
Identify Drug-Resistant Pathogens in Patients with Community-Acquired Pneumonia
 , , , ,
, , , ,  and
and
Abstract
:Highlights
- The identification of patients with CAP at high risk for resistant pathogens is of outstanding clinical interest due to the worse outcome of these patients.
- However, the HCAP classification and the scores proposed in literature to identify resistant pathogens in CAP are overly sensitive, leading to inappropriately broad-spectrum antibiotic use.
- As suggested by the new IDSA/ATS guidelines, it is crucial to generate local data concerning DRP in order to identify and validate risk factors at a local level.
- Identification of new, rapid and specific diagnostic tests for DRP represents a clinical priority to improve the outcomes of CAP patients.
Abstract
1. Introduction
2. The Impact of Broad-Spectrum Antibiotic Use in CAP
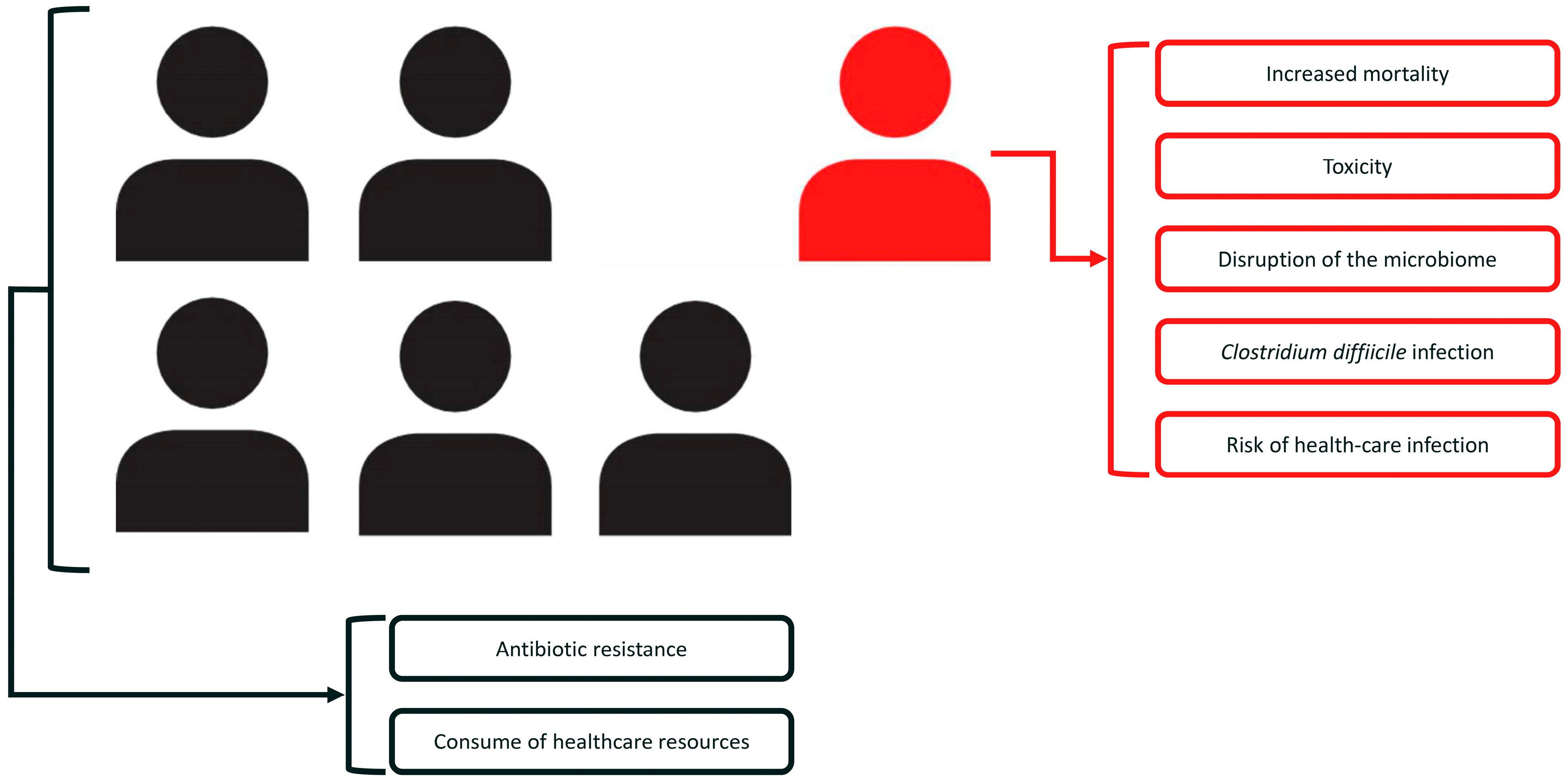
2.1. Impact on Individual-Patient Level
2.2. Impact on Public Health
3. DRP
3.1. Definition
3.2. Prevalence
3.3. The Identification of DRP: The Failing of the HCAP Classification
3.4. The Identification of DRP: The Surge of Probabilistic Approaches
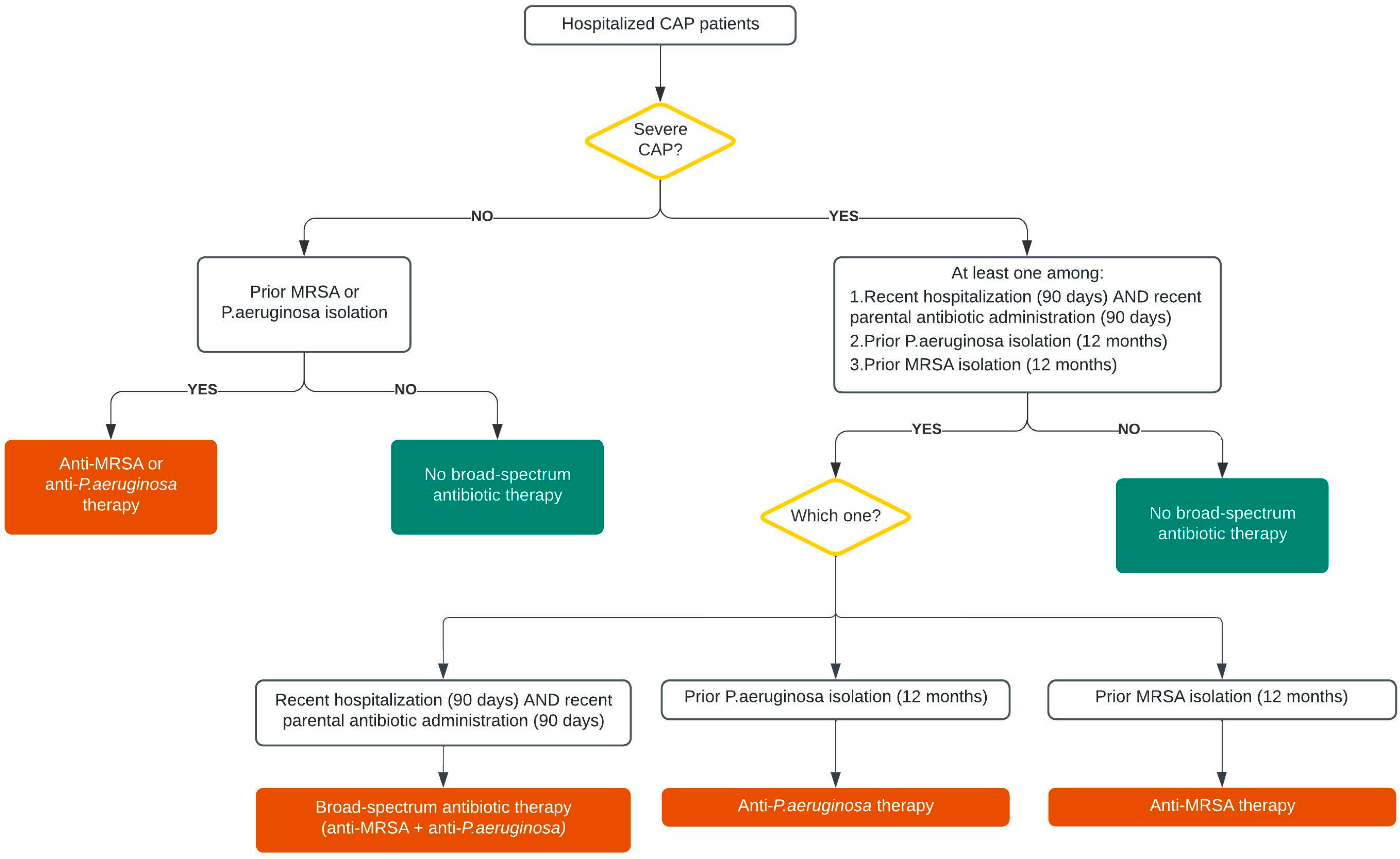
4. The New IDSA/ATS Guidelines Criteria to Identify DRP
5. Rapid Tests for DRP
6. Conclusions
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Aliberti, S.; Dela Cruz, C.S.; Amati, F.; Sotgiu, G.; Restrepo, M.I. Community-acquired pneumonia. Lancet 2021, 398, 906–919. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.S.; Giesler, D.L.; Gellad, W.F.; Fine, M.J. Antibiotic Therapy for Adults Hospitalized with Community-Acquired Pneumonia: A Systematic Review. JAMA 2016, 315, 593–602. [Google Scholar] [CrossRef] [PubMed]
- Tomczyk, S.; Jain, S.; Bramley, A.M.; Self, W.H.; Anderson, E.J.; Trabue, C.; Courtney, D.M.; Grijalva, C.G.; Waterer, G.W.; Edwards, K.M.; et al. Antibiotic Prescribing for Adults Hospitalized in the Etiology of Pneumonia in the Community Study. Open Forum Infect. Dis. 2017, 4, ofx088. [Google Scholar] [CrossRef] [PubMed]
- Jones, B.E.; Jones, M.M.; Huttner, B.; Stoddard, G.; Brown, K.A.; Stevens, V.W.; Greene, T.; Sauer, B.; Madaras-Kelly, K.; Rubin, M.; et al. Trends in Antibiotic Use and Nosocomial Pathogens in Hospitalized Veterans With Pneumonia at 128 Medical Centers, 2006–2010. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2015, 61, 1403–1410. [Google Scholar] [CrossRef] [PubMed]
- Waagsbø, B.; Tranung, M.; Damås, J.K.; Heggelund, L. Antimicrobial therapy of community-acquired pneumonia during stewardship efforts and a coronavirus pandemic: An observational study. BMC Pulm. Med. 2022, 22, 379. [Google Scholar] [CrossRef]
- Aliberti, S.; Reyes, L.F.; Faverio, P.; Sotgiu, G.; Dore, S.; Rodriguez, A.H.; Soni, N.J.; Restrepo, M.I.; GLIMP investigators. Global initiative for meticillin-resistant Staphylococcus aureus pneumonia (GLIMP): An international, observational cohort study. Lancet Infect. Dis. 2016, 16, 1364–1376. [Google Scholar] [CrossRef] [PubMed]
- Chalmers, J.D.; Taylor, J.K.; Singanayagam, A.; Fleming, G.B.; Akram, A.R.; Mandal, P.; Choudhury, G.; Hill, A.T. Epidemiology, antibiotic therapy, and clinical outcomes in health care-associated pneumonia: A UK cohort study. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2011, 53, 107–113. [Google Scholar] [CrossRef]
- von Baum, H.; Welte, T.; Marre, R.; Suttorp, N.; Ewig, S.; CAPNETZ Study Group. Community-acquired pneumonia through Enterobacteriaceae and Pseudomonas aeruginosa: Diagnosis, incidence and predictors. Eur. Respir. J. 2010, 35, 598–605. [Google Scholar] [CrossRef]
- Cillóniz, C.; Gabarrús, A.; Ferrer, M.; Puig de la Bellacasa, J.; Rinaudo, M.; Mensa, J.; Niederman, M.S.; Torres, A. Community-Acquired Pneumonia Due to Multidrug- and Non-Multidrug-Resistant Pseudomonas aeruginosa. Chest 2016, 150, 415–425. [Google Scholar] [CrossRef]
- Restrepo, M.I.; Babu, B.L.; Reyes, L.F.; Chalmers, J.D.; Soni, N.J.; Sibila, O.; Faverio, P.; Cilloniz, C.; Rodriguez-Cintron, W.; Aliberti, S.; et al. Burden and risk factors for Pseudomonas aeruginosa community-acquired pneumonia: A multinational point prevalence study of hospitalised patients. Eur. Respir. J. 2018, 52, 1701190. [Google Scholar] [CrossRef]
- Arancibia, F.; Bauer, T.T.; Ewig, S.; Mensa, J.; Gonzalez, J.; Niederman, M.S.; Torres, A. Community-acquired pneumonia due to gram-negative bacteria and pseudomonas aeruginosa: Incidence, risk, and prognosis. Arch. Intern. Med. 2002, 162, 1849–1858. [Google Scholar] [CrossRef] [PubMed]
- Jung, W.J.; Kang, Y.A.; Park, M.S.; Park, S.C.; Leem, A.Y.; Kim, E.Y.; Chung, K.S.; Kim, Y.S.; Kim, S.K.; Chang, J.; et al. Prediction of methicillin-resistant Staphylococcus aureus in patients with non-nosocomial pneumonia. BMC Infect. Dis. 2013, 13, 370. [Google Scholar] [CrossRef] [PubMed]
- Minejima, E.; Lou, M.; Nieberg, P.; Wong-Beringer, A. Patients presenting to the hospital with MRSA pneumonia: Differentiating characteristics and outcomes with empiric treatment. BMC Infect. Dis. 2014, 14, 252. [Google Scholar] [CrossRef] [PubMed]
- Wooten, D.A.; Winston, L.G. Risk factors for methicillin-resistant Staphylococcus aureus in patients with community-onset and hospital-onset pneumonia. Respir. Med. 2013, 107, 1266–1270. [Google Scholar] [CrossRef] [PubMed]
- Aliberti, S.; Cilloniz, C.; Chalmers, J.D.; Zanaboni, A.M.; Cosentini, R.; Tarsia, P.; Pesci, A.; Blasi, F.; Torres, A. Multidrug-resistant pathogens in hospitalised patients coming from the community with pneumonia: A European perspective. Thorax 2013, 68, 997–999. [Google Scholar] [CrossRef] [PubMed]
- Shorr, A.F.; Zilberberg, M.D.; Micek, S.T.; Kollef, M.H. Prediction of infection due to antibiotic-resistant bacteria by select risk factors for health care-associated pneumonia. Arch. Intern. Med. 2008, 168, 2205–2210. [Google Scholar] [CrossRef]
- Idigo, A.J.; Wells, J.M.; Brown, M.L.; Wiener, H.W.; Griffin, R.L.; Cutter, G.; Shrestha, S.; Lee, R.A. Clinical risk factors for admission with Pseudomonas and multidrug-resistant Pseudomonas community-acquired pneumonia. Antimicrob. Resist. Infect. Control. 2022, 11, 95. [Google Scholar] [CrossRef]
- Park, S.C.; Kim, E.Y.; Kang, Y.A.; Park, M.S.; Kim, Y.S.; Kim, S.K.; Chang, J.; Jung, J.Y. Validation of a scoring tool to predict drug-resistant pathogens in hospitalised pneumonia patients. Int. J. Tuberc. Lung Dis. Off. J. Int. Union Against Tuberc. Lung Dis. 2013, 17, 704–709. [Google Scholar] [CrossRef]
- Webb, B.J.; Dascomb, K.; Stenehjem, E.; Vikram, H.R.; Agrwal, N.; Sakata, K.; Williams, K.; Bockorny, B.; Bagavathy, K.; Mirza, S.; et al. Derivation and Multicenter Validation of the Drug Resistance in Pneumonia Clinical Prediction Score. Antimicrob. Agents Chemother. 2016, 60, 2652–2663. [Google Scholar] [CrossRef]
- American Thoracic Society; Infectious Diseases Society of America. Guidelines for the management of adults with hospital-acquired, ventilator-associated, and healthcare-associated pneumonia. Am. J. Respir. Crit. Care Med. 2005, 171, 388–416. [Google Scholar] [CrossRef]
- Aliberti, S.; Di Pasquale, M.; Zanaboni, A.M.; Cosentini, R.; Brambilla, A.M.; Seghezzi, S.; Tarsia, P.; Mantero, M.; Blasi, F. Stratifying risk factors for multidrug-resistant pathogens in hospitalized patients coming from the community with pneumonia. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2012, 54, 470–478. [Google Scholar] [CrossRef] [PubMed]
- Shindo, Y.; Ito, R.; Kobayashi, D.; Ando, M.; Ichikawa, M.; Shiraki, A.; Goto, Y.; Fukui, Y.; Iwaki, M.; Okumura, J.; et al. Risk factors for drug-resistant pathogens in community-acquired and healthcare-associated pneumonia. Am. J. Respir. Crit. Care Med. 2013, 188, 985–995. [Google Scholar] [CrossRef] [PubMed]
- Ma, H.M.; Ip, M.; Woo, J.; Hui, D.S. Development and validation of a clinical risk score for predicting drug-resistant bacterial pneumonia in older Chinese patients. Respirology 2014, 19, 549–555. [Google Scholar] [CrossRef]
- Prina, E.; Ranzani, O.T.; Polverino, E.; Cillóniz, C.; Ferrer, M.; Fernandez, L.; Puig de la Bellacasa, J.; Menéndez, R.; Mensa, J.; Torres, A. Risk factors associated with potentially antibiotic-resistant pathogens in community-acquired pneumonia. Ann. Am. Thorac. Soc. 2015, 12, 153–160. [Google Scholar] [CrossRef]
- Falcone, M.; Russo, A.; Giannella, M.; Cangemi, R.; Scarpellini, M.G.; Bertazzoni, G.; Alarcón, J.M.; Taliani, G.; Palange, P.; Farcomeni, A.; et al. Individualizing risk of multidrug-resistant pathogens in community-onset pneumonia. PLoS ONE 2015, 10, e0119528. [Google Scholar] [CrossRef]
- Shorr, A.F.; Myers, D.E.; Huang, D.B.; Nathanson, B.H.; Emons, M.F.; Kollef, M.H. A risk score for identifying methicillin-resistant Staphylococcus aureus in patients presenting to the hospital with pneumonia. BMC Infect. Dis. 2013, 13, 268. [Google Scholar] [CrossRef] [PubMed]
- Rothberg, M.B.; Haessler, S.; Deshpande, A.; Yu, P.C.; Lindenauer, P.K.; Zilberberg, M.D.; Higgins, T.L.; Imrey, P.B. Derivation and validation of a risk assessment model for drug-resistant pathogens in hospitalized patients with community-acquired pneumonia. Infect. Control. Hosp. Epidemiol. 2022, 1–8, advance online publication. [Google Scholar] [CrossRef]
- Amati, F.; Restrepo, M.I. Emerging Resistance of Gram Negative Pathogens in Community-Acquired Pneumonia. Semin. Respir. Crit. Care Med. 2020, 41, 480–495. [Google Scholar] [CrossRef] [PubMed]
- Webb, B.J.; Sorensen, J.; Jephson, A.; Mecham, I.; Dean, N.C. Broad-spectrum antibiotic use and poor outcomes in community-onset pneumonia: A cohort study. Eur. Respir. J. 2019, 54, 1900057. [Google Scholar] [CrossRef] [PubMed]
- Rothberg, M.B.; Zilberberg, M.D.; Pekow, P.S.; Priya, A.; Haessler, S.; Belforti, R.; Skiest, D.; Lagu, T.; Higgins, T.L.; Lindenauer, P.K. Association of guideline-based antimicrobial therapy and outcomes in healthcare-associated pneumonia. J. Antimicrob. Chemother. 2015, 70, 1573–1579. [Google Scholar] [CrossRef]
- Webb, B.J.; Dangerfield, B.S.; Pasha, J.S.; Agrwal, N.; Vikram, H.R. Guideline-concordant antibiotic therapy and clinical outcomes in healthcare-associated pneumonia. Respir. Med. 2012, 106, 1606–1612. [Google Scholar] [CrossRef]
- Falcone, M.; Corrao, S.; Licata, G.; Serra, P.; Venditti, M. Clinical impact of broad-spectrum empirical antibiotic therapy in patients with healthcare-associated pneumonia: A multicenter interventional study. Intern. Emerg. Med. 2012, 7, 523–531. [Google Scholar] [CrossRef]
- Jones, B.E.; Ying, J.; Stevens, V.; Haroldsen, C.; He, T.; Nevers, M.; Christensen, M.A.; Nelson, R.E.; Stoddard, G.J.; Sauer, B.C.; et al. Empirical Anti-MRSA vs Standard Antibiotic Therapy and Risk of 30-Day Mortality in Patients Hospitalized for Pneumonia. JAMA Intern. Med. 2020, 180, 552–560. [Google Scholar] [CrossRef] [PubMed]
- Attridge, R.T.; Frei, C.R.; Restrepo, M.I.; Lawson, K.A.; Ryan, L.; Pugh, M.J.; Anzueto, A.; Mortensen, E.M. Guideline-concordant therapy and outcomes in healthcare-associated pneumonia. Eur. Respir. J. 2011, 38, 878–887. [Google Scholar] [CrossRef]
- Kobayashi, H.; Shindo, Y.; Kobayashi, D.; Sakakibara, T.; Murakami, Y.; Yagi, M.; Matsuura, A.; Sato, K.; Matsui, K.; Emoto, R.; et al. Extended-spectrum antibiotics for community-acquired pneumonia with a low risk for drug-resistant pathogens. Int. J. Infect. Dis. IJID Off. Publ. Int. Soc. Infect. Dis. 2022, 124, 124–132. [Google Scholar] [CrossRef] [PubMed]
- Vaughn, V.M.; Flanders, S.A.; Snyder, A.; Conlon, A.; Rogers, M.A.M.; Malani, A.N.; McLaughlin, E.; Bloemers, S.; Srinivasan, A.; Nagel, J.; et al. Excess Antibiotic Treatment Duration and Adverse Events in Patients Hospitalized With Pneumonia: A Multihospital Cohort Study. Ann. Intern. Med. 2019, 171, 153–163. [Google Scholar] [CrossRef] [PubMed]
- GBD 2019 Antimicrobial Resistance Collaborators. Global mortality associated with 33 bacterial pathogens in 2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet 2022, 400, 2221–2248. [Google Scholar] [CrossRef] [PubMed]
- Zak-Doron, Y.; Dishon Benattar, Y.; Pfeffer, I.; Daikos, G.L.; Skiada, A.; Antoniadou, A.; Durante-Mangoni, E.; Andini, R.; Cavezza, G.; Leibovici, L.; et al. The Association Between Empirical Antibiotic Treatment and Mortality in Severe Infections Caused by Carbapenem-resistant Gram-negative Bacteria: A Prospective Study. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2018, 67, 1815–1823. [Google Scholar] [CrossRef]
- Chalmers, J.D.; Rother, C.; Salih, W.; Ewig, S. Healthcare-associated pneumonia does not accurately identify potentially resistant pathogens: A systematic review and meta-analysis. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2014, 58, 330–339. [Google Scholar] [CrossRef]
- Klompas, M. Overuse of Broad-Spectrum Antibiotics for Pneumonia. JAMA Intern. Med. 2020, 180, 485–486. [Google Scholar] [CrossRef]
- Tarrant, C.; Colman, A.M.; Jenkins, D.R.; Chattoe-Brown, E.; Perera, N.; Mehtar, S.; Nakkawita, W.M.I.D.; Bolscher, M.; Krockow, E.M. Drivers of Broad-Spectrum Antibiotic Overuse across Diverse Hospital Contexts-A Qualitative Study of Prescribers in the UK, Sri Lanka and South Africa. Antibiotics 2021, 10, 94. [Google Scholar] [CrossRef] [PubMed]
- Jiao, J.; Yang, X.Y.; Li, Z.; Zhao, Y.W.; Cao, J.; Li, F.F.; Liu, Y.; Liu, G.; Song, B.Y.; Jin, J.F.; et al. Incidence and Related Factors for Hospital-Acquired Pneumonia Among Older Bedridden Patients in China: A Hospital-Based Multicenter Registry Data Based Study. Front. Public Health 2019, 7, 221. [Google Scholar] [CrossRef]
- Kalil, A.C.; Metersky, M.L.; Klompas, M.; Muscedere, J.; Sweeney, D.A.; Palmer, L.B.; Napolitano, L.M.; O’Grady, N.P.; Bartlett, J.G.; Carratalà, J.; et al. Management of Adults With Hospital-acquired and Ventilator-associated Pneumonia: 2016 Clinical Practice Guidelines by the Infectious Diseases Society of America and the American Thoracic Society. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2016, 63, e61–e111. [Google Scholar] [CrossRef] [PubMed]
- El Solh, A.A.; Akinnusi, M.E.; Alfarah, Z.; Patel, A. Effect of antibiotic guidelines on outcomes of hospitalized patients with nursing home-acquired pneumonia. J. Am. Geriatr. Soc. 2009, 57, 1030–1035. [Google Scholar] [CrossRef] [PubMed]
- Taylor, S.P.; Taylor, B.T. Health care-associated pneumonia in haemodialysis patients: Clinical outcomes in patients treated with narrow versus broad spectrum antibiotic therapy. Respirology 2013, 18, 364–368. [Google Scholar] [CrossRef]
- Berger, A.; Edelsberg, J.; Oster, G.; Huang, X.; Weber, D.J. Patterns of initial antibiotic therapy for community-acquired pneumonia in U.S. hospitals, 2000 to 2009. Am. J. Med. Sci. 2014, 347, 347–356. [Google Scholar] [CrossRef] [PubMed]
- Luther, M.K.; Timbrook, T.T.; Caffrey, A.R.; Dosa, D.; Lodise, T.P.; LaPlante, K.L. Vancomycin Plus Piperacillin-Tazobactam and Acute Kidney Injury in Adults: A Systematic Review and Meta-Analysis. Crit. Care Med. 2018, 46, 12–20. [Google Scholar] [CrossRef]
- Lee, J.D.; Heintz, B.H.; Mosher, H.J.; Livorsi, D.J.; Egge, J.A.; Lund, B.C. Risk of Acute Kidney Injury and Clostridioides difficile Infection With Piperacillin/Tazobactam, Cefepime, and Meropenem With or Without Vancomycin. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2021, 73, e1579–e1586. [Google Scholar] [CrossRef] [PubMed]
- Wunderink, R.G.; Niederman, M.S.; Kollef, M.H.; Shorr, A.F.; Kunkel, M.J.; Baruch, A.; McGee, W.T.; Reisman, A.; Chastre, J. Linezolid in methicillin-resistant Staphylococcus aureus nosocomial pneumonia: A randomized, controlled study. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2012, 54, 621–629. [Google Scholar] [CrossRef]
- Kang, S.; Park, J.; Yu, Y.M.; Park, M.S.; Han, E.; Chang, M.J. Comparison of acute kidney injury and clinical prognosis of vancomycin monotherapy and combination therapy with beta-lactams in the intensive care unit. PLoS ONE 2019, 14, e0217908. [Google Scholar] [CrossRef] [PubMed]
- Nishino, Y.; Takemura, S.; Minamiyama, Y.; Hirohashi, K.; Tanaka, H.; Inoue, M.; Okada, S.; Kinoshita, H. Inhibition of vancomycin-induced nephrotoxicity by targeting superoxide dismutase to renal proximal tubule cells in the rat. Redox Rep. Commun. Free. Radic. Res. 2002, 7, 317–319. [Google Scholar] [CrossRef] [PubMed]
- Elyasi, S.; Khalili, H.; Dashti-Khavidaki, S.; Mohammadpour, A. Vancomycin-induced nephrotoxicity: Mechanism, incidence, risk factors and special populations. A literature review. Eur. J. Clin. Pharmacol. 2012, 68, 1243–1255. [Google Scholar] [CrossRef]
- Gomes, D.M.; Smotherman, C.; Birch, A.; Dupree, L.; Della Vecchia, B.J.; Kraemer, D.F.; Jankowski, C.A. Comparison of acute kidney injury during treatment with vancomycin in combination with piperacillin-tazobactam or cefepime. Pharmacotherapy 2014, 34, 662–669. [Google Scholar] [CrossRef] [PubMed]
- Burgess, L.D.; Drew, R.H. Comparison of the incidence of vancomycin-induced nephrotoxicity in hospitalized patients with and without concomitant piperacillin-tazobactam. Pharmacotherapy 2014, 34, 670–676. [Google Scholar] [CrossRef]
- Chawla, L.S.; Amdur, R.L.; Faselis, C.; Li, P.; Kimmel, P.L.; Palant, C.E. Impact of Acute Kidney Injury in Patients Hospitalized With Pneumonia. Crit. Care Med. 2017, 45, 600–606. [Google Scholar] [CrossRef]
- Chalmers, J.D.; Al-Khairalla, M.; Short, P.M.; Fardon, T.C.; Winter, J.H. Proposed changes to management of lower respiratory tract infections in response to the Clostridium difficile epidemic. J. Antimicrob. Chemother. 2010, 65, 608–618. [Google Scholar] [CrossRef] [PubMed]
- Baggs, J.; Jernigan, J.A.; Halpin, A.L.; Epstein, L.; Hatfield, K.M.; McDonald, L.C. Risk of Subsequent Sepsis Within 90 Days After a Hospital Stay by Type of Antibiotic Exposure. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2018, 66, 1004–1012. [Google Scholar] [CrossRef]
- Geller, A.I.; Lovegrove, M.C.; Shehab, N.; Hicks, L.A.; Sapiano, M.R.P.; Budnitz, D.S. National Estimates of Emergency Department Visits for Antibiotic Adverse Events Among Adults-United States, 2011-2015. J. Gen. Intern. Med. 2018, 33, 1060–1068. [Google Scholar] [CrossRef] [PubMed]
- Vardakas, K.Z.; Kalimeris, G.D.; Triarides, N.A.; Falagas, M.E. An update on adverse drug reactions related to β-lactam antibiotics. Expert Opin. Drug Saf. 2018, 17, 499–508. [Google Scholar] [CrossRef]
- Carrabba, M.; Zarantonello, M.; Formica, S.; Mellace, L.; Castaldi, S.; Cappellini, M.D.; Fabio, G. Pneumonia and Clostridium difficile infection: Hospital acquired infection in a non-ICU department. Eur. Respir. J. 2012, 40 (Suppl. S56), 2469. [Google Scholar]
- Piccioni, A.; Rosa, F.; Manca, F.; Pignataro, G.; Zanza, C.; Savioli, G.; Covino, M.; Ojetti, V.; Gasbarrini, A.; Franceschi, F.; et al. Gut Microbiota and Clostridium difficile: What We Know and the New Frontiers. Int. J. Mol. Sci. 2022, 23, 13323. [Google Scholar] [CrossRef] [PubMed]
- Patangia, D.V.; Anthony Ryan, C.; Dempsey, E.; Paul Ross, R.; Stanton, C. Impact of antibiotics on the human microbiome and consequences for host health. MicrobiologyOpen 2022, 11, e1260. [Google Scholar] [CrossRef] [PubMed]
- Becerra, M.B.; Becerra, B.J.; Banta, J.E.; Safdar, N. Impact of Clostridium difficile infection among pneumonia and urinary tract infection hospitalizations: An analysis of the Nationwide Inpatient Sample. BMC Infect. Dis. 2015, 15, 254. [Google Scholar] [CrossRef] [PubMed]
- Costelloe, C.; Metcalfe, C.; Lovering, A.; Mant, D.; Hay, A.D. Effect of antibiotic prescribing in primary care on antimicrobial resistance in individual patients: Systematic review and meta-analysis. BMJ 2010, 340, c2096. [Google Scholar] [CrossRef]
- Lode, H. Safety and tolerability of commonly prescribed oral antibiotics for the treatment of respiratory tract infections. Am. J. Med. 2010, 123 (Suppl. S4), S26–S38. [Google Scholar] [CrossRef]
- Mba, I.E.; Nweze, E.I. Nanoparticles as therapeutic options for treating multidrug-resistant bacteria: Research progress, challenges, and prospects. World J. Microbiol. Biotechnol. 2021, 37, 108. [Google Scholar] [CrossRef]
- Infectious Diseases Society of America The 10 × ′20 Initiative: Pursuing a global commitment to develop 10 new antibacterial drugs by 2020. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2010, 50, 1081–1083. [CrossRef]
- WHO Publishes List of Bacteria for Which New Antibiotics Are Urgently Needed. Available online: https://www.who.int/news-room/detail/27-02-2017-who-publishes-list-of-bacteria-for-which-new-antibiotics-are-urgently-needed (accessed on 27 September 2022).
- Ko Kostyanev, T.; Bonten, M.J.; O’Brien, S.; Steel, H.; Ross, S.; François, B.; Tacconelli, E.; Winterhalter, M.; Stavenger, R.A.; Karlén, A.; et al. The Innovative Medicines Initiative’s New Drugs for Bad Bugs programme: European public-private partnerships for the development of new strategies to tackle antibiotic resistance. J. Antimicrob. Chemother. 2016, 71, 290–295. [Google Scholar] [CrossRef]
- Terreni, M.; Taccani, M.; Pregnolato, M. New Antibiotics for Multidrug-Resistant Bacterial Strains: Latest Research Developments and Future Perspectives. Molecules 2021, 26, 2671. [Google Scholar] [CrossRef]
- Nori, P.; Cowman, K.; Chen, V.; Bartash, R.; Szymczak, W.; Madaline, T.; Punjabi Katiyar, C.; Jain, R.; Aldrich, M.; Weston, G.; et al. Bacterial and fungal coinfections in COVID-19 patients hospitalized during the New York City pandemic surge. Infect. Control. Hosp. Epidemiol. 2021, 42, 84–88. [Google Scholar] [CrossRef]
- Trouillet, J.L.; Chastre, J.; Vuagnat, A.; Joly-Guillou, M.L.; Combaux, D.; Dombret, M.C.; Gibert, C. Ventilator-associated pneumonia caused by potentially drug-resistant bacteria. Am. J. Respir. Crit. Care Med. 1998, 157, 531–539. [Google Scholar] [CrossRef] [PubMed]
- Magiorakos, A.P.; Srinivasan, A.; Carey, R.B.; Carmeli, Y.; Falagas, M.E.; Giske, C.G.; Harbarth, S.; Hindler, J.F.; Kahlmeter, G.; Olsson-Liljequist, B.; et al. Multidrug-resistant, extensively drug-resistant and pandrug-resistant bacteria: An international expert proposal for interim standard definitions for acquired resistance. Clin. Microbiol. Infect. Off. Publ. Eur. Soc. Clin. Microbiol. Infect. Dis. 2012, 18, 268–281. [Google Scholar] [CrossRef] [PubMed]
- Schreiber, M.P.; Chan, C.M.; Shorr, A.F. Resistant pathogens in nonnosocomial pneumonia and respiratory failure: Is it time to refine the definition of health-care-associated pneumonia? Chest 2010, 137, 1283–1288. [Google Scholar] [CrossRef] [PubMed]
- Kollef, M.H.; Shorr, A.; Tabak, Y.P.; Gupta, V.; Liu, L.Z.; Johannes, R.S. Epidemiology and outcomes of health-care-associated pneumonia: Results from a large US database of culture-positive pneumonia. Chest 2005, 128, 3854–3862. [Google Scholar] [CrossRef] [PubMed]
- Metersky, M.L.; Frei, C.R.; Mortensen, E.M. Predictors of Pseudomonas and methicillin-resistant Staphylococcus aureus in hospitalized patients with healthcare-associated pneumonia. Respirology 2016, 21, 157–163. [Google Scholar] [CrossRef]
- Metlay, J.P.; Waterer, G.W.; Long, A.C.; Anzueto, A.; Brozek, J.; Crothers, K.; Cooley, L.A.; Dean, N.C.; Fine, M.J.; Flanders, S.A.; et al. Diagnosis and Treatment of Adults with Community-acquired Pneumonia. An Official Clinical Practice Guideline of the American Thoracic Society and Infectious Diseases Society of America. Am. J. Respir. Crit. Care Med. 2019, 200, e45–e67. [Google Scholar] [CrossRef]
- Di Pasquale, M.F.; Sotgiu, G.; Gramegna, A.; Radovanovic, D.; Terraneo, S.; Reyes, L.F.; Rupp, J.; González Del Castillo, J.; Blasi, F.; Aliberti, S.; et al. Prevalence and Etiology of Community-acquired Pneumonia in Immunocompromised Patients. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2019, 68, 1482–1493. [Google Scholar] [CrossRef]
- Buchan, B.W.; Windham, S.; Faron, M.L.; Balada-Llasat, J.M.; Relich, R.F.; Humphries, R.; Miller, S.; Harrington, A.; Murphy, C.; Leber, A.; et al. Clinical Evaluation and Potential Impact of a Semi-Quantitative Multiplex Molecular Assay for the Identification of Pathogenic Bacteria and Viruses in Lower Respiratory specimens. In Proceedings of the American Thoracic Society Conference, San Diego, CA, USA, 20 May 2018. [Google Scholar]
- Johansson, N.; Kalin, M.; Tiveljung-Lindell, A.; Giske, C.G.; Hedlund, J. Etiology of community-acquired pneumonia: Increased microbiological yield with new diagnostic methods. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2010, 50, 202–209. [Google Scholar] [CrossRef]
- Dangerfield, B.; Chung, A.; Webb, B.; Seville, M.T. Predictive value of methicillin-resistant Staphylococcus aureus (MRSA) nasal swab PCR assay for MRSA pneumonia. Antimicrob. Agents Chemother. 2014, 58, 859–864. [Google Scholar] [CrossRef]
- Parente, D.M.; Cunha, C.B.; Mylonakis, E.; Timbrook, T.T. The Clinical Utility of Methicillin-Resistant Staphylococcus aureus (MRSA) Nasal Screening to Rule Out MRSA Pneumonia: A Diagnostic Meta-analysis With Antimicrobial Stewardship Implications. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2018, 67, 1–7. [Google Scholar] [CrossRef]
- Sakr, A.; Brégeon, F.; Mège, J.L.; Rolain, J.M.; Blin, O. Staphylococcus aureus Nasal Colonization: An Update on Mechanisms, Epidemiology, Risk Factors, and Subsequent Infections. Front. Microbiol. 2018, 9, 2419. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| First Author and Year | Country | Number of Patients | Culture Positive | Number of DRP (%) | MRSA (%) | Pseudomonas aeruginosa (%) | Other DRP (%) |
|---|---|---|---|---|---|---|---|
| Shorr 2008 [26] | USA | 639 | 639 (100%) | 289 (45.2%) | 157 (24.6%) | 120 (18.8%) | 47 (7.4%) |
| Schrieber 2010 [74] | USA | 190 | 190 (100%) | 62 (32.6%) | 35 (18.4%) | 25 (13.2%) | 2 (1%) |
| Aliberti 2012 [21] | Italy | 935 | 170 (18%) | 33 (3.5%) | 16 (1.7%) | 7 (0.7%) | 10 (1.1%) |
| Park 2013 [18] | South Korea | 339 | 339 (100%) | 122 (36%) | 27 (8%) | 58 (17.1%) | 37 (10.9%) |
| Shindo 2013 [22] | Japan | 1413 | 795 (56,3%) | 170 (12.3%) | 77 (5.4%) | 79 (5.6%) | 14 (1%) |
| Ma 2014 [23] | China | 450 | 450 (100%) | 69 (15.3%) | 8 (1.8%) | 56 (12.4%) | 6 (1.3%) |
| Prina 2015 [24] | Spain | 1597 | 1597 (100%) | 108 (6.8%) | 21 (1.3%) | 72 (4.5%) | 15 (0.9%) |
| Falcone 2015 [25] | Italy | 900 | 300 (33.3%) | 99 (11%) | 50 (5.6%) | 17 (1.9%) | 32 (3.5%) |
| Webb 2016 [19] | USA | 400 | 400 (100%) | 124 (31%) | 57 (14.2%) | 34 (8.5%) | 33 (8.2%) |
| Rothberg 2022 [27] | USA | 138,940 | 12,181 (8.8%) | 5200 (3.8%) | Not analyzed | Not analyzed | Not analyzed |
| First Author and Year | Country | DRP | Number of Patients | Risk Factors and Points | Design | External Validation | Threshold for Definition of Risk for DRP |
|---|---|---|---|---|---|---|---|
| Shorr 2008 [26] | USA | MRSA, P aeruginosa, extended-spectrum β-lactamase–producing Klebsiella species, and other nonfermenting gram-negative bacteria * | 639 | Recent hospitalization = 3 Nursing home residence = 2 Hemodialysis = 2 ICU admission= 1 | Retrospective Single center Culture positive Hospitalized | Yes | ≥1 point |
| Schrieber 2010 [74] | USA | MRSA, P. aeruginosa, ESBL-producing bacteria | 190 | Immunosuppression = 3 Admission from long-term care= 2 Prior antibiotics, 1 | Retrospective Single center Culture-positive ICU patients | No | ≥2 points |
| Aliberti 2012 [21] | Italy | MRSA; P. aeruginosa resistant to antipseudomonal penicillins, cephalosporins, carbapenems, and quinolones; Stenotrophomonas maltophilia; vancomycin-resistant Enterococcus; A. baumanii; ESBL–producing Enterobacteriaceae; other nonfermenting gram-negative bacilli | 935 | Chronic renal failure =5 Hospitalization in the preceding 90 days =4 Residence in a nursing home =3 Others (cerebrovascular disease, diabetes, COPD, immunosuppression, home wound care, prior antimicrobial therapy and home infusion therapy) = 0.5 | Prospective Single center Ward and ICU All CAP patients | Yes | ≥3 points |
| Park 2013 [18] | South Korea | MRSA, P.aeruginosa, A. baumannii, S. maltophilia, and ESBL-producing Enterobacteriaceae | 339 | Tube feeding = 5 Recent hospitalization= 3 Recent (30 days) intravenous antibiotics =2 Admission from long-term care facility= 1 Recent (30 days) chemotherapy =1 Recent (30 days) wound care = 1 Chronic dialysis =1 | Retrospective Single center Ward and ICU Culture-positive | No | ≥3 points |
| Shindo 2013 [22] | Japan | Any microorganism resistant to at least one agent in three or more groups of antibiotics | 1413 | Recent hospitalization (last 90 days) =1 Immunosuppression =1 Home infusion therapy (last 90 days) =1 Use of gastric acid-suppressive agents =1 Tube feeding =1 Non-ambulatory status =1 | Prospective Multicenter Inpatients All CAP patients | Yes | ≥3 points |
| Ma 2014 [23] | China | MRSA, P. aeruginosa, extended-spectrumβ-lactamase (ESBL)-producing Enterobacteriaceae and A. baumannii. | 450 | Bronchiectasis =14 Recent hospitalization = 5 Severe pneumonia = 2 Others (nursing home residence, home infusion therapy, chronic wound care, chronic dialysis or immunosuppression) = 0.5 each | Prospective Single center Inpatients Culture positive | No | ≥2.5 points |
| Prina 2015 [24] | Spain | P. aeruginosa, ESBL-positive Enterobacteriaceae, and MRSA | 1597 | Age 40–65 years =1 Age >65 years =2 Male =1 Previous antibiotic use =2 Chronic respiratory disease (COPD or bronchiectasis) = 2 Chronic renal disease =3 Consciousness impairment= 2 Fever = 1 | Prospective Single center Inpatients Culture positive | Yes | ≥2 points |
| Falcone 2015 [25] | Italy | MRSA, S. maltophilia, ESBL–producing or carbapenem-resistant Enterobacteriaceae, PLUS any bacterial strain non-susceptible to at least one agent in three or more antimicrobial categories. | 900 | HCAP criteria= 1 Bilateral pulmonary infiltrations= 0.5 Pleural effusion= 0.5 PaO2/FiO2 <300 = 1.5 | Prospective Single center All CAP patients | Yes | ≥3 points |
| Webb 2016 [19] | USA | MRSA, P. aeruginosa, Enterobacteriaceae drug-resistant | 400 | Prior antibiotics = 2 Residence in a long-term care facility = 2 Tube feeding = 2 Infection with a drug-resistant pathogen in the previous year = 2 Hospitalization (60 days) = 1 Chronic pulmonary disease= 1 Poor functional status= 1 Gastric acid suppression = 1 Wound care = 1 MRSA colonization in the previous year = 1 | Retrospective Multicenter Culture positive | Yes | ≥4 points |
| Rothberg 2022 [27] | USA | Any organism resistant to either a quinolone or the combination of a third-generation cephalosporin and a macrolide | 138,940 | Resistant organism in previous year † = 2.5 Invasive mechanical ventilation (IMV) = 2 Pressure ulcer = 1.5 Vasopressor Administration = 1.5 Paralysis = 1.5 Admission to intensive care unit (ICU) = 1.5 Low functional status/weight loss = 1.5 Hospital admission in previous year = 1.5 Admitted from skilled nursing or intermediate care Facility = 1.5 Chronic pulmonary disease = 1.5 Male sex = 1.5 Current tobacco smoker = 1 | Retrospective Multicenter Inpatients All CAP patients | No | >4 points |
| Risk Factor | MRSA | P. aeruginosa |
|---|---|---|
| Comorbidity | ||
| Chronic lung diseases (defined as COPD and or bronchiectasis) | X | X |
| Cerebrovascular diseases | X | |
| Diabetes mellitus | X | |
| Altered mental status | X | |
| Recurrent skin infection | X | |
| Prior exposure | ||
| Prior infection or colonization | X | X |
| Prior antibiotic | X | X |
| Prior hospitalization (12 months) | X | X |
| Prior tracheostomy | X | |
| Demographic characteristics | ||
| Age (<30 years or >79 years) | X | |
| Male gender | X | |
| Enteral tube feeding | X | X |
| Residence in a nursing home | X | |
| Tobacco use | X | |
| Severity of illness | ||
| Severe CAP | X | |
| PaO2/FiO2 <200 | X | |
| Invasive respiratory or vasopressors support | X | |
| High serum levels of CRP | X | |
| PSI IV or V | X | X |
| Outstanding Research and Clinical Priorities | |
|---|---|
| 1 | Identification and implementation of antibiotic stewardship strategies at a local level, such as prospective audits with intervention and feedback, clinical pathways, and dedicated multidisciplinary teams. |
| 2 | Collection of data concerning the local prevalence of DRP to find stronger locally validated risk factors. |
| 3 | Validation of ATS/IDSA criteria in case of absence of a local database. |
| 4 | Identification of new, rapid, cost-effective, sensitive, and specific diagnostic tests for DRP. |
| 5 | Implementation of new diagnostic strategy in low-income and middle-income countries. |
| 6 | Identification of non-antibiotic drugs (such as bacteriophages) targeting DRP for effective treatment in vivo. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Amati, F.; Bindo, F.; Stainer, A.; Gramegna, A.; Mantero, M.; Nigro, M.; Bussini, L.; Bartoletti, M.; Blasi, F.; Aliberti, S. Identify Drug-Resistant Pathogens in Patients with Community-Acquired Pneumonia. Adv. Respir. Med. 2023, 91, 224-238. https://doi.org/10.3390/arm91030018
Amati F, Bindo F, Stainer A, Gramegna A, Mantero M, Nigro M, Bussini L, Bartoletti M, Blasi F, Aliberti S. Identify Drug-Resistant Pathogens in Patients with Community-Acquired Pneumonia. Advances in Respiratory Medicine. 2023; 91(3):224-238. https://doi.org/10.3390/arm91030018
Chicago/Turabian StyleAmati, Francesco, Francesco Bindo, Anna Stainer, Andrea Gramegna, Marco Mantero, Mattia Nigro, Linda Bussini, Michele Bartoletti, Francesco Blasi, and Stefano Aliberti. 2023. "Identify Drug-Resistant Pathogens in Patients with Community-Acquired Pneumonia" Advances in Respiratory Medicine 91, no. 3: 224-238. https://doi.org/10.3390/arm91030018