
Adipolin and IL-6 Serum Levels in Chronic Obstructive Pulmonary Disease

Abstract
:Highlights
- This study showed reduced adipolin serum levels as a pro-inflammatory molecule in COPD patients.
- Serum adipolin levels correlate with serum levels of IL-6, exercise capacity (based on mMRC dyspnea score), and quality of life (based on CAT score).
- Imbalance in the serum levels of pro-inflammatory and anti-inflammatory markers in COPD patients.
- Correlation between pro-inflammatory and anti-inflammatory markers with disease severity and quality of life in COPD patients.
Abstract
1. Introduction
2. Methods
Statistical Analysis
3. Results
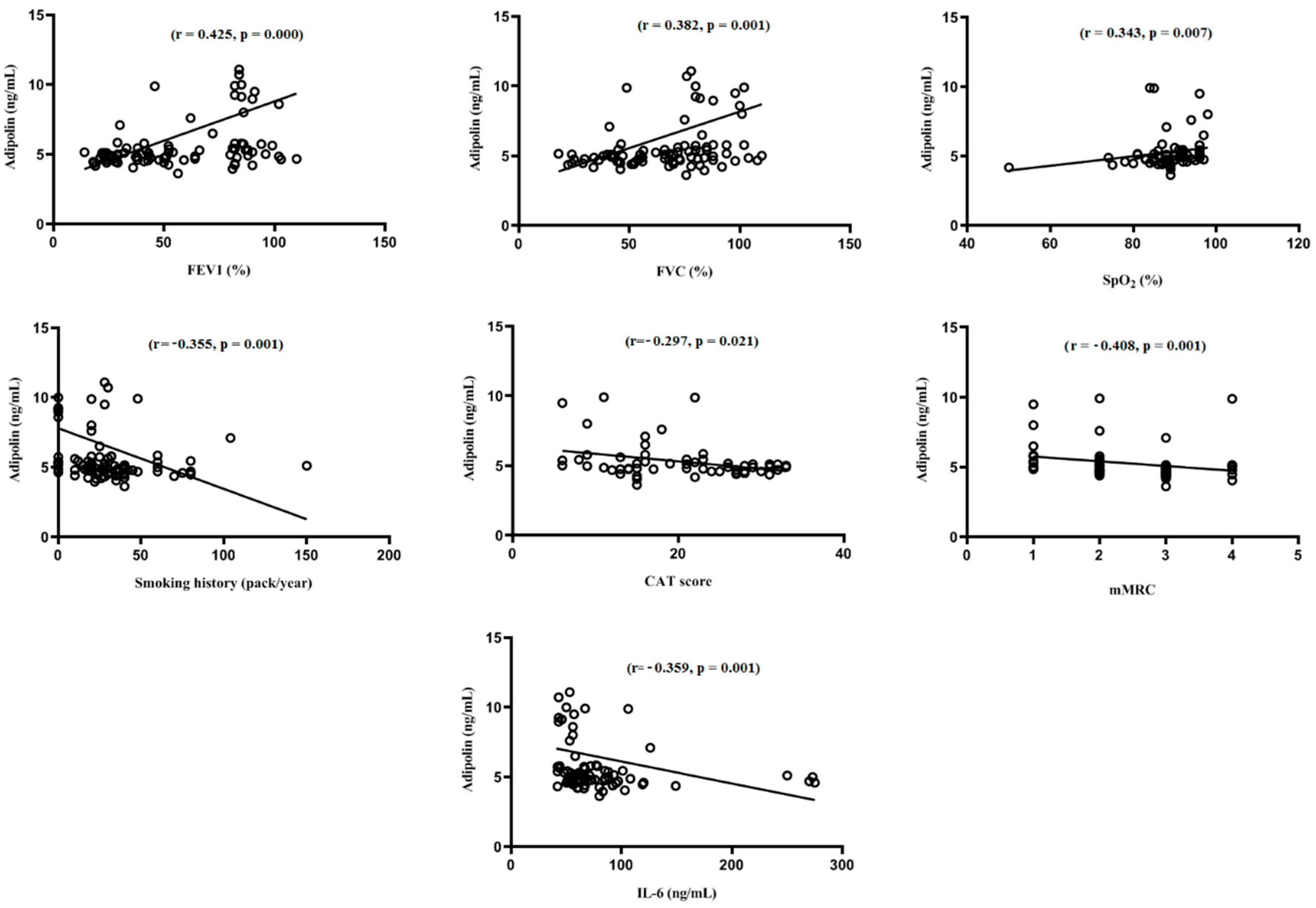
Relationship of Serum Levels of Adipolin and IL-6 with the Study Parameters
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Barnes, P.J. Inflammatory mechanisms in patients with chronic obstructive pulmonary disease. J. Allergy Clin. Immunol. 2016, 138, 16–27. [Google Scholar] [CrossRef] [PubMed]
- Barnes, P.J. Cellular and molecular mechanisms of asthma and COPD. Clin. Sci. 2017, 131, 1541–1558. [Google Scholar] [CrossRef] [PubMed]
- Ghobadi, H.; Mokhtari, S.; Aslani, M.R. Serum levels of visfatin sirtuin 1 and interleukin 6 in stable and acute exacerbation of chronic obstructive pulmonary disease. J. Res. Med. Sci. 2021, 26, 17. [Google Scholar] [PubMed]
- Moghoofei, M.; Jamalkandi, S.A.; Moein, M.; Salimian, J.; Ahmadi, A. Bacterial infections in acute exacerbation of chronic obstructive pulmonary disease: A systematic review and meta-analysis. Infection 2020, 48, 19–35. [Google Scholar] [CrossRef]
- Wouters, E.F.; Groenewegen, K.H.; Dentener, M.A.; Vernooy, J.H. Systemic inflammation in chronic obstructive pulmonary disease: The role of exacerbations. Proc. Am. Thorac. Soc. 2007, 4, 626–634. [Google Scholar] [CrossRef] [PubMed]
- Aslani, M.R.; Ghobadi, H.; Panahpour, H.; Ahmadi, M.; Khaksar, M.; Heidarzadeh, M. Modification of lung endoplasmic reticulum genes expression and NF-kB protein levels in obese ovalbumin-sensitized male and female rats. Life Sci. 2020, 247, 117446. [Google Scholar] [CrossRef]
- Aslani, M.R.; Sharghi, A.; Boskabady, M.H.; Ghobadi, H.; Keyhanmanesh, R.; Alipour, M.R.; Ahmadi, M.; Saadat, S.; Naghizadeh, P. Altered gene expression levels of IL-17/TRAF6/MAPK/USP25 axis and pro-inflammatory cytokine levels in lung tissue of obese ovalbumin-sensitized rats. Life Sci. 2022, 296, 120425. [Google Scholar] [CrossRef]
- Ouchi, N.; Parker, J.L.; Lugus, J.J.; Walsh, K. Adipokines in inflammation and metabolic disease. Nat. Rev. Immunol. 2011, 11, 85–97. [Google Scholar] [CrossRef]
- Withers, S.B.; Dewhurst, T.; Hammond, C.; Topham, C.H. MiRNAs as novel adipokines: Obesity-related circulating MiRNAs influence chemosensitivity in cancer patients. Non-Coding RNA 2020, 6, 5. [Google Scholar] [CrossRef] [PubMed]
- Withers, S.B.; Forman, R.; Meza-Perez, S.; Sorobetea, D.; Sitnik, K.; Hopwood, T.; Lawrence, C.B.; Agace, W.W.; Else, K.J.; Heagerty, A.M.; et al. Eosinophils are key regulators of perivascular adipose tissue and vascular functionality. Sci. Rep. 2017, 7, 44571. [Google Scholar] [CrossRef] [Green Version]
- Akhavanakbari, G.; Babapour, B.; Alipour, M.R.; Keyhanmanesh, R.; Ahmadi, M.; Aslani, M.R. Effect of high fat diet on NF-кB microRNA146a negative feedback loop in ovalbumin-sensitized rats. Biofactors 2019, 45, 75–84. [Google Scholar] [CrossRef] [PubMed]
- Aslani, M.R.; Ghazaei, Z.; Ghobadi, H. Correlation of serum fatty acid binding protein-4 and interleukin-6 with airflow limitation and quality of life in stable and acute exacerbation of COPD. Turk. J. Med. Sci. 2020, 50, 337–345. [Google Scholar] [CrossRef] [PubMed]
- Ghobadi, H.; Alipour, M.R.; Keyhanmanesh, R.; Boskabady, M.H.; Aslani, M.R. Effect of High-fat Diet on Tracheal Responsiveness to Methacholine and Insulin Resistance Index in Ovalbumin-sensitized Male and Female Rats. Iran J. Allergy Asthma Immunol. 2019, 18, 48–61. [Google Scholar] [CrossRef] [PubMed]
- Wong, G.W.; Wang, J.; Hug, C.; Tsao, T.-S.; Lodish, H.F. A family of Acrp30/adiponectin structural and functional paralogs. Proc. Natl. Acad. Sci. USA 2004, 101, 10302–10307. [Google Scholar] [CrossRef] [PubMed]
- Wei, Z.; Peterson, J.M.; Lei, X.; Cebotaru, L.; Wolfgang, M.J.; Baldeviano, G.C.; Wong, G.W. C1q/TNF-related protein-12 (CTRP12), a novel adipokine that improves insulin sensitivity and glycemic control in mouse models of obesity and diabetes. J. Biol. Chem. 2012, 287, 10301–10315. [Google Scholar] [CrossRef]
- Ohashi, K.; Shibata, R.; Murohara, T.; Ouchi, N. Role of anti-inflammatory adipokines in obesity-related diseases. Trends Endocrinol. Metab. 2014, 25, 348–355. [Google Scholar] [CrossRef] [PubMed]
- Babapour, B.; Doustkami, H.; Avesta, L.; Moradi, A.; Saadat, S.; Piralaei, K.; Aslani, M.R. Correlation of Serum Adipolin with Epicardial Fat Thickness and Severity of Coronary Artery Diseases in Acute Myocardial Infarction and Stable Angina Pectoris Patients. Med. Princ. Pr. 2020, 30, 52–61. [Google Scholar] [CrossRef]
- Fadaei, R.; Moradi, N.; Kazemi, T.; Chamani, E.; Azdaki, N.; Moezibady, S.A.; Shahmohamadnejad, S.; Fallah, S. Decreased serum levels of CTRP12/adipolin in patients with coronary artery disease in relation to inflammatory cytokines and insulin resistance. Cytokine 2018, 113, 326–331. [Google Scholar] [CrossRef]
- Tan, B.K.; Chen, J.; Hu, J.; Amar, O.; Mattu, H.S.; Ramanjaneya, M.; Patel, V.; Lehnert, H.; Randeva, H.S. Circulatory changes of the novel adipokine adipolin/CTRP 12 in response to metformin treatment and an oral glucose challenge in humans. Clin. Endocrinol. 2014, 81, 841–846. [Google Scholar] [CrossRef]
- Rodriguez-Roisin, R.; Rabe, K.F.; Vestbo, J.; Vogelmeier, C.; Agustí, A. Global Initiative for Chronic Obstructive Lung Disease (GOLD) 20th anniversary: A brief history of time. Eur. Respir. Soc. 2017, 50, 1700671. [Google Scholar] [CrossRef] [Green Version]
- Amani, M.; Ghadimi, N.; Aslani, M.R.; Ghobadi, H. Correlation of serum vascular adhesion protein-1 with airflow limitation and quality of life in stable chronic obstructive pulmonary disease. Respir. Med. 2017, 132, 149–153. [Google Scholar] [CrossRef] [PubMed]
- Emamgholipour, S.; Moradi, N.; Beigy, M.; Shabani, P.; Fadaei, R.; Poustchi, H.; Doosti, M. The association of circulating levels of complement-C1q TNF-related protein 5 (CTRP5) with nonalcoholic fatty liver disease and type 2 diabetes: A case–control study. Diabetol. Metab. Syndr. 2015, 7, 108. [Google Scholar] [CrossRef] [PubMed]
- Shanaki, M.; Fadaei, R.; Moradi, N.; Emamgholipour, S.; Poustchi, H. The circulating CTRP13 in type 2 diabetes and non-alcoholic fatty liver patients. PLoS ONE 2016, 11, e0168082. [Google Scholar] [CrossRef] [PubMed]
- Yuasa, D.; Ohashi, K.; Shibata, R.; Takeshita, K.; Kikuchi, R.; Takahashi, R.; Kataoka, Y.; Miyabe, M.; Joki, Y.; Kambara, T.; et al. Association of circulating C1q/TNF-related protein 1 levels with coronary artery disease in men. PLoS ONE 2014, 9, e99846. [Google Scholar]
- Enomoto, T.; Ohashi, K.; Shibata, R.; Higuchi, A.; Maruyama, S.; Izumiya, Y.; Walsh, K.; Murohara, T.; Ouchi, N. Adipolin/C1qdc2/CTRP12 protein functions as an adipokine that improves glucose metabolism. J. Biol. Chem. 2011, 286, 34552–34558. [Google Scholar] [CrossRef]
- Garcia, P.; Sood, A. Adiponectin in pulmonary disease and critically ill patients. Curr. Med. Chem. 2012, 19, 5493–5500. [Google Scholar] [CrossRef]
- Wolf, A.M.; Wolf, D.; Rumpold, H.; Enrich, B.; Tilg, H. Adiponectin induces the anti-inflammatory cytokines IL-10 and IL-1RA in human leukocytes. Biochem. Biophys. Res. Commun. 2004, 323, 630–635. [Google Scholar] [CrossRef]
- Masaki, T.; Chiba, S.; Tatsukawa, H.; Yasuda, T.; Noguchi, H.; Seike, M.; Yoshimatsu, H. Adiponectin protects LPS-induced liver injury through modulation of TNF-α in KK-Ay obese mice. Hepatology 2004, 40, 177–184. [Google Scholar] [CrossRef]
- Lin, Y.H.; Jiang, T.X.; Hu, S.X.; Shi, Y.H. Association between serum adiponectin concentrations and chronic obstructive pulmonary disease: A meta-analysis. Biosci. Rep. 2020, 40, 1–10. [Google Scholar] [CrossRef]
- Ghobadi, H.; Aslani, M.R.; Hosseinian, A.; Farzaneh, E. The Correlation of Serum Brain Natriuretic Peptide and Interleukin-6 with Quality of Life Using the Chronic Obstructive Pulmonary Disease Assessment Test. Med. Princ. Pract. 2017, 26, 509–515. [Google Scholar] [CrossRef]
- Cebron Lipovec, N.; Beijers, R.J.; van den Borst, B.; Doehner, W.; Lainscak, M.; Schols, A.M. The prevalence of metabolic syndrome in chronic obstructive pulmonary disease: A systematic review. COPD J. Chronic. Obstr. Pulm. Dis. 2016, 13, 399–406. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Parameters | Control Group (n = 30) | COPD Group (n = 60) | p-Value |
|---|---|---|---|
| Mean age (year) | 56.40 ± 6.29 | 58.92 ± 6.22 | 0.099 |
| Body mass index (kg/m2) | 26.73 ± 3.88 | 24.72 ± 4.79 | 0.051 |
| Smoking history (pack/year) | 13.03 ± 13.61 | 38.83 ± 25.34 | 0.000 |
| Pulmonary function test: | |||
| FEV1 (% of predicted) | 89.06 ± 7.60 | 43.82 ± 20.59 | 0.000 |
| FVC (% of predicted) | 85.50 ± 8.79 | 58.71 ± 22.42 | 0.000 |
| FEV1/FVC | 83.65 ± 5.89 | 59.43 ± 11.69 | 0.000 |
| Adipolin (ng/mL) | 8.88 ± 5.59 | 5.28 ± 1.28 | 0.001 |
| Adjusted adipolin | 8.89 ± 0.34 | 5.28 ± 0.61 | 0.000 |
| IL-6 (ng/mL) | 54.56 ± 10.47 | 87.71 ± 52.92 | 0.001 |
| Adjusted IL-6 | 52.22 ± 14.09 | 88.41 ± 30.86 | 0.000 |
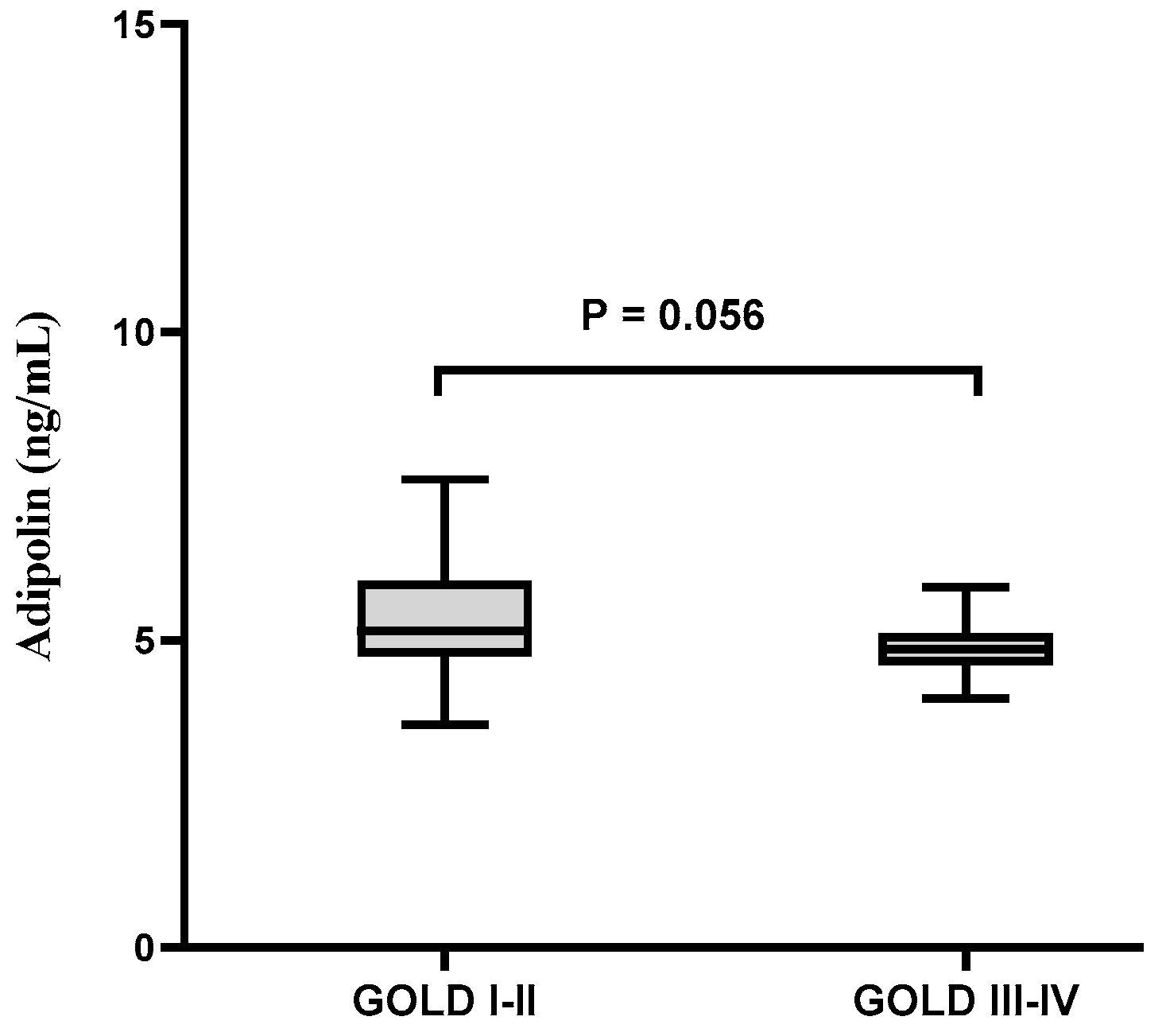
| Variables | GOLD I-II | GOLD III-IV | p-Value |
|---|---|---|---|
| Number | 22 | 38 | |
| Age (year) | 58.41 ± 6.55 | 59.21 ± 6.10 | 0.642 |
| BMI (kg/m2) | 24.53 ± 3.84 | 24.83 ± 5.31 | 0.817 |
| Smoking (pack per year) | 21 (20–40) | 38 (28–60) | 0.008 |
| CAT score | 13 (9–15) | 27 (22–29) | 0.000 |
| mMRC | 2 (1–2) | 3 (2–3) | 0.000 |
| IL-6 (ng/mL) | 62.81 ± 10.56 | 102.13 ± 61.82 | 0.005 |
| Adipolin (ng/mL) | 5.69 ± 1.63 | 5.04 ± 0.96 | 0.056 |
| Adipolin | |||
|---|---|---|---|
| B | 95% CI for B | p-Value | |
| FEV1 | 0.544 | 0.009–0.058 | 0.008 |
| cigarette history (pack/year) | 0.117 | −0.010–0.022 | 0.459 |
| IL-6 | 0.045 | −0.007–0.009 | 0.781 |
| CAT score | 0.031 | −0.056–0.066 | 0.873 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Aslani, M.R.; Amani, M.; Moghadas, F.; Ghobadi, H. Adipolin and IL-6 Serum Levels in Chronic Obstructive Pulmonary Disease. Adv. Respir. Med. 2022, 90, 391-398. https://doi.org/10.3390/arm90050049
Aslani MR, Amani M, Moghadas F, Ghobadi H. Adipolin and IL-6 Serum Levels in Chronic Obstructive Pulmonary Disease. Advances in Respiratory Medicine. 2022; 90(5):391-398. https://doi.org/10.3390/arm90050049
Chicago/Turabian StyleAslani, Mohammad Reza, Mojtaba Amani, Faranak Moghadas, and Hassan Ghobadi. 2022. "Adipolin and IL-6 Serum Levels in Chronic Obstructive Pulmonary Disease" Advances in Respiratory Medicine 90, no. 5: 391-398. https://doi.org/10.3390/arm90050049