
Ketogenic Diet in the Management of Glioblastomas: A Bibliometric Analysis
 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Literature Search
2.3. Bibliometric Analysis
3. Results
3.1. Literature Search
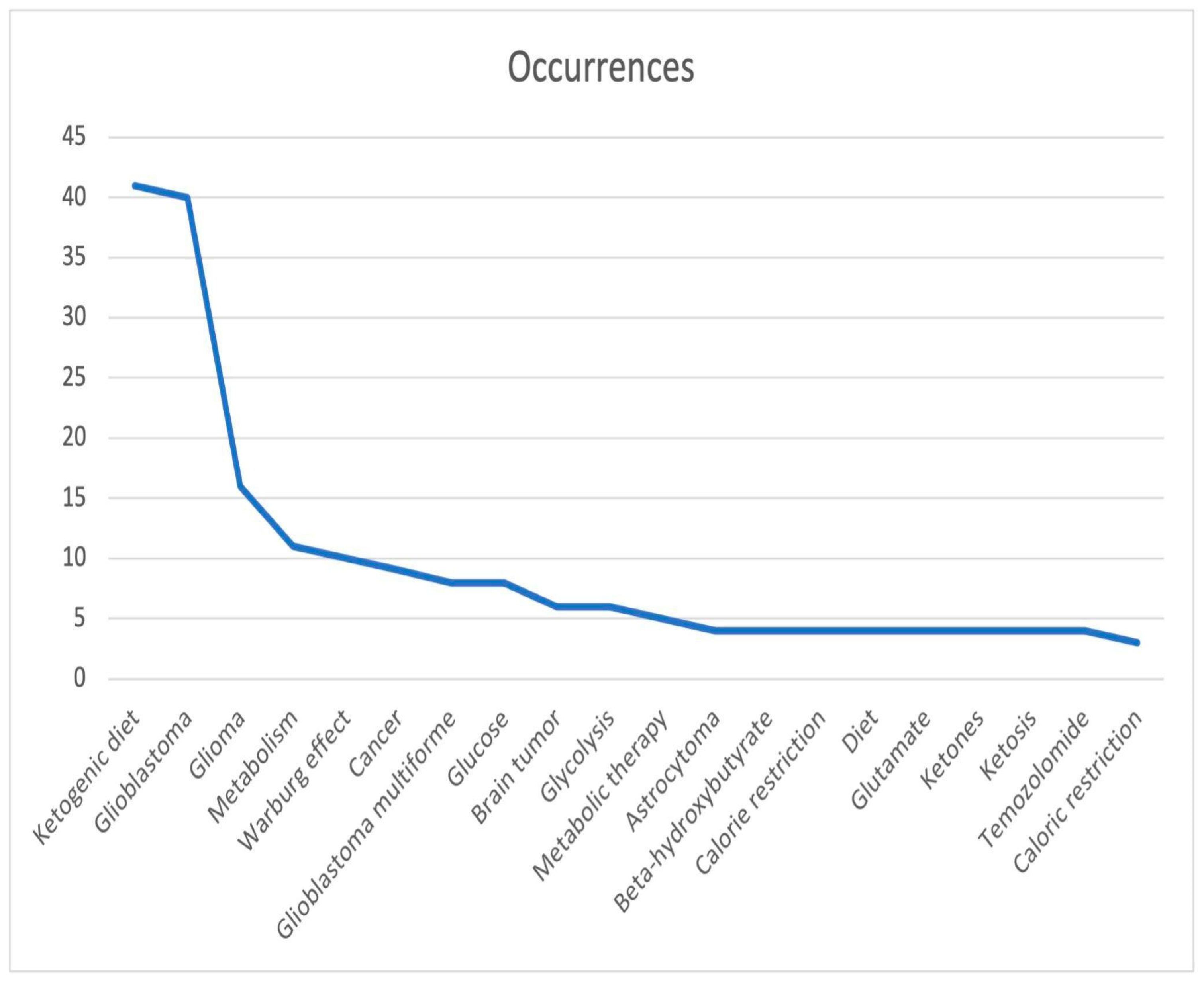
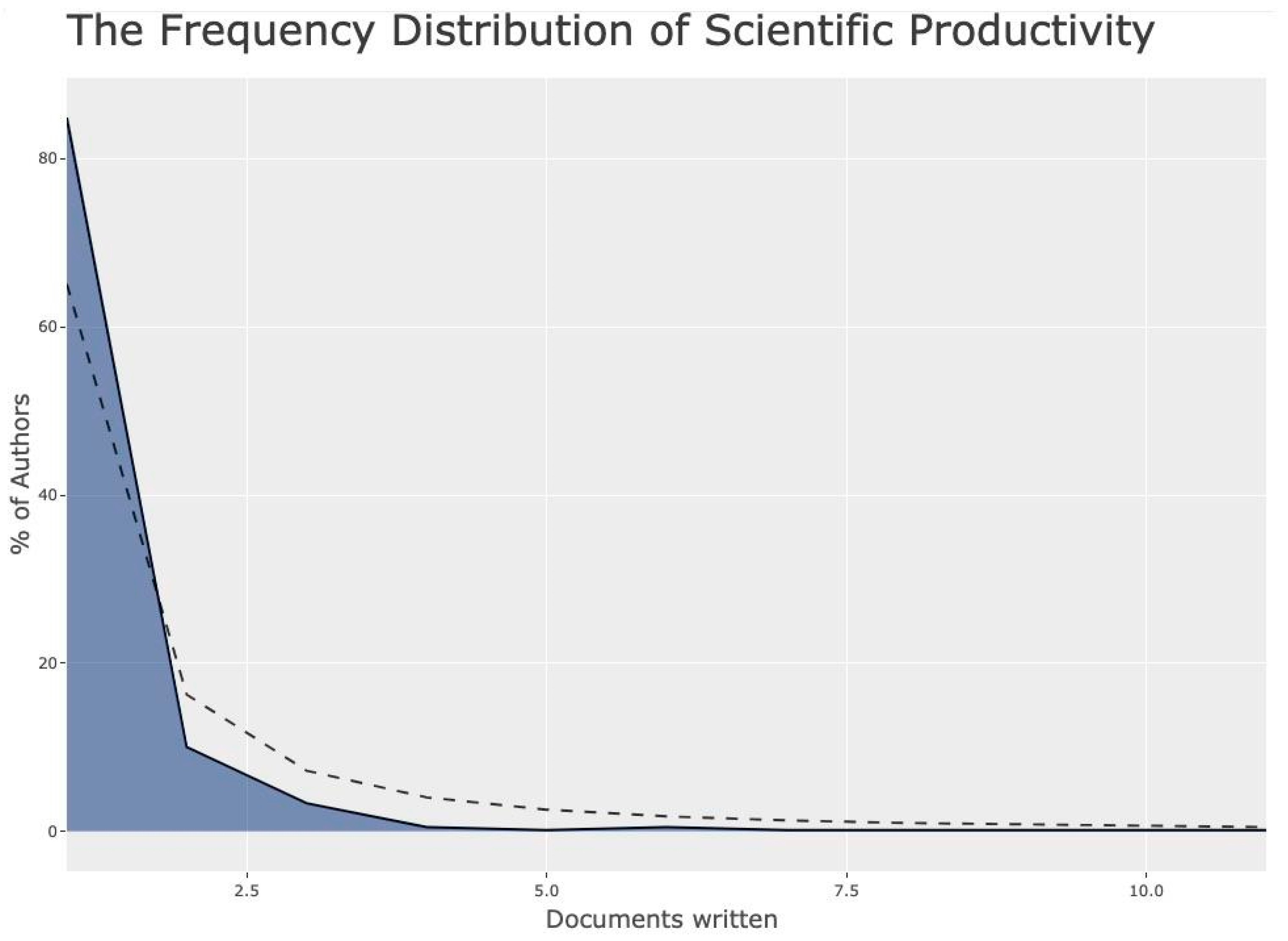
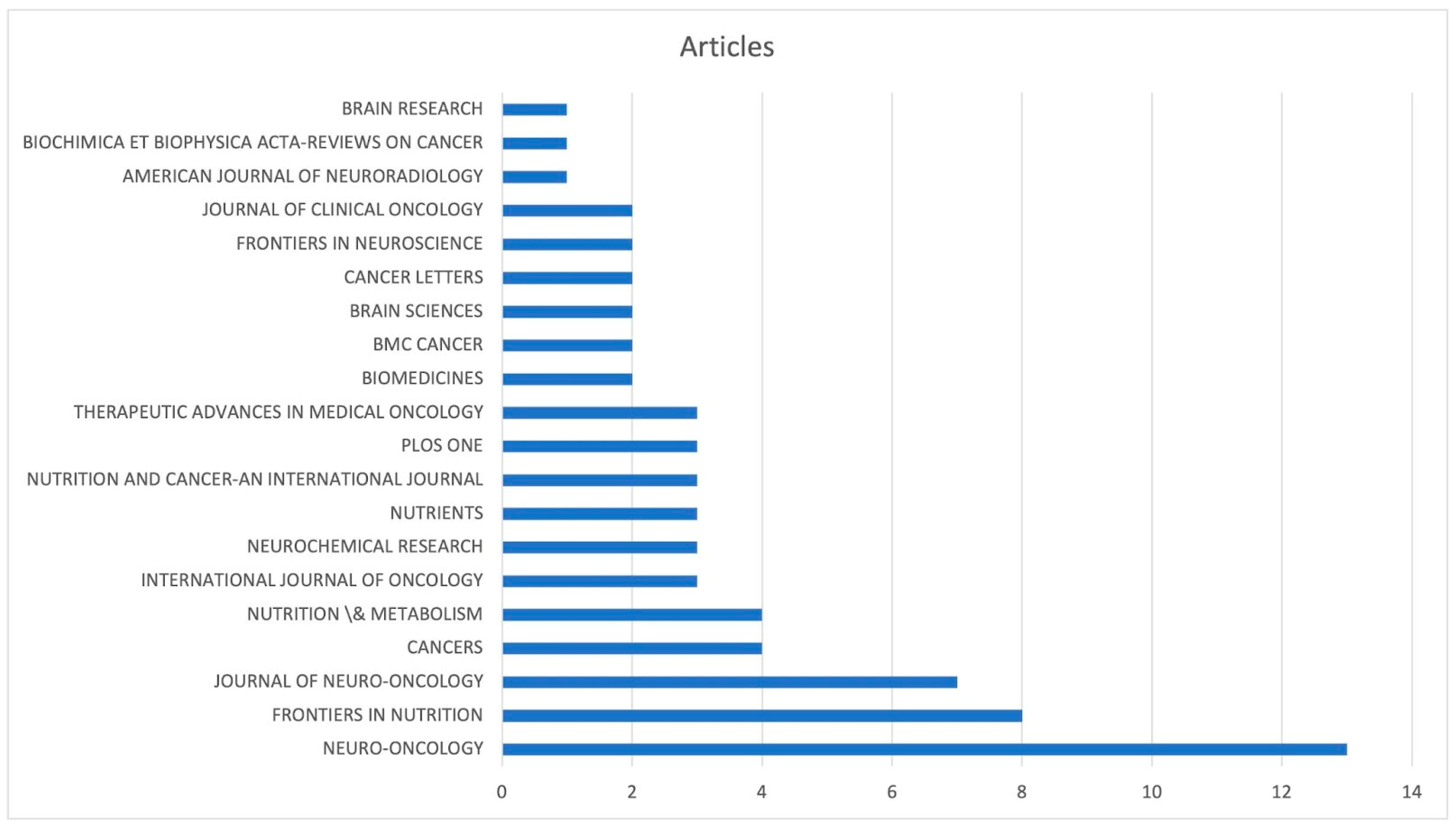
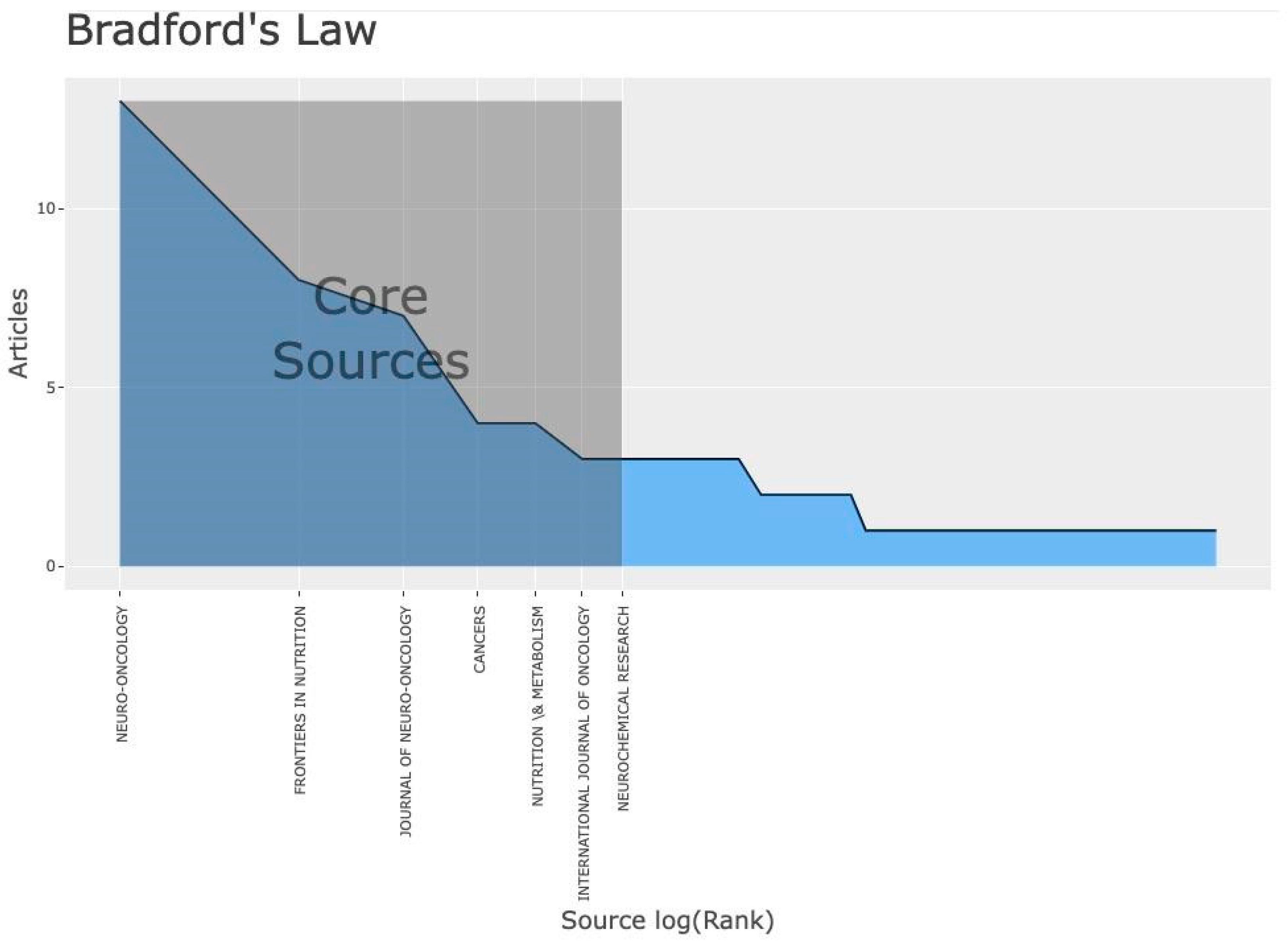
3.2. Background Knowledge
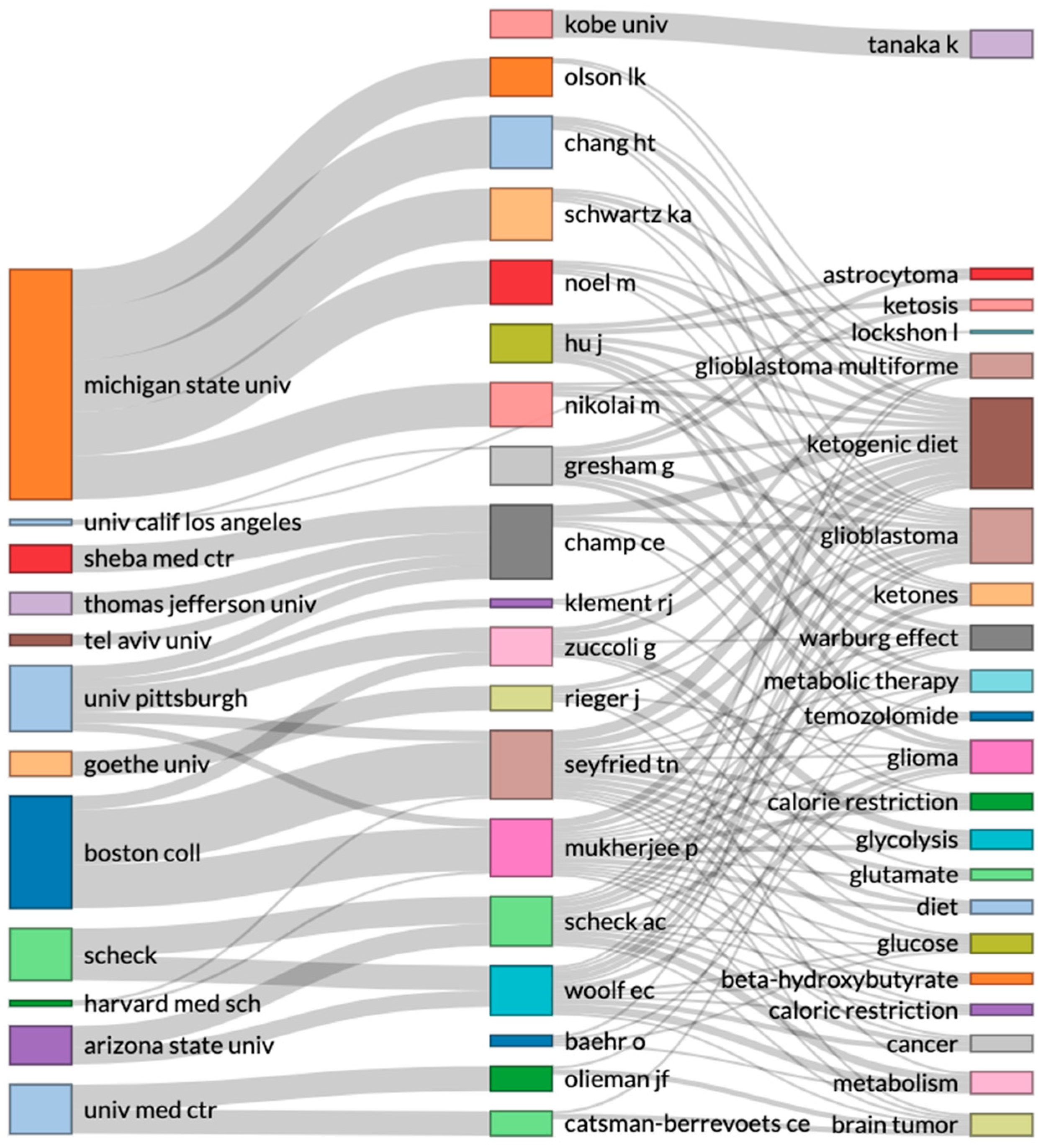
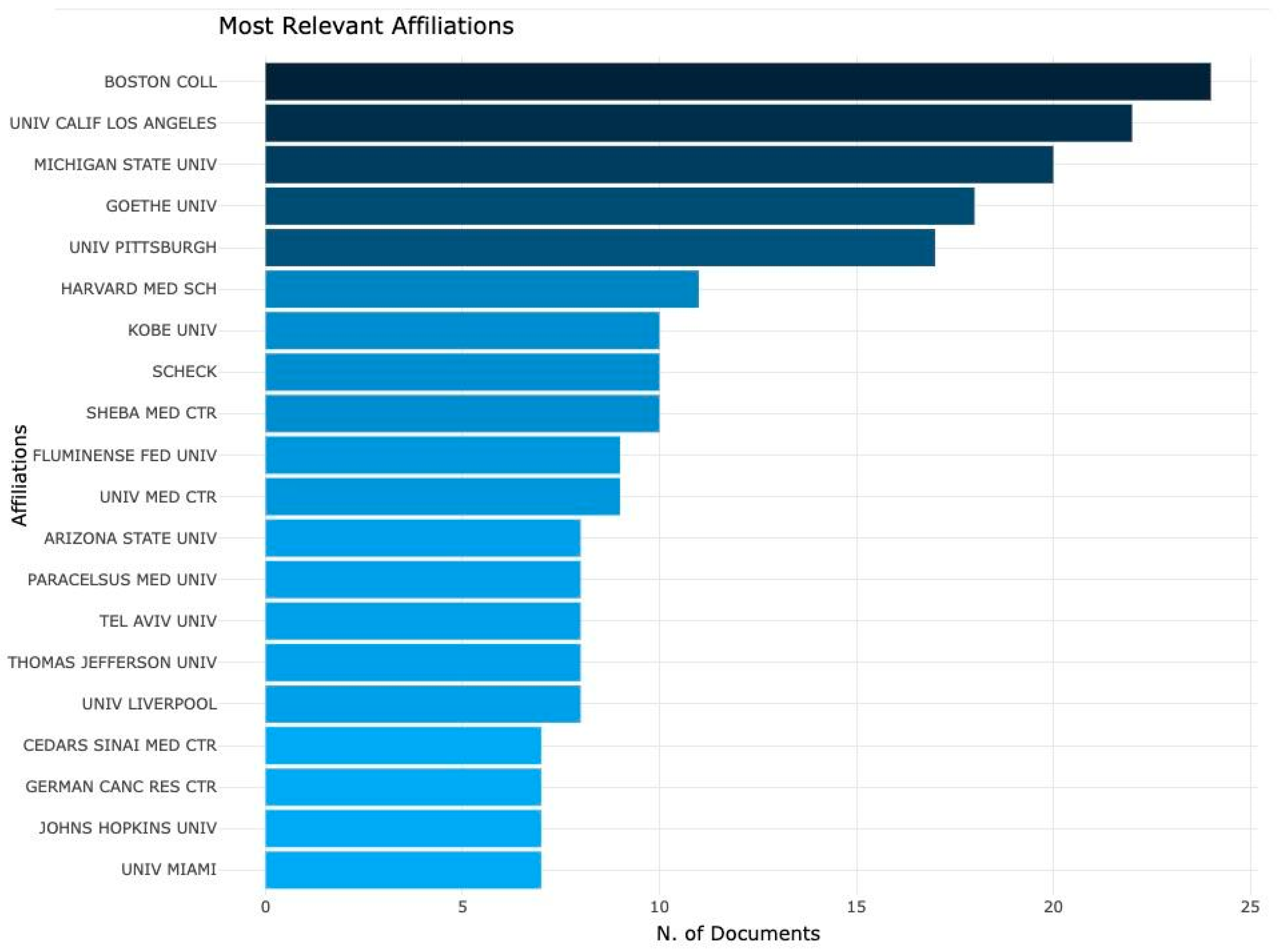
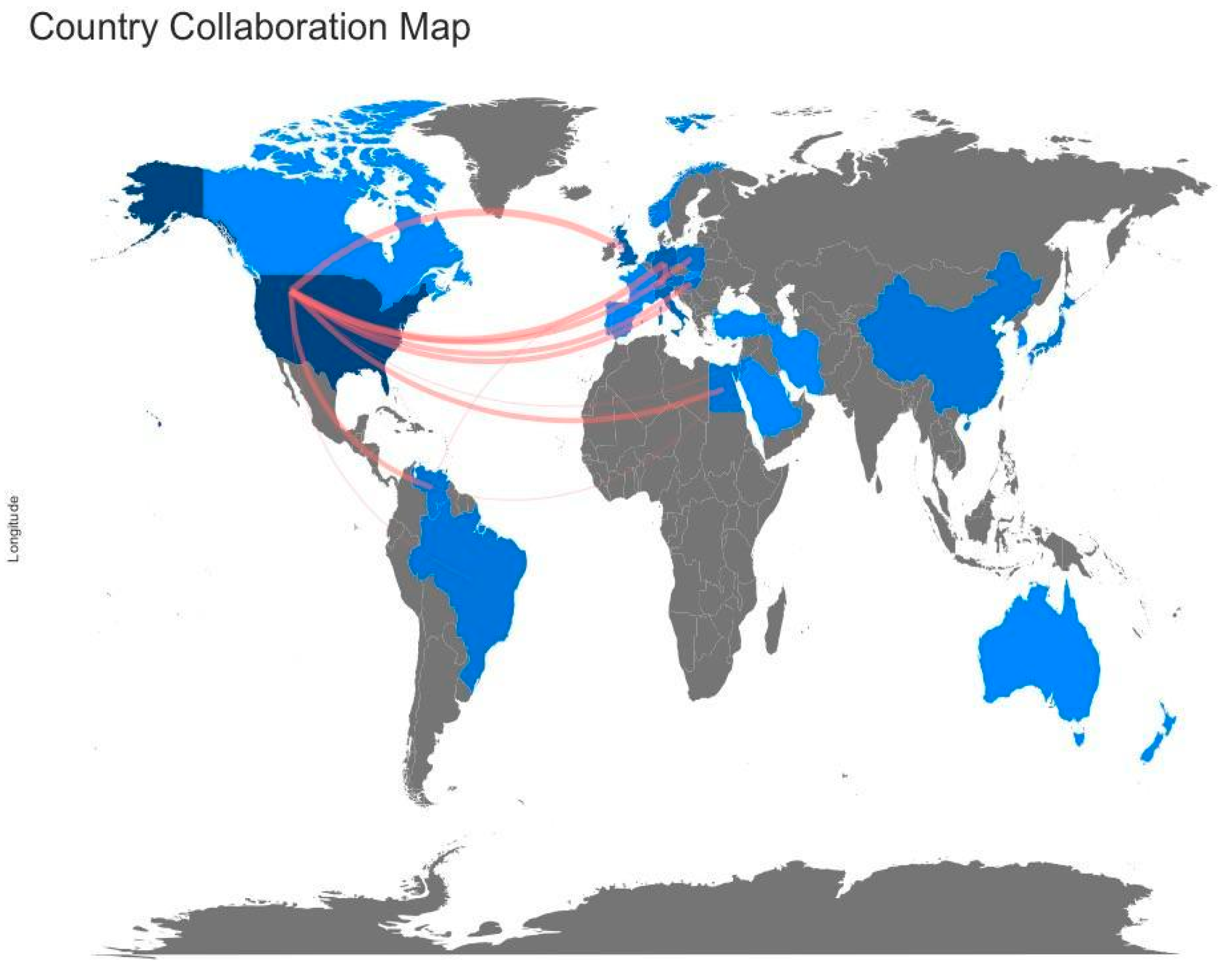
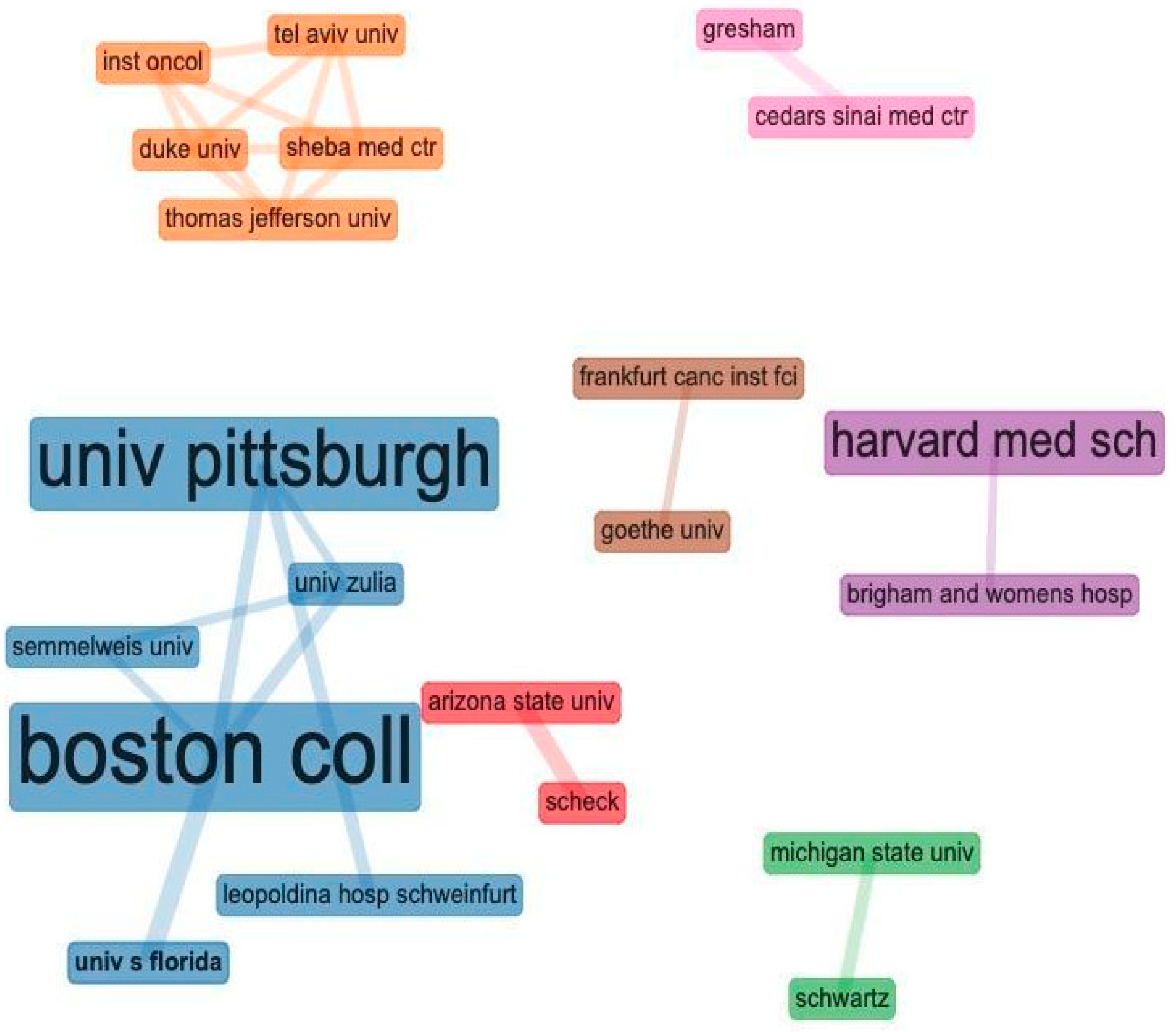
3.3. Cooperations
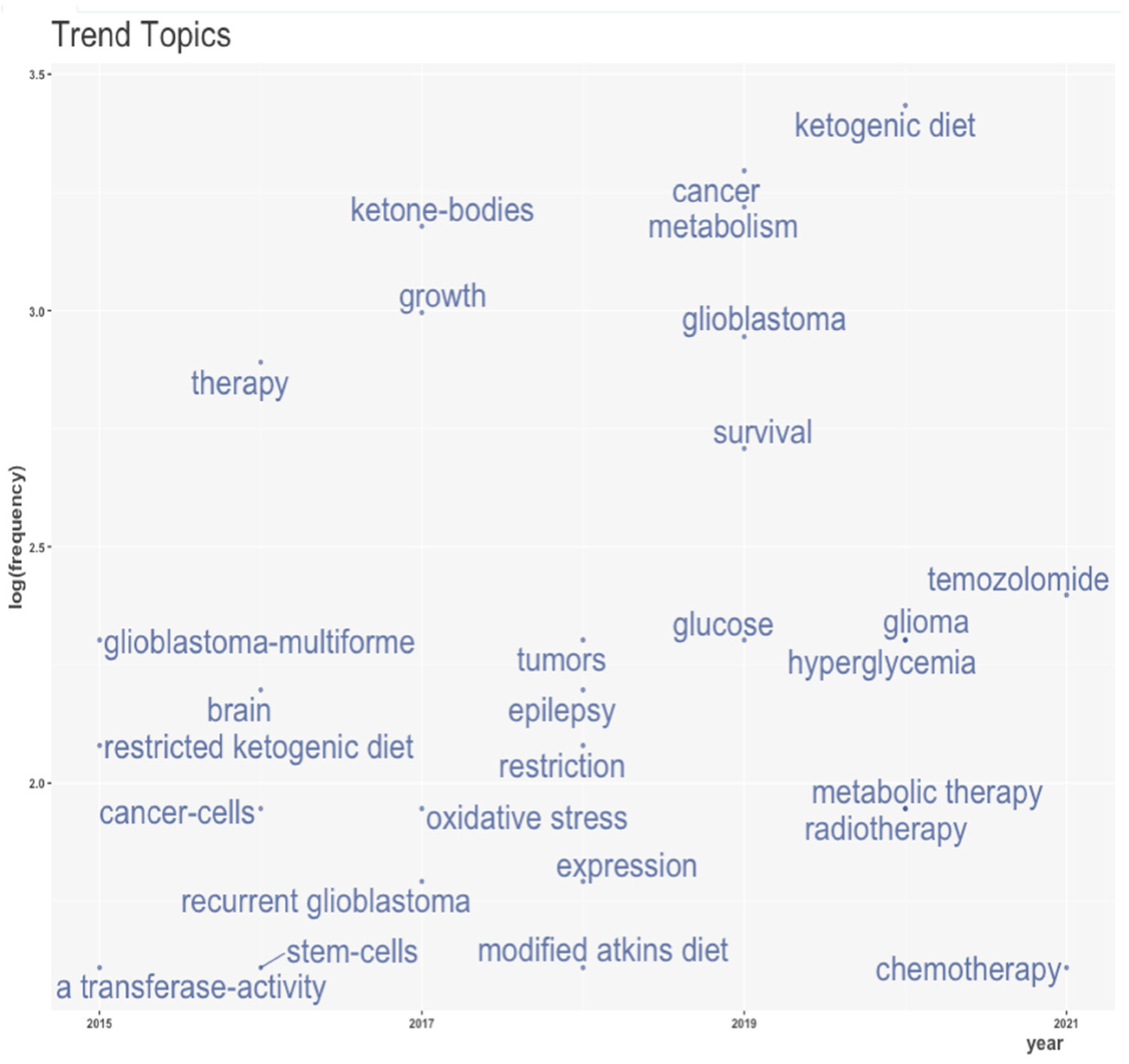
3.4. Research Front
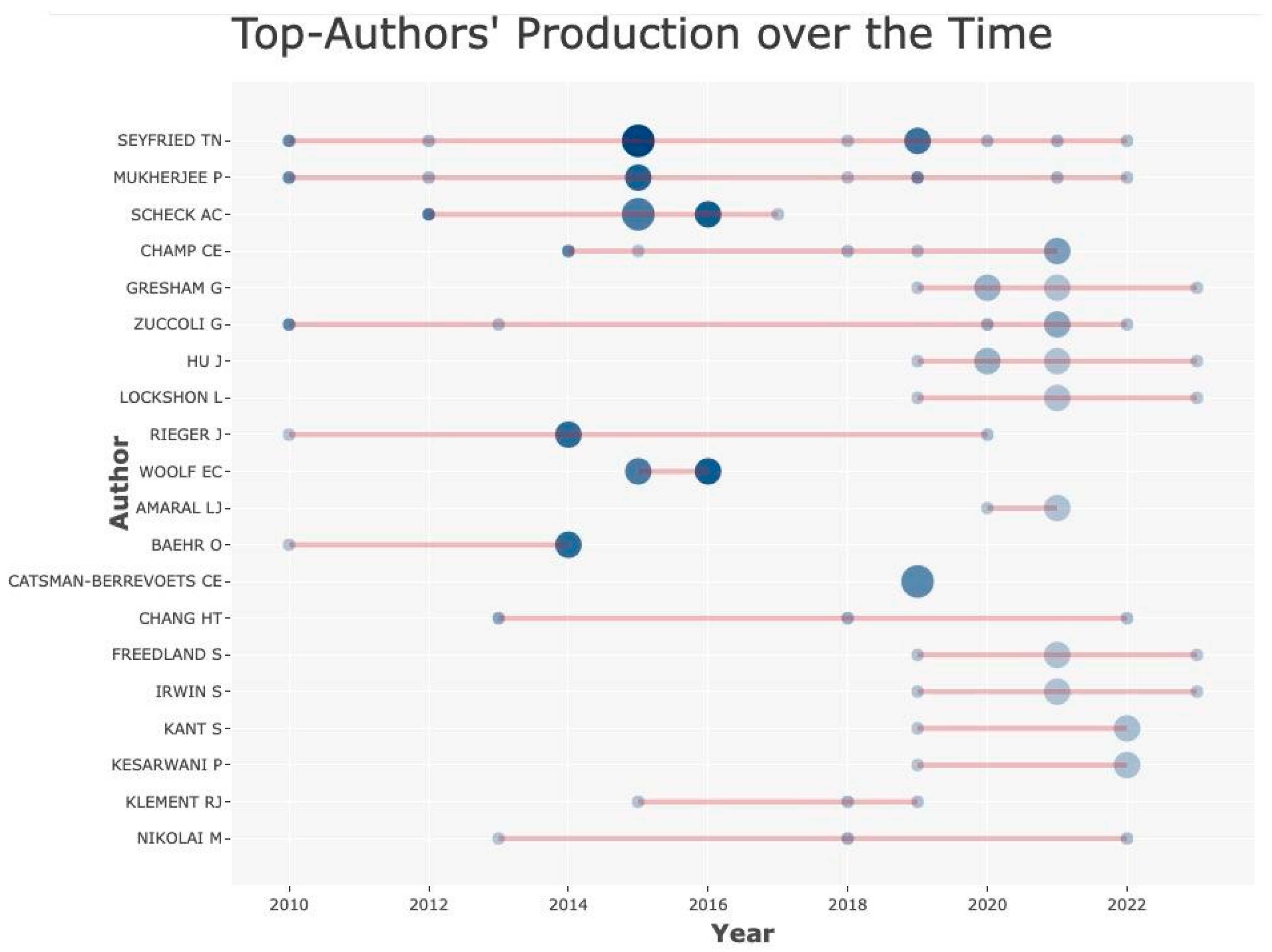
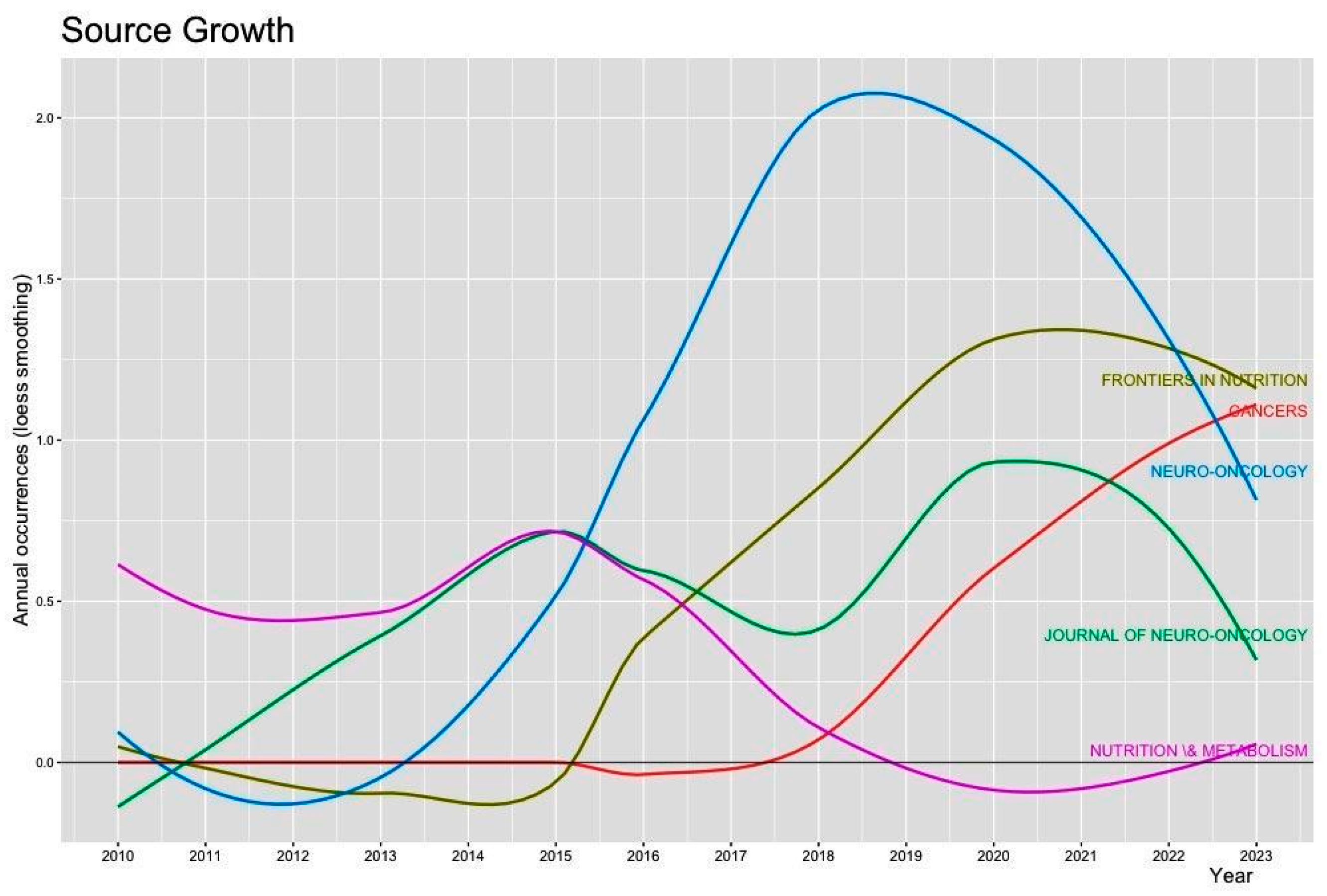
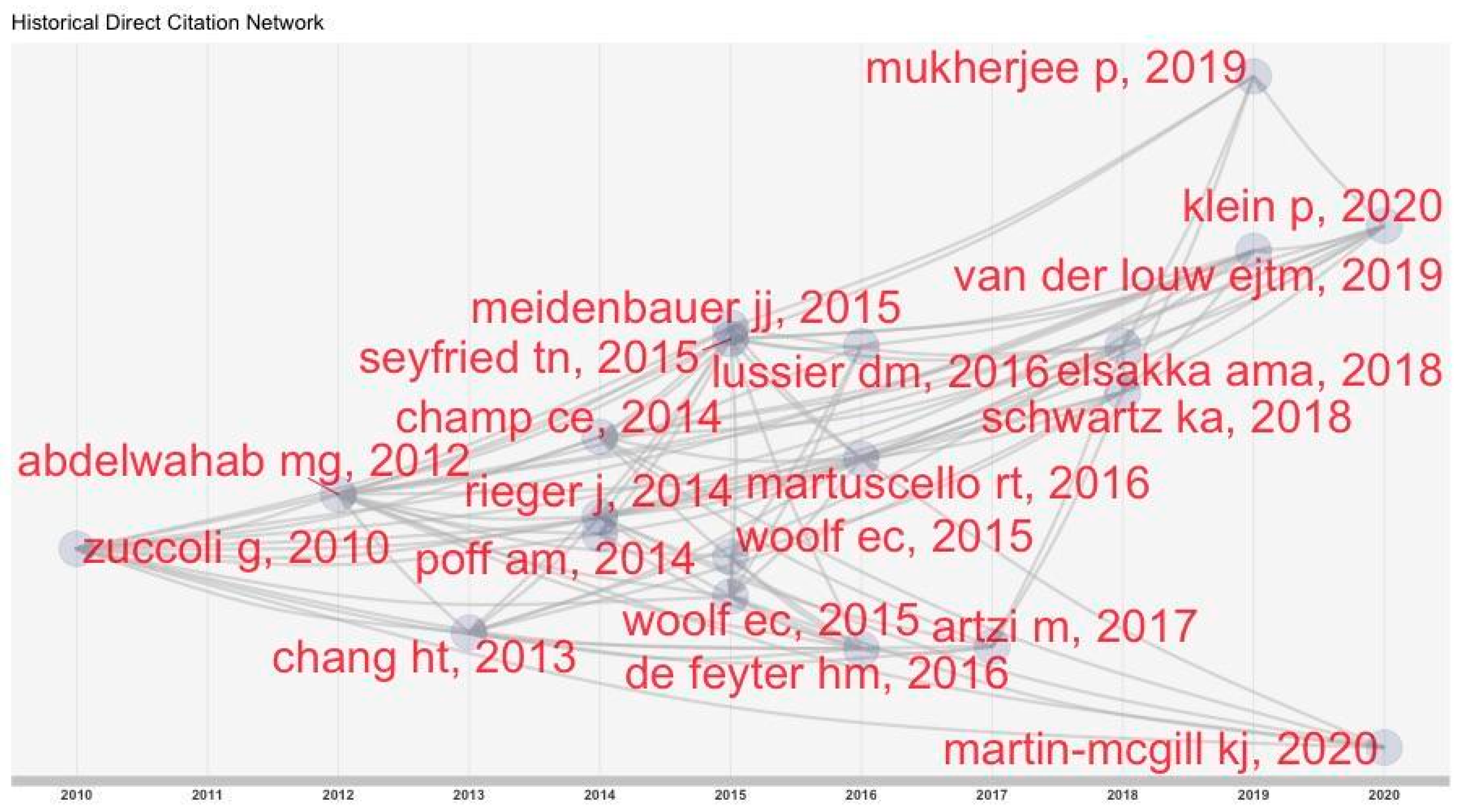
3.5. Historical Overview
4. Discussion
Limitations
5. Conclusions
Author Contributions
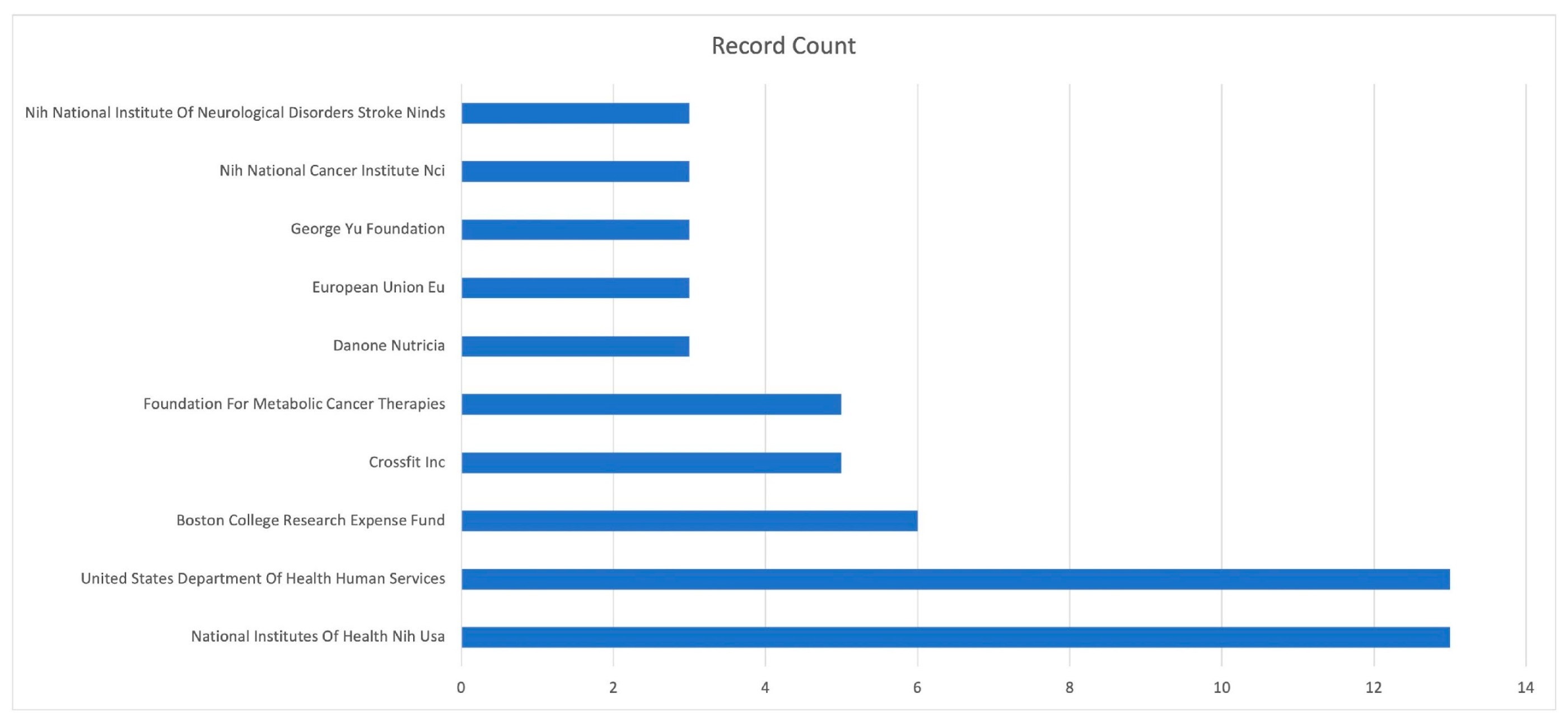
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Grochans, S.; Cybulska, A.M.; Simińska, D.; Korbecki, J.; Kojder, K.; Chlubek, D.; Baranowska-Bosiacka, I. Epidemiology of Glioblastoma Multiforme–Literature Review. Cancers 2022, 14, 2412. [Google Scholar] [CrossRef]
- Ostrom, Q.T.; Cioffi, G.; Waite, K.; Kruchko, C.; Barnholtz-Sloan, J.S. CBTRUS Statistical Report: Primary Brain and Other Central Nervous System Tumors Diagnosed in the United States in 2014–2018. Neuro-Oncol. 2021, 23, iii1–iii105. [Google Scholar] [CrossRef] [PubMed]
- Louis, D.N.; Perry, A.; Wesseling, P.; Brat, D.J.; Cree, I.A.; Figarella-Branger, D.; Hawkins, C.; Ng, H.K.; Pfister, S.M.; Reifenberger, G.; et al. The 2021 WHO Classification of Tumors of the Central Nervous System: A summary. Neuro-Oncol. 2021, 23, 1231–1251. [Google Scholar] [CrossRef] [PubMed]
- Wen, P.Y.; Weller, M.; Lee, E.Q.; Alexander, B.M.; Barnholtz-Sloan, J.S.; Barthel, F.P.; Batchelor, T.T.; Bindra, R.S.; Chang, S.M.; Chiocca, E.A.; et al. Glioblastoma in adults: A Society for Neuro-Oncology (SNO) and European Society of Neuro-Oncology (EANO) consensus review on current management and future directions. Neuro-Oncol. 2020, 22, 1073–1113. [Google Scholar] [CrossRef] [PubMed]
- Germano, I.M.; Ziu, M.; Wen, P.; Ormond, D.R.; Olson, J.J. Congress of Neurological Surgeons systematic review and evidence-based guidelines update on the role of cytotoxic chemotherapy and other cytotoxic therapies in the management of progressive glioblastoma in adults. J. Neuro-Oncol. 2022, 158, 225–253. [Google Scholar] [CrossRef] [PubMed]
- Shimizu, H. Our Experience with Pediatric Epilepsy Surgery Focusing on Corpus Callosotomy and Hemispherotomy. Epilepsia 2005, 46, 30–31. [Google Scholar] [CrossRef] [PubMed]
- Kawabata, S.; Suzuki, M.; Hirose, K.; Tanaka, H.; Kato, T.; Goto, H.; Narita, Y.; Miyatake, S.-I. Accelerator-based BNCT for patients with recurrent glioblastoma: A multicenter phase II study. Neuro-Oncol. Adv. 2021, 3, vdab067. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.-W.; Lee, Y.-Y.; Lin, C.-F.; Pan, P.-S.; Chen, J.-K.; Wang, C.-W.; Hsu, S.-M.; Kuo, Y.-C.; Lan, T.-L.; Hsu, S.P.C.; et al. Salvage Boron Neutron Capture Therapy for Malignant Brain Tumor Patients in Compliance with Emergency and Compassionate Use: Evaluation of 34 Cases in Taiwan. Biology 2021, 10, 334. [Google Scholar] [CrossRef] [PubMed]
- Goel, N.J.; Bird, C.E.; Hicks, W.H.; Abdullah, K.G. Economic implications of the modern treatment paradigm of glioblastoma: An analysis of global cost estimates and their utility for cost assessment. J. Med. Econ. 2021, 24, 1018–1024. [Google Scholar] [CrossRef]
- Fuentes-Raspall, R.; Solans, M.; Roca-Barceló, A.; Vilardell, L.; Puigdemont, M.; del Barco, S.; Comas, R.; García-Velasco, A.; Astudillo, A.; Carmona-Garcia, M.C.; et al. Descriptive epidemiology of primary malignant and non-malignant central nervous tumors in Spain: Results from the Girona Cancer Registry (1994–2013). Cancer Epidemiol. 2017, 50, 1–8. [Google Scholar] [CrossRef]
- Narita, Y.; Shibui, S.; On Behalf of the Committee of Brain Tumor Registry of Japan Supported by the Japan Neurosurgical Society. Trends and Outcomes in the Treatment of Gliomas Based on Data during 2001–2004 from the Brain Tumor Registry of Japan. Neurol. Med.-Chir. 2015, 55, 286–295. [Google Scholar] [CrossRef] [PubMed]
- Seyfried, T.N.; Marsh, J.; Shelton, L.M.; Huysentruyt, L.C.; Mukherjee, P. Is the restricted ketogenic diet a viable alternative to the standard of care for managing malignant brain cancer? Epilepsy Res. 2012, 100, 310–326. [Google Scholar] [CrossRef] [PubMed]
- Sargaço, B.; Oliveira, P.A.; Antunes, M.L.; Moreira, A.C. Effects of the Ketogenic Diet in the Treatment of Gliomas: A Systematic Review. Nutrients 2022, 14, 1007. [Google Scholar] [CrossRef] [PubMed]
- Römer, M.; Dörfler, J.; Huebner, J. The use of ketogenic diets in cancer patients: A systematic review. Clin. Exp. Med. 2021, 21, 501–536. [Google Scholar] [CrossRef] [PubMed]
- Noorlag, L.; De Vos, F.Y.; Kok, A.; Broekman, M.L.; Seute, T.; Robe, P.A.; Snijders, T.J. Treatment of malignant gliomas with ketogenic or caloric restricted diets: A systematic review of preclinical and early clinical studies. Clin. Nutr. 2019, 38, 1986–1994. [Google Scholar] [CrossRef] [PubMed]
- Winter, S.F.; Loebel, F.; Dietrich, J. Role of ketogenic metabolic therapy in malignant glioma: A systematic review. Crit. Rev. Oncol./Hematol. 2017, 112, 41–58. [Google Scholar] [CrossRef]
- Vidali, S.; Aminzadeh, S.; Lambert, B.; Rutherford, T.; Sperl, W.; Kofler, B.; Feichtinger, R.G. Mitochondria: The ketogenic diet—A metabolism-based therapy. Int. J. Biochem. Cell Biol. 2015, 63, 55–59. [Google Scholar] [CrossRef]
- Bello, S.D.; Valdemarin, F.; Martinuzzi, D.; Filippi, F.; Gigli, G.L.; Valente, M. Ketogenic Diet in the Treatment of Gliomas and Glioblastomas. Nutrients 2022, 14, 3851. [Google Scholar] [CrossRef]
- Seyfried, T.N.; Flores, R.; Poff, A.M.; D’agostino, D.P.; Mukherjee, P. Metabolic therapy: A new paradigm for managing malignant brain cancer. Cancer Lett. 2015, 356, 289–300. [Google Scholar] [CrossRef] [PubMed]
- Shingler, E.; Perry, R.; Mitchell, A.; England, C.; Perks, C.; Herbert, G.; Ness, A.; Atkinson, C. Dietary restriction during the treatment of cancer: Results of a systematic scoping review. BMC Cancer 2019, 19, 811. [Google Scholar] [CrossRef] [PubMed]
- Deshmukh, R.; Allega, M.F.; Tardito, S. A map of the altered glioma metabolism. Trends Mol. Med. 2021, 27, 1045–1059. [Google Scholar] [CrossRef]
- Klement, R.J.; Bandyopadhyay, P.S.; Champ, C.E.; Walach, H. Application of Bayesian evidence synthesis to modelling the effect of ketogenic therapy on survival of high grade glioma patients. Theor. Biol. Med. Model. 2018, 15, 12. [Google Scholar] [CrossRef]
- Al-Jada, D.N.; Takruri, H.R.; Talib, W.H. From antiepileptic therapy to promising adjuvant in medical oncology: A historical view of the ketogenic diet. PharmaNutrition 2023, 24, 100340. [Google Scholar] [CrossRef]
- Weber, D.D.; Aminzadeh-Gohari, S.; Tulipan, J.; Catalano, L.; Feichtinger, R.G.; Kofler, B. Ketogenic diet in the treatment of cancer—Where do we stand? Mol. Metab. 2020, 33, 102–121. [Google Scholar] [CrossRef] [PubMed]
- Aria, M.; Cuccurullo, C. bibliometrix: An R-tool for comprehensive science mapping analysis. J. Informetr. 2017, 11, 959–975. [Google Scholar] [CrossRef]
- Bailón-Moreno, R.; Jurado-Alameda, E.; Ruiz-Baños, R.; Courtial, J.P. Bibliometric laws: Empirical flaws of fit. Scientometrics 2005, 63, 209–229. [Google Scholar] [CrossRef]
- Bradford, S. Sources of Information on Scientific Subjects. Eng. Illus Wkly J. 1934, 137, 85–86. [Google Scholar]
- Tennant, D.A.; Durán, R.V.; Gottlieb, E. Targeting metabolic transformation for cancer therapy. Nat. Rev. Cancer 2010, 10, 267–277. [Google Scholar] [CrossRef] [PubMed]
- Abdelwahab, M.G.; Fenton, K.E.; Preul, M.C.; Rho, J.M.; Lynch, A.; Stafford, P.; Scheck, A.C. The Ketogenic Diet Is an Effective Adjuvant to Radiation Therapy for the Treatment of Malignant Glioma. PLoS ONE 2012, 7, e36197. [Google Scholar] [CrossRef] [PubMed]
- Haar, C.P.; Hebbar, P.; Wallace, G.C.T.; Das, A.; Vandergrift, W.A., 3rd; Smith, J.A.; Giglio, P.; Patel, S.J.; Ray, S.K.; Banik, N.L. Drug Resistance in Glioblastoma: A Mini Review. Neurochem. Res. 2012, 37, 1192–1200. [Google Scholar] [CrossRef] [PubMed]
- Rieger, J.; Bähr, O.; Maurer, G.D.; Hattingen, E.; Franz, K.; Brucker, D.; Walenta, S.; Kämmerer, U.; Coy, J.F.; Weller, M.; et al. ERGO: A pilot study of ketogenic diet in recurrent glioblastoma. Int. J. Oncol. 2014, 44, 1843–1852. [Google Scholar] [CrossRef]
- Champ, C.E.; Palmer, J.D.; Volek, J.S.; Werner-Wasik, M.; Andrews, D.W.; Evans, J.J.; Glass, J.; Kim, L.; Shi, W. Targeting metabolism with a ketogenic diet during the treatment of glioblastoma multiforme. J. Neuro-Oncol. 2014, 117, 125–131. [Google Scholar] [CrossRef]
- Chang, H.T.; Olson, L.K.; Schwartz, K.A. Ketolytic and glycolytic enzymatic expression profiles in malignant gliomas: Implication for ketogenic diet therapy. Nutr. Metab. 2013, 10, 47. [Google Scholar] [CrossRef]
- Tan-Shalaby, J.L.; Carrick, J.; Edinger, K.; Genovese, D.; Liman, A.D.; Passero, V.A.; Shah, R.B. Modified Atkins diet in advanced malignancies-final results of a safety and feasibility trial within the Veterans Affairs Pittsburgh Healthcare System. Nutr. Metab. 2016, 13, 52. [Google Scholar] [CrossRef]
- Feichtinger, R.G.; Weis, S.; Mayr, J.A.; Zimmermann, F.; Geilberger, R.; Sperl, W.; Kofler, B. Alterations of oxidative phosphorylation complexes in astrocytomas. Glia 2014, 62, 514–525. [Google Scholar] [CrossRef]
- Poff, A.; Ari, C.; Arnold, P.; Seyfried, T.; D’Agostino, D. Ketone supplementation decreases tumor cell viability and prolongs survival of mice with metastatic cancer. Int. J. Cancer 2014, 135, 1711–1720. [Google Scholar] [CrossRef] [PubMed]
- Lussier, D.M.; Woolf, E.C.; Johnson, J.L.; Brooks, K.S.; Blattman, J.N.; Scheck, A.C. Enhanced immunity in a mouse model of malignant glioma is mediated by a therapeutic ketogenic diet. BMC Cancer 2016, 16, 310. [Google Scholar] [CrossRef]
- Woolf, E.C.; Curley, K.L.; Liu, Q.; Turner, G.H.; Charlton, J.A.; Preul, M.C.; Scheck, A.C. The Ketogenic Diet Alters the Hypoxic Response and Affects Expression of Proteins Associated with Angiogenesis, Invasive Potential and Vascular Permeability in a Mouse Glioma Model. PLoS ONE 2015, 10, e0130357. [Google Scholar] [CrossRef] [PubMed]
- Martuscello, R.T.; Vedam-Mai, V.; McCarthy, D.J.; Schmoll, M.E.; Jundi, M.A.; Louviere, C.D.; Griffith, B.G.; Skinner, C.L.; Suslov, O.; Deleyrolle, L.P.; et al. A Supplemented High-Fat Low-Carbohydrate Diet for the Treatment of Glioblastoma. Clin. Cancer Res. 2016, 22, 2482–2495. [Google Scholar] [CrossRef] [PubMed]
- De Feyter, H.M.; Behar, K.L.; Rao, J.U.; Madden-Hennessey, K.; Ip, K.L.; Hyder, F.; Drewes, L.R.; Geschwind, J.-F.; de Graaf, R.A.; Rothman, D.L. A ketogenic diet increases transport and oxidation of ketone bodies in RG2 and 9L gliomas without affecting tumor growth. Neuro-Oncol. 2016, 18, 1079–1087. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, L.; Seyfried, T.; Alfarouk, K.O.; Moreira, J.D.V.; Fais, S. Out of Warburg effect: An effective cancer treatment targeting the tumor specific metabolism and dysregulated pH. Semin. Cancer Biol. 2017, 43, 134–138. [Google Scholar] [CrossRef]
- Woolf, E.C.; Syed, N.; Scheck, A.C. Tumor Metabolism, the Ketogenic Diet and β-Hydroxybutyrate: Novel Approaches to Adjuvant Brain Tumor Therapy. Front. Mol. Neurosci. 2016, 9, 122. [Google Scholar] [CrossRef]
- Landis, C.J.; Tran, A.N.; Scott, S.E.; Griguer, C.; Hjelmeland, A.B. The pro-tumorigenic effects of metabolic alterations in glioblastoma including brain tumor initiating cells. Biochim. Biophys. Acta-Rev. Cancer 2018, 1869, 175–188. [Google Scholar] [CrossRef]
- Zuccoli, G.; Marcello, N.; Pisanello, A.; Servadei, F.; Vaccaro, S.; Mukherjee, P.; Seyfried, T.N. Metabolic management of glioblastoma multiforme using standard therapy together with a restricted ketogenic diet: Case Report. Nutr. Metab. 2010, 7, 33. [Google Scholar] [CrossRef] [PubMed]
- Mukherjee, P.; Augur, Z.M.; Li, M.; Hill, C.; Greenwood, B.; Domin, M.A.; Kondakci, G.; Narain, N.R.; Kiebish, M.A.; Bronson, R.T.; et al. Therapeutic benefit of combining calorie-restricted ketogenic diet and glutamine targeting in late-stage experimental glioblastoma. Commun. Biol. 2019, 2, 200. [Google Scholar] [CrossRef] [PubMed]
- Stupp, R.; Taillibert, S.; Kanner, A.; Read, W.; Steinberg, D.M.; Lhermitte, B.; Toms, S.; Idbaih, A.; Ahluwalia, M.S.; Fink, K.; et al. Effect of Tumor-Treating Fields Plus Maintenance Temozolomide vs Maintenance Temozolomide Alone on Survival in Patients with Glioblastoma: A Randomized Clinical Trial. JAMA 2017, 318, 2306–2316. [Google Scholar] [CrossRef]
- Wick, W.; Stupp, R.; Gorlia, T.; Bendszus, M.; Sahm, F.; Bromberg, J.E.; Brandes, A.A.; Vos, M.J.; Domont, J.; Idbaih, A.; et al. Phase II part of EORTC study 26101: The sequence of bevacizumab and lomustine in patients with first recurrence of a glioblastoma. J. Clin. Oncol. 2016, 34, 2019. [Google Scholar] [CrossRef]
- Reardon, D.A.; Schuster, J.; Tran, D.D.; Fink, K.L.; Nabors, L.B.; Li, G.; Bota, D.A.; Lukas, R.V.; Desjardins, A.; Ashby, L.S.; et al. ReACT: Overall survival from a randomized phase II study of rindopepimut (CDX-110) plus bevacizumab in relapsed glioblastoma. J. Clin. Oncol. 2015, 33, 2009. [Google Scholar] [CrossRef]
- Zhao, K.; Yu, C.M.; Gan, Z.M.; Huang, M.M.; Wu, T.M.; Zhao, N. Rehabilitation therapy for patients with glioma. Medicine 2020, 99, e23087. [Google Scholar] [CrossRef] [PubMed]
- Nikolai, M.; Noel, M.; Schwartz, K.; Kurniali, P.; Chang, H.; Olson, L.K. Energy restricted ketogenic diet (ERKD) treatment for advanced glioblastoma multiforme (GBM): Case report. FASEB J. 2013, 27, lb302. [Google Scholar] [CrossRef]
















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| https://www.webofscience.com/wos/woscc/summary/9c5ac2ac-0b72-42c3-9931-b23b7ad4b4e5-b89a8e8e/relevance/1 (accessed on 5 January 2024) |
| Main Information about | Description | Results |
|---|---|---|
| Data | ||
| Timespan | 2010:2023 | |
| Sources (Journals, Books, etc) | 70 | |
| Documents | 119 | |
| Average years from publication | 5.66 | |
| Average citations per document | 36.85 | |
| Average citations per year per doc | 4.26 | |
| References | 4647 | |
| Document types | ||
| Article | 60 | |
| Article; early access | 1 | |
| Correction | 2 | |
| Editorial material | 2 | |
| Letter | 2 | |
| Meeting abstract | 17 | |
| Review | 35 | |
| Document contents | ||
| Keywords Plus | 424 | |
| Author’s Keywords | 269 | |
| Authors | ||
| Authors | 568 | |
| Author Appearances | 714 | |
| Authors of single-authored documents | 1 | |
| Authors of multi-authored documents | 567 | |
| Author collaboration | ||
| Single-authored documents | 1 | |
| Documents per Author | 0.21 | |
| Co-Authors per Documents | 6 | |
| Collaboration Index | 4.81 |
| Paper | Year | Study Design | Journal | Total Citations | Total Citations per Year |
|---|---|---|---|---|---|
| Tennant DA et al. [28] | 2010 | Review | Nature Review Cancers | 863 | 57,533 |
| Abdelwahab MG et al. [29] | 2012 | Laboratory study | Plos One | 186 | 14,308 |
| Haar CP et al. [30] | 2012 | Mini review | Neurochem Res | 183 | 14,077 |
| Rieger J et al. [31] | 2014 | Case series (N = 20) | Int J Oncol | 179 | 16,273 |
| Zuccoli G et al. [44] | 2010 | Case report | Nutr Metab | 171 | 11.4 |
| Champ CE et al. [32] | 2014 | Case series (N = 6) | J Neuro-Oncol | 138 | 12,545 |
| Seyfried TN et al. [19] | 2015 | Mini review | Cancer Lett | 128 | 12.8 |
| Poff AM et al. [36] | 2014 | Laboratory study | Int J Cancer | 125 | 11,364 |
| Vidali S ET et al. [17] | 2015 | Review | Int J Biochem Cell Biol | 115 | 11.5 |
| Lussier DM et al. [37] | 2016 | Laboratory study | Bmc Cancer | 99 | 11 |
| Schwartz L et al. [41] | 2017 | Review | Semin Cancer Biol | 95 | 11,875 |
| Woolf EC et al. [38] | 2015 | Laboratory study | Plos One | 75 | 7.5 |
| Woolf EC et al. [42] | 2016 | Review | Front Molec Neurosci | 74 | 8222 |
| Martuscello RT et al. [39] | 2016 | Laboratory study | Clin Cancer Res | 71 | 7889 |
| Mukherjee P et al. [45] | 2019 | Laboratory study | Commun Biol | 67 | 11,167 |
| Chang HT et al. [33] | 2013 | Case series (N = 22) | Nutr Metab | 67 | 5583 |
| Tan-Shalaby Jl et al. [34] | 2016 | Case series (N = 17) | Nutr Metab | 63 | 7 |
| De Feyter HM et al. [40] | 2016 | Laboratory study | Euro-Oncology | 63 | 7 |
| Feichtinger RG et al. [31] | 2014 | Case series (N = 25) | Glia | 62 | 5636 |
| Landis CJ et al. [43] | 2018 | Review | Biochim Biophys Acta-Rev Cancer | 61 | 8714 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Brotis, A.G.; Arvaniti, C.; Kontou, M.; Tsekouras, A.; Fountas, K.N. Ketogenic Diet in the Management of Glioblastomas: A Bibliometric Analysis. Neuroglia 2024, 5, 63-79. https://doi.org/10.3390/neuroglia5020005
Brotis AG, Arvaniti C, Kontou M, Tsekouras A, Fountas KN. Ketogenic Diet in the Management of Glioblastomas: A Bibliometric Analysis. Neuroglia. 2024; 5(2):63-79. https://doi.org/10.3390/neuroglia5020005
Chicago/Turabian StyleBrotis, Alexandros G., Christina Arvaniti, Marina Kontou, Alexandros Tsekouras, and Kostas N. Fountas. 2024. "Ketogenic Diet in the Management of Glioblastomas: A Bibliometric Analysis" Neuroglia 5, no. 2: 63-79. https://doi.org/10.3390/neuroglia5020005