Climate Change and Respiratory Diseases: Relationship between SARS and Climatic Parameters and Impact of Climate Change on the Geographical Distribution of SARS in Iran

 ,
, 
Abstract
:Highlights
- This is the first study on the effects of climate change on SARS in Iran.
- The result shows a positive association between the incidence of SARS and bio-climatic variables.
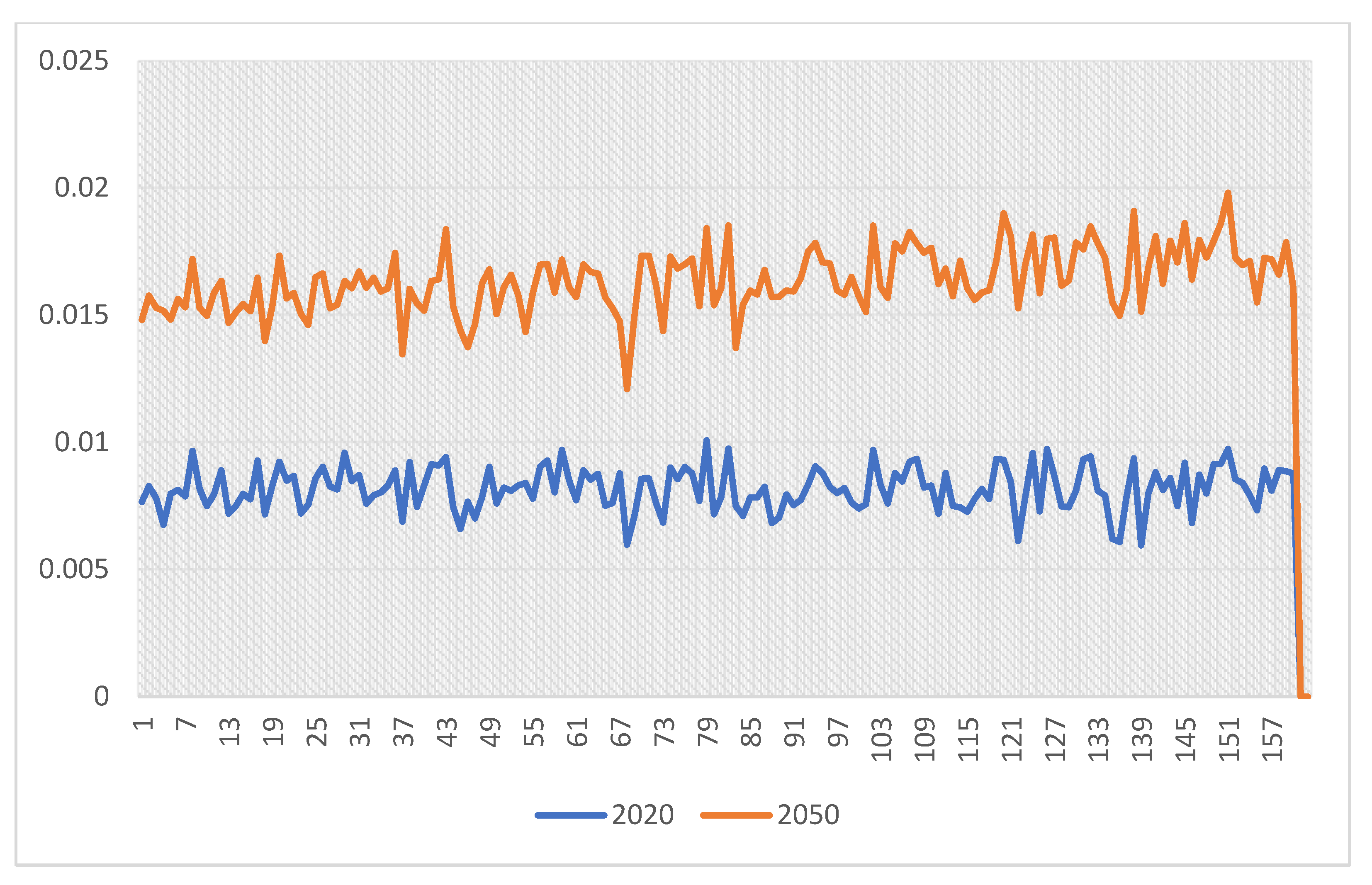
- This study shows the hospital admissions for climate-related respiratory diseases in Iran will increase by 36% in 2020–2050.
- The geographical distribution of the SARS will also change in 2050 in Iran.
Abstract
1. Introduction
2. Methods
3. Results
3.1. Gender-Based Results
3.2. Results Based on Climate
3.2.1. Semi-Arid Cold Climate (BSK)
3.2.2. Arid-Hot Climate (BWH)
3.2.3. Humid, Hot, and Temperate Oceanic Climate (Doa)
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Analitis, A.; Michelozzi, P.; D’Ippoliti, D.; de’Donato, F.; Menne, B.; Matthies, F.; Atkinson, R.W.; Iñiguez, C.; Basagaña, X.; Schneider, A. Effects of heat waves on mortality: Effect modification and confounding by air pollutants. Epidemiology 2014, 25, 15–22. [Google Scholar] [CrossRef] [PubMed]
- Baccini, M.; Biggeri, A.; Accetta, G.; Kosatsky, T.; Katsouyanni, K.; Analitis, A.; Anderson, H.R.; Bisanti, L.; D’ippoliti, D.; Danova, J. Heat effects on mortality in 15 European cities. Epidemiology 2008, 19, 711–719. [Google Scholar] [CrossRef] [PubMed]
- Checkley, W.; Epstein, L.D.; Gilman, R.H.; Figueroa, D.; Cama, R.I.; Patz, J.A.; Black, R.E. Effect of El Nino and ambient temperature on hospital admissions for diarrhoeal diseases in Peruvian children. Lancet 2000, 355, 442–450. [Google Scholar] [CrossRef]
- Curriero, F.C.; Patz, J.A.; Rose, J.B.; Lele, S. The association between extreme precipitation and waterborne disease outbreaks in the United States, 1948-1994. Am. J. Public Health 2001, 91, 1194–1199. [Google Scholar] [CrossRef] [PubMed]
- Eisenberg, J.N.; Desai, M.A.; Levy, K.; Bates, S.J.; Liang, S.; Naumoff, K.; Scott, J.C. Environmental determinants of infectious disease: A framework for tracking causal links and guiding public health research. Environ. Health Perspect. 2007, 115, 1216–1223. [Google Scholar] [CrossRef] [PubMed]
- Khader, Y.S.; Abdelrahman, M.; Abdo, N.; Al-Sharif, M.; Elbetieha, A.; Bakir, H.; Alemam, R. Climate change and health in the Eastern Mediterranean countries: A systematic review. Rev. Environ. Health 2015, 30, 163–181. [Google Scholar] [CrossRef]
- Li, C.L.; Lu, Y.M.; Liu, J.N.; Wu, X.X. Climate change and dengue fever transmission in China: Evidences and challenges. Sci. Total Environ. 2018, 622, 493–501. [Google Scholar] [CrossRef]
- Naumova, E.N.; Jagai, J.S.; Matyas, B.; DeMaria, A., Jr.; MacNeill, I.B.; Griffiths, J.K. Seasonality in six enterically transmitted diseases and ambient temperature. Epidemiol. Infect. 2007, 135, 281–292. [Google Scholar] [CrossRef]
- Pachauri, R.K.; Allen, M.R.; Barros, V.R.; Broome, J.; Cramer, W.; Christ, R.; Church, J.A.; Clarke, L.; Dahe, Q.; Dasgupta, P. Climate Change 2014: Synthesis Report. Contribution of Working Groups I, II and III to the Fifth Assessment Report of the Intergovernmental Panel on Climate Change; IPCC: Geneva, Switzerland, 2014. [Google Scholar]
- Parry, M.L. Assessing the Costs of Adaptation to Climate Change: A Review of the UNFCCC and Other Recent Estimates; IIED: London, UK, 2009. [Google Scholar]
- Watts, N.; Adger, W.N.; Ayeb-Karlsson, S.; Bai, Y.; Byass, P.; Campbell-Lendrum, D.; Colbourn, T.; Cox, P.; Davies, M.; Depledge, M.; et al. The Lancet Countdown: Tracking progress on health and climate change. Lancet 2017, 389, 1151–1164. [Google Scholar] [CrossRef]
- Woodward, A.; Smith, K.R.; Campbell-Lendrum, D.; Chadee, D.D.; Honda, Y.; Liu, Q.; Olwoch, J.; Revich, B.; Sauerborn, R.; Chafe, Z.; et al. Climate change and health: On the latest IPCC report. Lancet 2014, 383, 1185–1189. [Google Scholar] [CrossRef]
- Wu, X.; Lu, Y.; Zhou, S.; Chen, L.; Xu, B. Impact of climate change on human infectious diseases: Empirical evidence and human adaptation. Environ. Int. 2016, 86, 14–23. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.; Liu, Z.; Zhang, Y.; Jiang, B. Quantitative analysis of burden of bacillary dysentery associated with floods in Hunan, China. Sci. Total Environ. 2016, 547, 190–196. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.; Liu, Z.; Zhang, Y.; Jiang, B. The Effects of Floods on the Incidence of Bacillary Dysentery in Baise (Guangxi Province, China) from 2004 to 2012. Int. J. Environ. Res. Public Health 2017, 14, 179. [Google Scholar] [CrossRef] [PubMed]
- Ni, W.; Ding, G.; Li, Y.; Li, H.; Jiang, B. Impacts of floods on dysentery in Xinxiang city, China, during 2004-2010: A time-series Poisson analysis. Glob. Health Action 2014, 7, 23904. [Google Scholar] [CrossRef] [PubMed]
- Watson, J.T.; Gayer, M.; Connolly, M.A. Epidemics after natural disasters. Emerg. Infect. Dis. 2007, 13, 1–5. [Google Scholar] [CrossRef]
- Zhang, F.; Ding, G.; Liu, Z.; Zhang, C.; Jiang, B. Association between flood and the morbidity of bacillary dysentery in Zibo City, China: A symmetric bidirectional case-crossover study. Int. J. Biometeorol. 2016, 60, 1919–1924. [Google Scholar] [CrossRef]
- Vicedo-Cabrera, A.M.; Scovronick, N.; Sera, F.; Royé, D.; Schneider, R.; Tobias, A.; Astrom, C.; Guo, Y.; Honda, Y.; Hondula, D. The burden of heat-related mortality attributable to recent human-induced climate change. Nat. Clim. Chang. 2021, 11, 492–500. [Google Scholar] [CrossRef] [PubMed]
- Mathers, C.; Fat, D.; Boerma, J. The Global Burden of Disease: 2004 Update; World Health Organization: Geneva, Switzerland, 2008. [Google Scholar]
- Anderson, B.G.; Bell, M.L. Weather-related mortality: How heat, cold, and heat waves affect mortality in the United States. Epidemiol. 2009, 20, 205. [Google Scholar] [CrossRef]
- Chapman, K.; Mannino, D.; Soriano, J.; Vermeire, P.; Buist, A.S.; Thun, M.; Connell, C.; Jemal, A.; Lee, T.; Miravitlles, M. Epidemiology and costs of chronic obstructive pulmonary disease. Eur. Respir. J. 2006, 27, 188–207. [Google Scholar] [CrossRef]
- Anderson, G.B.; Dominici, F.; Wang, Y.; McCormack, M.C.; Bell, M.L.; Peng, R.D. Heat-related emergency hospitalizations for respiratory diseases in the Medicare population. Am. J. Respir. Crit. Care Med. 2013, 187, 1098–1103. [Google Scholar] [CrossRef] [Green Version]
- Thompson, A.A.; Matamale, L.; Kharidza, S.D. Impact of climate change on children’s health in Limpopo Province, South Africa. Int. J. Environ. Res. Public Health 2012, 9, 831–854. [Google Scholar] [CrossRef] [PubMed]
- Silva, D.R.; Viana, V.P.; Müller, A.M.; Livi, F.P.; Dalcin, P.D.T.R. Respiratory viral infections and effects of meteorological parameters and air pollution in adults with respiratory symptoms admitted to the emergency room. Influenza Other Respir. Viruses 2014, 8, 42–52. [Google Scholar] [CrossRef] [PubMed]
- Davis, R.E.; Dougherty, E.; McArthur, C.; Huang, Q.S.; Baker, M.G. Cold, dry air is associated with influenza and pneumonia mortality in Auckland, New Zealand. Influenza Other Respir. Viruses 2016, 10, 310–313. [Google Scholar] [CrossRef] [PubMed]
- Zhang, A.; Hu, W.; Li, J.; Wei, R.; Lin, J.; Ma, W. Impact of heatwaves on daily outpatient visits of respiratory disease: A time-stratified case-crossover study. Environ. Res. 2019, 169, 196–205. [Google Scholar] [CrossRef] [PubMed]
- Wichmann, J.; Andersen, Z.; Ketzel, M.; Ellermann, T.; Loft, S. Apparent temperature and cause-specific emergency hospital admissions in Greater Copenhagen, Denmark. PLoS ONE 2011, 6, e22904. [Google Scholar] [CrossRef]
- Gouya, M.; Rezaei, F.; Haghdoost, A.; Nabavi, M.; Farahi, K.S.; Mostafavi, E.; Azad, T.M.; Akbari, H.; Soroush, M.; Riazi, H. Estimation of influenza and severe acute respiratory illness incidence [burden] in three provinces of the Islamic Republic of Iran, 2012 and 2013. East. Mediterr. Health J. 2016, 22, 432–439. [Google Scholar] [CrossRef]
- Mansouri, A.; Aminnejad, B.; Ahmadi, H. Investigating the Effect of Climate Change on Inflow Runoff into the Karun-4 Dam Based on IPCC’s Fourth and Fifth Report. J. Water Soil Sci. 2018, 22, 345–359. [Google Scholar] [CrossRef]
- Climate Change and Health. Country Profile—2015 United Kingdom; WHO: Geneva, Switzerland, 2015. [Google Scholar]
- Bahrami, G.; Noroozi, M.; Shakiba, A.; Rafiey, H.; Sajjadi, H. The relationship between dysentery and climatic parameters in Iran. Urban Clim. 2020, 34, 100697. [Google Scholar] [CrossRef]
- Derakhshandeh, K.; Hamedi, Z.; Karimi, M.; Amiri, M.; Ahmadi, F. Formulation optimization of low bioavailable drug loaded alginate microparticles using artificial neural networks. J. Rep. Pharm. Sci 2012, 1, 41–51. [Google Scholar]
- Celik, A.N.; Kolhe, M. Generalized feed-forward based method for wind energy prediction. Appl. Energy 2013, 101, 582–588. [Google Scholar] [CrossRef]
- Chai, T.; Draxler, R.R. Root mean square error (RMSE) or mean absolute error (MAE)?—Arguments against avoiding RMSE in the literature. Geosci. Model Dev. 2014, 7, 1247–1250. [Google Scholar] [CrossRef] [Green Version]
- Moriyama, M.; Hugentobler, W.J.; Iwasaki, A. Seasonality of respiratory viral infections. Annu. Rev. Virol. 2020, 7, 83–101. [Google Scholar] [CrossRef] [PubMed]
- Alessandrini, E.; Sajani, S.Z.; Scotto, F.; Miglio, R.; Marchesi, S.; Lauriola, P. Emergency ambulance dispatches and apparent temperature: A time series analysis in Emilia–Romagna, Italy. Environ. Res. 2011, 111, 1192–1200. [Google Scholar] [CrossRef]
- Bambrick, H.; Dear, K.; Woodruff, R.; Hanigan, I.; McMichael, A. The Impacts of Climate Change on Three Health Outcomes: Temperature-Related Mortality and Hospitalisations, Salmonellosis and Other Bacterial Gastroenteritis, and Population at Risk from Dengue; Garnaut Climate Change Review: Canberra, Australia, 2008. [Google Scholar]
- Peng, R.D.; Bobb, J.F.; Tebaldi, C.; McDaniel, L.; Bell, M.L.; Dominici, F. Toward a quantitative estimate of future heat wave mortality under global climate change. Environ. Health Perspect. 2011, 119, 701–706. [Google Scholar] [CrossRef] [PubMed]
- Dessai, S. Heat stress and mortality in Lisbon Part II. An assessment of the potential impacts of climate change. Int. J. Biometeorol. 2003, 48, 37–44. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
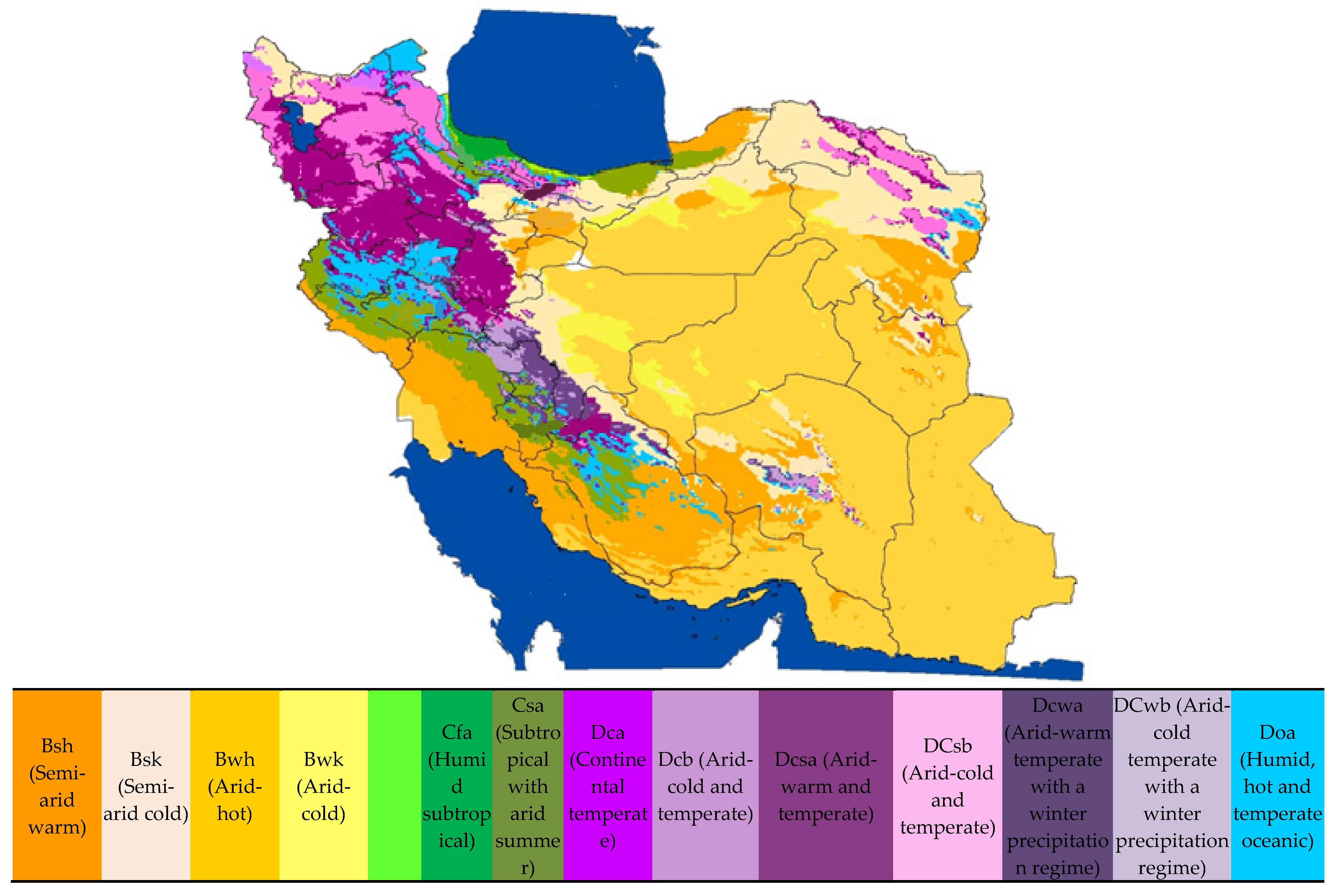
| Description of Climate Type in Iran Name of Climate Type | Type of Climate Based on Köppen | Code of Climate in This Study (Based of Köppen) | Percentage of This Climate Type in Iran Base Classification in 2000 | Percentage of SARS Distribution in Iran between 2016–2018 |
|---|---|---|---|---|
| Semi-arid warm | BSh | 211 | 14.24 | 24.85 |
| Semi-arid cold | BSk | 212 | 12.82 | 22.15 |
| Arid-hot | BWh | 221 | 43.30 | 12.23 |
| Arid-cold | BWk | 222 | 2.58 | 6.76 |
| Humid subtropical | Cfa | 311 | 0.40 | 2.87 |
| Subtropical with arid summer | Csa | 331 | 5.36 | 5.22 |
| Continental temperate | Dca | 411 | 0.06 | - |
| Arid-warm and temperate | Dcsa | 421 | 8.01 | 11.34 |
| Arid-cold and temperate | Dcsb | 422 | 5.10 | 0.99 |
| Humid, hot and temperate oceanic | Doa | 451 | 4.33 | 9.19 |
| Arid-warm temperate with a winter precipitation regime | Dcwa | 431 | 1.95 | 4.04 |
| Arid-cold temperate with a winter precipitation regime | Dcwb | 432 | 1.22 | - |
| Time Span | Sampling Frequency | Variable |
|---|---|---|
| 17 February 2016–17 February 2018 | daily | Maximum temperature |
| 17 February 2016–17 February 2018 | daily | Minimum temperature |
| 17 February 2016–17 February 2018 | daily | Precipitation |
| 17 February 2016–17 February 2018 | daily | Incidence of SRRS In women |
| 17 February 2016–17 February 2018 | daily |
| Model Statistics | Exper. | Project |
|---|---|---|
| Data Set | Optim. | Leave-N-Out |
| Score | 60/172 | 42/512 |
| Avg. Correlation | 0/340 | 0/000 |
| Avg. Norm. MSE | 0/233 | 0/278 |
| Avg. Norm. MAE | 0/172 | 0/206 |
| Max. Abs. Error | 0/026 | 0/030 |
| Training Epochs | 57 | |
| Training Seconds | 1 |
| Variable | Women | Men | ||||
|---|---|---|---|---|---|---|
| IRR | p Value | 95% CI | IRR | p Value | 95% CI | |
| t min °C | 0.99 | 0.169 | 0.98–1.00 | 0.98 | <0.000 | 0.98–0.99 |
| t max °C | 1.00 | 0.716 | 0.99–1.00 | 1.00 | 0.549 | 0.99–1.00 |
| rrr24 a mL | 1.00 | 0.539 | 0.99–1.00 | 0.99 | 0.060 | 0.98–1.00 |
| Type of Climate | Variable | Women | Men | ||||
|---|---|---|---|---|---|---|---|
| IRR | p Value | 95% CI | IRR | p Value | 95% CI | ||
| Csa | t max | 1.00 | 0.373 | 0.98–1.03 | 1.02 | 0.075 | 0.99–1.04 |
| BWk | t min | 1.01 | 0.117 | 0.99–1.04 | 1.01 | 0.127 | 0.99–1.03 |
| BWk | rrr24 | 0.74 | 0.075 | 0.53–1.03 | 0.61 | 0.030 | 0.39–0.95 |
| BSk | t min | 1.01 | 0.004 | 1.00–1.02 | 1.01 | 0.010 | 1.00–1.03 |
| BSk | rrr24 | 1.02 | 0.000 | 1.00–1.05 | 1.03 | 0.003 | 1.01–1.05 |
| BWh | T min | 0.98 | 0.136 | 0.97–1.00 | 0.97 | 0.005 | 0.95–0.99 |
| BWh | T max | 0.98 | 0.046 | 0.97–0.99 | 0.99 | 0.289 | 0.97–1.00 |
| BSh | t min | 0.98 | 0.059 | 0.97–1.00 | 0.98 | 0.001 | 0.97–0.99 |
| Dcsa | t min | 1.01 | 0.126 | 0.99–1.03 | 1.02 | 0.071 | 0.99–1.04 |
| Dcsa | t max | 1.00 | 0.257 | 0.99–1.02 | 0.98 | 0.078 | 0.96–1.00 |
| Doa | t max | 0.98 | 0.038 | 0.96–0.99 | 0.96 | <0.000 | 0.95–0.98 |
| Doa | rrr24 | 0.99 | 0.642 | 0.97–1.01 | 0.95 | 0.009 | 0.92–0.98 |
| Dcwa | t min | 0.98 | 0.261 | 0.95–1.01 | 0.95 | 0.001 | 0.93–0.98 |
| Dcwa | t max | 0.98 | 0.381 | 0.95–1.01 | 0.99 | 0.973 | 0.97–1.02 |
| Dcwa | rrr24 | 1.00 | 0.901 | 0.96–1.03 | 0.97 | 0.286 | 0.92–1.02 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bahrami, G.; Rafiey, H.; Shakiba, A.; Noroozi, M.; Sajjadi, H.; Seddighi, H. Climate Change and Respiratory Diseases: Relationship between SARS and Climatic Parameters and Impact of Climate Change on the Geographical Distribution of SARS in Iran. Adv. Respir. Med. 2022, 90, 378-390. https://doi.org/10.3390/arm90050048
Bahrami G, Rafiey H, Shakiba A, Noroozi M, Sajjadi H, Seddighi H. Climate Change and Respiratory Diseases: Relationship between SARS and Climatic Parameters and Impact of Climate Change on the Geographical Distribution of SARS in Iran. Advances in Respiratory Medicine. 2022; 90(5):378-390. https://doi.org/10.3390/arm90050048
Chicago/Turabian StyleBahrami, Giti, Hassan Rafiey, Alireza Shakiba, Mehdi Noroozi, Homeira Sajjadi, and Hamed Seddighi. 2022. "Climate Change and Respiratory Diseases: Relationship between SARS and Climatic Parameters and Impact of Climate Change on the Geographical Distribution of SARS in Iran" Advances in Respiratory Medicine 90, no. 5: 378-390. https://doi.org/10.3390/arm90050048