
Association of Serum Albumin and Copeptin with Early Clinical Deterioration and Instability in Community-Acquired Pneumonia

 , , , and
, , , and
Abstract
:Highlights
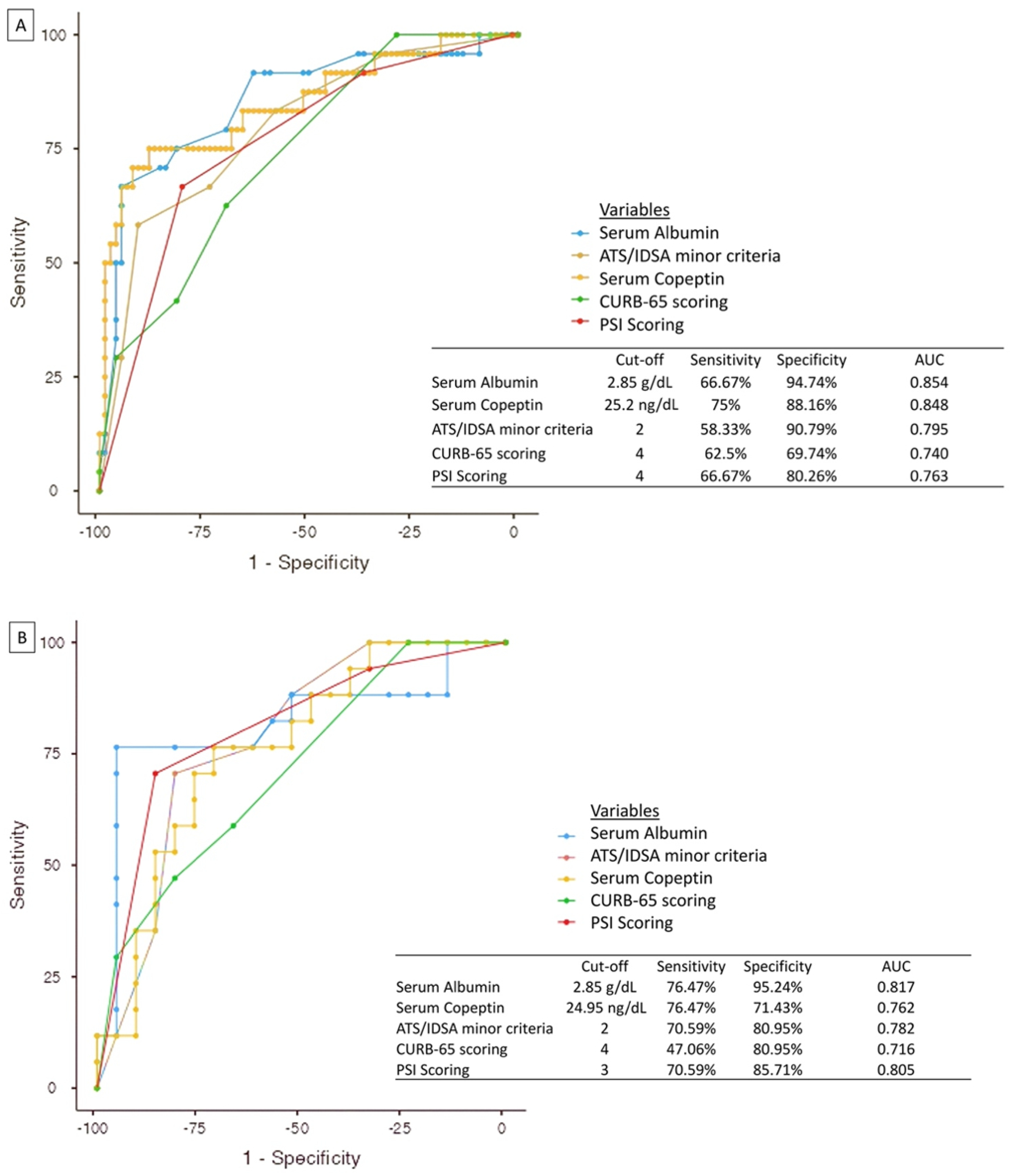
- Serum albumin lower than 2.85 g/dL is the best predictor of mortality in CAP patients
- The addition of serum albumin and copeptin to the traditional clinical scoring systems increases it’s prognostic power
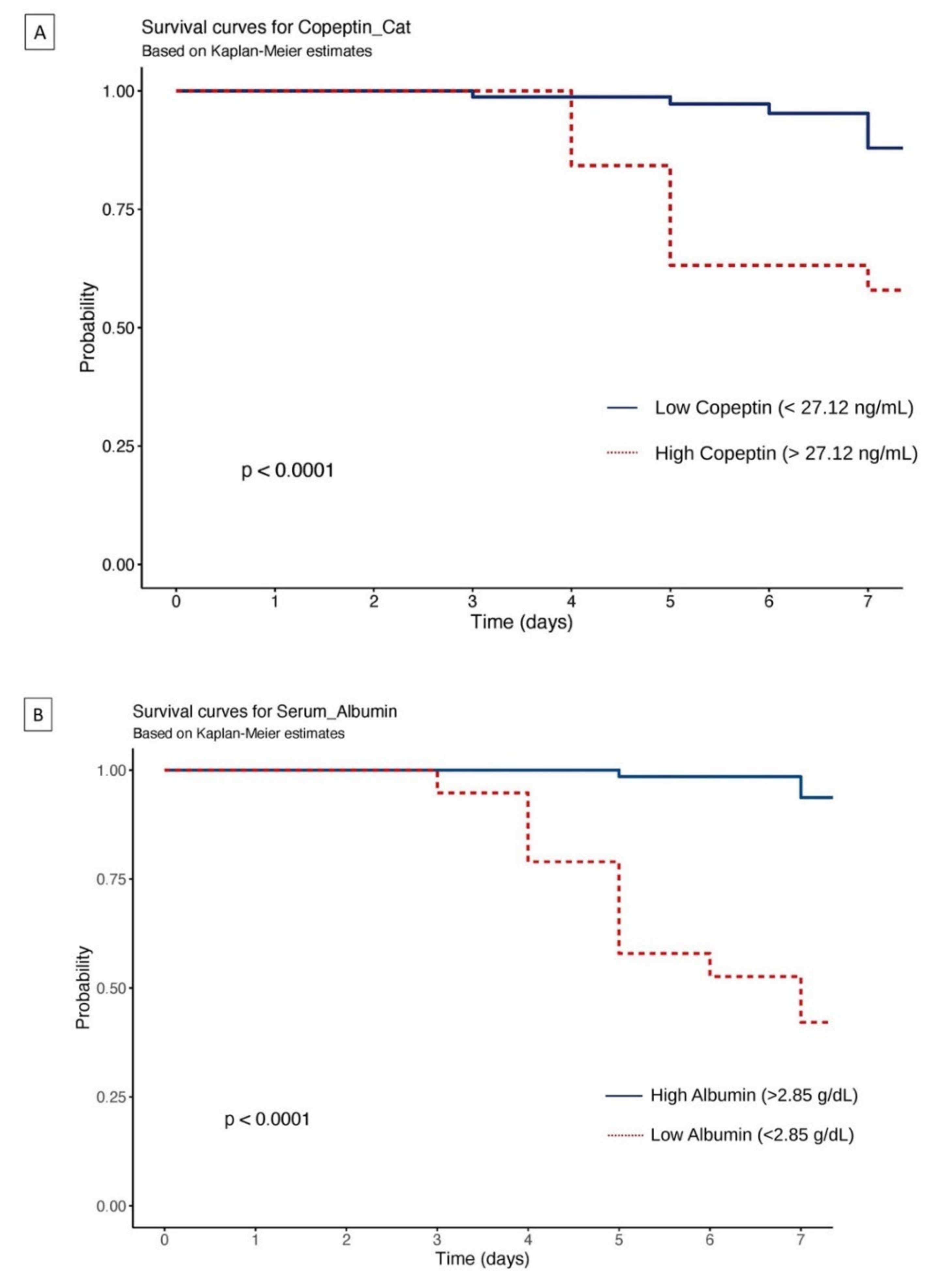
- Biomarkers serum albumin and copeptin can predict early deterioration and clinical instability in hospitalized CAP patients
- Serum albumin, copeptin and ATS/IDSA criteria should be used to predict mortality in patients for predicting clinical instability after 72 h, ICU admission and mortality at day 7 after hospital admission
Abstract
1. Clinical Rationale for the Study
2. Introduction
3. Methodology
3.1. Study Population
- Chest X-ray with patchy infiltrates, segment/leaf consolidation, interstitial change or ground-glass opacity;
- At least one of the following signs:
- ◦
- Symptoms of cough, phlegm, or dyspnea;
- ◦
- Temperature greater than 38.0 °C;
- ◦
- Abnormal auscultatory findings such as abnormal breath sounds and rales;
- ◦
- Leukocytosis (greater than 10 × 109/L).
- The onset of symptoms should be in a community setting, not a health care setting.
3.2. Laboratory and Clinical Assessments
3.3. Statistical Analysis
4. Results
5. Discussion
6. Conclusions
Clinical Implications/Future Directions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Han, X.; Zhou, F.; Li, H.; Xing, X.; Chen, L.; Wang, Y.; Zhang, C.; Liu, X.; Suo, L.; Wang, J.; et al. Effects of age, comorbidity and adherence to current antimicrobial guidelines on mortality in hospitalized elderly patients with community-acquired pneumonia. BMC Infect. Dis. 2018, 18, 192. [Google Scholar] [CrossRef] [PubMed]
- Lopardo, G.D.; Fridman, D.; Raimondo, E.; Albornoz, H.; Lopardo, A.; Bagnulo, H.; Goleniuk, D.; Sanabria, M.; Stamboulian, D.; Luchetti, P.; et al. Incidence rate of community-acquired pneumonia in adults: A population-based prospective active surveillance study in three cities in South America. BMJ Open 2018, 8, e019439. [Google Scholar] [PubMed]
- GBD 2016 Lower Respiratory Infections Collaborators. Estimates of the global, regional, and national morbidity, mortality, and aetiologies of lower respiratory infections in 195 countries, 1990–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet Infect. Dis. 2018, 18, 1191–1210. [Google Scholar] [CrossRef] [Green Version]
- Ramirez, A.J.; Wiemken, T.L.; Peyrani, P.; Arnold, F.W.; Kelley, R.; Mattingly, A.W.; Nakamatsu, R.; Pena, S.; Guinn, E.B.; Furmanek, S.P.; et al. Adults Hospitalized with Pneumonia in the United States: Incidence, Epidemiology, and Mortality. Clin. Infect. Dis. 2017, 65, 1806–1812. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jaton, J.C.; Huser, H.; Blatt, Y.; Pecht, I. Circular dichroism and fluorescence studies of homogeneous antibodies to type III pneumococcal polysaccharide. Biochemistry 1975, 14, 5308–5311. [Google Scholar] [CrossRef]
- Shah, B.A.; Singh, G.; Naik, M.A.; Dhobi, G.N. Bacteriological and clinical profile of Community acquired pneumonia in hospitalized patients. Lung India 2010, 27, 54–57. [Google Scholar]
- Farooqui, H.; Jit, M.; Heymann, D.L.; Zodpey, S. Burden of Severe Pneumonia, Pneumococcal Pneumonia and Pneumonia Deaths in Indian States: Modelling Based Estimates. PLoS ONE 2015, 10, e0129191. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fine, M.J.; Auble, T.E.; Yealy, D.M.; Hanusa, B.H.; Weissfeld, L.A.; Singer, D.E.; Coley, C.M.; Marrie, T.J.; Kapoor, W.N. A prediction rule to identify low-risk patients with community-acquired pneumonia. N. Engl. J. Med. 1997, 336, 243–250. [Google Scholar] [CrossRef]
- Lim, W.S.; Van Der Eerden, M.M.; Laing, R.; Boersma, W.G.; Karalus, N.; Town, I.G.; Lewis, S.A.; Macfarlane, J.T. Defining community acquired pneumonia severity on presentation to hospital: An international derivation and validation study. Thorax 2003, 58, 377–382. [Google Scholar] [CrossRef] [Green Version]
- Chalmers, J.D.; Singanayagam, A.; Akram, A.; Mandal, P.; Short, P.M.; Choudhury, G.; Wood, V.; Hill, A.T. Severity assessment tools for predicting mortality in hospitalised patients with community-acquired pneumonia. Systematic review and meta-analysis. Thorax 2010, 65, 878–883. [Google Scholar] [CrossRef] [Green Version]
- Loke, Y.K.; Kwok, C.S.; Niruban, A.; Myint, P.K. Value of severity scales in predicting mortality from community-acquired pneumonia: Systematic review and meta-analysis. Thorax 2010, 65, 884–890. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Metlay, J.P.; Waterer, G.W.; Long, A.C.; Anzueto, A.; Brozek, J.; Crothers, K.; Cooley, L.A.; Dean, N.C.; Fine, M.J.; Flanders, S.A.; et al. Diagnosis and Treatment of Adults with Community-acquired Pneumonia. An Official Clinical Practice Guideline of the American Thoracic Society and Infectious Diseases Society of America. Am. J. Respir. Crit. Care Med. 2019, 200, e45–e67. [Google Scholar] [CrossRef] [PubMed]
- Chalmers, J.D.; Mandal, P.; Singanayagam, A.; Akram, A.; Choudhury, G.; Short, P.M.; Hill, A.T. Severity assessment tools to guide ICU admission in community-acquired pneumonia: Systematic review and meta-analysis. Intensive Care Med. 2011, 37, 1409–1420. [Google Scholar] [CrossRef] [PubMed]
- Liapikou, A.; Ferrer, M.; Polverino, E.; Balasso, V.; Esperatti, M.; Piñer, R.; Mensa, J.; Luque, N.; Ewig, S.; Menendez, R.; et al. Severe community-acquired pneumonia: Validation of the Infectious Diseases Society of America/American Thoracic Society guidelines to predict an intensive care unit admission. Clin. Infect. Dis. 2009, 48, 377–385. [Google Scholar] [CrossRef] [PubMed]
- Parthasarathi, A.; Basavaraja, C.K.; Arunachala, S.; Chandran, S.; Venkataraman, H.; Satheesh, A.; Mahesh, P.A. Comorbidities Influence the Predictive Power of Hematological Markers for Mortality in Hospitalized COVID-19 Patients. Adv. Respir. Med. 2022, 86, 45–59. [Google Scholar] [CrossRef] [PubMed]
- Mohan, M.; Parthasarathi, A.; Chaya, S.K.; Siddaiah, J.B.; Mahesh, P.A. Fibrinogen: A Feasible Biomarker in Identifying the Severity and Acute Exacerbation of Chronic Obstructive Pulmonary Disease. Cureus 2021, 13, e16864. [Google Scholar] [CrossRef]
- Sibila, O.; Restrepo, M.I. Biomarkers in community-acquired pneumonia: Still searching for the one. Eur. Respir. J. 2019, 53, 1802469. [Google Scholar] [CrossRef] [Green Version]
- Sungurlu, S.; Balk, R.A. The Role of Biomarkers in the Diagnosis and Management of Pneumonia. Clin. Chest Med. 2018, 39, 691–701. [Google Scholar] [CrossRef] [PubMed]
- Sibila, O.; Restrepo, M.I.; Anzueto, A. What is the best antimicrobial treatment for severe community-acquired pneumonia (including the role of steroids and statins and other immunomodulatory agents). Infect. Dis. Clin. 2013, 27, 133–147. [Google Scholar] [CrossRef]
- Aliberti, S.; Amir, A.; Peyrani, P.; Mirsaeidi, M.; Allen, M.; Moffett, B.K.; Myers, J.; Shaib, F.; Cirino, M.; Bordon, J.; et al. Incidence, etiology, timing, and risk factors for clinical failure in hospitalized patients with community-acquired pneumonia. Chest 2008, 134, 955–962. [Google Scholar] [CrossRef]
- Niederman, M.S.; Mandell, L.A.; Anzueto, A.; Bass, J.B.; Broughton, W.A.; Campbell, G.D.; Dean, N.; File, T.; Fine, M.J.; Gross, P.A.; et al. Guidelines for the management of adults with community-acquired pneumonia. Diagnosis, assessment of severity, antimicrobial therapy, and prevention. Am. J. Respir. Crit. Care Med. 2001, 163, 1730–1754. [Google Scholar] [CrossRef] [PubMed]
- Indian Council of Medical Research (ICMR). Treatment Guidelines for Antimicrobial Use in Common Syndromes. 2019. Available online: https://main.icmr.nic.in/sites/default/files/guidelines/Treatment_Guidelines_2019_Final.pdf (accessed on 24 July 2021).
- Halm, E.A.; Fine, M.J.; Marrie, T.J.; Coley, C.M.; Kapoor, W.N.; Obrosky, D.S.; Singer, D.E. Time to clinical stability in patients hospitalized with community-acquired pneumonia: Implications for practice guidelines. JAMA 1998, 279, 1452–1457. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dobsa, L.; Edozien, K.C. Copeptin and its potential role in diagnosis and prognosis of various diseases. Biochem. Med. 2013, 23, 172–190. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morgenthaler, N.G.; Müller, B.; Struck, J.; Bergmann, A.; Redl, H.; Christ-Crain, M. Copeptin, a stable peptide of the arginine vasopressin precursor, is elevated in hemorrhagic and septic shock. Shock 2007, 28, 219–226. [Google Scholar] [CrossRef] [PubMed]
- Muller, B.; Morgenthaler, N.; Stolz, D.; Schuetz, P.; Muller, C.; Bingisser, R.; Bergmann, A.; Tamm, M.; Christ-Crain, M. Circulating levels of copeptin, a novel biomarker, in lower respiratory tract infections. Eur. J. Clin. Investig. 2007, 37, 145–152. Available online: https://onlinelibrary.wiley.com/doi/10.1111/j.1365-2362.2007.01762.x (accessed on 24 July 2021). [CrossRef] [PubMed]
- Kolditz, M.; Halank, M.; Schulte-Hubbert, B.; Bergmann, S.; Albrecht, S.; Höffken, G. Copeptin predicts clinical deterioration and persistent instability in community-acquired pneumonia. Respir. Med. 2012, 106, 1320–1328. Available online: https://linkinghub.elsevier.com/retrieve/pii/S0954611112002223 (accessed on 4 September 2021). [CrossRef] [Green Version]
- Krüger, S.; Ewig, S.; Kunde, J.; Hartmann, O.; Suttorp, N.; Welte, T.; the CAPNETZ Study Group. Pro-atrial natriuretic peptide and pro-vasopressin for predicting short-term and long-term survival in community-acquired pneumonia: Results from the German Competence Network CAPNETZ. Thorax 2010, 65, 208–214. [Google Scholar] [CrossRef] [Green Version]
- Viasus, D.; Del Rio-Pertuz, G.; Simonetti, A.F.; Garcia-Vidal, C.; Acosta-Reyes, J.; Garavito, A.; Carratala, J. Biomarkers for predicting short-term mortality in community-acquired pneumonia: A systematic review and meta-analysis. J. Infect. 2016, 72, 273–282. [Google Scholar] [CrossRef]
- Masiá, M.; Papassotiriou, J.; Morgenthaler, N.G.; Hernández, I.; Shum, C.; Gutiérrez, F. Midregional Pro-A-Type Natriuretic Peptide and Carboxy-Terminal Provasopressin May Predict Prognosis in Community-Acquired Pneumonia. Clin. Chem. 2007, 53, 2193–2201. Available online: https://academic.oup.com/clinchem/article/53/12/2193/5627386 (accessed on 24 July 2021). [CrossRef] [Green Version]
- Fanali, G.; di Masi, A.; Trezza, V.; Marino, M.; Fasano, M.; Ascenzi, P. Human serum albumin: From bench to bedside. Mol. Asp. Med. 2012, 33, 209–290. [Google Scholar] [CrossRef]
- Rothschild, M.A.; Oratz, M.; Schreiber, S.S. Serum albumin. Hepatology 1988, 8, 385–401. [Google Scholar] [CrossRef] [PubMed]
- Viasus, D.; Garcia-Vidal, C.; Simonetti, A.; Manresa, F.; Dorca, J.; Gudiol, F.; Carratala, J. Prognostic value of serum albumin levels in hospitalized adults with community-acquired pneumonia. J. Infect. 2013, 66, 415–423. Available online: https://linkinghub.elsevier.com/retrieve/pii/S016344531200388X (accessed on 24 July 2021). [CrossRef] [PubMed]
- Çelikhisar, H.; Daşdemir Ilkhan, G.; Arabaci, Ç. Prognostic factors in elderly patients admitted to the intensive care unit with community-acquired pneumonia. Aging Male 2020, 23, 1425–1431. [Google Scholar] [CrossRef]
- Shi, T.; Chen, C.; Huang, L.; Fan, H.; Lu, G.; Yang, D.; Zhao, C.; Zhang, D. Risk factors for mortality from severe community-acquired pneumonia in hospitalized children transferred to the pediatric intensive care unit. Pediatr. Neonatol. 2020, 61, 577–583. [Google Scholar] [CrossRef] [PubMed]
- Falcão, H.; Japiassú, A.M. Albumin in critically ill patients: Controversies and recommendations. Rev. Bras. Ter. Intensiva 2011, 23, 87–95. [Google Scholar] [CrossRef] [PubMed]
- Zhao, L.; Bao, J.; Shang, Y.; Yin, L.; Yu, Y.; Xie, Y.; Chen, L.; Zheng, Y.; Xu, Y.; Gao, Z. The prognostic value of serum albumin levels and respiratory rate for community-acquired pneumonia: A prospective, multi-center study. PLoS ONE 2021, 16, e0248002. [Google Scholar] [CrossRef]
- Corrales-Medina, V.F.; Suh, K.N.; Rose, G.; Chirinos, J.A.; Doucette, S.; Cameron, B.; Fergusson, D. Cardiac complications in patients with community-acquired pneumonia: A systematic review and meta-analysis of observational studies. PLoS Med. 2011, 8, e1001048. [Google Scholar] [CrossRef] [Green Version]
- Avci, S.; Perincek, G. The Alveolar-Arterial Gradient, Pneumonia Severity Scores and Inflammatory Markers to Predict 30-Day Mortality in Pneumonia. Am. J. Emerg. Med. 2020, 38, 1796–1801. [Google Scholar] [CrossRef] [PubMed]
- He, Y.; Li, M.; Mai, C.; Chen, L.; Zhang, X.; Zhou, J.; Yang, Z.; Ni, J.; Chen, Y.; Cai, M.; et al. Anemia and Low Albumin Levels Are Associated with Severe Community-Acquired Pneumonia in Pregnancy: A Case-Control Study. Tohoku J. Exp. Med. 2019, 248, 297–305. [Google Scholar] [CrossRef]
- Adnan, M.; Hashmat, N.; Latif, M.; Ali, Z.; Rahat, T. Hypoalbuminemia Predicts Intensive Care Need among Adult Inpatients with Community Acquired Pneumonia: A Cross Sectional Study. J. Infect. Dev. Ctries. 2018, 12, 636–641. [Google Scholar] [CrossRef]
- Miyazaki, H.; Nagata, N.; Akagi, T.; Takeda, S.; Harada, T.; Ushijima, S.; Aoyama, T.; Yoshida, Y.; Yatsugi, H.; Fujita, M.; et al. Comprehensive Analysis of Prognostic Factors in Hospitalized Patients with Pneumonia Occurring Outside Hospital: Serum Albumin Is Not Less Important than Pneumonia Severity Assessment Scale. J. Infect. Chemother. 2018, 24, 602–609. [Google Scholar] [CrossRef] [PubMed]
- Curbelo, J.; Luquero Bueno, S.; Galván-Román, J.M.; Ortega-Gómez, M.; Rajas, O.; Fernández-Jiménez, G.; Vega-Piris, L.; Rodríguez-Salvanes, F.; Arnalich, B.; Díaz, A.; et al. Inflammation Biomarkers in Blood as Mortality Predictors in Community-Acquired Pneumonia Admitted Patients: Importance of Comparison with Neutrophil Count Percentage or Neutrophil-Lymphocyte Ratio. PLoS ONE 2017, 12, e0173947. [Google Scholar] [CrossRef] [PubMed]
- Holter, J.C.; Ueland, T.; Jenum, P.A.; Müller, F.; Brunborg, C.; Frøland, S.S.; Aukrust, P.; Husebye, E.; Heggelund, L. Risk Factors for Long-Term Mortality after Hospitalization for Community-Acquired Pneumonia: A 5-Year Prospective Follow-Up Study. PLoS ONE 2016, 11, e0148741. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alcoba, G.; Manzano, S.; Lacroix, L.; Galetto-Lacour, A.; Gervaix, A. Proadrenomedullin and Copeptin in Pediatric Pneumonia: A Prospective Diagnostic Accuracy Study. BMC Infect. Dis. 2015, 15, 347. [Google Scholar] [CrossRef] [Green Version]
- Suter-Widmer, I.; Christ-Crain, M.; Zimmerli, W.; Albrich, W.; Mueller, B.; Schuetz, P.; for the ProHOSP Study Group. Predictors for Length of Hospital Stay in Patients with Community-Acquired Pneumonia: Results from a Swiss Multicenter Study. BMC Pulm. Med. 2012, 12, 21. [Google Scholar] [CrossRef] [Green Version]
- Lee, J.H.; Kim, J.; Kim, K.; Jo, Y.H.; Rhee, J.; Kim, T.Y.; Na, S.H.; Hwang, S.S. Albumin and C-Reactive Protein Have Prognostic Significance in Patients with Community-Acquired Pneumonia. J. Crit. Care 2011, 26, 287–294. [Google Scholar] [CrossRef]
- Schuetz, P.; Wolbers, M.; Christ-Crain, M.; Thomann, R.; Falconnier, C.; Widmer, I.; Neidert, S.; Fricker, T.; Blum, C.; Schild, U.; et al. Prohormones for Prediction of Adverse Medical Outcome in Community-Acquired Pneumonia and Lower Respiratory Tract Infections. Crit. Care 2010, 14, R106. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| ICU Admission/Death within 7 days | Clinical Instability within 72 h of Admission | ||||||
|---|---|---|---|---|---|---|---|
| Outcome | Measure | Yes | No | p-Value | Yes | No | p-Value |
| (n = 17) | (n = 83) | (n = 38) | (n = 62) | ||||
| Age | Mean (SD) | 57.3 (11.5) | 54.7 (18.9) | 0.584 * | 54.7 (17.6) | 55.5 (18.1) | 0.838 * |
| Sex | Male | 11 (64.7%) | 53 (63.9%) | 0.947 ^ | 21 (55.3) | 43 (69.4) | 0.226 ^ |
| Female | 6 (35.3%) | 30 (36.1%) | 17 (44.7) | 19 (30.6) | |||
| Total number of days of admission | Median (IQR) | 6.5 (5.0 to 9.8) | 7.0 (5.0 to 9.0) | 0.917 # | 7.0 (5.0 to 9.5) | 6.0 (5.0 to 8.0) | 0.045 # |
| Basal body temperature | Median (IQR) | 97.8 (97.6 to 99.1) | 98.7 (97.5 to 99.5) | 0.381 # | 98.6 (97.6 to 99.5) | 98.6 (97.3 to 99.0) | 0.398 # |
| Smokers | N (%) | 7 (41.2%) | 29 (34.9%) | 0.626 # | 16 (42.1) | 20 (32.3) | 0.435 # |
| PSI Score | Median (IQR) | 5.0 (4.0 to 5.0) | 4.0 (3.0 to 4.0) | <0.001 # | 4.0 (4.0 to 5.0) | 4.0 (3.0 to 4.0) | <0.01 # |
| ATS/IDSA Minor criteria | Median (IQR) | 5.0 (3.0 to 6.0) | 2.0 (1.0 to 4.0) | 0.004 # | 3.0 (2.0 to 4.8) | 2.0 (1.0 to 4.0) | 0.05 # |
| CURB-65 score | Median (IQR) | 2.0 (2.0 to 3.0) | 2.0 (1.0 to 2.0) | <0.001 # | 2.0 (2.0 to 2.0) | 2.0 (1.0 to 2.0) | 0.01 # |
| Respiratory rate (per min) | Median (IQR) | 29.0 (27.0 to 34.0) | 25.0 (20.0 to 28.0) | <0.001 # | 27.0 (23.0 to 30.0) | 24.0 (20.0 to 28.0) | 0.005 # |
| Comorbidities | |||||||
| COPD | N (%) | 6 (35.3%) | 23 (27.7%) | 0.53 ^ | 14 (36.8) | 15 (24.2) | 0.26 ^ |
| Asthma | N (%) | 1 (5.9%) | 8 (9.6%) | 0.622 ^ | 2 (5.3) | 7 (11.3) | 0.508 ^ |
| Diabetes mellitus | N (%) | 5 (29.4%) | 16 (19.3%) | 0.35 ^ | 11 (28.9) | 21 (21.0) | 0.202 ^ |
| Obesity | N (%) | 1 (5.9%) | 4 (4.8%) | 0.855 ^ | 1 (2.6) | 4 (6.5) | 0.705 ^ |
| Hypertension | N (%) | 4 (23.5%) | 17 (20.5%) | 0.779 ^ | 7 (18.4) | 14 (22.6) | 0.808 ^ |
| Haematological Investigations | |||||||
| Haemoglobin (g/dL) | Mean (SD) | 13.3 (1.8) | 12.6 (1.9) | 0.172 * | 13.0 (2.2) | 12.6 (1.8) | 0.277 * |
| Monocytes ×109 cells/L | Mean (SD) | 5.8 (2.7) | 5.3 (2.3) | 0.507 * | 5.4 (2.6) | 5.4 (2.3) | 0.898 * |
| TLC ×109 cells/L | Mean (SD) | 16638.3 (6651.8) | 11315.9 (5137.7) | <0.001 * | 13452.1 (6400.9) | 11551.8 (5290.5) | 0.111 * |
| ANC ×109 cells/L | Median (IQR) | 87.2 (82.0 to 91.8) | 83.7 (77.0 to 89.0) | 0.111 # | 82.3 (75.2 to 88.0) | 86.8 (77.8 to 91.5) | 0.03 # |
| ALC ×109 cells/L | Median (IQR) | 8.6 (6.0 to 13.0) | 9.9 (6.7 to 16.8) | 0.476 # | 11.0 (7.6 to 17.6) | 9.0 (6.0 to 15.2) | 0.092 # |
| Platelets (lakh cells/cu.mm) | Median (IQR) | 2.7 (1.9 to 3.1) | 2.7 (2.3 to 3.3) | 0.481 # | 2.7 (2.2 to 3.3) | 2.7 (2.1 to 3.5) | 0.699 # |
| NLR | Median (IQR) | 10.1 (6.4 to 15.3) | 8.5 (4.6 to 13.4) | 0.419 # | 7.5 (4.6 to 11.7) | 9.8 (5.1 to 15.2) | 0.079 # |
| PLR | Median (IQR) | 0.2 (0.2 to 0.3) | 0.3 (0.2 to 0.4) | 0.6 # | 0.2 (0.2 to 0.4) | 0.3 (0.2 to 0.5) | 0.076 # |
| CRP (mg/L) | Mean (SD) | 29.2 (13.6) | 23.1 (13.0) | 0.079 * | 24.8 (12.5) | 23.9 (13.7) | 0.75 * |
| Serum Albumin (g/dL) | Mean (SD) | 2.6 (0.4) | 3.4 (0.4) | <0.001 * | 3.1 (0.6) | 3.4 (0.4) | 0.002 * |
| Serum Copeptin (ng/mL) | Mean (SD) | 33.1 (7.1) | 18.1 (6.7) | <0.001 * | 24.0 (9.9) | 18.9 (7.6) | 0.004 * |
| Complications ** | Yes | 8 (44.4) | 4 (4.9) | <0.001 ^ | 10 (26.3) | 4 (6.5) | 0.013 ^ |
| No | 10 (55.6) | 78 (95.1) | 28 (73.7) | 58 (93.5) | |||
| Albumin | Copeptin | PSI | ATS | CURB-65 | ||
|---|---|---|---|---|---|---|
| Albumin | Pearson’s r | - | ||||
| p-value | - | |||||
| 95% CI Upper | - | |||||
| 95% CI Lower | - | |||||
| Spearman’s rho | - | |||||
| p-value | - | |||||
| Copeptin | Pearson’s r | −0.554 *** | - | |||
| p-value | <0.001 | - | ||||
| 95% CI Upper | −0.401 | - | ||||
| 95% CI Lower | −0.677 | - | ||||
| PSI | Spearman’s rho | −0.333 *** | 0.865 *** | - | ||
| p-value | <0.001 | <0.001 | - | |||
| 95% CI Upper | −0.137 | 0.88 | - | |||
| 95% CI Lower | −0.49 | 0.751 | - | |||
| ATS/IDSA | Spearman’s rho | −0.326 *** | 0.295 ** | 0.22 * | - | |
| p-value | < .001 | 0.003 | 0.028 | - | ||
| 95% CI Upper | −0.195 | 0.457 | 0.39 | - | ||
| 95% CI Lower | −0.534 | 0.095 | 0.013 | - | ||
| CURB-65 | Spearman’s rho | −0.207 * | 0.274 ** | 0.209 * | 0.822 *** | 0.539 *** |
| p-value | 0.038 | 0.006 | 0.037 | <0.001 | <0.001 | |
| 95% CI Upper | −0.051 | 0.432 | 0.366 | 0.861 | 0.552 | |
| 95% CI Lower | −0.421 | 0.065 | −0.014 | 0.716 | 0.22 |
| Dependent | HR (Univariable) | HR (Multivariable) |
|---|---|---|
| PSI | 2.06 (1.06–4.03, p = 0.034) | 1.31 (0.61–2.78, p = 0.487) |
| CURB-65 | 11.31 (1.25–102.27, p = 0.031) | 8.92 (0.74–107.35, p = 0.085) |
| ATS/IDSA | 7.16 (1.01–56.10, p = 0.041) | 1.35 (0.06–30.93, p = 0.849) |
| Respiratory rate | 1.12 (1.05–1.20, p < 0.001) | 1.42 (1.08-1.88, p = 0.013) |
| TLC | 1.00 (1.00–1.00, p = 0.113) | 1.00 (1.00–1.00, p = 0.873) |
| Complications * | 5.35 (2.26–12.68, p < 0.001) | 3.02 (1.02–9.25, p = 0.048) |
| Albumin | 0.28 (0.15–0.54, p < 0.001) | 0.41 (0.18–0.94, p = 0.034) |
| Copeptin | 1.09 (1.04–1.15, p ≤0.001) | 1.94 (1.03–3.67, p = 0.042) |
| Clinical Instability | ||||
|---|---|---|---|---|
| Predictor | SENS | SPE | AUC | p-Value |
| Serum Albumin + PSI | 0.857 | 0.706 | 0.885 | 0.021 * |
| Serum Albumin + ATS/IDSA | 0.857 | 0.765 | 0.894 | 0.012 * |
| Serum Albumin + CURB-65 | 0.81 | 0.765 | 0.838 | 0.15 |
| Serum Copeptin + PSI | 0.81 | 0.706 | 0.84 | 0.026 * |
| Serum Copeptin + ATS/IDSA | 0.857 | 0.706 | 0.863 | 0.007 * |
| Serum Copeptin + CURB-65 | 0.81 | 0.647 | 0.849 | 0.026 * |
| Serum Albumin + Serum Copeptin + PSI | 0.857 | 0.765 | 0.894 | 0.043 * |
| Serum Albumin + Serum Copeptin + ATS/IDSA | 0.857 | 0.785 | 0.905 | 0.019 * |
| Serum Albumin + Serum Copeptin + CURB-65 | 0.857 | 0.706 | 0.885 | 0.096 * |
| Mortality/ICU admission in 7 days | ||||
| Predictor | SENS | SPE | AUC | p-value |
| Serum Albumin + PSI | 0.947 | 0.625 | 0.89 | 0.010 * |
| Serum Albumin + ATS/IDSA | 0.934 | 0.583 | 0.885 | 0.004 * |
| Serum Albumin + CURB-65 | 0.947 | 0.542 | 0.897 | 0.061 * |
| Serum Copeptin + PSI | 0.974 | 0.542 | 0.852 | 0.351 |
| Serum Copeptin + ATS/IDSA | 0.961 | 0.708 | 0.898 | 0.001 * |
| Serum Copeptin + CURB-65 | 0.974 | 0.583 | 0.864 | 0.075 * |
| Serum Albumin + Serum Copeptin + PSI | 0.947 | 0.667 | 0.888 | 0.942 |
| Serum Albumin + Serum Copeptin + ATS/IDSA | 0.947 | 0.75 | 0.911 | 0.007 * |
| Serum Albumin + Serum Copeptin + CURB-65 | 0.947 | 0.667 | 0.895 | 0.013 * |
| Author | Sample Size | Marker | Outcome | Result |
|---|---|---|---|---|
| Present study, 2021, India | 100 | Albumin, copeptin | Combined ICU admission or mortality at day 7 and clinical instability after 72 h. | Albumin was the best predictor of mortality (AUC = 0.854), followed by copeptin (AUC = 0.848). The combination of serum albumin + serum copeptin + ATS/IDSA had the highest AUC for prediction of ICU admission or death within 7 days (AUC = 0.911) and for prediction of clinical instability after 72 h of admission (AUC = 0.905). |
| Zhao L et al. [37], 2021, China | 366 | Albumin | 30-day mortality | PSI and CURB-65 were found to be better independent predictors compared to albumin (AUC: 0.79 and 0.78 vs. 0.76) |
| Avci S et al. [39], 2020, Turkey | 206 | Albumin, c-reactive protein/albumin ratio (CAR), CRP, NLR, PLR, procalcitonin, A-a o2 gradient, A-a o2 difference | Prediction of 30-day mortality | Albumin (AUC: 0.80) was found to be a better predictor of 30-day mortality than all blood parameters and CURB-65 scores. PSI score was found to be better than albumin (AUC: 0.86) |
| Celikhisar H et al. [34], 2020, Turkey | 86 | Lactate, procalcitonin, blood glucose, serum albumin | Risk factors for ICU mortality | Lactate, procalcitonin, albumin (OR: 3.34) and blood glucose were found to be significant independent risk factors |
| Shi T et al. [35], 2020, China | 113 | Albumin, ALT, AST, hemoglobin | Risk factors for mortality | <90% oxygen saturation and albumin < 35 g/L were found to be significant risk factors for mortality (OR: 8.77 and 4.73, respectively) |
| He Y et al. [40], 2019, China | 175 | WBC count, CRP, procalcitonin, hemoglobin, platelet count, albumin, BUN, creatinine, uric acid, AST and ALT | Risk factors for severe pneumonia | On admission, albumin was significantly lower in SCAP patients compared to non-severe patients |
| Adnan M et al. [41], 2018, Pakistan | 134 | Albumin, B/A ratio, BUN | Prediction of ICU admission | Albumin was found to be the better predictor for ICU admission (AUC: 0.718) compared to B/A ratio, BUN or CURB-65 |
| Miyazaki H et al. [42], 2018, Japan | 534 | Albumin, PCT | 30-day mortality | Lowest albumin within 1 week of admission was found to be the best predictor (AUC:0.85), followed by albumin at admission (0.81) |
| Curbelo J et al. [43], 2017, Spain | 154 | Copeptin, proadrenomedullin, lymphocyte%, neutrophil%, NLR, procalcitonin | Prediction of 30-day and 90-day mortality | On admission, pro-ADM followed by copeptin were found to be the best predictors of both 30-day (AUC: 0.89 and 0.84, respectively) and 90-day (AUC: 0.84 and 0.79, respectively) mortality |
| Holter JC et al. [44], 2016, Norway | 259 | CRP, creatinine, albumin | Prediction of risk of long-term mortality | It was found that every 5 g/L decrease in albumin levels increased the risk of death by 25%. |
| Alcoba G et. [45], 2015, Switzerland | 88 | Copeptin, proadrenomedullin, CRP | Prediction of complicated pneumonia | Proadrenomedullin and CRP performed much better than copeptin in predicting complicated pneumonia (AUC: 0.85 each vs. 0.59) |
| Kruger S et al. [28], 2013, Germany | 1740 | CRP, procalcitonin, MR-proadrenomedullin, WBC count and copeptin | 28-day mortality and 180-day mortality | Copeptin was found to have superior diagnostic accuracy to MR-proANP, CRP, CRB-65 and WBC count (AUC: 0.84) in prediction of 28-day mortality. Similar results were found for 180-day mortality (AUC: 0.78), except for MR-proANP (AUC: 0.81) |
| Kolditz M et al. [27], 2012, Germany | 51 | Copeptin, C-reactive protein, MR-proadrenomedullin and pro-calcitonin | Combined ICU admission or mortality at day 7 and clinical instability after 72 h. | The diagnostic accuracy of copeptin for both ICU admission and mortality, as well as clinical instability (AUC: 0.81 and 0.74, respectively). Addition of copeptin to ATS/IDSA minor criteria resulted in significant improvement in prediction of 7-day mortality (AUC: 0.85) and prediction of clinical instability (combined AUC: 0.81). |
| Suter-Widmer I et al. [46], 2012, Switzerland | 875 | Albumin, CRP, procalcitonin | Prediction of length of hospital stay | Albumin was associated with increased duration of hospital stay (HR: 0.77) |
| Lee JH et al. [47], 2011, South Korea | 424 | Albumin, CRP | 28-day mortality, ICU admission or vasopressor use or mechanical ventilation | Albumin was found to be the best predictor of 28-day mortality (AUC: 0.66). When added with PSI and CRP, the predictive capability significantly increased (AUC: 0.76) |
| Schuetz P et al. [48], 2010, Switzerland | 925 | Procalcitonin, pro-ADM, pro-ANP, pro-ET1, copeptin | Prediction of severe outcome | Copeptin (AUC: 0.70) was superior to PSI and curb-65 alone but inferior to pro-ET1 and pro-ADM (AUC: 0.72, respectively) |
| Muller B et al. [26], 2007, Germany | 545 | Copeptin, CRP, leucocyte count, procalcitonin | 6-week mortality | Copeptin was found to be the better predictor (AUC: 0.75) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Parthasarathi, A.; Padashetti, V.C.; Padukudru, S.; Chaya, S.K.; Siddaiah, J.B.; Anand, M.P. Association of Serum Albumin and Copeptin with Early Clinical Deterioration and Instability in Community-Acquired Pneumonia. Adv. Respir. Med. 2022, 90, 323-337. https://doi.org/10.3390/arm90040042
Parthasarathi A, Padashetti VC, Padukudru S, Chaya SK, Siddaiah JB, Anand MP. Association of Serum Albumin and Copeptin with Early Clinical Deterioration and Instability in Community-Acquired Pneumonia. Advances in Respiratory Medicine. 2022; 90(4):323-337. https://doi.org/10.3390/arm90040042
Chicago/Turabian StyleParthasarathi, Ashwaghosha, Vaibhav C. Padashetti, Sunag Padukudru, Sindaghatta Krishnarao Chaya, Jayaraj Biligere Siddaiah, and Mahesh Padukudru Anand. 2022. "Association of Serum Albumin and Copeptin with Early Clinical Deterioration and Instability in Community-Acquired Pneumonia" Advances in Respiratory Medicine 90, no. 4: 323-337. https://doi.org/10.3390/arm90040042