
Model Predictive Control and Its Role in Biomedical Therapeutic Automation: A Brief Review




Abstract
:1. Introduction
1.1. Background of MPC
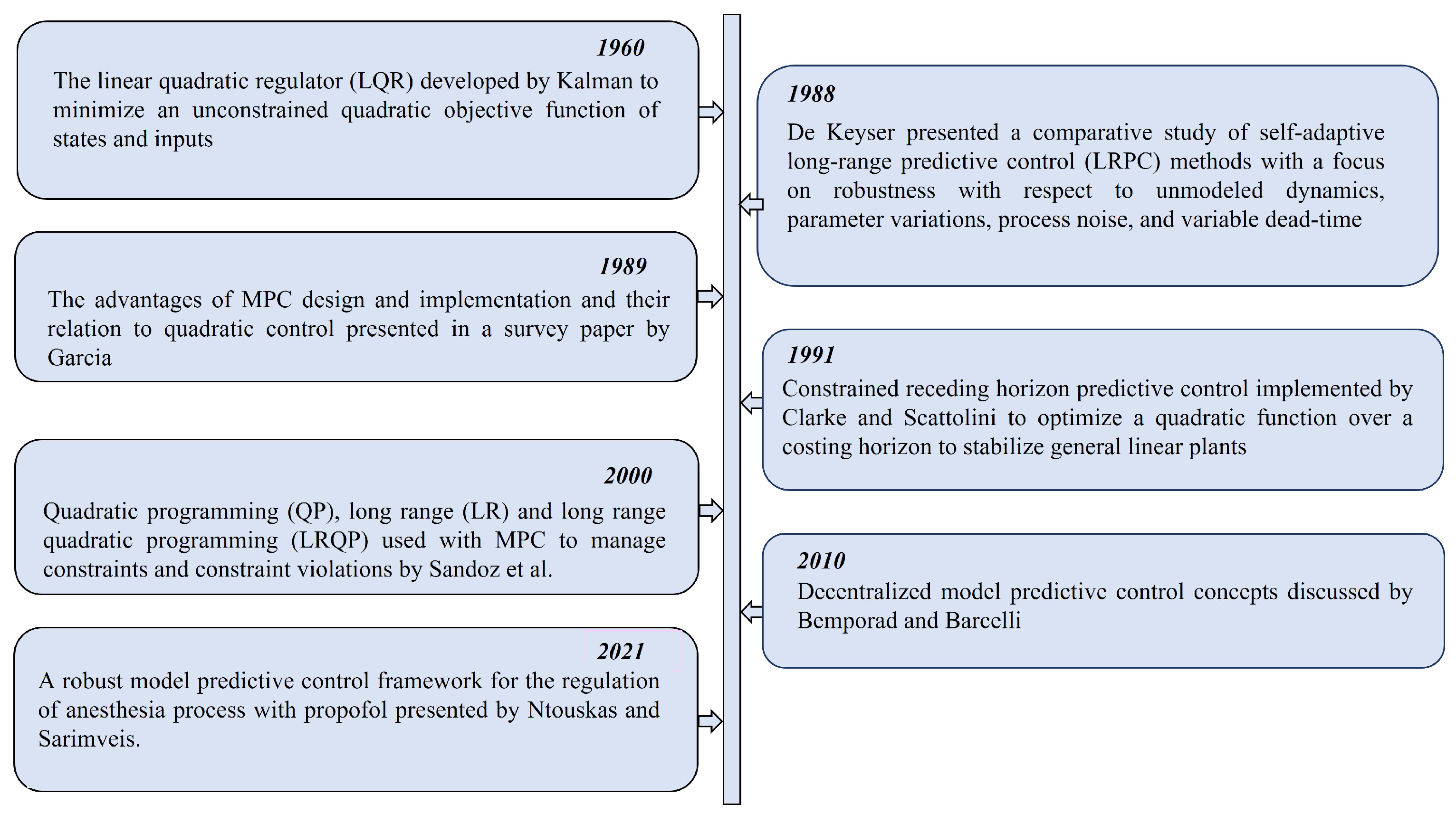
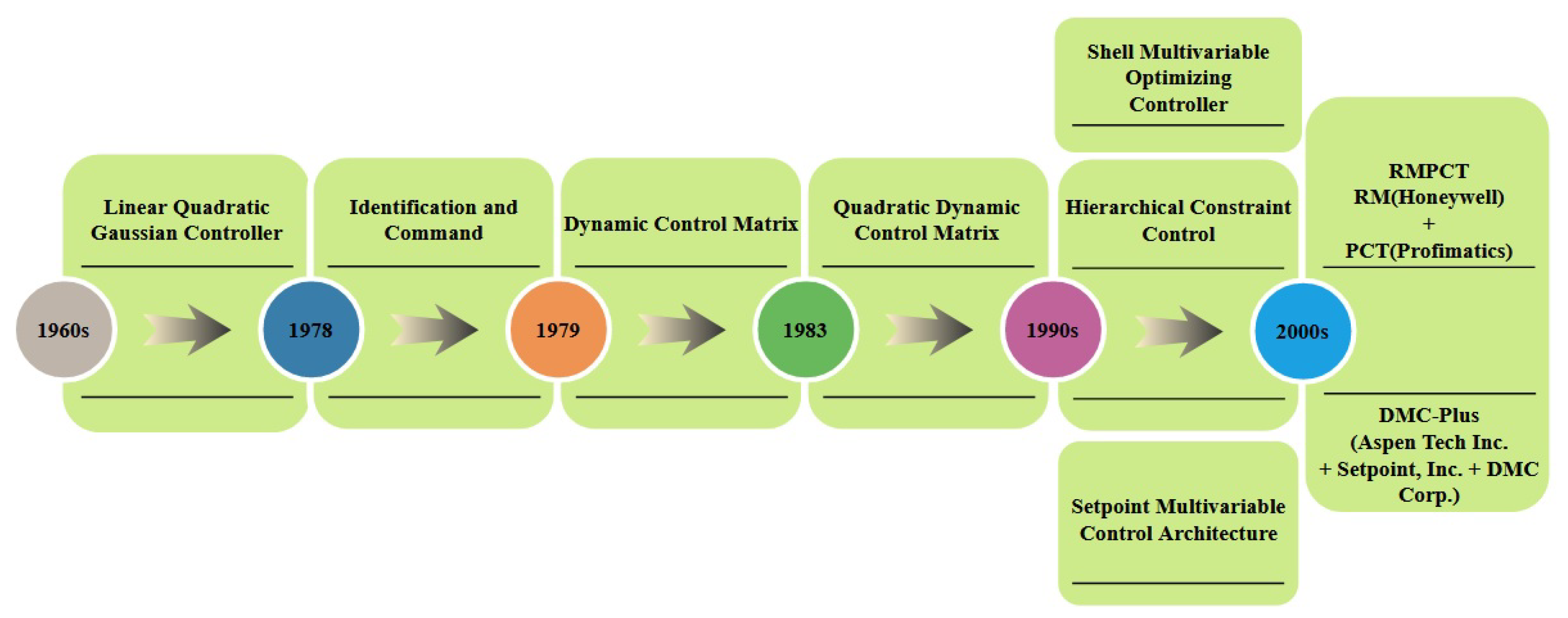
1.2. Evolution of MPC Algorithms
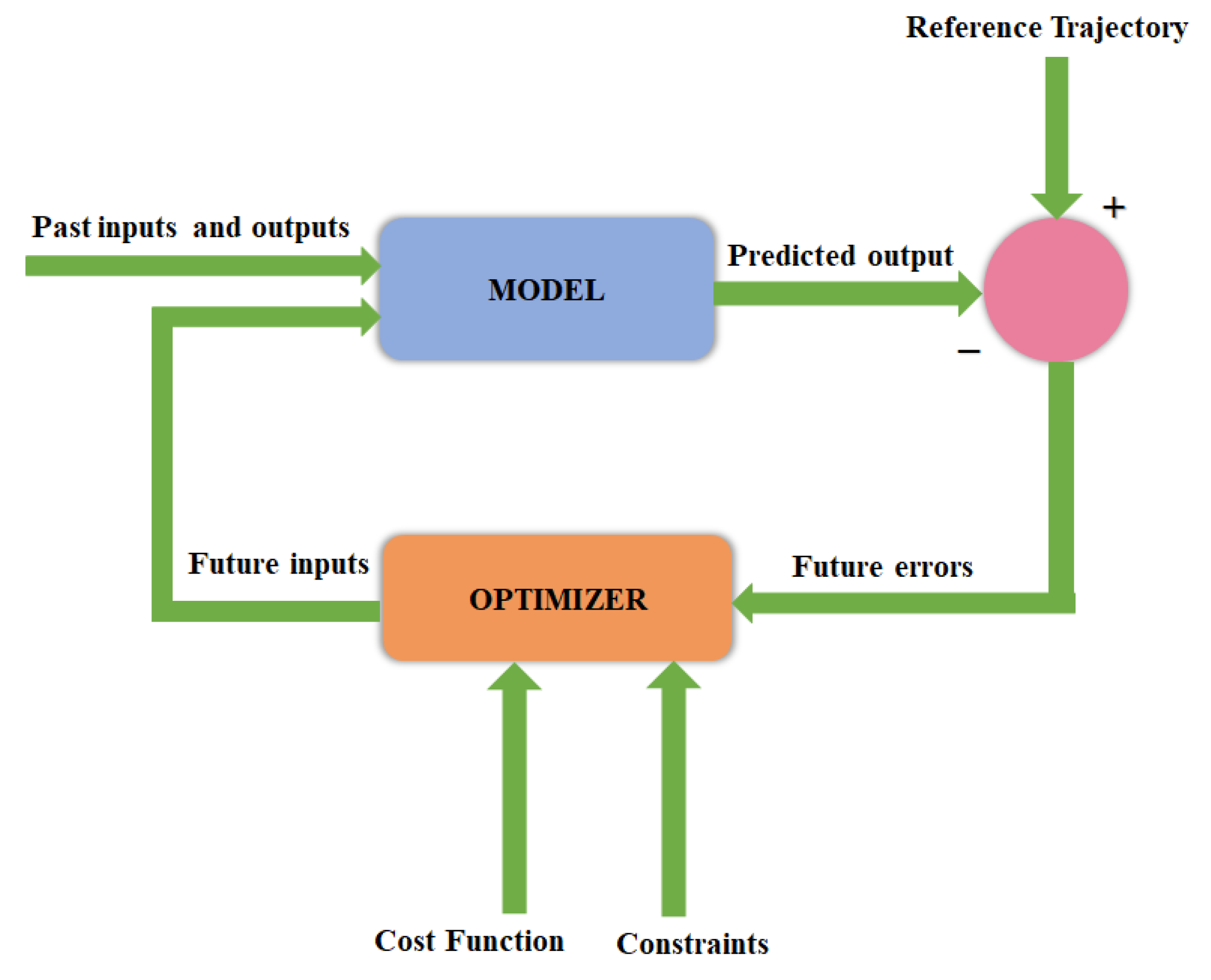
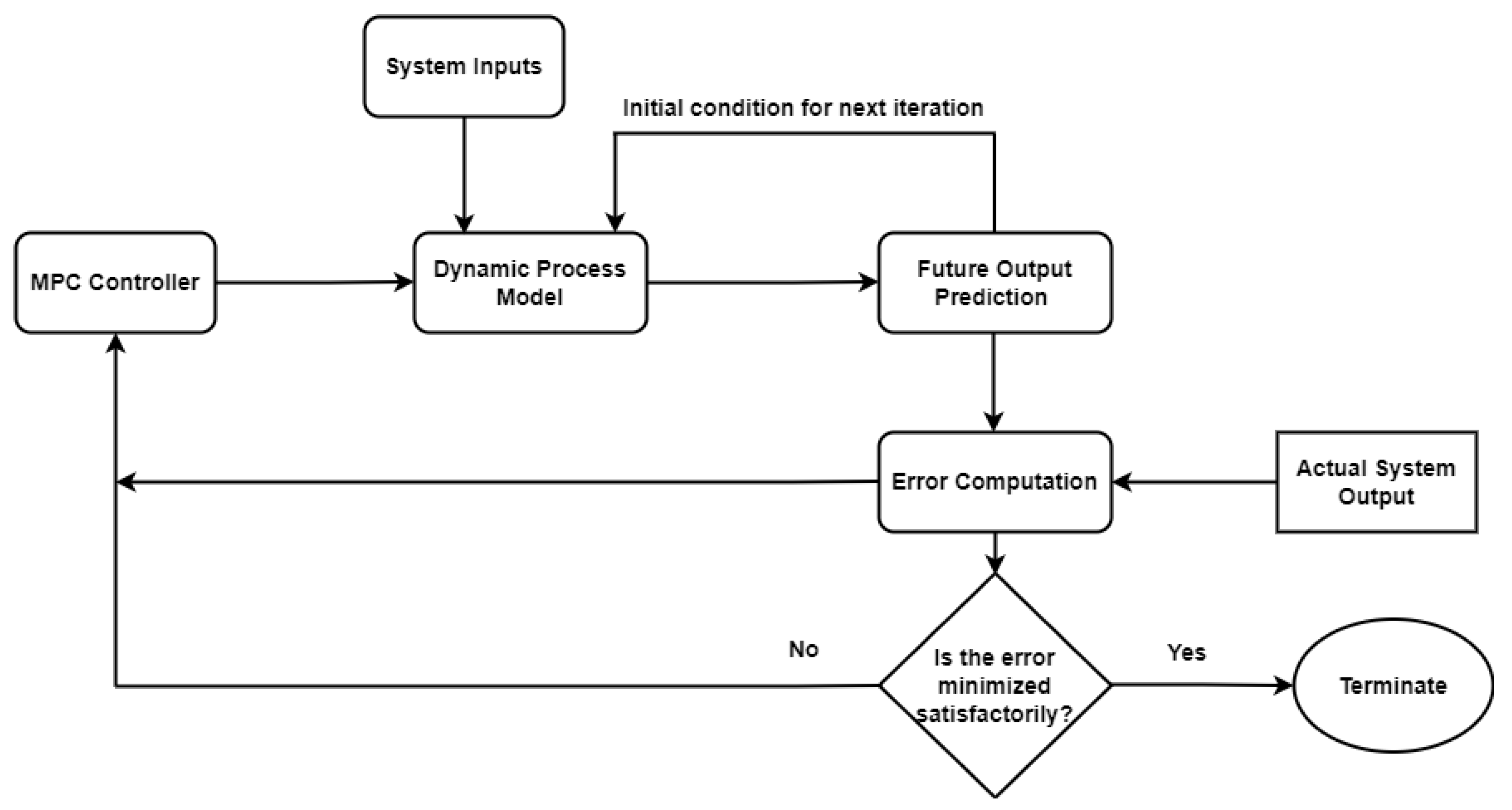
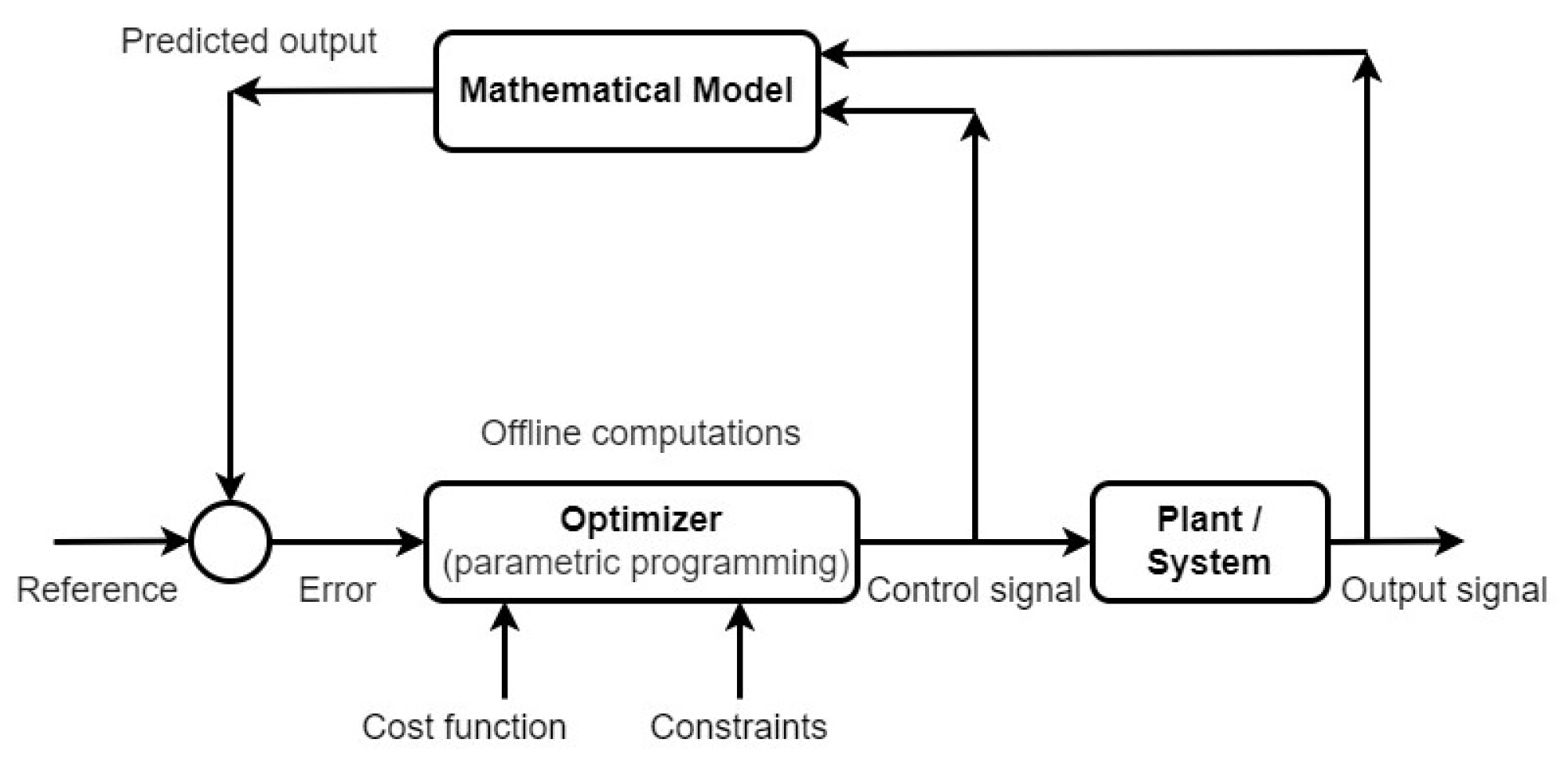
1.3. MPC Methodology
- Anticipate the outcome of a process over a future time horizon via the explicit application of a system model;
- Calculate and optimizate the control sequence;
- Implement a receding horizon strategy in which the horizon is moved towards the future at each step while applying the control sequence for that step.
1.4. Advantages and Limitations of MPC
- Multi-variable control problems can be naturally handled by MPCs;
- Actuator limitations can be taken into account by MPCs;
- MPCs permit operations nearer to constraints, resulting in higher performance;
- Structural changes can be handled by MPCs;
- MPCs have sufficient capability for online calculations;
- Unstable processes and non-minimal phases can be handled by MPCs;
- MPCs can be easily tuned.
2. MPC Implementation
2.1. Linear MPC
2.2. Nonlinear MPC
2.3. Explicit MPC
2.4. Robust MPC
- Min-max: The min/max MPC approach essentially converts a “min” optimization problem into “min-max” optimization by decreasing the worst-case objective functions and maximising them across all feasible points in the uncertainty set [45]. In this formulation, optimization is performed with respect to all possible disturbance evolutions. The min-max MPC has been proven to be the most effective for solving linear robust control applications. However, it is also relatively computationally expensive.
- Constraint tightening: In this approach, the state constraints are widened by a certain amount to ensure that a trajectory is discovered regardless of the disturbance evolution [46].
- Tube: The tube method employs a separate nominal system model and a feedback controller for converging the active state to the nominal state as quickly as possible [47]. This MPC collects all possible state deviations due to disturbances in a robust positively invariant (RPI) set, which are then used to determine the degree of separation of the states from the set of constraints.
- Multi-stage: The multi-stage approach accommodates different control decisions at every stage. It is non-conservative in nature due to the availability of measurement information at each time step in the forecast as well as the fact that it can be used to mitigate the effects of uncertainties. The inherent disadvantage of this strategy is that the complexity of the control problem increases as the number of uncertainties and the time between predictions increases [48,49].
- Tube-enhanced multi-stage: This approach combines the advantages of tube-based and multi-stage MPC architectures to furnish more options for optimality versus simplicity trade-offs. This method has been found to be quite useful in system forecasting using various control and uncertainty principles [50,51].
2.5. Other MPCs
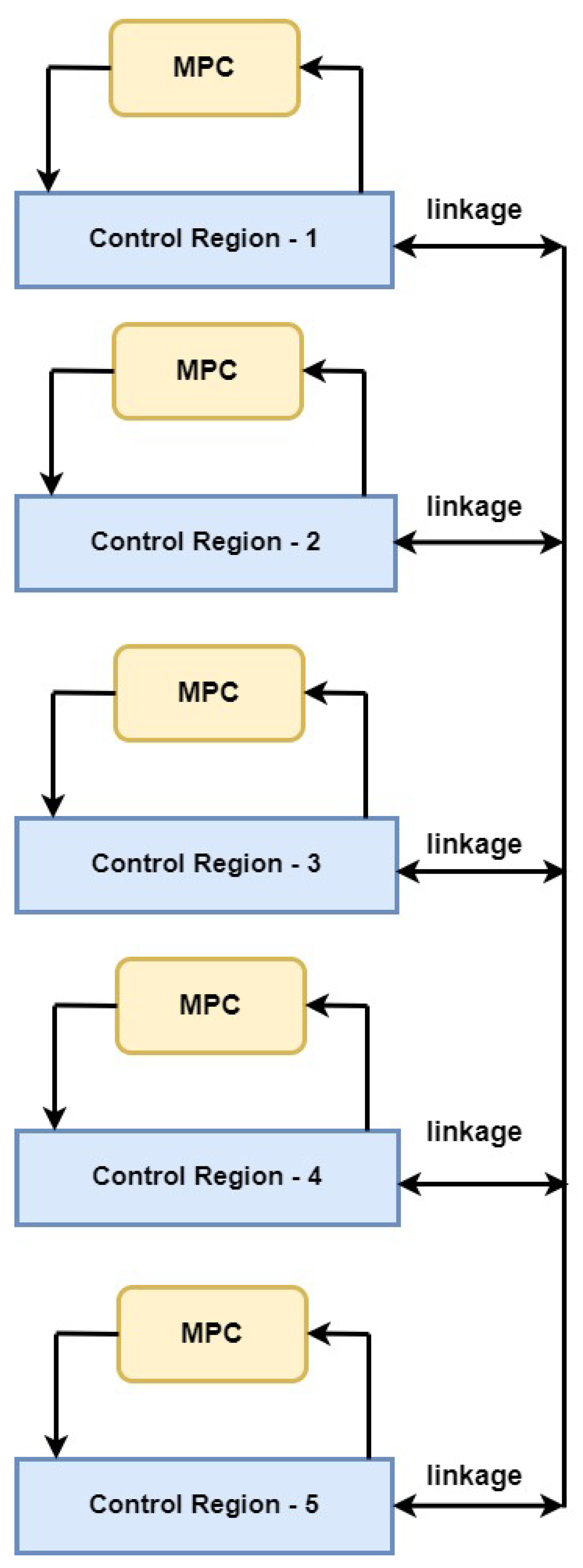
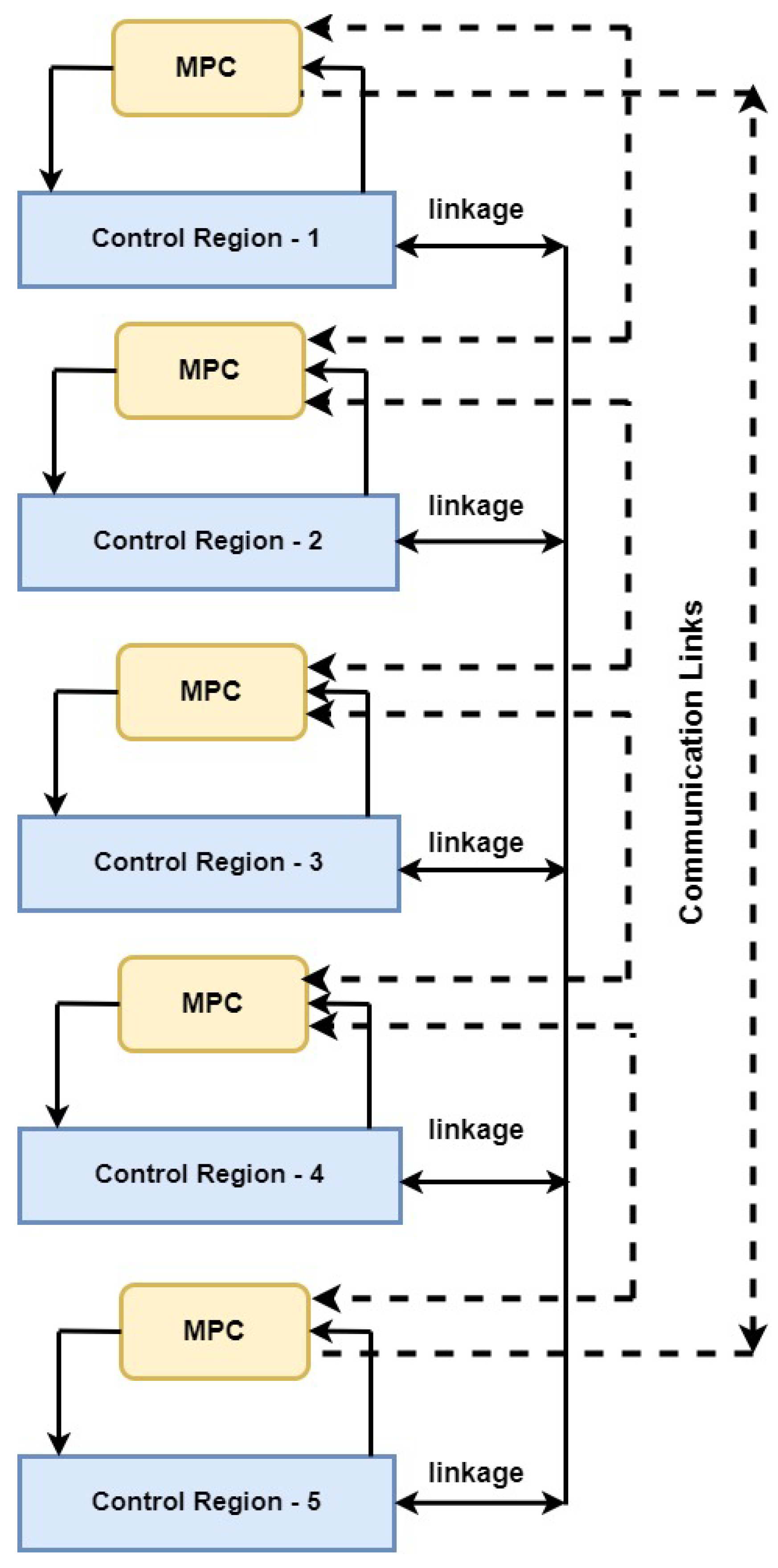
- Decentralized and distributed MPC: Each controller in a decentralised and/or distributed control system simply monitors and regulates local outputs and inputs. Decentralization has profound benefits for controller implementation and maintenance. During maintenance, some functional aspects of the overall process are interrupted, but the remainder of the components continue to function uninterrupted with local controllers in a closed-loop, as against total shutdown in the case of centralised control architectures. Similarly, redesigning a part of the process does not imply complete remodeling of the entire controller architecture, as would happen in the case of centralised control. Under decentralization, it is important to specify the applicable conditions for which the local closed-loop controller laws are capable of keeping the entire system stabilized. In the process industries, MPC techniques are generally utilised to solve large-scale multivariable control problems. An MPC formulates the control problem in the form of an optimization problem in which several (possibly competing) goals and constraints (state- and control-related) can be specified. Due to scalability and model maintenance issues, a centralised MPC is typically inadequate for large-scale networked systems. In light of the above, it makes sense to envisage decentralised model predictive control (DeMPC) and distributed model predictive control (DMPC) algorithms, which involve compartmentalizing a big optimization objective into multiple smaller units that iterate independently (DeMPC) or cooperatively (DMPC) to ultimately attain the overall system objective. The primary distinction between "decentralised" and "distributed" is the way information is shared among control regions. In DeMPC, local controllers make independent decisions. Prior control choices and measurements can only be provided before and after a decision is made. Communication considerations such as network delays and packet loss have no effect on the decision-making time for local control actions. Figure 6 depicts a DeMPC architecture wherein five distinct control regions are controlled individually by local MPC controllers. On the other hand, Figure 7 shows a corresponding DMPC layout wherein candidate control decisions may be exchanged and iterated during the decision-making process until local controllers agree on a stopping condition [52].
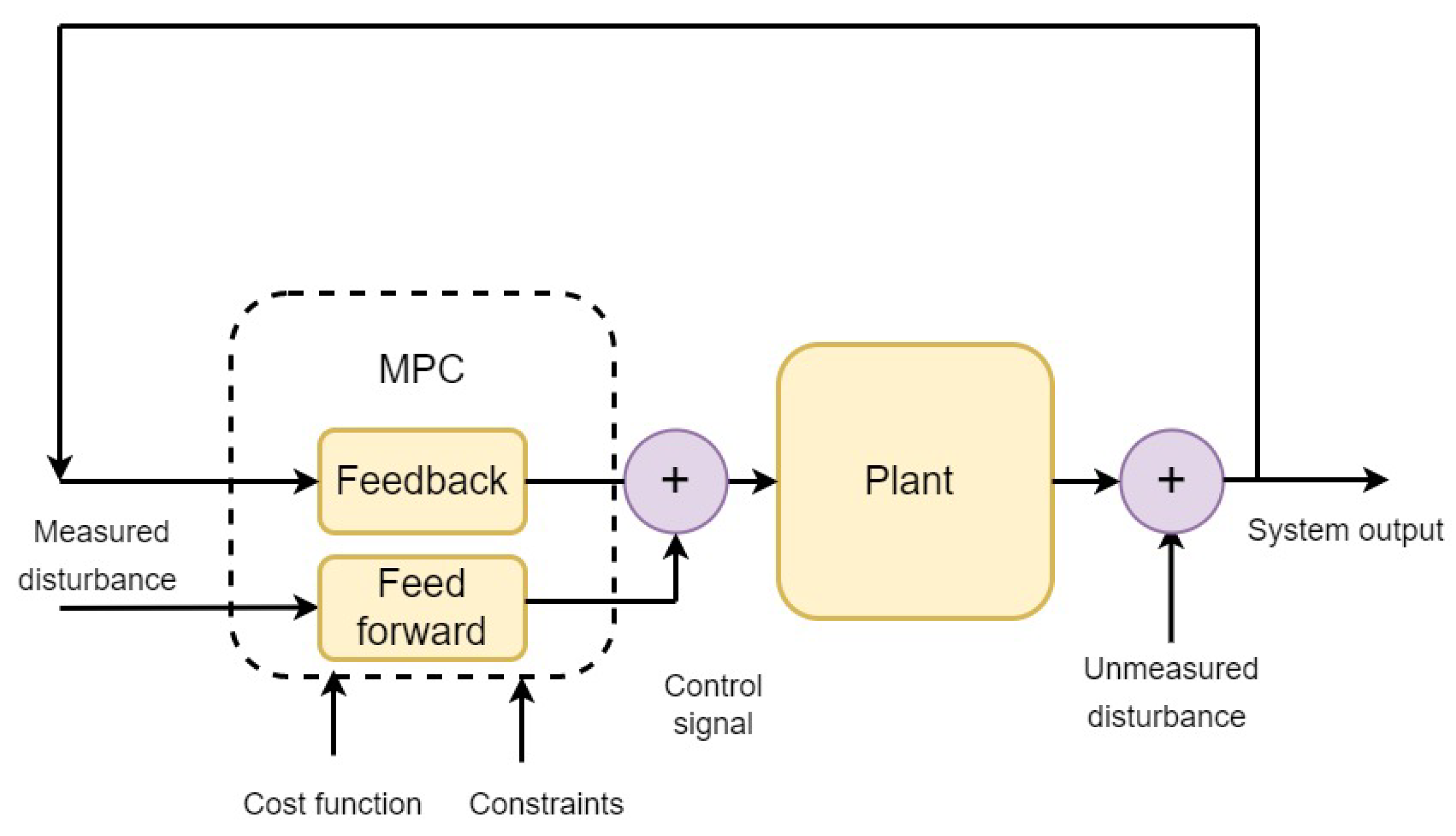
- Feedback and feedforward MPCs: Feedback correction is an inherent feature of MPCs, along with rolling optimization and predictive modeling characteristics [18]. The combination of MPC and feedback linearization (FL) has been popular among researchers for many years due to the ease of controllability of FL plants using linear MPCs [53]. For instance, Parekh et al. [54] applied a state feedback linearization (SFL)-enabled MPC to effectively control a pharmaceutical coolant temperature application. However, some researchers [55] have supported MPC architectures inclusive of feedback as well as feedforward control signals. This architecture overcomes the inherent drawback of purely feedback control loops with regards to the detection of system deviations after they have occurred. The feedforward and feedback loops act together to eliminate all measured and unmeasured system disturbances (Figure 8). Kayacan et al. [55] also proposed linear MPC architectures with feedback as well as feedforward loops for multi-input and multi-output mobile robot systems. Sbarciog et al. [56] designed cascaded linearized feedback controllers to control animal cell concentrations and nutrients in a cultivation plant. Wang et al. [57] incorporated a feedforward-feedback regulation regime to effectively control disturbances in a multiple-effect falling film evaporator system. Zhao et al. [18] applied active feedback correction in a trajectory-tracking controller for an unmanned vehicle to overcome system interference and uncertainties. Table 3 furnishes a featured summary of the above-discussed MPC variants.
2.6. MPC Softwares
- MATLAB: The model predictive control toolbox of Matlab includes application, function and Simulink blocks for designing and simulating linear and nonlinear model predictive control (MPC) controllers [58]. This toolbox allows users to specify plant model parameters, horizons, constraints and weights. Closed-loop simulations can be used to assess controller performance. Controller weights and constraints can be changed during runtime to update output behaviour. In addition to deployable solvers, control designers can employ a custom optimizer from the toolbox. Nonlinear, gain-scheduled and adaptive MPCs can be used to control nonlinear plants. For applications with high sample rates, this toolbox can generate explicit MPCs from regular controllers to approximate feasible solutions.
- Oravec’s MUP: This software uses the MATLAB/Simulink toolbox to implement a robust MPC in the LMI (linear matrix inequalities) framework online [59]. The MUP toolbox is a practical and user-friendly solution for MPC control engineering. It is also an excellent choice for educational purposes. The MUP package is provided "as is," with no warranties of any kind. YALMIP (yet another LMI parser and SeDuMi (self dual minimization)) are the required MUP dependencies, with Mosek as the recommended solver. These are not included in the MUP toolbox.
- do-MPC: do-MPC is an open-source toolbox used for moving horizon and parameter estimation to develop robust multi-stage MPC architectures. do-MPC includes specialized tools to deal with time discretization and system uncertainties. Its modular layout easily accommodates different combinations of control, estimation and simulation components in seamless integration for various applications. do-MPC is widely used for nonlinear system modeling, estimation and simulations. It supports differential algebraic equations as well [60].
3. MPC in Biomedical Applications
3.1. Type-1 Diabetes
Artificial Pancreas
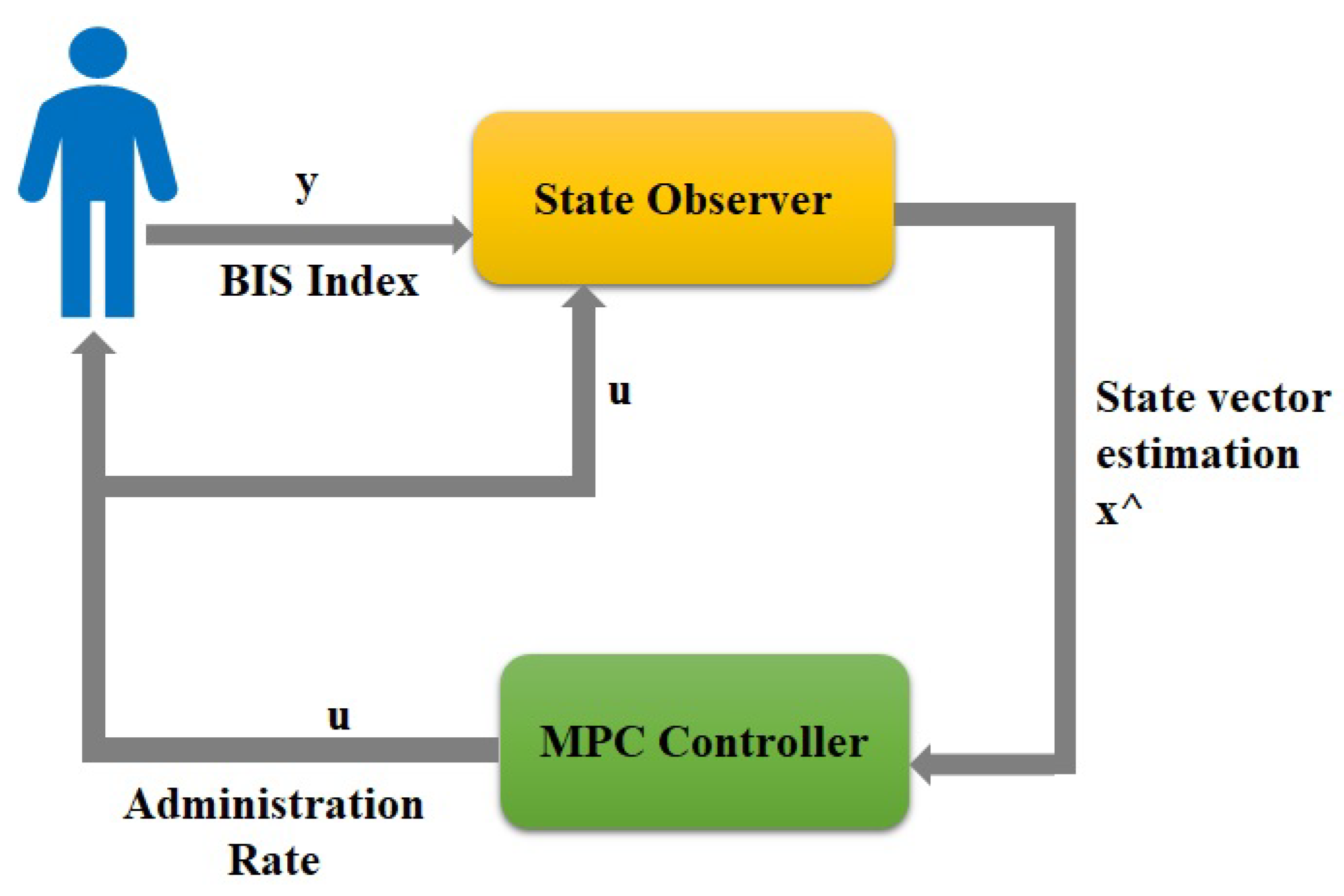
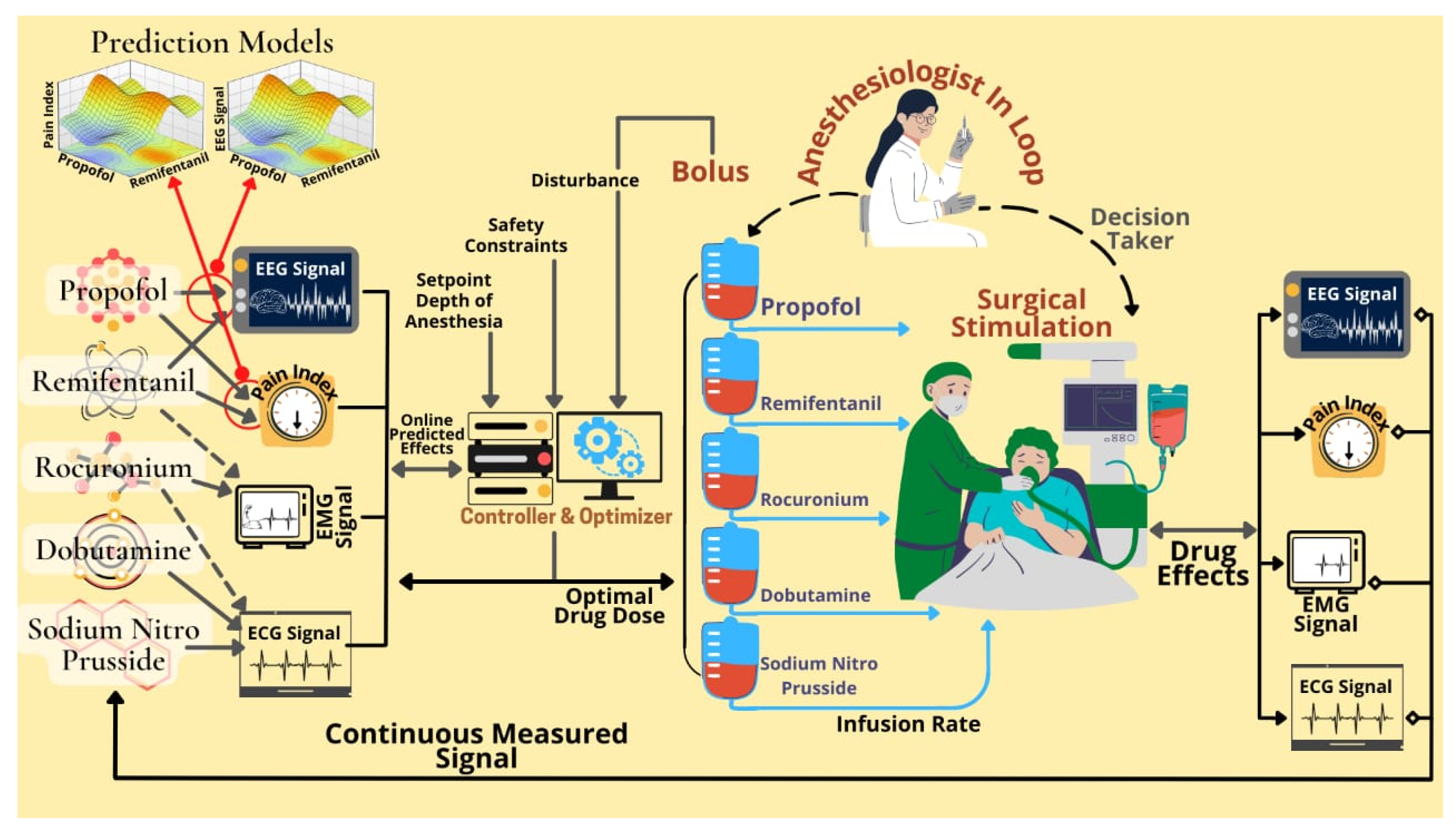
3.2. Anaesthesia
- Optimization of drug dose regimen;
- Better efficiency as compared to manual control;
- Chances of unintended under- or over-dosing are reduced;
- Clinicians can receive early alerts in case a crucial event occurs with the patient, allowing the clinician to intervene as soon as possible;
- Decision support is provided to the anaesthesiologist in the form of a recommended optimal drug infusion determined using context-aware methods;
- Reduction of the workload of clinicians while increasing the effectiveness and vigilance of anesthesiologists. This allows the physician to devote more attention to decisions that demand human expertise;
- Effectiveness in terms of cost, including the avoidance of repetitive treatment and saving costs by achieving accurately targeted drug delivery.
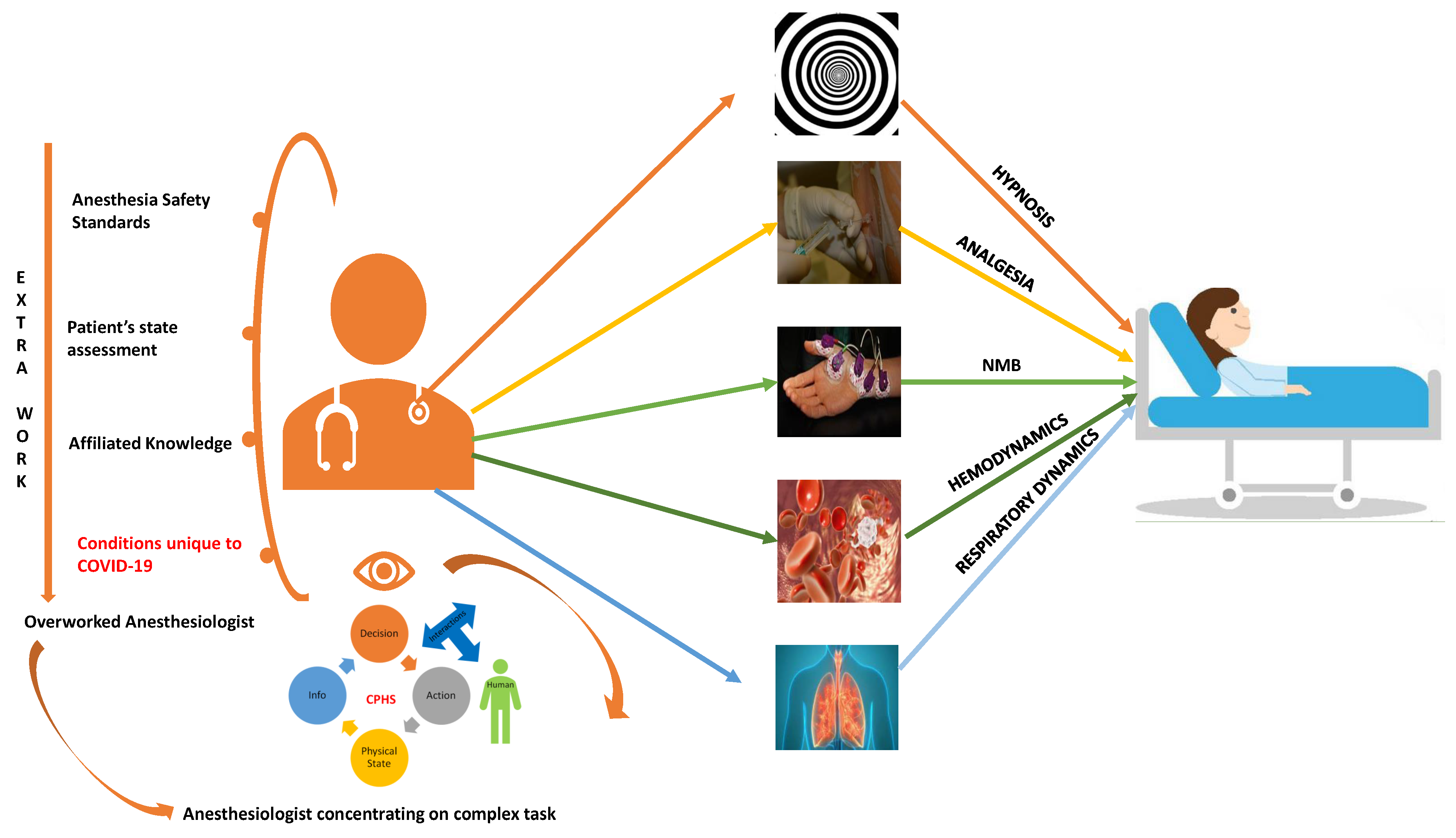
Cyber Physical Human Systems
3.3. Fibromyalgia
3.4. HIV
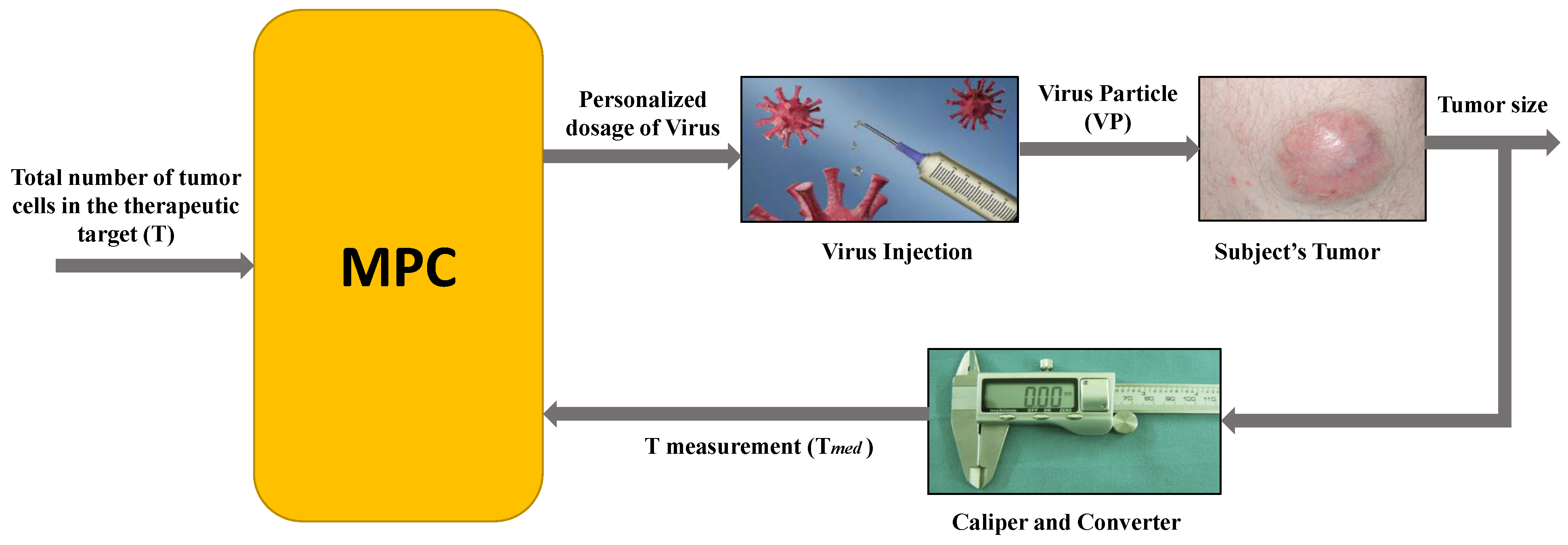
3.5. Cancer
3.5.1. Oncolytic Viral Therapy
3.5.2. Hyperthermia Therapy
4. Conclusions and Future Scope
- Better efficiency over manual monitoring and control;
- Automated and optimized drug delivery based on dynamic monitoring of therapeutic and patients’ bio-parameters;
- Minimization of unintended under- or over-dosing;
- Real-time data-based decision support to medical personnel;
- Routine workload reduction of medical personnel;
- Cost effectiveness by minimizing repetitive treatments.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Pannocchia, G.; Laurino, M.; Landi, A. A model predictive control strategy toward optimal structured treatment interruptions in anti-HIV therapy. IEEE Trans. Biomed. Eng. 2010, 57, 1040–1050. [Google Scholar] [CrossRef]
- Sekhar, R.; Singh, T.; Shah, P. Machine learning based predictive modeling and control of surface roughness generation while machining micro boron carbide and carbon nanotube particle reinforced Al-Mg matrix composites. Part. Sci. Technol. 2022, 40, 355–372. [Google Scholar] [CrossRef]
- Garcia, C.E.; Prett, D.M.; Morari, M. Model predictive control: Theory and practice—A survey. Automatica 1989, 25, 335–348. [Google Scholar] [CrossRef]
- De Keyser, R.M.; Van de Velde, P.G.; Dumortier, F. A comparative study of self-adaptive long-range predictive control methods. Automatica 1988, 24, 149–163. [Google Scholar] [CrossRef]
- Scattolini, R.; Bittanti, S. On the choice of the horizon in long-range predictive control—Some simple criteria. Automatica 1990, 26, 915–917. [Google Scholar] [CrossRef]
- Clarke, D.; Scattolini, R. Constrained receding-horizon predictive control. In Proceedings of the IEE Proceedings D (Control Theory and Applications); IET: London, UK, 1991; Volume 138, pp. 347–354. [Google Scholar] [CrossRef]
- Qin, S.J.; Badgwell, T.A. A survey of industrial model predictive control technology. Control Eng. Pract. 2003, 11, 733–764. [Google Scholar] [CrossRef]
- Jalali, A.A.; Nadimi, V. A survey on robust model predictive control from 1999–2006. In Proceedings of the 2006 International Conference on Computational Inteligence for Modelling Control and Automation and International Conference on Intelligent Agents Web Technologies and International Commerce (CIMCA’06), Sydney, NSW, Australia, 28 November–1 December 2006; IEEE: New York, NY, USA, 2006; p. 207. [Google Scholar] [CrossRef]
- Sandoz, D.J.; Desforges, M.J.; Lennox, B.; Goulding, P.R. Algorithms for industrial MPC. Comput. Control Eng. J. 2000, 11, 125–134. [Google Scholar] [CrossRef]
- Grimm, G.; Messina, M.J.; Tuna, S.E.; Teel, A. Examples of zero robustness in constrained model predictive control. In Proceedings of the 42nd IEEE International Conference on Decision and Control (IEEE Cat. No. 03CH37475), Maui, HI, USA, 9–12 December 2003; IEEE: New York, NY, USA, 2003; Volume 4, pp. 3724–3729. [Google Scholar] [CrossRef]
- Warren, A.L.; Marlin, T.E. Constrained MPC under closed-loop uncertainty. In Proceedings of the 2004 American Control Conference, Boston, MA, USA, 30 June–2 July 2004; IEEE: New York, NY, USA, 2004; Volume 5, pp. 4607–4612. [Google Scholar] [CrossRef]
- Li, G.; Lennox, B.; Ding, Z. Infinite horizon model predictive control for tracking problems. In Proceedings of the 2005 International Conference on Control and Automation, Budapest, Hungary, 26–29 June 2005; IEEE: New York, NY, USA, 2005; Volume 1, pp. 516–521. [Google Scholar] [CrossRef]
- Abu-Ayyad, M.; Dubay, R. Real-time comparison of a number of predictive controllers. ISA Trans. 2007, 46, 411–418. [Google Scholar] [CrossRef]
- Kalman, R.E. Contributions to the theory of optimal control. Bol. Soc. Mat. Mex. 1960, 5, 102–119. [Google Scholar] [CrossRef]
- Richalet, J.; Rault, A.; Testud, J.; Papon, J. Model algorithmic control of industrial processes. IFAC Proc. Vol. 1977, 10, 103–120. [Google Scholar] [CrossRef]
- Cutler, C.R.; Ramaker, B.L. Dynamic matrix control? A computer control algorithm. In Proceedings of the Joint Automatic Control Conference, San Francisco, CA, USA, 13–15 August 1980; Number 17. p. 72. [Google Scholar] [CrossRef]
- Krieger, A.; Pistikopoulos, E.N. Model predictive control of anesthesia under uncertainty. Comput. Chem. Eng. 2014, 71, 699–707. [Google Scholar] [CrossRef]
- Zhao, K.; Wang, C.; Xiao, G.; Li, H.; Ye, J.; Liu, Y. Research for Nonlinear Model Predictive Controls to Laterally Control Unmanned Vehicle Trajectory Tracking. Appl. Sci. 2020, 10, 6034. [Google Scholar] [CrossRef]
- Kalman, R.E. A New Approach to Linear Filtering and Prediction Problems; Wiley-IEEE Press: New York, NY, USA, 1960; pp. 167–179. [Google Scholar] [CrossRef] [Green Version]
- Richalet, J.; Rault, A.; Testud, J.; Papon, J. Model predictive heuristic control: Applications to industrial processes. Automatica 1978, 14, 413–428. [Google Scholar] [CrossRef]
- Cutler, C.; Ramaker, B. Dynamic matrix control A computer control algorithm, AICHE. In Proceedings of the 86th National Meeting, Houston, TX, USA, 1–5 April 1979. [Google Scholar]
- Cutler, C.; Morshedi, A.; Haydel, J. An industrial perspective on advanced control. In Proceedings of the AICHE Annual Meeting, Palm Beach, FL, USA, 9–11 June 1983. [Google Scholar]
- Garcia, C.E.; Morshedi, A. Quadratic programming solution of dynamic matrix control (QDMC). Chem. Eng. Commun. 1986, 46, 73–87. [Google Scholar] [CrossRef]
- Grosdidier, P.; Froisy, B.; Hammann, M. The Idocom–M controller. IFAC Proc. Vol. 1988, 21, 31–36. [Google Scholar] [CrossRef]
- Marquis, P.; Broustail, J. SMOC, a bridge between state space and model predictive controllers: Application to the automation of a hydrotreating unit. IFAC Proc. Vol. 1988, 21, 37–45. [Google Scholar] [CrossRef]
- Yousfi, C.; Tournier, R. Steady state optimization inside model predictive control. In Proceedings of the 1991 American Control Conference, Boston, MA, USA, 26–28 June 1991; IEEE: New York, NY, USA, 1991; pp. 1866–1870. [Google Scholar] [CrossRef]
- Camacho, E.F.; Alba, C.B. Model Predictive Control; Springer Science & Business Media: New York, NY, USA, 2013. [Google Scholar]
- Mesbah, A. Stochastic model predictive control: An overview and perspectives for future research. IEEE Control Syst. Mag. 2016, 36, 30–44. [Google Scholar] [CrossRef] [Green Version]
- Orukpe, P. Model predictive control fundamentals. Niger. J. Technol. 2012, 31, 139–148. [Google Scholar] [CrossRef]
- Al-Gherwi, W.; Budman, H.; Elkamel, A. A robust distributed model predictive control based on a dual-mode approach. Comput. Chem. Eng. 2013, 50, 130–138. [Google Scholar] [CrossRef]
- Goodarzi, N.; Dehghani, M.; Khayatian, A. Constrained RMPC algorithms for time delay systems with parametric uncertainties: Application to the cancer combined therapy. In Proceedings of the 2016 24th Iranian Conference on Electrical Engineering (ICEE), Shiraz, Iran, 10–12 May 2016; IEEE: New York, NY, USA, 2016; pp. 451–456. [Google Scholar] [CrossRef]
- Allgöwer, F.; Zheng, A. Nonlinear Model Predictive Control; Birkhäuser: Basel, Switzerland, 2012; Volume 26. [Google Scholar] [CrossRef]
- Findeisen, R.; Allgöwer, F.; Biegler, L.T. Assessment and Future Directions of Nonlinear Model Predictive Control; Springer: New York, NY, USA, 2007; Volume 358. [Google Scholar] [CrossRef]
- Ohtsuka, T. A continuation/GMRES method for fast computation of nonlinear receding horizon control. Automatica 2004, 40, 563–574. [Google Scholar] [CrossRef]
- Knyazev, A.; Malyshev, A. Sparse preconditioning for model predictive control. In Proceedings of the 2016 American Control Conference (ACC), Boston, MA, USA, 6–8 July 2016; IEEE: New York, NY, USA, 2016; pp. 4494–4499. [Google Scholar] [CrossRef] [Green Version]
- García, M.R.; Vilas, C.; Santos, L.O.; Alonso, A.A. A robust multi-model predictive controller for distributed parameter systems. J. Process Control 2012, 22, 60–71. [Google Scholar] [CrossRef] [Green Version]
- Merchant, R.; Mehendale, S. A new model for predicting flow boiling heat transfer coefficients in horizontal microfin tubes. In Proceedings of the ASME International Mechanical Engineering Congress and Exposition, Phoenix, AZ, USA, 11–17 November 2016; American Society of Mechanical Engineers: New York, NY, USA, 2016; Volume 50626, p. V008T10A014. [Google Scholar] [CrossRef]
- Bemporad, A.; Morari, M.; Dua, V.; Pistikopoulos, E.N. The explicit linear quadratic regulator for constrained systems. Automatica 2002, 38, 3–20. [Google Scholar] [CrossRef]
- Susuki, Y.; Mezić, I. A prony approximation of Koopman mode decomposition. In Proceedings of the 2015 54th IEEE Conference on Decision and Control (CDC), Osaka, Japan, 15–18 December 2015; IEEE: New York, NY, USA, 2015; pp. 7022–7027. [Google Scholar] [CrossRef]
- Klaučo, M.; Kaluz, M.; Kvasnica, M. Real-time implementation of an explicit MPC-based reference governor for control of a magnetic levitation system. Control Eng. Pract. 2017, 60, 99–105. [Google Scholar] [CrossRef]
- Bacic, M.; Cannon, M.; Lee, Y.; Kouvaritakis, B. General interpolation in MPC and its advantages. IEEE Trans. Autom. Control 2003, 48, 1092–1096. [Google Scholar] [CrossRef]
- Schwenzer, M.; Ay, M.; Bergs, T.; Abel, D. Review on model predictive control: An engineering perspective. Int. J. Adv. Manuf. Technol. 2021, 117, 1327–1349. [Google Scholar] [CrossRef]
- Mendes, P. Predictive Control for Energy Management of Renewable Energy Based Microgrids. Ph.D. Thesis, Universidade Federal de Santa Catarina, Florianopolis, Brazil, 2016. [Google Scholar]
- Piazzi, A.; Visioli, A. Robust multivariable set-point regulation via stable dynamic inversion. IFAC Proc. Vol. 2002, 35, 1–6. [Google Scholar] [CrossRef]
- Nevistić, V.; Morari, M. Robustness of mpc-based schemes for constrained control of nonlinear systems. IFAC Proc. Vol. 1996, 29, 5823–5828. [Google Scholar] [CrossRef]
- Richards, A.; How, J. Robust stable model predictive control with constraint tightening. In Proceedings of the 2006 American Control Conference, Minneapolis, MN, USA, 14–16 June 2006; IEEE: New York, NY, USA, 2006; pp. 1557–1562. [Google Scholar] [CrossRef]
- Langson, W.; Chryssochoos, I.; Raković, S.; Mayne, D.Q. Robust model predictive control using tubes. Automatica 2004, 40, 125–133. [Google Scholar] [CrossRef]
- Lucia, S.; Finkler, T.; Engell, S. Multi-stage nonlinear model predictive control applied to a semi-batch polymerization reactor under uncertainty. J. Process Control 2013, 23, 1306–1319. [Google Scholar] [CrossRef]
- Lucia, S.; Subramanian, S.; Limon, D.; Engell, S. Stability properties of multi-stage nonlinear model predictive control. Syst. Control Lett. 2020, 143, 104743. [Google Scholar] [CrossRef]
- Subramanian, S.; Lucia, S.; Paulen, R.; Engell, S. Tube-enhanced multi-stage model predictive control for flexible robust control of constrained linear systems with additive and parametric uncertainties. Int. J. Robust Nonlinear Control 2021, 31, 4458–4487. [Google Scholar] [CrossRef]
- Subramanian, S.; Abdelsalam, Y.; Lucia, S.; Engell, S. Robust Tube-enhanced Multi-stage NMPC with Stability Guarantees. IEEE Control Syst. Lett. 2021, 6, 1112–1117. [Google Scholar] [CrossRef]
- Bemporad, A.; Barcelli, D. Decentralized model predictive control. In Networked Control Systems; Springer: New York, NY, USA, 2010; pp. 149–178. [Google Scholar] [CrossRef]
- Deng, J.; Becerra, V.M.; Stobart, R.K. Input Constraints Handling in an MPC/Feedback Linearization Scheme. Int. J. Appl. Math. Comput. Sci. 2009, 19, 219–232. [Google Scholar] [CrossRef] [Green Version]
- Parekh, R.; Benyahia, B.; Rielly, C.D. A Global State Feedback Linearization and Decoupling MPC of a MIMO Continuous MSMPR Cooling Crystallization Process. In Proceedings of the 28th European Symposium on Computer Aided Process Engineering, Graz, Austria, 10–13 June 2018; Computer Aided Chemical Engineering Series. Friedl, A., Klemeš, J.J., Radl, S., Varbanov, P.S., Wallek, T., Eds.; Elsevier: Amsterdam, The Netherlands, 2018; Volume 43, pp. 1607–1612. [Google Scholar] [CrossRef]
- Morattab, A.; Shafiee, Q.; Bevrani, H. Decentralized Model Predictive load-frequency control for deregulated power systems in a tough situation. In Proceedings of the 2011 IEEE Trondheim PowerTech, Trondheim, Norway, 19–23 June 2011; pp. 1–5. [Google Scholar] [CrossRef]
- Sbarciog, M.; Coutinho, D.F.; Wouwer, A.V. A Cascade MPC-Feedback Linearizing Strategy for the Multivariable Control of Animal Cell Cultures. IFAC Proc. Vol. 2013, 46, 247–252. [Google Scholar] [CrossRef] [Green Version]
- Wang, X.; Li, C.; Chen, X. Disturbance rejection control for multiple-effect falling-film evaporator based on disturbance observer. Trans. Inst. Meas. Control 2016, 38, 773–783. [Google Scholar] [CrossRef]
- Model Predictive Control Toolbox. Available online: https://www.mathworks.com/products/model-predictive-control.html (accessed on 10 May 2022).
- Bakošov’a, M.; Oravec, J. Robust Model Predictive Control of Uncertain Linear Systems with Persistent Disturbances and Input Constraints. In Proceedings of the American Control Conference, Zurich, Switzerland, 17–19 July 2013; pp. 5242–5247. [Google Scholar]
- Lucia, S.; Tătulea-Codrean, A.; Schoppmeyer, C.; Engell, S. Rapid development of modular and sustainable nonlinear model predictive control solutions. Control Eng. Pract. 2017, 60, 51–62. [Google Scholar] [CrossRef]
- Azar, A.T. Control Applications for Biomedical Engineering Systems; Academic Press: New York, NY, USA, 2020. [Google Scholar] [CrossRef]
- Pannocchia, G.; Rawlings, J.B. Disturbance models for offset-free model-predictive control. AIChE J. 2003, 49, 426–437. [Google Scholar] [CrossRef]
- Mirzaee, A.; Dehghani, M.; Mohammadi, M. A Nonlinear MPC Approach for Blood Glucose Regulation in Diabetic Patients. In Proceedings of the 2021 7th International Conference on Control, Instrumentation and Automation (ICCIA), Tabriz, Iran, 23–24 February 2021; IEEE: New York, NY, USA, 2021; pp. 1–5. [Google Scholar] [CrossRef]
- Cryer, P. Preventing hypoglycaemia: What is the appropriate glucose alert value? Diabetologia 2009, 52, 35–37. [Google Scholar] [CrossRef] [Green Version]
- Mirzaee, A.; Dehghani, M.; Mohammadi, M. Robust LPV control design for blood glucose regulation considering daily life factors. Biomed. Signal Process. Control 2020, 57, 101830. [Google Scholar] [CrossRef]
- Nath, A.; Biradar, S.; Balan, A.; Dey, R.; Padhi, R. Physiological models and control for type 1 diabetes mellitus: A brief review. IFAC-PapersOnLine 2018, 51, 289–294. [Google Scholar] [CrossRef]
- Batmani, Y. Blood glucose concentration control for type 1 diabetic patients: A non-linear suboptimal approach. IET Syst. Biol. 2017, 11, 119–125. [Google Scholar] [CrossRef]
- Khodakaramzadeh, S.; Batmani, Y.; Meskin, N. Automatic blood glucose control for type 1 diabetes: A trade-off between postprandial hyperglycemia and hypoglycemia. Biomed. Signal Process. Control 2019, 54, 101603. [Google Scholar] [CrossRef]
- Rashid, T.A.; Hassan, M.K.; Mohammadi, M.; Fraser, K. Improvement of variant adaptable LSTM trained with metaheuristic algorithms for healthcare analysis. In Advanced Classification Techniques for Healthcare Analysis; IGI Global: Hershey, PA, USA, 2019; pp. 111–131. [Google Scholar] [CrossRef] [Green Version]
- Kovács, L. Linear parameter varying (LPV) based robust control of type-I diabetes driven for real patient data. Knowl.-Based Syst. 2017, 122, 199–213. [Google Scholar] [CrossRef] [Green Version]
- Hernández-Medina, A.; Flores-Gutiérrez, C.; Femat, R. Robustness properties preservation in suboptimal T1DM H∞ control: ω-SPR substitutions. Optim. Control Appl. Methods 2018, 39, 220–229. [Google Scholar] [CrossRef]
- Rahmanian, F.; Dehghani, M.; Karimaghaee, P.; Mohammadi, M. Glucose control in diabetic patients considering daily real life factors. In Proceedings of the 2019 6th International Conference on Control, Instrumentation and Automation (ICCIA), Sanandaj, Iran, 30–31 October 2019; IEEE: New York, NY, USA, 2019; pp. 1–5. [Google Scholar] [CrossRef]
- Rahmanian, F.; Dehghani, M.; Karimaghaee, P.; Mohammadi, M. Blood Glucose Control In Type 1 Diabetic Rat, Considering Food Intake Effects. In Proceedings of the 2020 28th Iranian Conference on Electrical Engineering (ICEE), Tabriz, Iran, 4–6 August 2020; IEEE: New York, NY, USA, 2020; pp. 1–5. [Google Scholar] [CrossRef]
- Javanmardi, H.R.; Dehghani, M.; Safavi, A.A.; Abolpour, R. Model predictive control of a class of uncertain nonlinear discrete time systems: The LMI approach. In Proceedings of the 2016 24th Iranian Conference on Electrical Engineering (ICEE), Shiraz, Iran; IEEE: New York, NY, USA, 2016; pp. 323–328. [Google Scholar] [CrossRef]
- Dua, P.; Doyle, F.J.; Pistikopoulos, E.N. Model-based blood glucose control for type 1 diabetes via parametric programming. IEEE Trans. Biomed. Eng. 2006, 53, 1478–1491. [Google Scholar] [CrossRef]
- Magni, L.; Raimondo, D.M.; Dalla Man, C.; De Nicolao, G.; Kovatchev, B.; Cobelli, C. Model predictive control of glucose concentration in type I diabetic patients: An in silico trial. Biomed. Signal Process. Control 2009, 4, 338–346. [Google Scholar] [CrossRef]
- Embaby, A.A.; Nossair, Z.; Badr, H. Adaptive Nonlinear Model Predictive Control algorithm for blood glucose regulation in type 1 diabetic patients. In Proceedings of the 2020 2nd Novel Intelligent and Leading Emerging Sciences Conference (NILES), Giza, Egypt, 24–26 October 2020; IEEE: New York, NY, USA, 2020; pp. 109–115. [Google Scholar] [CrossRef]
- Grancharova, A.; Valkova, I. Contractive Model Predictive Control for Insulin Delivery for Type 1 Diabetics. In Proceedings of the 2019 IEEE International Symposium on INnovations in Intelligent SysTems and Applications (INISTA), Sofia, Bulgaria, 3–5 July 2019; IEEE: New York, NY, USA, 2019; pp. 1–6. [Google Scholar] [CrossRef]
- Hajizadeh, I.; Rashid, M.; Sevil, M.; Brandt, R.; Samadi, S.; Hobbs, N.; Cinar, A. Adaptive model predictive control for nonlinearity in biomedical applications. IFAC-PapersOnLine 2018, 51, 368–373. [Google Scholar] [CrossRef]
- Ammirati, E.; Wang, D.W. SARS-CoV-2 inflames the heart. The importance of awareness of myocardial injury in COVID-19 patients. Int. J. Cardiol. 2020, 311, 122. [Google Scholar] [CrossRef]
- Savoca, A.; Barazzetta, J.; Pesenti, G.; Manca, D. Model predictive control for automated anesthesia. In Computer Aided Chemical Engineering; Elsevier: Amsterdam, The Netherlands, 2018; Volume 43, pp. 1631–1636. [Google Scholar]
- Ingole, D.D.; Sonawane, D.N.; Naik, V.V.; Ginoya, D.L.; Patki, V.V. Linear model predictive controller for closed-loop control of intravenous anesthesia with time delay. Int. J. Control Syst. Instrum. 2013, 4, 8. [Google Scholar]
- Ntouskas, S.; Sarimveis, H. A robust model predictive control framework for the regulation of anesthesia process with Propofol. Optim. Control Appl. Methods 2021, 42, 965–986. [Google Scholar] [CrossRef]
- Patel, B.J.; Patel, H.G. A Model Predictive Control with Fault Tolerance Concept to Regulate Hypnosis during Anesthesia. In Proceedings of the 2019 Sixth Indian Control Conference (ICC), Hyderabad, India, 18–20 December 2019; IEEE: New York, NY, USA, 2019; pp. 182–187. [Google Scholar] [CrossRef]
- Sawaguchi, Y.; Furutani, E.; Shirakami, G.; Araki, M.; Fukuda, K. A model-predictive hypnosis control system under total intravenous anesthesia. IEEE Trans. Biomed. Eng. 2008, 55, 874–887. [Google Scholar] [CrossRef] [Green Version]
- Ghita, M.; Neckebroek, M.; Muresan, C.; Copot, D. Closed-loop control of anesthesia: Survey on actual trends, challenges and perspectives. IEEE Access 2020, 8, 206264–206279. [Google Scholar] [CrossRef]
- Kuck, K.H. Arrhythmias and sudden cardiac death in the COVID-19 pandemic. Herz 2020, 45, 325–326. [Google Scholar] [CrossRef] [PubMed]
- Casas-Arroyave, F.D.; Fernández, J.M.; Zuleta-Tobón, J.J. Evaluation of a closed-loop intravenous total anesthesia delivery system with BIS monitoring compared to an open-loop target-controlled infusion (TCI) system: Randomized controlled clinical trial. Colomb. J. Anestesiol. 2019, 47, 84–91. [Google Scholar] [CrossRef]
- Wolfe, F.; Smythe, H.A.; Yunus, M.B.; Bennett, R.M.; Bombardier, C.; Goldenberg, D.L.; Tugwell, P.; Campbell, S.M.; Abeles, M.; Clark, P.; et al. The American College of Rheumatology 1990 criteria for the classification of fibromyalgia. Arthritis Rheum. Off. J. Am. Coll. Rheumatol. 1990, 33, 160–172. [Google Scholar] [CrossRef] [PubMed]
- Wolfe, F.; Clauw, D.J.; Fitzcharles, M.A.; Goldenberg, D.L.; Katz, R.S.; Mease, P.; Russell, A.S.; Russell, I.J.; Winfield, J.B.; Yunus, M.B. The American College of Rheumatology preliminary diagnostic criteria for fibromyalgia and measurement of symptom severity. Arthritis Care Res. 2010, 62, 600–610. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mattioli, T.A.M.; Milne, B.; Cahill, C.M. Ultra-low dose naltrexone attenuates chronic morphine-induced gliosis in rats. Mol. Pain 2010, 6, 1744–8069. [Google Scholar] [CrossRef] [Green Version]
- Boissevain, M.D.; McCain, G.A. Toward an integrated understanding of fibromyalgia syndrome. II. Psychological and phenomenological aspects. Pain 1991, 45, 239–248. [Google Scholar] [CrossRef] [PubMed]
- Deshpande, S.; Nandola, N.N.; Rivera, D.E.; Younger, J. A control engineering approach for designing an optimized treatment plan for fibromyalgia. In Proceedings of the 2011 American Control Conference, Hilton San Francisco, CA, USA, 29 June–1 July 2011; IEEE: New York, NY, USA, 2011; pp. 4798–4803. [Google Scholar] [CrossRef] [Green Version]
- Younger, J.; Mackey, S. Fibromyalgia symptoms are reduced by low-dose naltrexone: A pilot study. Pain Med. 2009, 10, 663–672. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wellstead, P.; Bullinger, E.; Kalamatianos, D.; Mason, O.; Verwoerd, M. The role of control and system theory in systems biology. Annu. Rev. Control 2008, 32, 33–47. [Google Scholar] [CrossRef] [Green Version]
- Deshpande, S.; Rivera, D.E.; Younger, J. Towards patient-friendly input signal design for optimized pain treatment interventions. IFAC Proc. Vol. 2012, 45, 1311–1316. [Google Scholar] [CrossRef] [Green Version]
- Riley, W.T.; Rivera, D.E.; Atienza, A.A.; Nilsen, W.; Allison, S.M.; Mermelstein, R. Health behavior models in the age of mobile interventions: Are our theories up to the task? Transl. Behav. Med. 2011, 1, 53–71. [Google Scholar] [CrossRef] [PubMed]
- Rivera, D.E.; Pew, M.D.; Collins, L.M. Using engineering control principles to inform the design of adaptive interventions: A conceptual introduction. Drug Alcohol Depend. 2007, 88, S31–S40. [Google Scholar] [CrossRef] [PubMed]
- Zafra-Cabeza, A.; Rivera, D.E.; Collins, L.M.; Ridao, M.A.; Camacho, E.F. A risk-based model predictive control approach to adaptive interventions in behavioral health. IEEE Trans. Control Syst. Technol. 2010, 19, 891–901. [Google Scholar] [CrossRef] [PubMed]
- Younger, J.; Noor, N.; McCue, R.; Mackey, S. Low-dose naltrexone for the treatment of fibromyalgia: Findings of a small, randomized, double-blind, placebo-controlled, counterbalanced, crossover trial assessing daily pain levels. Arthritis Rheum. 2013, 65, 529–538. [Google Scholar] [CrossRef]
- Deshpande, S.; Rivera, D.E.; Younger, J.W.; Nandola, N.N. A control systems engineering approach for adaptive behavioral interventions: Illustration with a fibromyalgia intervention. Transl. Behav. Med. 2014, 4, 275–289. [Google Scholar] [CrossRef] [Green Version]
- Deshpande, S.; Nandola, N.N.; Rivera, D.E.; Younger, J.W. Optimized treatment of fibromyalgia using system identification and hybrid model predictive control. Control Eng. Pract. 2014, 33, 161–173. [Google Scholar] [CrossRef] [Green Version]
- Wodarz, D.; Page, K.M.; Arnaout, R.A.; Thomsen, A.R.; Lifson, J.D.; Nowak, M.A. A new theory of cytotoxic T–lymphocyte memory: Implications for HIV treatment. Philos. Trans. R. Soc. Lond. Ser. B Biol. Sci. 2000, 355, 329–343. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wodarz, D.; Arnaout, R.A.; Nowak, M.A.; Lifson, J.D. Transient antiretroviral treatment during acute simian immunodeficiency virus infection facilitates long–term control of the virus. Philos. Trans. R. Soc. Lond. Ser. B Biol. Sci. 2000, 355, 1021–1029. [Google Scholar] [CrossRef]
- Wodarz, D.; Nowak, M.A. Specific therapy regimes could lead to long-term immunological control of HIV. Proc. Natl. Acad. Sci. USA 1999, 96, 14464–14469. [Google Scholar] [CrossRef] [Green Version]
- Kaufmann, D.E.; Lichterfeld, M.; Altfeld, M.; Addo, M.M.; Johnston, M.N.; Lee, P.K.; Wagner, B.S.; Kalife, E.T.; Strick, D.; Rosenberg, E.S.; et al. Limited durability of viral control following treated acute HIV infection. PLoS Med. 2004, 1, e36. [Google Scholar] [CrossRef]
- Ananworanich, J.; Gayet-Ageron, A.; Le Braz, M.; Prasithsirikul, W.; Chetchotisakd, P.; Kiertiburanakul, S.; Munsakul, W.; Raksakulkarn, P.; Tansuphasawasdikul, S.; Sirivichayakul, S.; et al. CD4-guided scheduled treatment interruptions compared with continuous therapy for patients infected with HIV-1: Results of the Staccato randomised trial. Lancet 2006, 368, 459–465. [Google Scholar] [CrossRef] [PubMed]
- Benson, C.A. Structured treatment interruptions–new findings. Top. HIV Med. 2006, 14, 107–111. [Google Scholar] [PubMed]
- Strategies for Management of Antiretroviral Therapy (SMART) Study Group; El-Sadr, W.M.; Lundgren, J.D.; Neaton, J.D.; Gordin, F.; Abrams, D.; Arduino, R.C.; Babiker, A.; Burman, W.; Clumeck, N.; et al. CD4+ count–guided interruption of antiretroviral treatment. N. Engl. J. Med. 2006, 355, 2283–2296. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zurakowski, R.; Teel, A.R. A model predictive control based scheduling method for HIV therapy. J. Theor. Biol. 2006, 238, 368–382. [Google Scholar] [CrossRef]
- Ko, J.H.; Kim, W.H.; Chung, C.C. Optimized structured treatment interruption for HIV therapy and its performance analysis on controllability. IEEE Trans. Biomed. Eng. 2006, 53, 380–386. [Google Scholar] [CrossRef]
- Wodarz, D.; Nowak, M.A. Mathematical models of HIV pathogenesis and treatment. BioEssays 2002, 24, 1178–1187. [Google Scholar] [CrossRef]
- Nowak, M.A.; Bangham, C.R. Population dynamics of immune responses to persistent viruses. Science 1996, 272, 74–79. [Google Scholar] [CrossRef] [Green Version]
- Landi, A.; Mazzoldi, A.; Andreoni, C.; Bianchi, M.; Cavallini, A.; Laurino, M.; Ricotti, L.; Iuliano, R.; Matteoli, B.; Ceccherini-Nelli, L. Modelling and control of HIV dynamics. Comput. Methods Prog. Biomed. 2008, 89, 162–168. [Google Scholar] [CrossRef]
- Twumasi-Boateng, K.; Pettigrew, J.L.; Kwok, Y.E.; Bell, J.C.; Nelson, B.H. Oncolytic viruses as engineering platforms for combination immunotherapy. Nat. Rev. Cancer 2018, 18, 419–432. [Google Scholar] [CrossRef]
- Kim, P.H.; Sohn, J.H.; Choi, J.W.; Jung, Y.; Kim, S.W.; Haam, S.; Yun, C.O. Active targeting and safety profile of PEG-modified adenovirus conjugated with herceptin. Biomaterials 2011, 32, 2314–2326. [Google Scholar] [CrossRef] [PubMed]
- Haseley, A.; Alvarez-Breckenridge, C.; Chaudhury, A.R.; Kaur, B. Advances in oncolytic virus therapy for glioma. Recent Patents CNS Drug Discov. (Discontin.) 2009, 4, 1–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jenner, A.L.; Yun, C.O.; Kim, P.S.; Coster, A.C. Mathematical modelling of the interaction between cancer cells and an oncolytic virus: Insights into the effects of treatment protocols. Bull. Math. Biol. 2018, 80, 1615–1629. [Google Scholar] [CrossRef] [PubMed]
- Komarova, N.L.; Wodarz, D. ODE models for oncolytic virus dynamics. J. Theor. Biol. 2010, 263, 530–543. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jenner, A.L.; Kim, P.S.; Frascoli, F. Oncolytic virotherapy for tumours following a Gompertz growth law. J. Theor. Biol. 2019, 480, 129–140. [Google Scholar] [CrossRef]
- Anelone, A.J.; Villa-Tamayo, M.F.; Rivadeneira, P.S. Oncolytic virus therapy benefits from control theory. R. Soc. Open Sci. 2020, 7, 200473. [Google Scholar] [CrossRef]
- Rivadeneira, P.S.; Moog, C.H. Impulsive control of single-input nonlinear systems with application to HIV dynamics. Appl. Math. Comput. 2012, 218, 8462–8474. [Google Scholar] [CrossRef]
- Magdaleno, G.D.V.; García, A.Y.A.; Hernandez-Vargas, E.A. Learning neural impulsive MPC for tailoring therapies in viral infections. Appl. Soft Comput. 2019, 85, 105767. [Google Scholar] [CrossRef]
- Hernandez-Mejia, G.; Alanis, A.Y.; Hernandez-Gonzalez, M.; Findeisen, R.; Hernandez-Vargas, E.A. Passivity-based inverse optimal impulsive control for influenza treatment in the host. IEEE Trans. Control Syst. Technol. 2019, 28, 94–105. [Google Scholar] [CrossRef]
- Villa-Tamayo, M.F.; Rivadeneira, P.S. Adaptive impulsive offset-free MPC to handle parameter variations for type 1 diabetes treatment. Ind. Eng. Chem. Res. 2020, 59, 5865–5876. [Google Scholar] [CrossRef]
- Anelone, A.J.; Spurgeon, S.K. Modelling and simulation of the dynamics of the antigen-specific T cell response using variable structure control theory. PLoS ONE 2016, 11, e0166163. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rivadeneira, P.S.; Ferramosca, A.; González, A.H. Control strategies for nonzero set-point regulation of linear impulsive systems. IEEE Trans. Autom. Control 2017, 63, 2994–3001. [Google Scholar] [CrossRef]
- Villa-Tamayo, M.F.; Caicedo, M.A.; Rivadeneira, P.S. Offset-free MPC strategy for nonzero regulation of linear impulsive systems. ISA Trans. 2020, 101, 91–101. [Google Scholar] [CrossRef] [PubMed]
- Villa-Tamayo, M.F.; Anelone, A.J.; Rivadeneira, P.S. Tumor reduction using oncolytic viruses under an impulsive nonlinear estimation and predictive control scheme. IEEE Control Syst. Lett. 2020, 5, 1705–1710. [Google Scholar] [CrossRef]
- Deenen, D.A.; Maljaars, B.; Sebeke, L.C.; de Jager, B.; Heijman, E.; Grüll, H.; Heemels, W.M.H. Offset-Free Model Predictive Temperature Control for Ultrasound-Based Hyperthermia Cancer Treatments. IEEE Trans. Control Syst. Technol. 2020, 29, 2351–2365. [Google Scholar] [CrossRef]
- van der Zee, J.; González, D.; van Rhoon, G.C.; van Dijk, J.D.; van Putten, W.L.; Hart, A.A. Comparison of radiotherapy alone with radiotherapy plus hyperthermia in locally advanced pelvic tumours: A prospective, randomised, multicentre trial. Lancet 2000, 355, 1119–1125. [Google Scholar] [CrossRef]
- Overgaard, J.; Bentzen, S.; Gonzalez, D.G.; Hulshof, M.; Arcangeli, G.; Dahl, O.; Mella, O. Randomised trial of hyperthermia as adjuvant to radiotherapy for recurrent or metastatic malignant melanoma. Lancet 1995, 345, 540–543. [Google Scholar] [CrossRef]
- Dewhirst, M.; Stauffer, P.; Das, S.; Craciunescu, O.; Vujaskovic, Z.; Gunderson, L.; Tepper, J. Clinical Radiation Oncology; Elsevier: Amsterdam, The Netherlands, 2016. [Google Scholar]
- Sapareto, S.A.; Dewey, W.C. Thermal dose determination in cancer therapy. Int. J. Radiat. Oncol. Biol. Phys. 1984, 10, 787–800. [Google Scholar] [CrossRef]
- Thrall, D.; Rosner, G.; Azuma, C.; Larue, S.; Case, B.; Samulski, T.; Dewhirst, M. Using units of CEM 43 C T90, local hyperthermia thermal dose can be delivered as prescribed. Int. J. Hyperth. 2000, 16, 415–428. [Google Scholar] [CrossRef]
- Lafon, C.; Prat, F.; Chapelon, J.; Gorry, F.; Margonari, J.; Theillere, Y.; Cathignol, D. Cylindrical thermal coagulation necrosis using an interstitial applicator with a plane ultrasonic transducer: In vitro and in vivo experiments versus computer simulations. Int. J. Hyperth. 2000, 16, 508–522. [Google Scholar] [CrossRef]
- Poorter, J.D.; Wagter, C.D.; Deene, Y.D.; Thomsen, C.; Ståhlberg, F.; Achten, E. Noninvasive MRI thermometry with the proton resonance frequency (PRF) method: In vivo results in human muscle. Magn. Reson. Med. 1995, 33, 74–81. [Google Scholar] [CrossRef]
- Borelli, M.; Thompson, L.; Cain, C.; Dewey, C. Time-temperature analysis of cell killing of BHK cells heated at temperatures in the range of 43.5 C to 57 C. Int. J. Radiat. Oncol. Biol. Phys 1990, 19, 389–399. [Google Scholar] [CrossRef] [PubMed]
- Landry, J.; Marceau, N. Rate-limiting events in hyperthermic cell killing. Radiat. Res. 1978, 75, 573–585. [Google Scholar] [CrossRef] [PubMed]
- Billard, B.; Hynynen, K.; Roemer, R. Effects of physical parameters on high temperature ultrasound hyperthermia. Ultrasound Med. Biol. 1990, 16, 409–420. [Google Scholar] [CrossRef] [PubMed]
- Dorr, L.; Hynynen, K. The effects of tissue heterogeneities and large blood vessels on the thermal exposure induced by short high-power ultrasound pulses. Int. J. Hyperth. 1992, 8, 45–59. [Google Scholar] [CrossRef] [PubMed]
- Arora, D.; Skliar, M.; Roemer, R.B. Model-predictive control of hyperthermia treatments. IEEE Trans. Biomed. Eng. 2002, 49, 629–639. [Google Scholar] [CrossRef]
- Sebeke, L.; Deenen, D.; Maljaars, E.; Heijman, E.; de Jager, B.; Heemels, W.; Grüll, H. Model predictive control for MR-HIFU-mediated, uniform hyperthermia. Int. J. Hyperth. 2019, 36, 1039–1049. [Google Scholar] [CrossRef] [PubMed]













{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Notation | Meaning | Notation | Meaning |
|---|---|---|---|
| AP | Artificial Pancreas | MPC | Model Predictive Control |
| BGL | Blood Glucose Level | NMPC | Nonlinear Model Predictive Control |
| BIS | Bispectral Index | OPC | Optimum Predictive Control |
| BMM | Bergman Minimal Model | OVT | Oncolytic Viral Therapy |
| CTLs | Cytotoxic T Lymphocytes | PCT | Predictive Control Technology |
| CPHS | Cyber-Physical Human System | ||
| DMC | Dynamic Matrix Control | PEG | Polyethylene Glycol |
| DoA | Depth of Anesthesia | PI | Protease Inhibitors |
| EEG | Electroencephalogram | PID | Proportional-Integral Derivative |
| eMPC | Explicit Model Predictive Control | PWA | Piece-wise Affine Function |
| FM | Fibromyalgia | QP | Quadratic Programming |
| HAART | Highly Active Antiretroviral Therapy | RHM | Receding Horizon Technique |
| hEKF | Hybrid Extended Kalman Filter | RMPCT | Robust Model Predictive Control Technology |
| HIV | Human Immunodeficiency Virus | RPI | Robust Positively Invariant |
| ICU | Intensive Care Unit | ||
| ICS | Impulsive Control System | RTI | Reverse Transcriptase Inhibitors |
| IDCOM | Identification and Command | SISO | Single-Input and Single-Output |
| iNMPC | Impulsive Nonlinear Model Predictive Control | SNAPL | Neuroscience and Pain Lab |
| LDN | Low-Dose Naltrexone | STIs | Structured Interruptions |
| LQR | Linear Quadratic Regulator | T1D | Type 1 Diabetes |
| LR | Long Range | T2D | Type 2 Diabetes |
| LRPC | Long-Range Predictive Control | TCI | Target Controlled Infusion |
| LRQP | Long-Range Quadratic Programming | TIVA | Total Intravenous Anesthesia |
| MIMO | Multi-Input Multi-Output | VL | Viral Load |
| Linear MPC | Nonlinear MPC |
|---|---|
| Uses linear model | Nonlinear model— |
| Quadratic cost function | Cost function can be nonquadratic |
| Linear constraints < 0 | Nonlinear constraints < 0 |
| Quadratic program | Nonlinear program |
| Class of MPC | Features |
|---|---|
| Linear MPC [30] | Corrects independent variables on the basis of the plant feedback |
| Nonlinear MPC [31] | Employs nonlinear dynamic model and nonlinear constraints, resulting in increased complexity |
| Explict MPC [38] | Allows for a more rapid evaluation of the control rule |
| Robust MPC [45] | Ensures viability and long-term stability |
| Decentralized and distributed MPC [52] | Monitors and regulates local outputs and inputs |
| Feedback and feedforward MPC [18] | Reduces contraction of the feasible solution region |
| Software | MATLAB | MUP | do-MPC |
|---|---|---|---|
| Year | 2004 | 2012 | 2017 |
| Developed/created by | Mathworks | Bakosov’a, M. and Oravec, J | S. Lucia, A. Tatulea-Codrean, C. Schoppmeyer, and S. Engell |
| Methodology | – | MATLAB/Simulink toolbox for online robust MPC design in LMI-framework | Comprehensive open-source toolbox for robust model predictive control (MPC) and moving horizon estimation (MHE) |
| Model type | Continuous and discrete model | Linear matrix inequalities | Differential algebraic equations (DAE) |
| Approach | Calculates the sequence of control actions based on current state of the plant | Optimally and robustly stabilizes state-feedback control law | Efficient formulation and solution of control and estimation problems for nonlinear systems |
| Tuning | Prediction, control horizon, constraints | – | Horizon state and parameter estimation |
| Usage | Design of implicit, explicit, adaptive, and gain-scheduled MPC. For nonlinear problems, single and multi-stage nonlinear MPCs can be implemented | Practical and user-friendly solution for MPC control engineering; also an excellent choice for educational purposes. | Contains simulation, estimation and control components that can be easily extended and combined to fit many different applications |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Parihar, S.; Shah, P.; Sekhar, R.; Lagoo, J. Model Predictive Control and Its Role in Biomedical Therapeutic Automation: A Brief Review. Appl. Syst. Innov. 2022, 5, 118. https://doi.org/10.3390/asi5060118
Parihar S, Shah P, Sekhar R, Lagoo J. Model Predictive Control and Its Role in Biomedical Therapeutic Automation: A Brief Review. Applied System Innovation. 2022; 5(6):118. https://doi.org/10.3390/asi5060118
Chicago/Turabian StyleParihar, Sushma, Pritesh Shah, Ravi Sekhar, and Jui Lagoo. 2022. "Model Predictive Control and Its Role in Biomedical Therapeutic Automation: A Brief Review" Applied System Innovation 5, no. 6: 118. https://doi.org/10.3390/asi5060118