
Association between Influenza and COVID-19 Viruses and the Risk of Atherosclerosis: Meta-Analysis Study and Systematic Review

Abstract
:Highlights
- Atherosclerosis is an important issue in health care systems and one of the main causes of morbidity and mortality in patients.
- There is evidence of an association between infectious diseases and atherosclerosis.
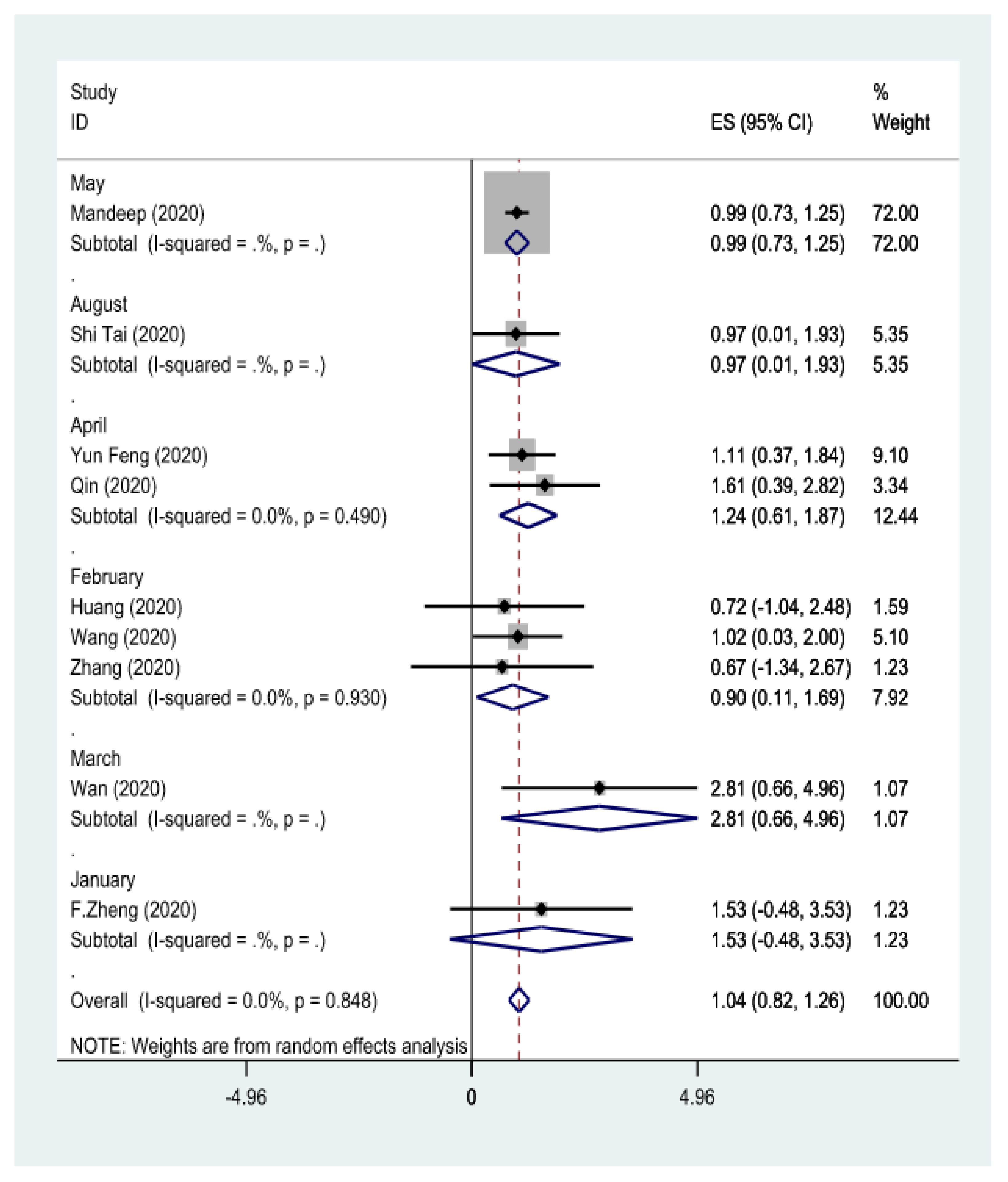
- The present study demonstrates that infections with influenza and COVID-19 are risk factors for arthrosclerosis.
- It seems necessary to consider different strategies for managing and eradicating viral infections.
Abstract
1. Introduction
2. Methods
2.1. Study Instructions
2.2. Eligibility Criteria and Information Sources
2.3. Search Strategy
2.4. Quality of Evaluation
2.5. Included and Excluded Studies
2.6. Study Selection
2.7. Information Extraction
2.8. Statistical Analysis
3. Results
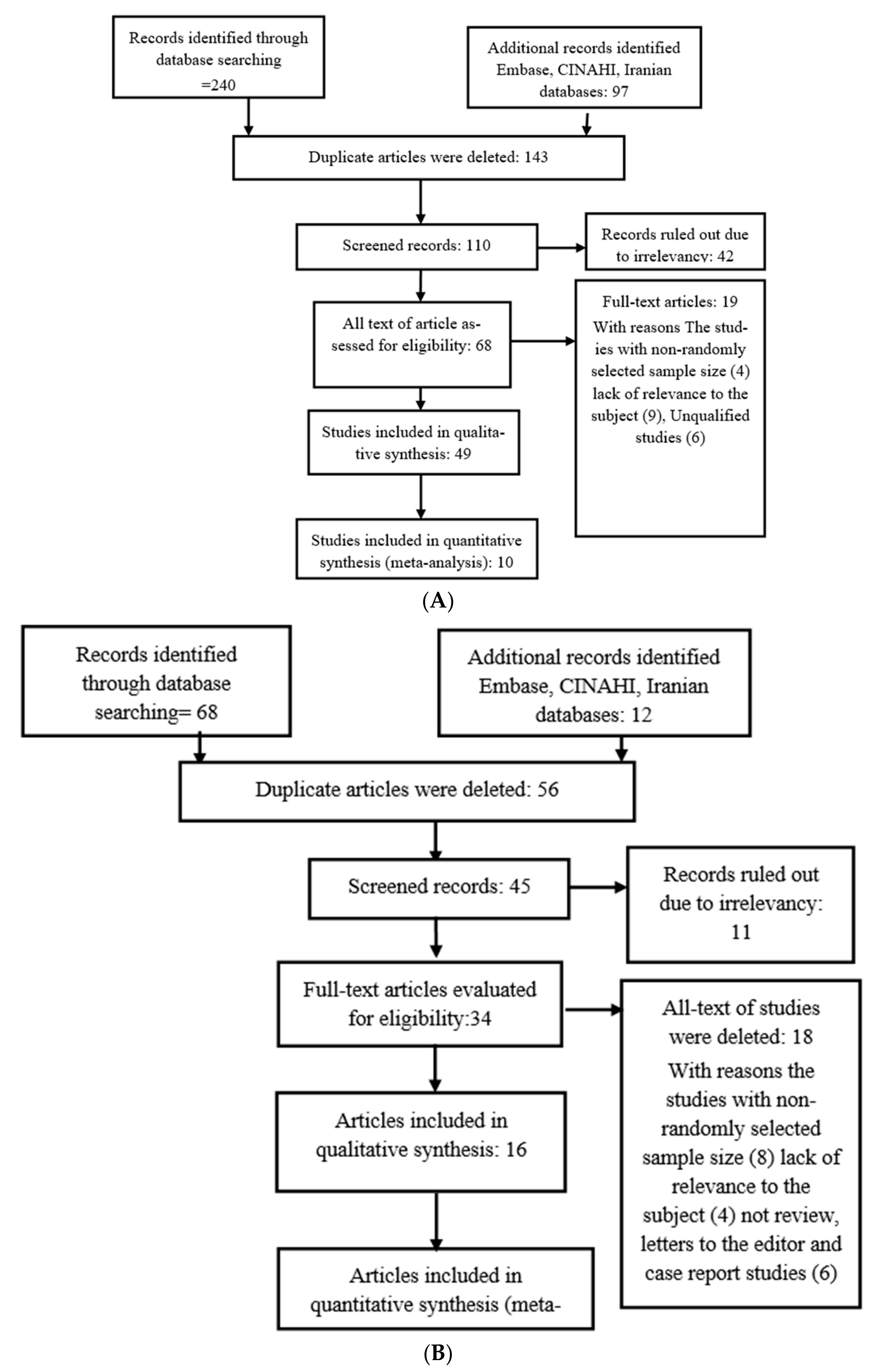
3.1. Search for Studies
3.2. Article Exclusivities
3.3. Risk of Bias in Articles
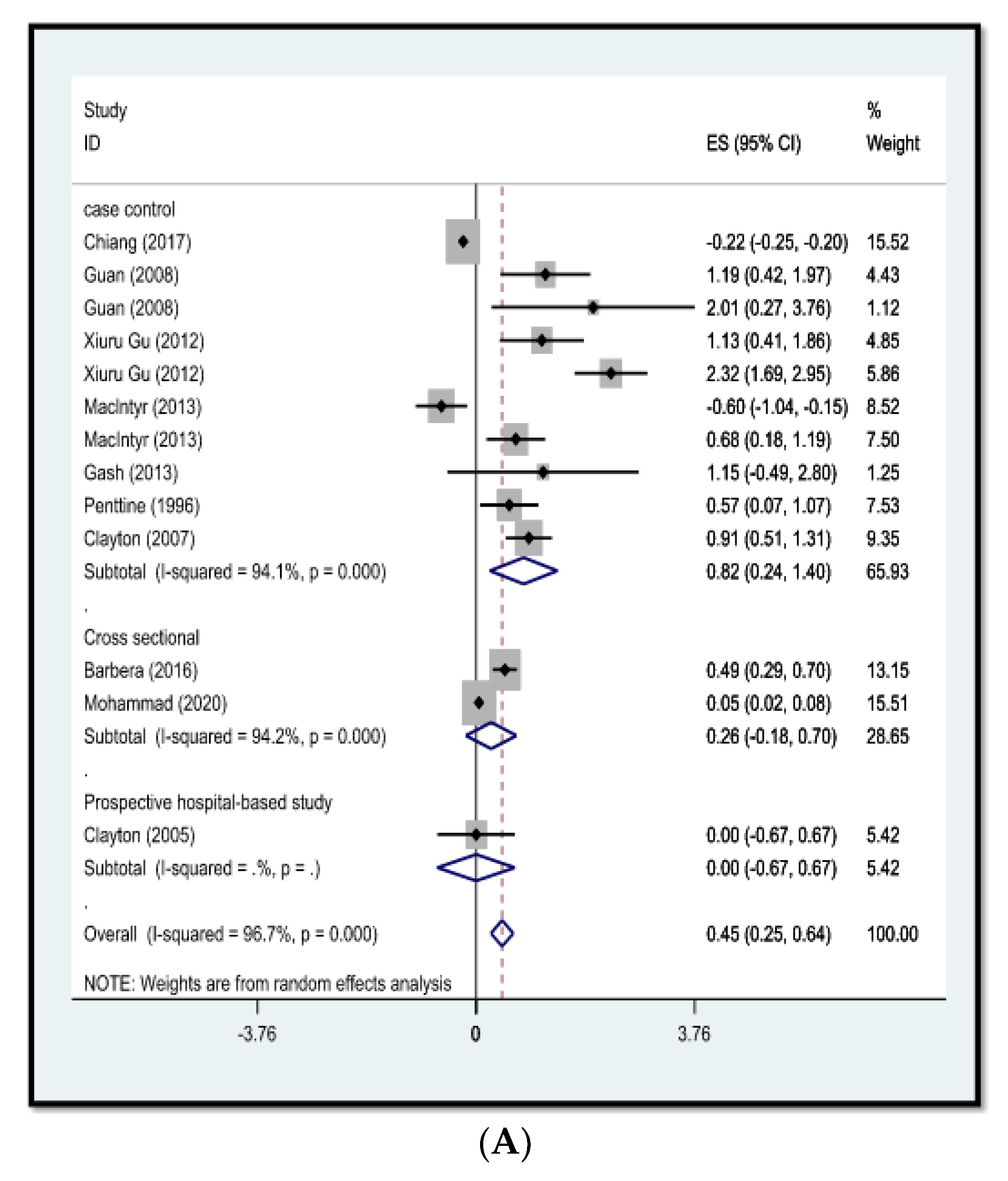
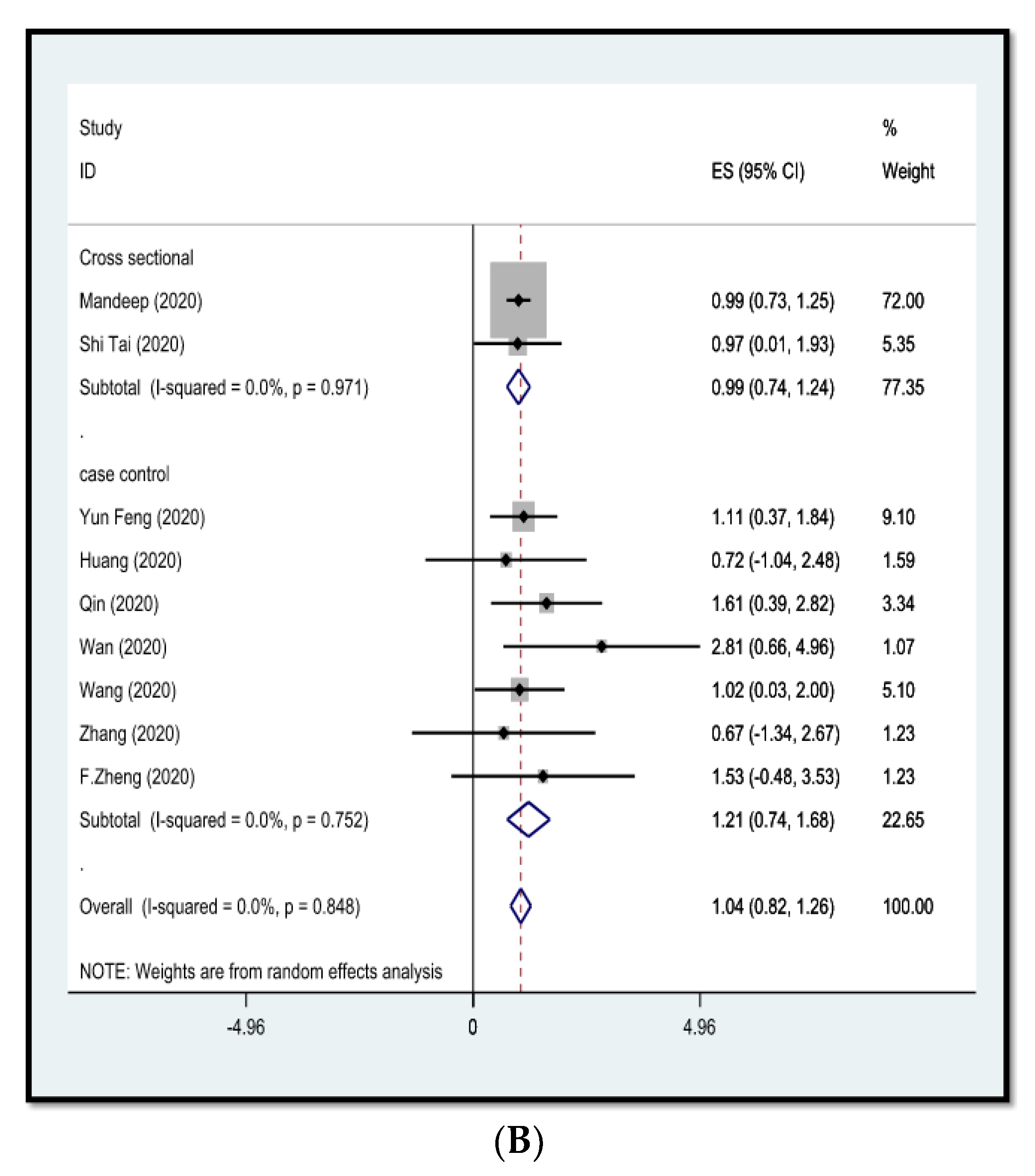
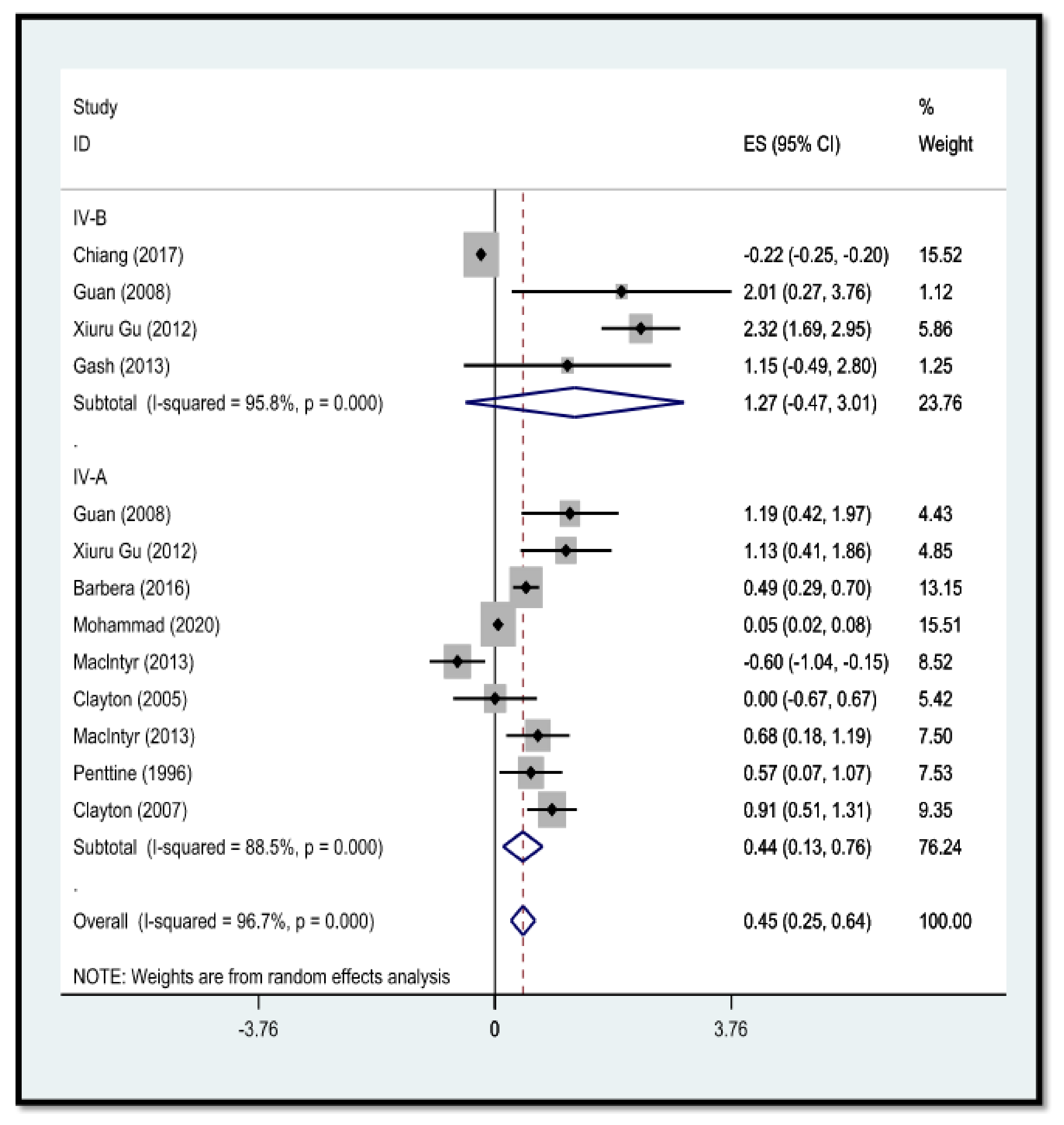
3.4. Outcome of Articles
3.5. Evaluation of Outcome
3.6. Additional Outcome
4. Discussion
Consolidation of Evidence
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Jalili, M.; Ansari, N.; Pourhossein, B.; Fazeli, M.; Jalilian, F.A. An Overview of Antiviral Properties of Bacteriophages with Emphasis on the Treatment of COVID-19 Infection. Infect. Disord. Drug Targets 2022, 22, e240122200472. [Google Scholar] [CrossRef] [PubMed]
- Mannino, D.M.; Doherty, D.E.; Buist, A.S. Global Initiative on Obstructive Lung Disease (GOLD) classification of lung disease and mortality: Findings from the Atherosclerosis Risk in Communities (ARIC) study. Respir. Med. 2006, 100, 115–122. [Google Scholar] [CrossRef] [PubMed]
- Jalili, M.; Nourmohammadi, H.; Sayehmiri, K. Chlamydia pneumoniae and Mycoplasma pneumoniae as two Emerging Risk Factors in Atherosclerosis: Meta-Analysis Study and Systematic Review. Infect. Disord. Drug Targets 2021, 22, 74–83. [Google Scholar] [CrossRef] [PubMed]
- Bonnet, F.; Irving, K.; Terra, J.-L.; Nony, P.; Berthezène, F.; Moulin, P. Anxiety and depression are associated with unhealthy lifestyle in patients at risk of cardiovascular disease. Atherosclerosis 2005, 178, 339–344. [Google Scholar] [CrossRef] [PubMed]
- Campbell, L.A.; Rosenfeld, M.E. Infection and atherosclerosis development. Arch. Med. Res. 2015, 46, 339–350. [Google Scholar] [CrossRef] [PubMed]
- Rosenfeld, M.E.; Campbell, L.A. Pathogens and atherosclerosis: Update on the potential contribution of multiple infectious organisms to the pathogenesis of atherosclerosis. Thromb. Haemost. 2011, 106, 858–867. [Google Scholar] [PubMed]
- Qin, C.; Zhou, L.; Hu, Z.; Zhang, S.; Yang, S.; Tao, Y.; Xie, C.; Ma, K.; Shang, K.; Wang, W.; et al. Dysregulation of immune response in patients with coronavirus 2019 (COVID-19) in Wuhan, China. Clin. Infect. Dis. 2020, 71, 762–768. [Google Scholar] [CrossRef] [PubMed]
- Wan, S.; Xiang, Y.I.; Fang, W.; Zheng, Y.; Li, B.; Hu, Y.; Yang, R. Clinical features and treatment of COVID-19 patients in northeast Chongqing. J. Med. Virol. 2020, 92, 797–806. [Google Scholar] [CrossRef] [PubMed]
- Wang, D.; Hu, B.; Hu, C.; Zhu, F.; Liu, X.; Zhang, J.; Peng, Z. Clinical characteristics of 138 hospitalized patients with 2019 novel coronavirus–infected pneumonia in Wuhan, China. JAMA 2020, 323, 1061–1069. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.J.; Dong, X.; Cao, Y.Y.; Yuan, Y.D.; Yang, Y.B.; Yan, Y.Q.; Gao, Y.D. Clinical characteristics of 140 patients infected with SARS-CoV-2 in Wuhan, China. Allergy 2020, 75, 1730–1741. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef]
- DerSimonian, R.; Laird, N. Meta-analysis in clinical trials. Control. Clin. Trials 1986, 7, 177–188. [Google Scholar] [CrossRef]
- Chiang, M.H.; Wu, H.H.; Shih, C.J.; Chen, Y.T.; Kuo, S.C.; Chen, T.L. Association between influenza vaccination and reduced risks of major adverse cardiovascular events in elderly patients. Am. Heart J. 2017, 193, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Guan, X.R.; Li, X.; Xin, X.M.; Jiang, L.X.; Cui, L.Y.; Wang, L.F.; Li, H.Y. Influenza virus infection and risk of acute myocardial infarction. Inflammation 2008, 31, 266–272. [Google Scholar] [CrossRef]
- Guan, X.; Yang, W.; Sun, X.; Wang, L.; Ma, B.; Li, H.; Zhou, J. Association of influenza virus infection and inflammatory cytokines with acute myocardial infarction. Inflamm. Res. 2012, 61, 591–598. [Google Scholar] [CrossRef] [PubMed]
- Puig-Barbera, J.; Natividad-Sancho, A.; Trushakova, S.; Sominina, A.; Pisareva, M.; Ciblak, M.A. Epidemiology of hospital admissions with influenza during the 2013/2014 northern hemisphere influenza season: Results from the global influenza hospital surveillance network. PLoS ONE 2016, 11, e0154970. [Google Scholar] [CrossRef]
- Mohammad, M.A.; Tham, J.; Koul, S.; Rylance, R.; Bergh, C.; Erlinge, D.; Fröbert, O. Association of acute myocardial infarction with influenza: A nationwide observational study. PLoS ONE 2020, 15, e0236866. [Google Scholar] [CrossRef]
- MacIntyre, C.R.; Heywood, A.E.; Kovoor, P.; Ridda, I.; Seale, H.; Tan, T.; Dwyer, D.E. Ischaemic heart disease, influenza and influenza vaccination: A prospective case control study. Heart 2013, 99, 1843–1848. [Google Scholar] [CrossRef]
- Warren-Gash, C.; Geretti, A.M.; Hamilton, G.; Rakhit, R.D.; Smeeth, L.; Hayward, A.C. Influenza-like illness in acute myocardial infarction patients during the winter wave of the influenza A H1N1 pandemic in London: A case–control study. BMJ Open 2013, 3, e002604. [Google Scholar] [CrossRef]
- Penttinen, J.; Valonen, P. The risk of myocardial infarction among Finnish farmers seeking medical care for an infection. Am. J. Public Health 1996, 86, 1440–1442. [Google Scholar] [CrossRef]
- Clayton, T.C.; Thompson, M.; Meade, T.W. Recent respiratory infection and risk of cardiovascular disease: Case-control study through a general practice database. Eur. Heart J. 2008, 29, 96–103. [Google Scholar] [CrossRef] [PubMed]
- Mehra, M.R.; Desai, S.S.; Kuy, S.; Henry, T.D.; Patel, A.N. Cardiovascular disease, drug therapy, and mortality in COVID-19. New Engl. J. Med. 2020, 382, e102. [Google Scholar] [CrossRef] [PubMed]
- Tai, S.; Tang, J.; Yu, B.; Tang, L.; Wang, Y.; Zhang, H.; Zhou, S. Association between cardiovascular burden and requirement of intensive care among patients with mild COVID-19. Cardiovasc. Ther. 2020, 2020, 9059562. [Google Scholar] [CrossRef] [PubMed]
- Feng, Y.; Ling, Y.; Bai, T.; Xie, Y.; Huang, J.; Li, J.; Qu, J. COVID-19 with different severities: A multicenter study of clinical features. Am. J. Respir. Crit. Care Med. 2020, 201, 1380–1388. [Google Scholar] [CrossRef] [PubMed]
- Huang, D.; Yang, H.; Yu, H.; Wang, T.; Yao, R.; Liang, Z. A novel risk score to predict cardiovascular complications in patients with coronavirus disease 2019 (COVID-19): A retrospective, multicenter, observational study. Immun. Inflamm. Dis. 2020, 8, 638–649. [Google Scholar] [CrossRef]
- Zheng, F.; Tang, W.; Li, H.; Huang, Y.; Xie, Y.; Zhou, Z. Clinical characteristics of 161 cases of corona virus disease 2019 (COVID-19) in Changsha. Eur. Rev. Med. Pharmacol. Sci. 2020, 24, 3404–3410. [Google Scholar]
- Clayton, T.; Capps, N.; Stephens, N.; Wedzicha, J.; Meade, T. Recent respiratory infection and the risk of myocardial infarction. Heart 2005, 91, 1601–1602. [Google Scholar] [CrossRef]
- Jalili, M.; Ghafourian, S.; Badakhsh, B. In vitro Eradication of Pseudomonas aeruginosa Persister Cell Producers by Peganum harmala. Clin. Lab. 2022, 68, 6. [Google Scholar] [CrossRef]
- Saigusa, R.; Winkels, H.; Ley, K. T cell subsets and functions in atherosclerosis. Nat. Rev. Cardiol. 2020, 17, 387–401. [Google Scholar] [CrossRef]
- Ndrepepa, G. Atherosclerosis & ischaemic heart disease: Here to stay or gone tomorrow. Indian J. Med. Res. 2017, 146, 293. [Google Scholar]
- Streblow, D.N.; Orloff, S.L.; Nelson, J.A. Do pathogens accelerate atherosclerosis? J. Nutr. 2001, 131, 2798S–2804S. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| ID | Ref | Writer | The Year the Study Was Conducted | The Country in Which the Study Was Conducted | Design | The Average Age of Study Participants | Effective Size | p Value | Number of Sample | Type of Flu | Quality | ||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| OR | 95% Cl | ||||||||||||
| 1 | [13] | Chiang | 2017 | Taiwan | CC | 76.8 | 0.8 | 0.78 | 0.82 | 0.01 | 160 | IV-B | High |
| 2-1 | [14] | Guan | 2008 | China | CC | 60.0 | 3.3 | 1.5 | 7.04 | 0.003 | 209 | IV-A | Moderate |
| 2-2 | [14] | Guan | 2008 | China | CC | 60.0 | 7.5 | 1.3 | 43.0 | 0.001 | 209 | IV-B | Moderate |
| 3-1 | [15] | Xiuru Gu | 2012 | China | CC | 57.0 | 3.1 | 1.5 | 6.4 | 0.004 | 252 | IV-A | High |
| 3-2 | [15] | Xiuru Gu | 2012 | China | CC | 57.0 | 10.2 | 5.7 | 20.0 | 0.001 | 252 | IV-B | High |
| 4 | [16] | Barbera | 2016 | Spain | CS | 85.0 | 1.64 | 1.33 | 2.02 | 0.001 | 728 | IV-A | Moderate |
| 5 | [17] | Mohammad | 2020 | Sweden | CS | 75.0 | 1.05 | 1.02 | 1.08 | 0.002 | 562 | IV-A | Moderate |
| 6-1 | [18] | Maclntyr | 2013 | Australi | CC | 65.0 | 0.55 | 0.35 | 0.85 | 0.008 | 559 | IV-B | Weak |
| 6-2 | [18] | MacIntyr | 2013 | Australi | CC | 65.0 | 1.98 | 1.2 | 3.3 | 0.001 | 559 | IV-A | Weak |
| 7 | [27] | Clayton | 2005 | USA | PHS | 63.0 | 1.0 | 0.5 | 1.9 | 0.002 | 534 | IV-A | High |
| 8 | [19] | Gash | 2013 | London | CC | 40.0 | 3.17 | 0.61 | 16.47 | 0.002 | 137 | IV-B | High |
| 9 | [20] | Penttine | 1996 | Finland | CC | 49.5 | 1.77 | 1.07 | 2.93 | 0.001 | 3172 | IV-A | Moderate |
| 10 | [21] | Clayton | 2007 | UK | CC | 72.0 | 2.48 | 1.67 | 3.7 | 0.002 | 115 | IV-A | Moderate |
| N total: 6428 | |||||||||||||
| ID | Ref | Author | Years | Months | Country | Design | Mean Age | Effect Size | p Value | Sample Size | Quality | ||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| OR | 95% Cl | ||||||||||||
| 1 | [22] | Mandeep | 2020 | May | Boston | CS | 65 | 2.70 | 2.08 | 3.51 | 0.001 | 8910 | Moderate |
| 2 | [23] | Shi Tai | 2020 | August | China | CC | 51 | 2.65 | 1.01 | 6.89 | 0.001 | 332 | High |
| 3 | [24] | Yun Feng | 2020 | April | China | CC | 58 | 3.02 | 1.45 | 6.32 | 0.004 | 476 | High |
| 4 | [25] | Huang | 2020 | February | China | CC | 49 | 2.05 | 0.43 | 14.54 | 0.001 | 41 | Moderate |
| 5 | [7] | Qin | 2020 | April | China | CC | 61 | 4.98 | 1.48 | 16.79 | 0.002 | 452 | Weak |
| 6 | [8] | Wan | 2020 | March | China | CC | 56 | 16.59 | 1.93 | 142.0 | 0.002 | 135 | Moderate |
| 7 | [9] | Wang | 2020 | February | China | CC | 66 | 2.76 | 1.03 | 7.35 | 0.001 | 138 | High |
| 8 | [10] | J. Zhang | 2020 | February | China | CC | 64 | 1.95 | 0.62 | 34.11 | 0.004 | 140 | High |
| 9 | [26] | F. Zheng | 2020 | January | China | CC | 57 | 4.61 | 0.62 | 34.11 | 0.002 | 161 | Moderate |
| N total: 10,785 | |||||||||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jalili, M.; Sayehmiri, K.; Ansari, N.; Pourhossein, B.; Fazeli, M.; Azizi Jalilian, F. Association between Influenza and COVID-19 Viruses and the Risk of Atherosclerosis: Meta-Analysis Study and Systematic Review. Adv. Respir. Med. 2022, 90, 338-348. https://doi.org/10.3390/arm90040043
Jalili M, Sayehmiri K, Ansari N, Pourhossein B, Fazeli M, Azizi Jalilian F. Association between Influenza and COVID-19 Viruses and the Risk of Atherosclerosis: Meta-Analysis Study and Systematic Review. Advances in Respiratory Medicine. 2022; 90(4):338-348. https://doi.org/10.3390/arm90040043
Chicago/Turabian StyleJalili, Mahsa, Kourosh Sayehmiri, Nastaran Ansari, Behzad Pourhossein, Maryam Fazeli, and Farid Azizi Jalilian. 2022. "Association between Influenza and COVID-19 Viruses and the Risk of Atherosclerosis: Meta-Analysis Study and Systematic Review" Advances in Respiratory Medicine 90, no. 4: 338-348. https://doi.org/10.3390/arm90040043