Cross-Sectional Study. Patient Prefer. Adherence 2020, 14, 1771–1777. [Google Scholar] [CrossRef]
- Alsubaiei, M.E.; Cafarella, P.A.; Frith, P.A.; McEvoy, R.D.; Effing, T.W. Barriers for setting up a pulmonary rehabilitation program in the Eastern Province of Saudi Arabia. Ann. Thorac. Med. 2016, 11, 121. [Google Scholar] [CrossRef]
- Aldhahir, A.M.; Alghamdi, S.M.; Alqahtani, J.S.; Alqahtani, K.A.; Al Rajah, A.M.; Alkhathlan, B.S.; Singh, S.J.; Mandal, S.; Hurst, J.R. Pulmonary rehabilitation for COPD: A narrative review and call for further implementation in Saudi Arabia. Ann. Thorac. Med. 2021, 16, 299–305. [Google Scholar] [CrossRef] [PubMed]
- Abu Hasheesh, M.O. Health care professionals’ awareness and knowledge of cardiac rehabilitation programs among cardiovascular disease patients in Al-Madinah, Saudi Arabia. Life Sci. J. 2014, 11, 911–917. [Google Scholar]
- Chindhy, S.; Taub, P.R.; Lavie, C.J.; Shen, J. Current challenges in cardiac rehabilitation: Strategies to overcome social factors and attendance barriers. Expert Rev. Cardiovasc. Ther. 2020, 18, 777–789. [Google Scholar] [CrossRef] [PubMed]
- Fini, A.; da Cruz, D.d.L.M. Characteristics of fatigue in heart failure patients: A literature review. Rev. Lat. Am. Enferm. 2009, 17, 557–565. [Google Scholar] [CrossRef] [Green Version]
- Franzen, K.; Blomqvist, K.; Saveman, B.I. Impact of chronic heart failure on elderly persons’ daily life: A validation study. Eur. J. Cardiovasc. Nurs. 2006, 5, 137–145. [Google Scholar] [CrossRef]
- Marchionni, N.; Fattirolli, F.; Fumagalli, S.; Oldridge, N.; Del Lungo, F.; Morosi, L.; Burgisser, C.; Masotti, G. Improved exercise tolerance and quality of life with cardiac rehabilitation of older patients after myocardial infarction: Results of a randomized, controlled trial. Circulation 2003, 107, 2201–2206. [Google Scholar] [CrossRef] [Green Version]
- Klompstra, L.; Jaarsma, T.; Stromberg, A. Physical activity in patients with heart failure: Barriers and motivations with special focus on sex differences. Patient Prefer. Adherence 2015, 9, 1603–1610. [Google Scholar] [CrossRef] [Green Version]
- Lindwall, M.; Rennemark, M.; Halling, A.; Berglund, J.; Hassmén, P. Depression and exercise in elderly men and women: Findings from the Swedish national study on aging and care. J. Aging Phys. Act. 2007, 15, 41–55. [Google Scholar] [CrossRef]
- Tian, Y.; Deng, P.; Li, B.; Wang, J.; Li, J.; Huang, Y.; Zheng, Y. Treatment models of cardiac rehabilitation in patients with coronary heart disease and related factors affecting patient compliance. Rev. Cardiovasc. Med. 2019, 20, 27–33. [Google Scholar]



{kind=link}
{kind=link}
| Demographic Variables | Number (%) |
|---|---|
| Gender | |
| Male | 194 (44%) |
| Female | 245 (56%) |
| Year of experience with heart failure patients (M ± SD) | 6 ± 5 |
| Responsibilities for care with heart failure patients | |
| Primary care | 330 (75.17%) |
| Oxygen therapy | 315 (72%) |
| Urgent assessments | 226 (51%) |
| Medication checks | 179 (41%) |
| Inpatient treatment | 161 (37%) |
| Non-urgent care | 121 (27.5%) |
| Diagnosis | 80 (18%) |
| Ongoing management | 67 (15%) |
| Admission prevention | 43 10%) |
| Prescribing | 33 (7.5%) |
| Outpatient clinics | 31 (7%) |
| Item | Number (%) |
|---|---|
| I believe CR will improve patients’ physical fitness | |
| Strongly agree | 107 (24%) |
| Agree | 255 (58%) |
| Neutral | 50 (11.38%) |
| Disagree | 14 (3.18%) |
| Strongly disagree | 13 (3%) |
| I believe CR will reduce patients’ breathlessness | |
| Strongly agree | 94 (21.1%) |
| Agree | 248 (56.4%) |
| Neutral | 70 (16%) |
| Disagree | 18 (4%) |
| Strongly disagree | 9 (2%) |
| I believe CR will improve patients’ palpitation & fatigue | |
| Strongly agree | 90 (20.5%) |
| Agree | 240 (55%) |
| Neutral | 81 (18.45%) |
| Disagree | 18 (4.1%) |
| Strongly disagree | 10 (2.27%) |
| I believe CR will improve patients’ ability to perform daily actives | |
| Strongly agree | 87 (19.81%) |
| Agree | 262 (59.68%) |
| Neutral | 73 (16.62%) |
| Disagree | 10 (2.27%) |
| Strongly disagree | 7 (2%) |
| I believe CR will reduce hospital readmission | |
| Strongly agree | 51 (11.6%) |
| Agree | 223 (51%) |
| Neutral | 87 (19.81%) |
| Disagree | 40 (9.11%) |
| Strongly disagree | 38 (8.65%) |
| Item | Number (%) |
|---|---|
| The best way to deliver CR program for HF patients | |
| In hospital supervised program. | 360 (82%) |
| Online program with HCP support. | 121 (27.56%) |
| At home. | 110 (25%) |
| Tailored program with HCP support through phone. | 81 (18.45%) |
| Component of CR program aside from exercise component | |
| Information about heart failure disease. | 368 (83.8%) |
| Information about medications. | 305 (69.4%) |
| Symptoms management. | 303 (69%) |
| Smoking cessation. | 292 (66.5%) |
| Weight management. | 287 (65.37%) |
| Stress management. | 268 (61%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alzahrani, E.M. Nurses’ Beliefs and Barriers of Delivering Cardiopulmonary Rehabilitation for Heart Failure Patients in Saudi Arabia: A Cross-Sectional Study. Reports 2022, 5, 44. https://doi.org/10.3390/reports5040044
Alzahrani EM. Nurses’ Beliefs and Barriers of Delivering Cardiopulmonary Rehabilitation for Heart Failure Patients in Saudi Arabia: A Cross-Sectional Study. Reports. 2022; 5(4):44. https://doi.org/10.3390/reports5040044
Chicago/Turabian StyleAlzahrani, Eidan M. 2022. "Nurses’ Beliefs and Barriers of Delivering Cardiopulmonary Rehabilitation for Heart Failure Patients in Saudi Arabia: A Cross-Sectional Study" Reports 5, no. 4: 44. https://doi.org/10.3390/reports5040044