1. Introduction
Operators of heavy equipment are exposed to high levels of whole-body vibration (WBV) [
1,
2,
3]. The literature has shown an association between increased low back pain (LBP) and anthropometric factors such as increased height [
4] and increased body mass [
4,
5]. WBV has been related to a variety of adverse health outcomes including degenerative changes in the spine [
6,
7], low back pain [
7,
8,
9] and sciatic nerve pain [
7,
9]. WBV exposure can lead to increased muscle activation and spinal instability [
10], thus increasing the back injury risk [
10,
11,
12].
ISO 2631-1 provides health guidance zones for vibration exposure. ISO 2631-1 provides health weightings that are used to determine RMS (root mean square) values of frequency weighted acceleration [
13]. Once the RMS acceleration values have been determined, they can be compared to the health guidance caution zones, assuming exposure times of 4–8 h [
13]. These caution zones are used to evaluate the risks of injury related to WBV; however, anthropometric factors are not incorporated into the risk estimation, although they may affect the vibration dose [
3,
5,
13,
14].
The relationship between vibration dose and anthropometric factors during WBV has been investigated in vehicles [
14], machinery [
3,
15], and vibration simulators [
16,
17,
18,
19,
20]. Increased BMI has been associated with a decreased vibration dose in the z-axis [
3,
5,
14]. Individuals with an increased BMI tend to report increased levels of comfort when exposed to WBV [
15] which may indicate that increased BMI may lead to vibration attenuation [
3,
14]. Further studies have indicated that increased BMI is associated with an increase in the vibration power absorbed (VPA) [
17]. Similarly, increased body mass has also been found to be associated with increased VPA [
16,
17,
19,
20]. In comparison to body mass and BMI, increased height is associated with an increased vibration dose [
5].
Furthermore, the impedance of the human body is strongly correlated with body mass up to approximately 4 Hz, with larger body masses having a higher impedance, leading to lower resonant frequencies [
18]. Similarly, increased BMI has been associated with a decreased resonant frequency of the human body [
21]. It has also been indicated that female participants have increased damping when compared to male participants. Female participants exhibited a decreased peak VPA, and a lower frequency at which the peak VPA occurred [
20]. However, Dewangan et al. has suggested that sex effects in relation to the VPA are strongly coupled with anthropometric factors which may be due in part to the increased body fat content and reduced lean body mass of females relative to males [
20]. It has also been proposed that body mass impacts the damping characteristics of air-filled cushions used in suspension seats [
19]. In mechanical seat suspensions it has been found that an increased vibration dose is experienced by individuals with a smaller body mass [
22].
The literature has shown an association between low back pain (LBP) and anthropometric factors such as height [
4,
5] and BMI [
4,
5,
23] in farmers who are exposed to WBV. For example, Seidel et al. showed that spinal stress during WBV varied according to body mass and height [
24]. WBV exposure leads to increased loading in the spine [
25], increased trunk muscle activation [
12], trunk muscle fatigue and decreased spine stability. Prolonged muscle activation has been shown to be a contributing factor to repetitive strain injuries [
26].
Several studies have suggested that prolonged exposure to WBV leads to muscle fatigue [
27,
28], where both WBV exposure and muscle fatigue lead to increased levels of muscle activation [
27,
29]. Muscle fatigue when experienced separately to WBV may lead to neuromuscular recruitment errors, which may lead to increased injury risk [
30]. Similarly, when back muscle fatigue and WBV exposure are experienced, concurrently muscle latency, muscle activation, and discomfort are increased [
31], leading to escalated back injury risk [
32,
33,
34,
35]. Furthermore, muscle activation in the trunk significantly alters the biodynamics for the seated body under WBV [
36].
Although literature has suggested that anthropometric factors influence vibration dose [
3,
5,
15,
20] and risk of low back pain [
4,
37], no studies have investigated the relationship between anthropometric factors, muscle fatigue, and muscle activation during WBV. Muscle activation may contribute to risk of injury and low back pain through both prolonged activation [
26] or inadequate activation [
38], compromising spine stability [
39]. Therefore, to understand the relationships between the anthropometry of the driver (height, body mass, BMI) and muscle activation, the purpose of this study was to quantify the relationships between trunk muscle activation and selected anthropometric factors both pre- and post-fatigue during WBV exposure.
3. Results
Of the 29 participants included in this study, 1 participant had a BMI in the obesity class 2 range (male), 4 participants had a BMI within the obesity class 1 range (1 female, 3 male), 5 were pre-obesity (1 female, 4 male), 1 was underweight (male) and 18 were within the normal range (9 male, 9 female) based on the BMI classes outlined by the World Health Organization [
50].
3.1. Spearman’s Rank Coefficient of Correlation
Muscle activation and vibration frequency were positively correlated for pre-fatigue transformed %MVE data (%MVET) of the IO (ρ = 0.25, p < 0.0001), LE (ρ = 0.17, p < 0.0001), and TE (ρ = 0.17, p < 0.0001), but negatively correlated in the EO (ρ = −0.16, p < 0.0001). Post-fatigue, the EO (ρ = 0.17, p < 0.0001), IO (ρ = 0.27, p < 0.0001), LE (ρ = 0.19, p < 0.0001), and TE (ρ = 0.20, p < 0.0001) showed positive correlations of similar magnitudes. Participants showed increased muscle activation with increasing frequency for all muscles. BMI showed positive correlations with IO (ρ = 0.34, p < 0.0001), LE (ρ = 0.14, p < 0.0001) and TE (ρ= 0.11, p < 0.0001) pre-fatigue, and continued to show similar trends post-fatigue with Spearman’s rho values of 0.30 (p < 0.0001), 0.10 (p < 0.0001) and 0.15 (p < 0.0001) for the IO, LE, and TE, respectively. BMI did not exhibit significant correlations with %MVET of the EO. These results indicate increased muscle activation with increased BMI in the IO, LE and TE. Pre-fatigue, height was negatively correlated with IO (ρ = −0.34, p < 0.0001), and TE (ρ = −0.20, p < 0.0001), while the EO (ρ = 0.38, p < 0.0001) and LE (ρ = 0.38, p < 0.0001) exhibited a positive correlation. Post-fatigue, height was negatively correlated with EO (ρ = −0.41, p < 0.0001), IO (ρ = −0.28, p < 0.0001), and TE (ρ = −0.17, p < 0.0001), while the LE (ρ = 0.35, p < 0.0001) exhibited a positive correlation. Thus, participants exhibited decreased muscle activation with increased height in the IO, and TE pre- and post-fatigue, while exhibiting increased muscle activation with increased height in the LE. However, in the EO, participants exhibited increased muscle activation with increased height pre-fatigue and decreased muscle activation with increased height post-fatigue. Pre-fatigue, significant correlations between body mass and EO (ρ = 0.13, p < 0.0001), IO (ρ = 0.20, p < 0.0001), LE (ρ = 0.40, p < 0.0001) and TE (ρ = 0.08, p = 0.004) were observed. Furthermore, significant correlations of a similar magnitude between the %MVET and body mass were observed post-fatigue in EO (ρ = −0.18, p < 0.0001), IO (ρ = 0.20, p < 0.0001), LE (ρ = 0.35, p < 0.0001) and TE (ρ = 0.11, p < 0.0001). Therefore, participants exhibited increased muscle activation with increasing body mass in the EO, IO, LE, and TE pre-fatigue and in the IO, LE and TE post-fatigue.
A further analysis performed for each frequency group showed similar findings; however, the correlation between muscle activation and body mass in the pre-fatigue EO was not significant at 1.25 Hz and 4.5 Hz, and the correlation between muscle activation and BMI was not significant in the pre-fatigue LE at 1.25 Hz (
Table 1). In the TE, the correlations between %MVE
T and mass were not significant for any frequency pre-fatigue, and the correlation between %MVE
T and BMI was not significant from 1.25 to 2.5 Hz in the pre-fatigue data. In the pre-fatigue data, the largest correlations between muscle activation and BMI occurred in the IO, while the largest correlation between muscle activation and body mass occurred in the LE. Interestingly, the IO, EO, and LE all showed similar magnitudes of correlations between muscle activation and height, although the IO showcased a negative correlation while the EO and LE were positive.
In the IO, the post-fatigue data shows a slightly lower correlation between %MVE and height (
Table 2). Further, in the EO, the correlations between %MVE and mass as well as %MVE and height are lower magnitude than the pre-fatigue correlation coefficients for all frequencies. Interestingly, in the EO, muscle activation was correlated positively with both height and mass pre-fatigue, however, post-fatigue muscle activation of the EO is negatively correlated with both body mass and height. Similar to the pre-fatigue data, the % MVE
T of the LE did not show a significant correlation with BMI at 1.25 Hz, however, post-fatigue, the LE does not exhibit a significant correlation with BMI from 1.25 Hz to 2.5 Hz. Furthermore, pre-fatigue the TE does not show a significant correlation with mass at any frequency, however the correlations are significant for all frequencies except 2.5 Hz and 4.5 Hz post-fatigue.
3.2. Stepwise Linear Regression Models
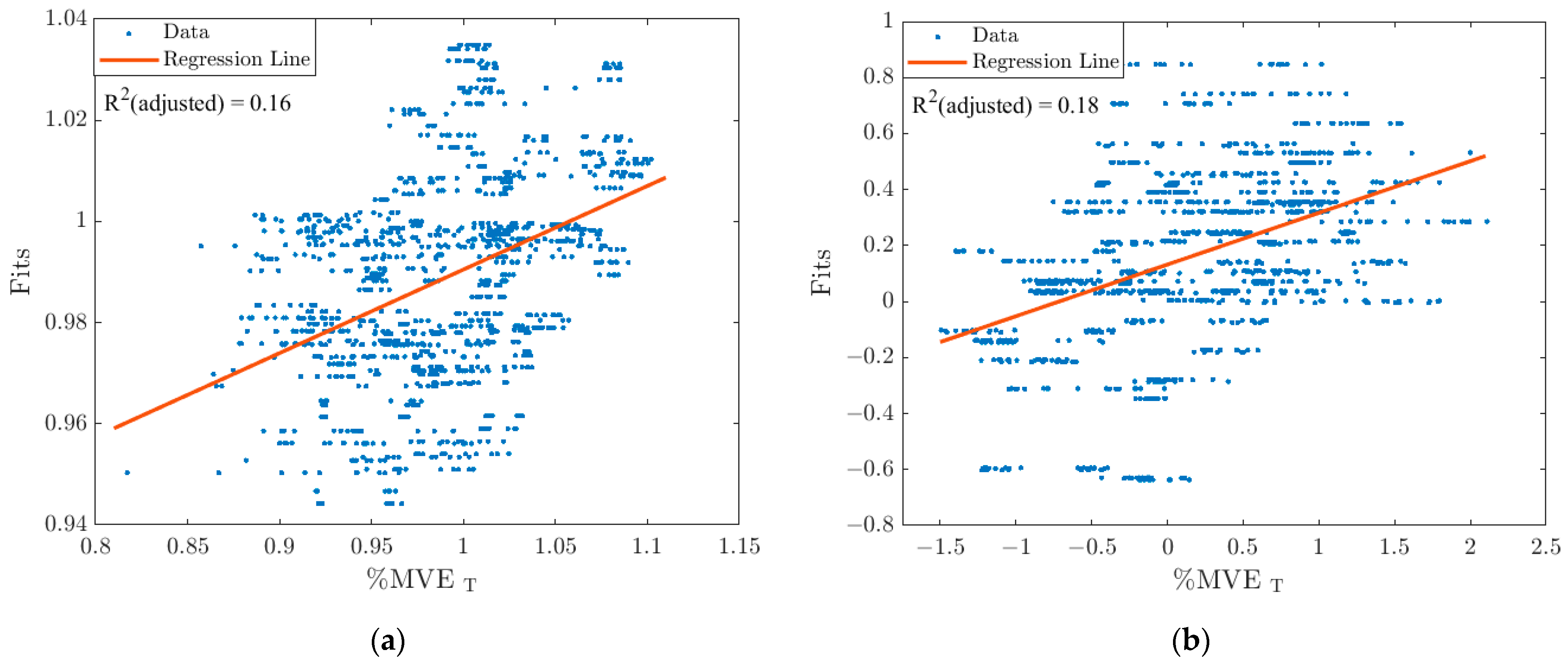
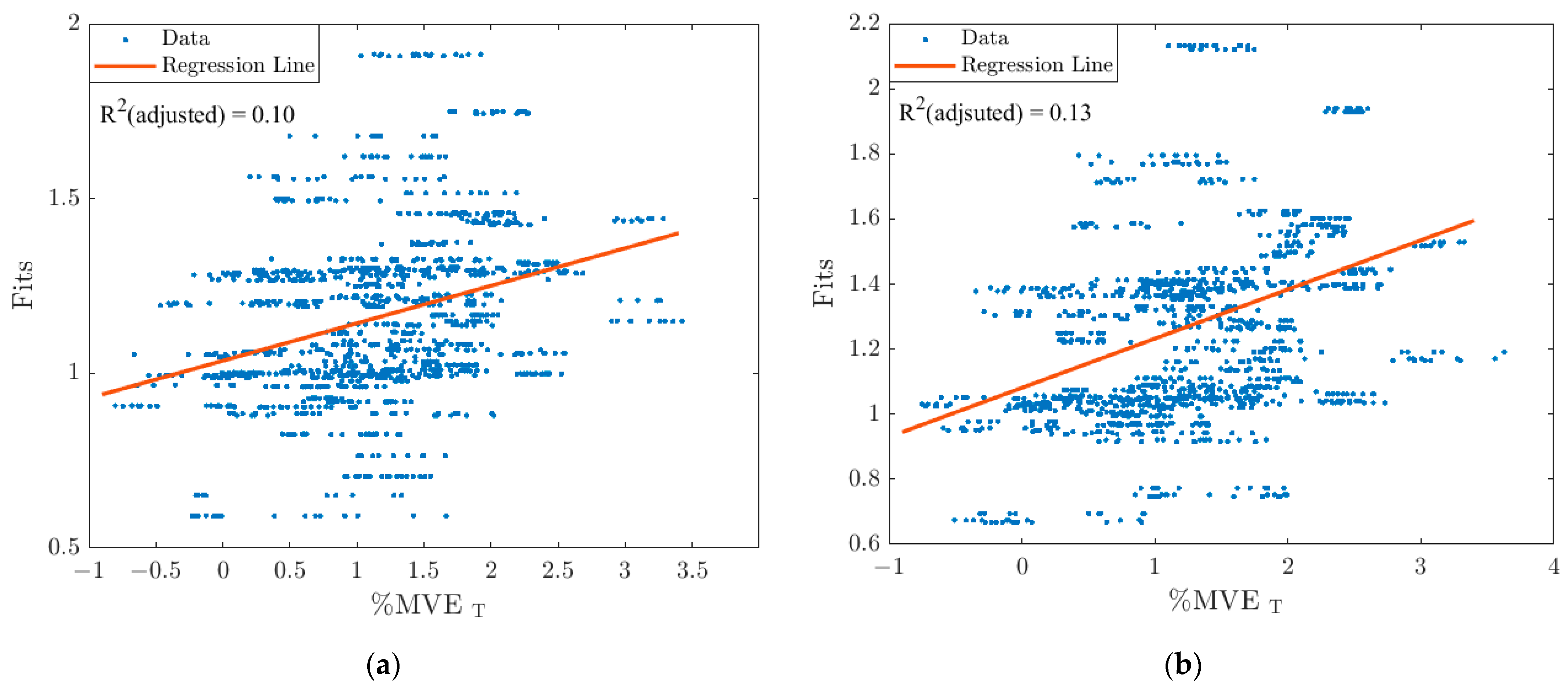
When comparing the pre- and post-fatigue regression models of the EO, there is a minimal change in the R
2 (adj) value, with a difference of 0.03 (
Figure 3). The regression equations for the pre-fatigue and post-fatigue regression models are presented in
Table 3.
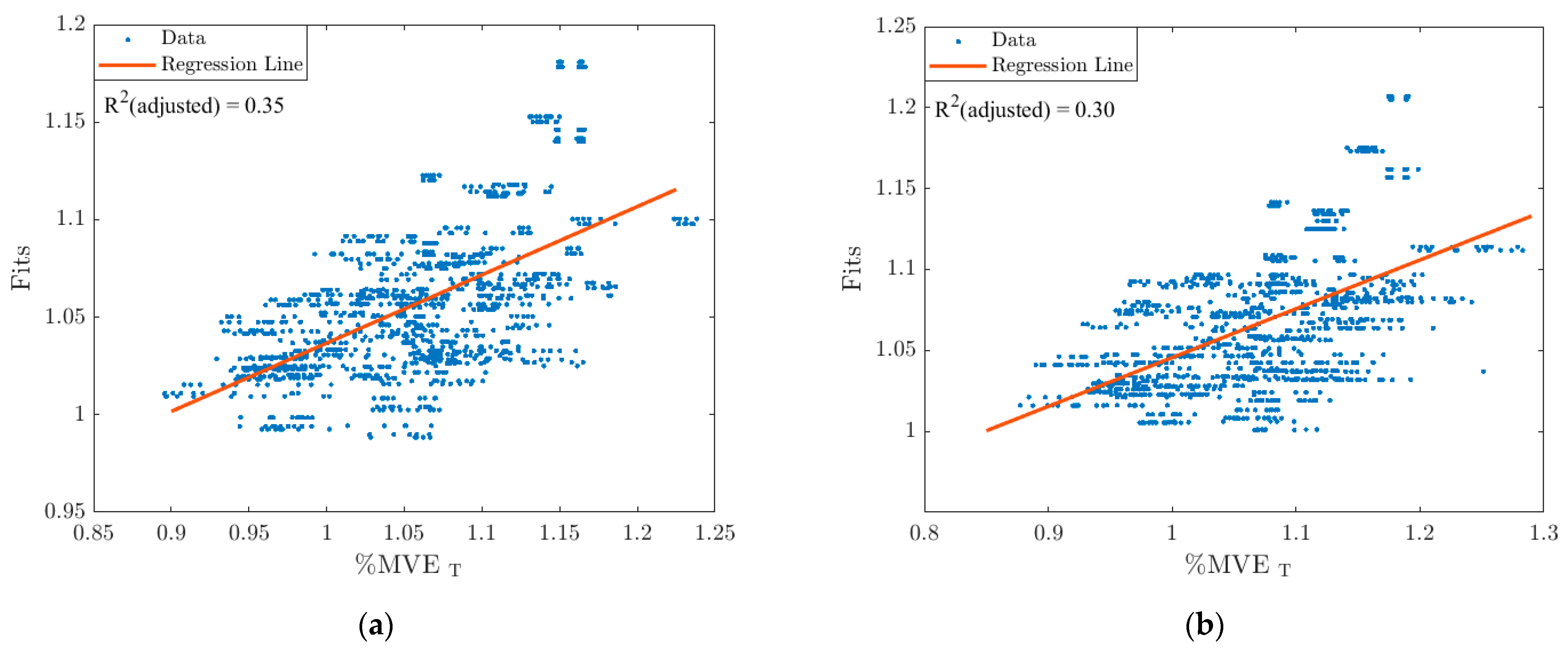
The IO showed the largest difference in R
2 (adj) values of all the muscles. The pre-fatigue regression was able to explain an additional 5% of the variance in the %MVE
T data compared to the post-fatigue regression model (
Figure 4). The resultant regression model equations for the pre-fatigue and post-fatigue models are presented in
Table 4.
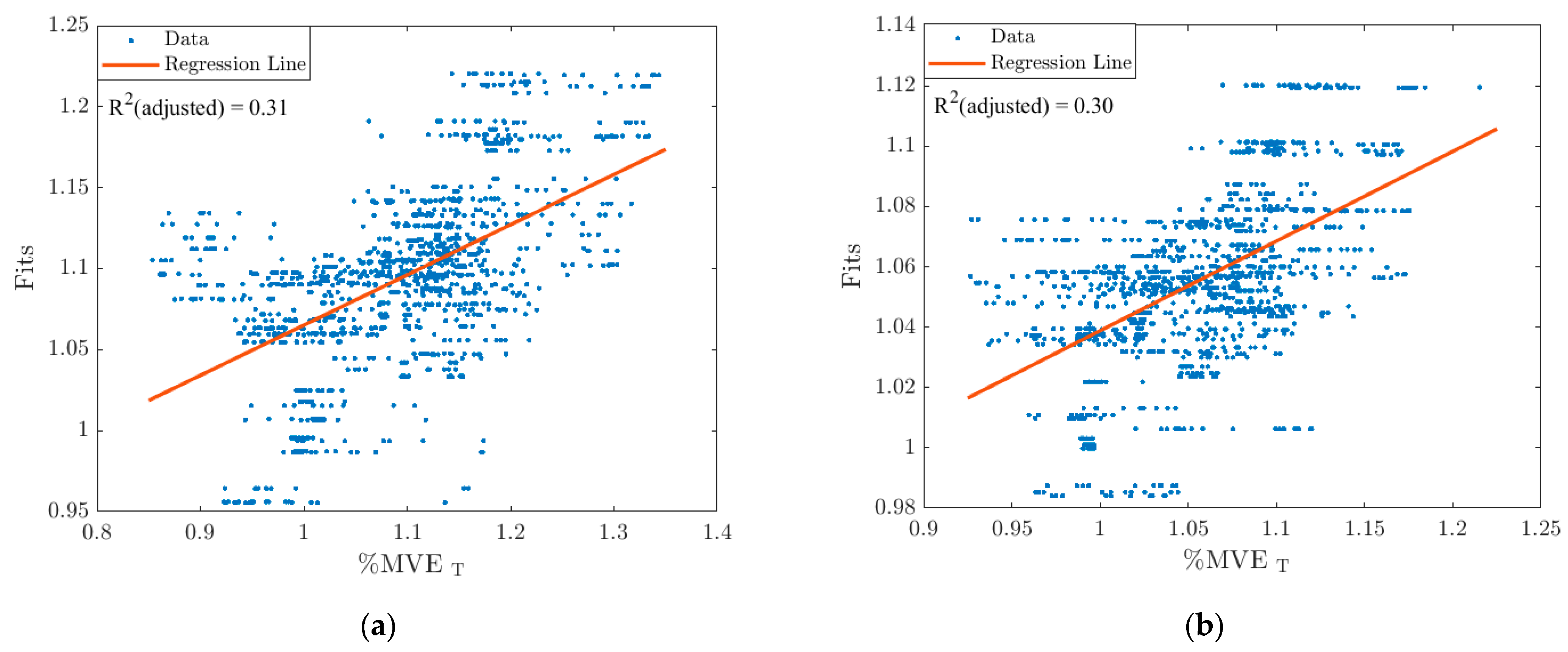
The LE shows minimal changes in the R
2 (adj) value and the regression equations (
Table 5) between the pre- and post-fatigue regression results (
Figure 5).
The TE shows minimal changes in the R
2 (adj) value depending on the fatigue condition and the resultant regression model equations (
Figure 6). The regression equations for the pre- and post-fatigue models presented in
Figure 6 are summarized in
Table 6.
When anthropometric factors are excluded from the regression, and frequency is the only factor considered, the resultant pre-fatigue regressions have R2 (adj) values of 0.03, 0.08, 0.02, and 0.03 for the EO, IO, LE and TE, respectively. The post-fatigue regressions result in R2 (adj) values of 0.04, 0.90, 0.04 and 0.05 for the EO, IO, LE and TE, respectively, when frequency is the only factor. These results indicate that using frequency alone describes a small amount of the variance in muscle activation of the muscle groups studied compared to using a combination of frequency and anthropometric factors. The incorporation of anthropometric factors and frequency in the regressions results in increased R2 (adj) values for all muscle groups investigated in both the pre- and post-fatigue regressions. Overall, the weakest regression models were in the TE followed by the EO, while the LE and IO regressions have the largest R2 (adj) values.
4. Discussion
The IO, LE, and TE showed significant positive correlations with frequency in both the pre-and post-fatigue data while the EO exhibited a negative correlation pre-fatigue and a positive correlation post-fatigue. Additionally, frequency was a significant term in the regression models for all muscle groups. This positive correlation may be explained by the forcing frequency of the vibration approaching the peak transmissibility of the thoracic and lumbar spines. When exposed to vertical WBV, peak muscle activation in the thoracic and lumbar erector spinae occurs between 4 and 5 Hz [
27], which corresponds to the peak transmissibility of the thoracic and lumbar spines, which occurs at 4 Hz [
27]. The negative correlation between muscle activation in the EO pre-fatigue may suggest that participants relied more on the IO, LE, and TE to stabilize their spine pre-fatigue. The positive correlation post-fatigue may suggest that participants began increasing activation of their EO once their erector spinae were fatigued.
IO, LE, and TE resulted in significant positive correlations with BMI as well as body mass, both of which may lead to increased shear forces on the spine [
24]. The neuromuscular system often responds to increased forces within the spine by increasing overall trunk muscle activation [
38], as this may provide additional stability to the lumbar spine [
39]. Although this increased muscle activation is necessary to maintain spine stability, it may lead to increased shear and compression forces on the spine, introducing risk of tissue injury [
36]. In contrast to IO, EO had a negative correlation with body mass and post-fatigue. This aligns with previous findings, in which an increased body mass was correlated with reduced WBV transmission [
14], thus reducing the muscle activation necessary to stabilize the spine.
Like increased body mass and increased BMI, increased height may lead to increased shear forces within the spine [
24]. Furthermore, it has been shown that vertical vibration transmission through the thorax is increased in individuals of increased height in the frequencies investigated [
38], thus thoracic muscle activation would be expected to increase to maintain spine stability [
39]. However, the correlation between height and muscle activation was negative in the IO and TE both pre- and post-fatigue, as well as negative in the EO post-fatigue. This indicates decreased levels of muscle activation with increased height. Pre- and post-fatigue in the LE, and pre-fatigue in the EO, participants demonstrated increased muscle activation with increased height. This would be beneficial for stabilizing the spine, but the negative correlations observed in the IO, TE, and post-fatigue EO may lead to decreased spine stability due to reduced thoracic muscle activation. This finding may be a contributing factor to the association between low back pain and increased body height in farmers [
4]. Therefore, when returning to work following a WBV related low-back injury it may be beneficial to train operators to properly engage the muscles of the abdomen to brace their thorax and increase spine stability during WBV exposure.
Furthermore, the incorporation of anthropometric factors in addition to frequency greatly improved the fit of the regressions, allowing an explanation of 11–35% of the variation in muscle activation, as compared to 2–9% of the variance which was accounted for using frequency alone. However, ISO 2631-1 health guidance caution zones are based on frequency weighted RMS acceleration [
13]. The current study suggests that ISO health guidance should consider body mass, BMI, and height in addition to frequency weighted RMS acceleration as these anthropometric factors may influence muscle activation during seated WBV exposure and influence the risk of low back injury when exposed to WBV.
The current problem with the ISO standard is that according to our accelerometry measurements and the determination of the RMS values of the frequency weighted acceleration, all of our participants were in the same health guidance zone. However, our data suggests that their injury risk levels were likely not equal as evidenced by their different muscle activations. When applying the health guidance caution zones from ISO 2631-1, this results in an underestimation of risk in some individuals and an overestimation in others. Moreover, by analyzing pre- and post- fatigue data, we have shown that these potential differences in risk level are present regardless of muscle fatigue status. The evidence that we present is that individuals of increased height as well as individuals of increased BMI may have increased risk both prior to and following fatigue. The increased risk with height is due to lower muscle activation in the thoracic erector spinae (TE), external oblique (EO) and internal oblique (IO) muscles, which may result in decreased spinal stability [
39]. Increased risk with increasing BMI is due to increased muscle activation in the IO, LE, and TE, which may lead to increased risk of soft tissue injury [
36].
Although the values of the frequency weighted RMS accelerations are different across the five frequency levels (i.e., due to the peak-to-peak displacement always being 5 mm), they result in all participants falling into the same health guidance caution zone because the frequency values are not different enough from each other. Moreover, the health frequency weighted RMS accelerations are all below the lower boundary of the health guidance caution zone.
We propose adding additional features for consideration in health guidance alongside the frequency weighted accelerations. The determination of appropriate features will require much more research, which includes both retrospective and prospective epidemiological studies, as well as a better understanding of how body resonant frequencies are affected by factors such as body composition and seat contact area. This research may also include a sensitivity analysis to determine at which point increased height begins to increase injury risk due to decreased muscle activation and thus decreased spine stability. Furthermore, the point at which increased BMI begins to increase tissue injury risk due to increased muscle activation should also be investigated. This would require a larger and more anthropometrically diverse sample population than the population investigated in this study. This sensitivity analysis could include further factors such as body type (e.g., endomorphic, ectomorphic, mesomorphic), lean body mass, % body fat, age, sex, and the anthropometric variables investigated in this study to determine which factors are the most robust predictors of muscle activation.
Several studies have suggested that obesity is related to decreased postural stability in standing tasks [
51,
52,
53] which may be due to the increased torque necessary to stabilize the body [
54], or poor sensory input from the foot mechanoreceptors [
55]. Body weight, height, and age have also been shown to be predictors of postural stability [
56]. Furthermore, Arora et al. demonstrated decreased postural stability during seated WBV exposure as evidenced by an increased center of pressure (COP) displacement and an increased mean velocity of COP displacement [
12]. Thus, the effect of anthropometric factors on postural stability during seated WBV should be investigated. Increased muscle activation in conjunction with increased forces in the spine due to WBV can lead to muscle fatigue and spinal instability, increasing the back injury risk [
10,
57]. It is therefore important to consider the effect of anthropometric factors on muscle activation, since this may lead to an increased back injury risk.
One of the limitations of the current study was the lack of posture monitoring during data collection, therefore, it cannot be ruled out that some of the differences in muscle activation may be due to postural changes. Additionally, BMI does not differentiate between body fat and muscle [
58]. It has been suggested that body fat and muscle mass may impact the resonant frequency of the human body due to their anti-thixotropic and thixotropic properties, respectively [
20]. To provide a more complete picture of the correlations between muscle activation and driver anthropometry, further research should be conducted to evaluate muscle activations throughout the range of human torso resonant frequencies (i.e., 4–14 Hz). Furthermore, lean body mass [
20], body fat, and hip circumference [
59] should also be considered due their influence on biodynamics during WBV exposure.
5. Conclusions
The results indicate increased muscle activation in individuals with increased body mass and BMI in all the trunk muscle groups investigated (EO, IO, LE, TE (pre-fatigue)), as well as decreased muscle activation with increased height in the IO and TE, as well as the EO post-fatigue. The increased activation with increased body mass and BMI may be due to the body responding by increasing thoracic muscle activation to increase spinal stability. Muscle activation was expected to increase with increased height, which is necessary to increase spine stability. However, the results show that muscle activation in the IO, TE, and post-fatigue EO decreased with increasing height. This may be a contributing factor to the increased incidence of low back pain in taller farmers. Additionally, there is increased muscle activation in the IO, LE, TE, and post-fatigue EO with an increased vertical vibration frequency. This is likely due to the vibration frequency approaching the resonant frequency of the thoracic and lumbar spines, requiring increased muscle activation to maintain spinal stability.
The incorporation of BMI, body mass, and height with vibration frequency greatly improves the explanation of variance in the muscle activation of the trunk muscles. These anthropometric differences may pre-dispose certain groups to increased risk of low back injury due to decreased muscle activation leading to decreased spine stability or increased activation leading to risk of repetitive strain injuries. Therefore, this research suggests that ISO 2631-1 health guidance may need to consider anthropometric factors to capture their potential influence on injury risk.









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}