
Perception of Quality of Life and Fatigue in Multiple Sclerosis Patients Treated with High-Dose Vitamin D


Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants and Procedures
- sociodemographic information (i.e., age, gender, weight, marital status, employment status);
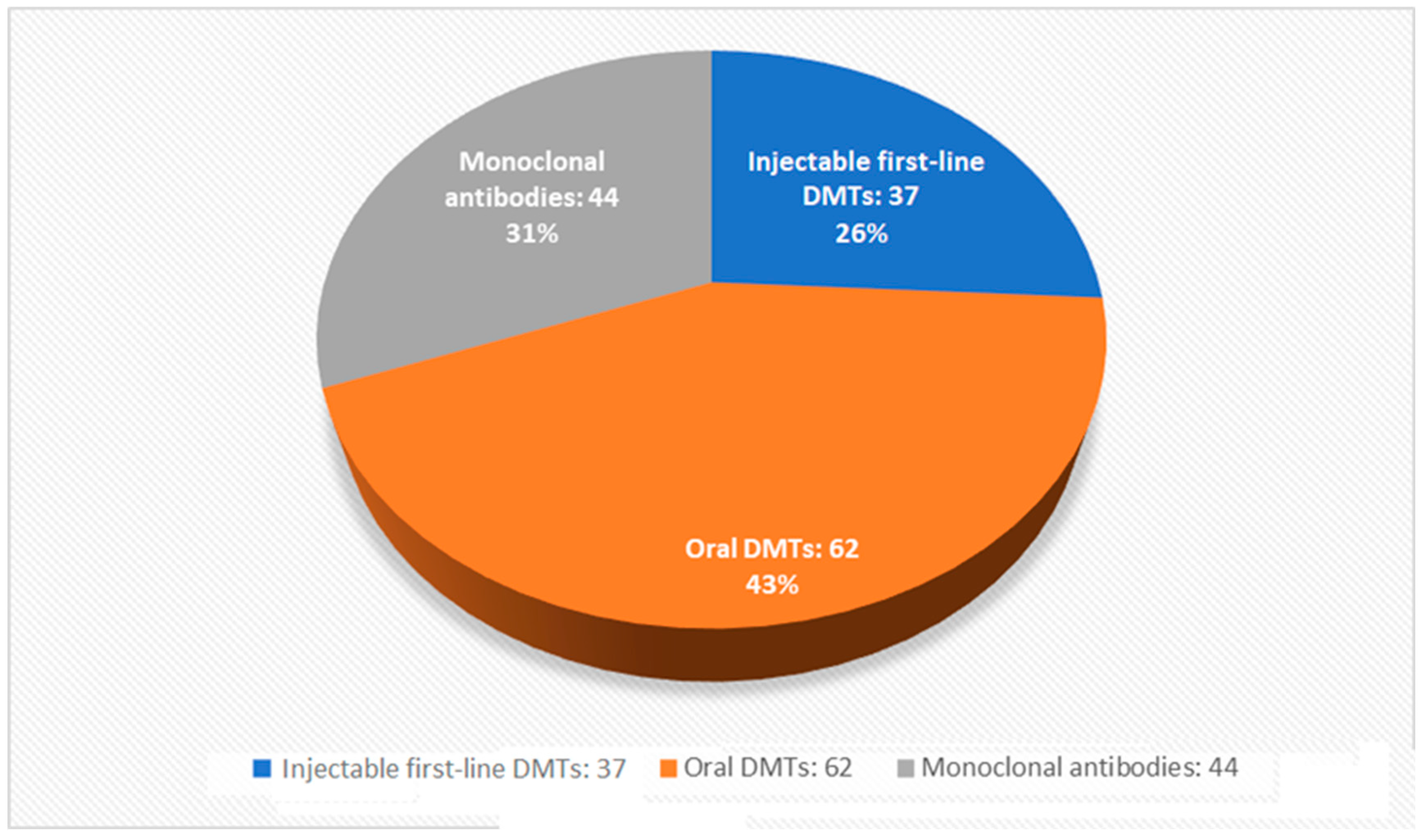
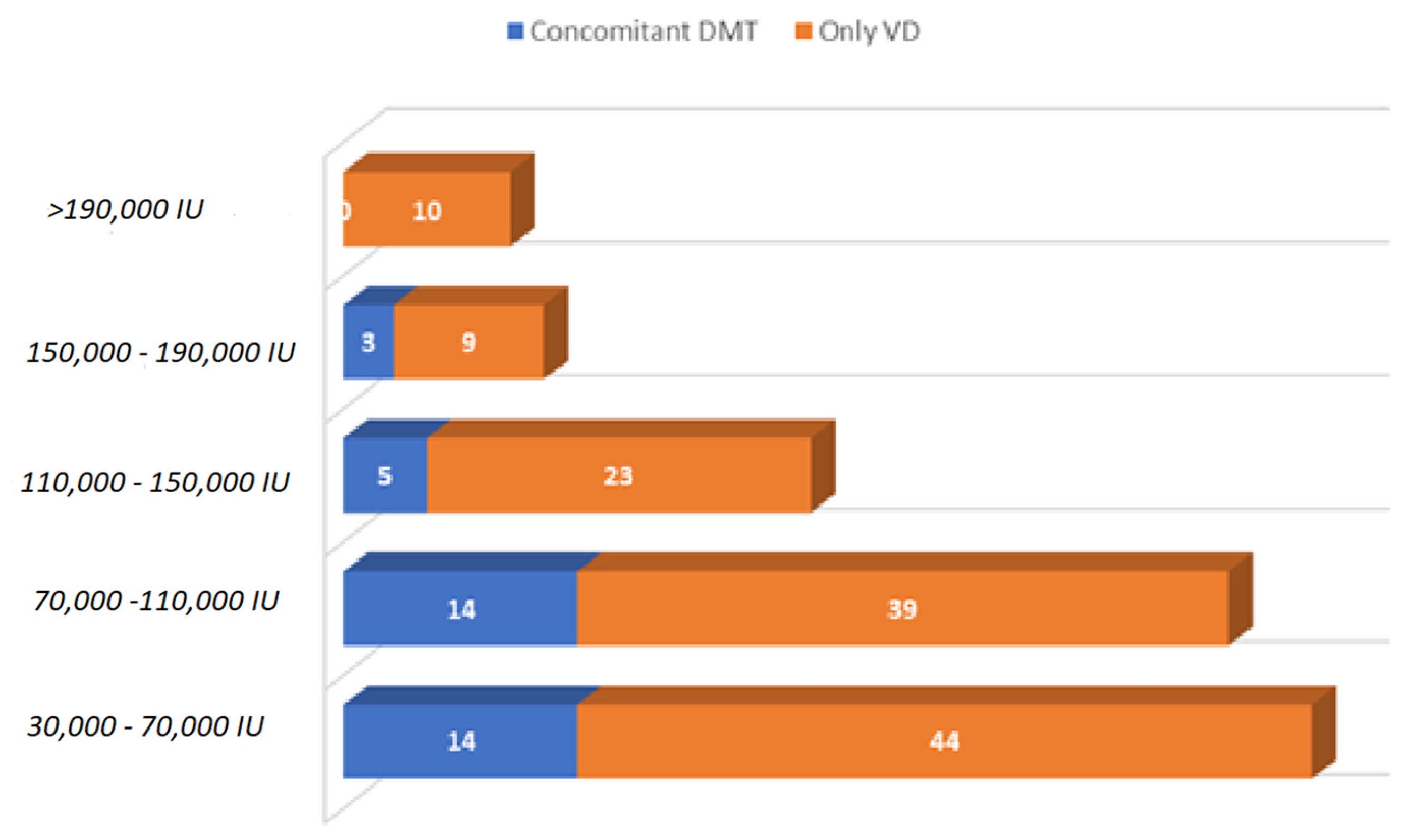
- clinical information (i.e., MS duration, EDSS, dosage of vitamin D taken, use of DMTs, adherence to the Coimbra protocol);
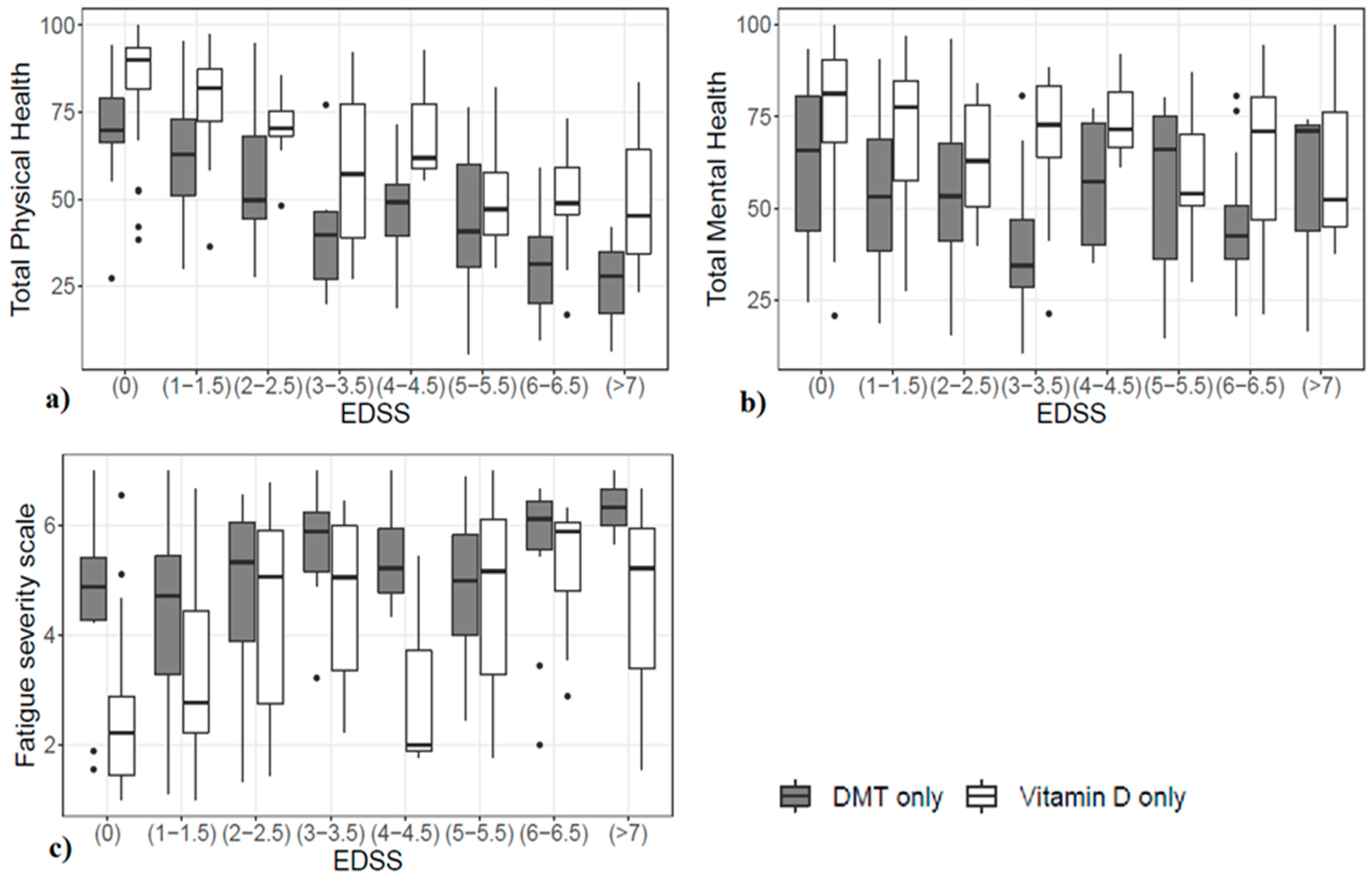
- perception of quality of life: total physical health (TPH) and total mental health (TMH) (the two components of the MSQOL-54 questionnaire);
- perception of the impact of fatigue in daily life (FSS).
2.2. Statistical Analysis
3. Results
3.1. Characteristics of the Study Sample
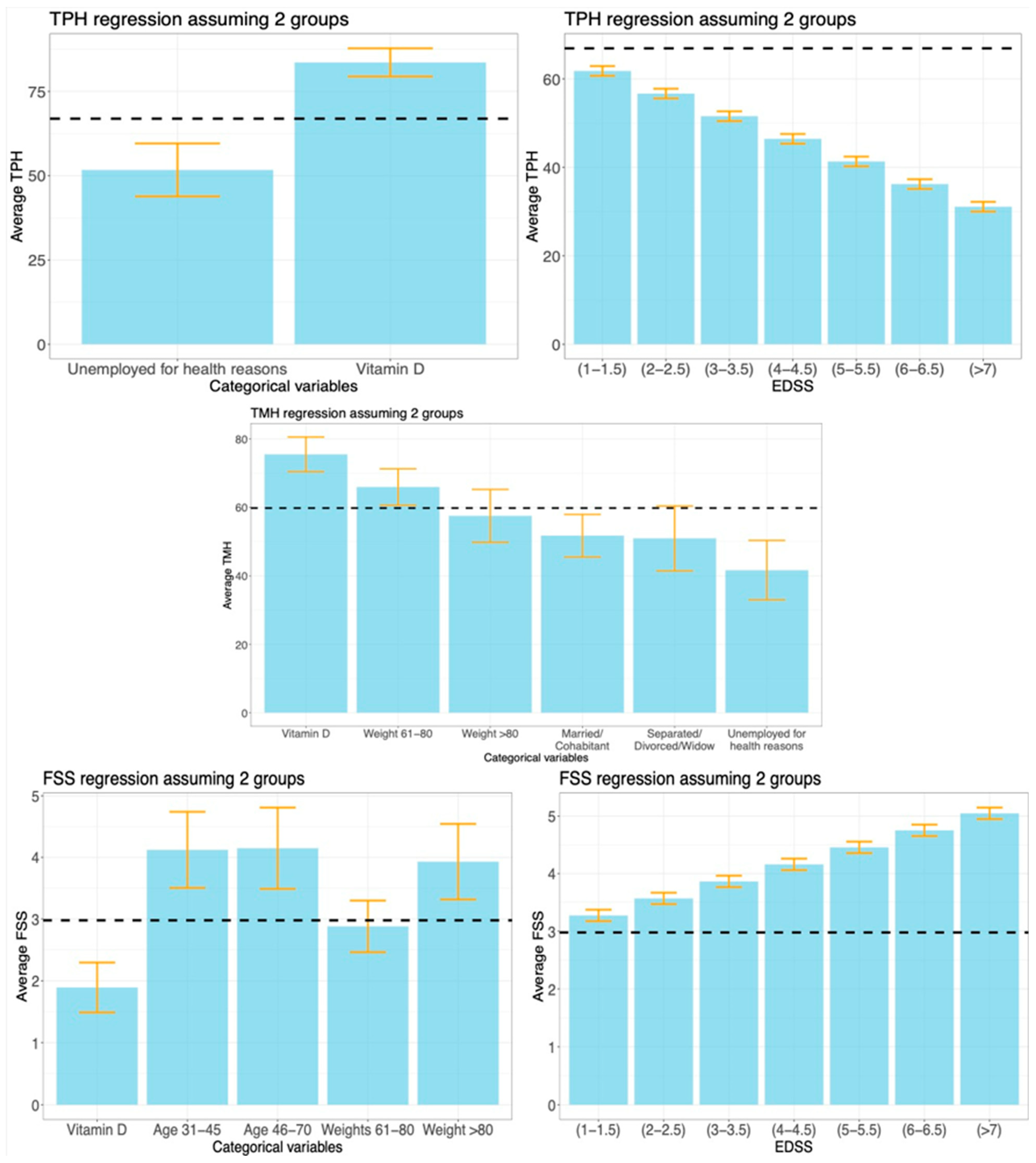
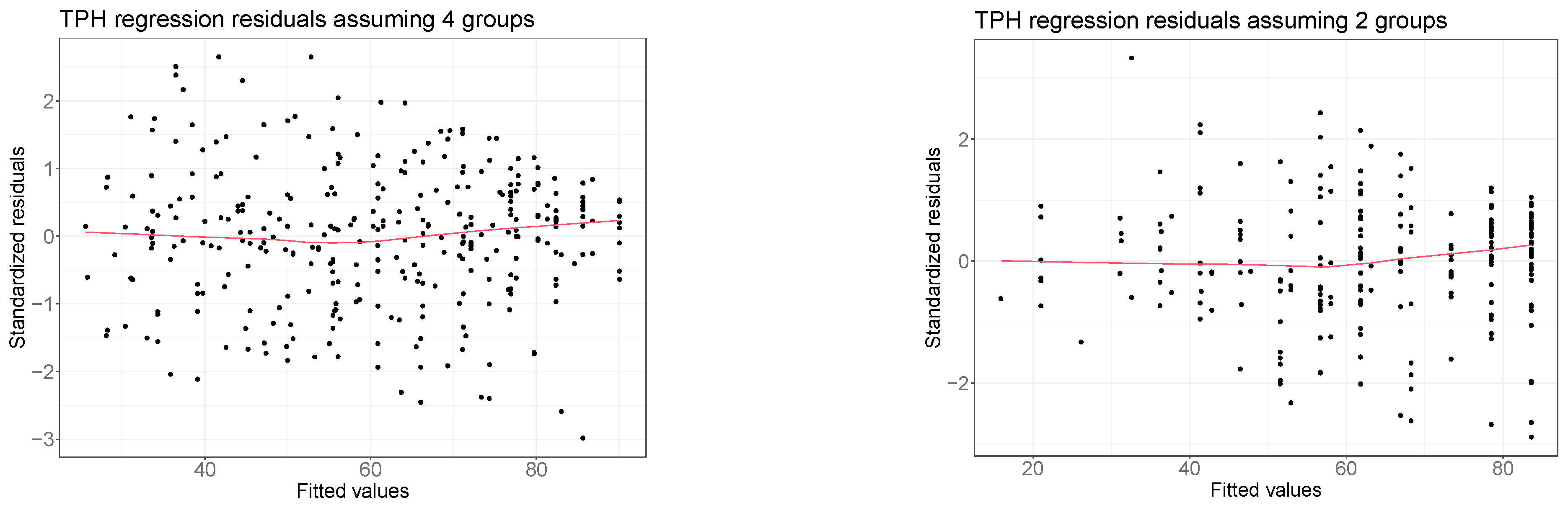
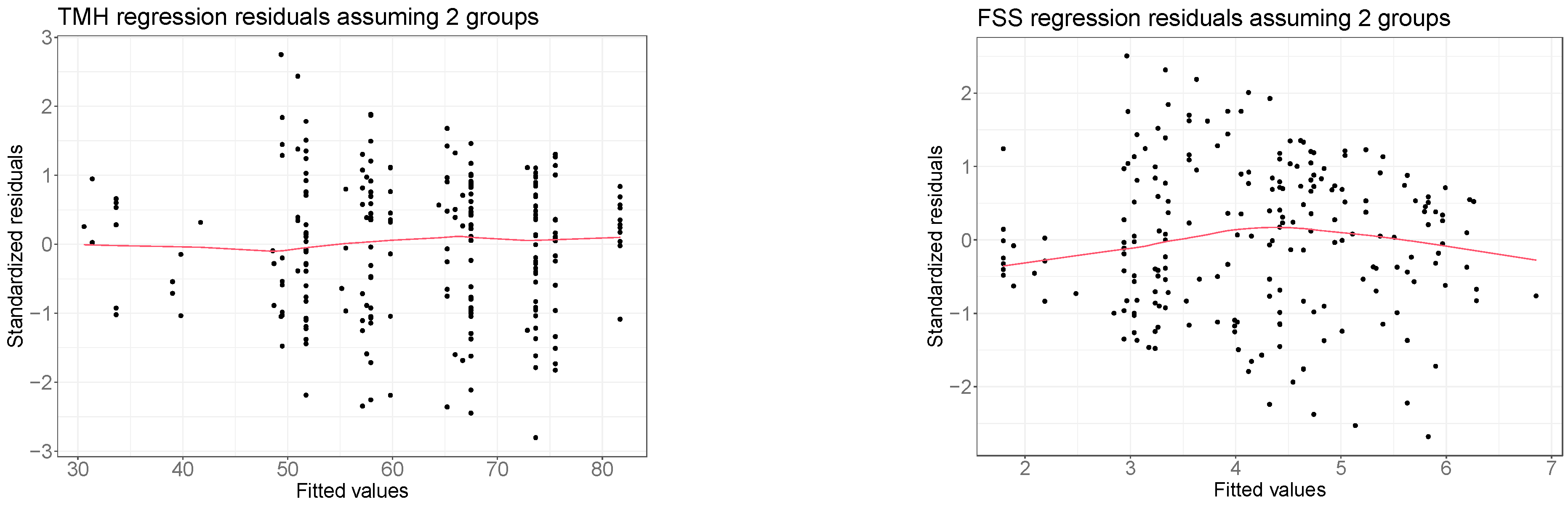
3.2. Results of the Regression Analysis on TPH in All Four Groups
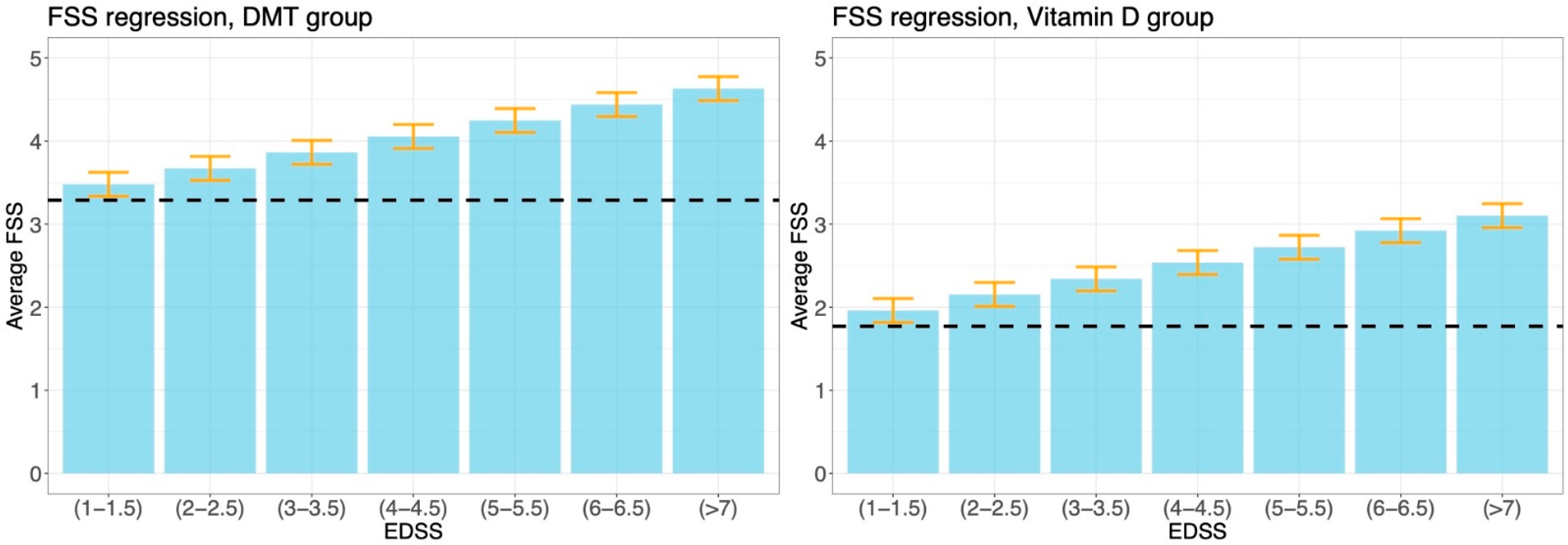
3.3. Analysis of VD-Only Versus DMT-Only Groups
4. Discussion
4.1. Summary and Contributions
4.2. Strengths and Limitations
4.3. Future Work
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
Appendix A



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Mean Result (Diff. from Reference) | Standard Error | p-Value | |
|---|---|---|---|
| Total Physical Health * | |||
| Reference group | 66.91 | 2.03 | <0.001 |
| EDSS single-point increase | (−5.12) | 0.55 | <0.001 |
| Inactive worker (for health reasons) | 51.71 (−15.20) | 4.01 | <0.001 |
| VD group | 83.60 (16.69) | 2.10 | <0.001 |
| Total Mental Health * | |||
| Reference group | 59.80 | 3.35 | <0.001 |
| Weight 61–80 kg | 65.97 (6.17) | 2.67 | 0.021 |
| Weight >80 kg | 57.53 (−2.27) | 3.87 | 0.565 |
| Married/Cohabitant | 51.75 (−8.05) | 3.18 | 0.014 |
| Separated/Divorced/Widow | 50.96 (−8.84) | 4.79 | 0.062 |
| Inactive worker (for health reasons) | 41.69 (−18.11) | 4.37 | <0.001 |
| VD group | 75.52 (15.72) | 2.56 | <0.001 |
| Fatigue Severity Scale | |||
| Reference group | 2.98 | 0.34 | <0.001 |
| EDSS single-point increase | (0.30) | 0.05 | <0.001 |
| Age 31–45 | 4.12 (1.15) | 0.32 | <0.001 |
| Age 46–70 | 4.15 (1.17) | 0.34 | <0.001 |
| Weight 61–80 kg | 2.88 (−0.1) | 0.21 | 0.649 |
| Weight > 80 kg | 3.93 (0.95) | 0.31 | 0.003 |
| VD group | 1.89 (−1.09) | 0.21 | <0.001 |

References
- Thompson, A.J.; Baranzini, S.E.; Geurts, J.; Hemmer, B.; Ciccarelli, O. Multiple sclerosis. Lancet 2018, 391, 1622–1636. [Google Scholar] [CrossRef] [PubMed]
- Hagström, I.T.; Schneider, R.; Bellenberg, B.; Salmen, A.; Weiler, F.; Köster, O.; Gold, R.; Lukas, C. Relevance of early cervical cord volume loss in the disease evolution of clinically isolated syndrome and early multiple sclerosis: A 2-year follow-up study. J. Neurol. 2017, 264, 1402–1412. [Google Scholar] [CrossRef] [PubMed]
- Ruggieri, S.; Petracca, M.; de Giglio, L.; de Luca, F.; Giannì, C.; Gurreri, F.; Petsas, N.; Tommasin, S.; Pozzilli, C.; Pantano, P. A matter of atrophy: Differential impact of brain and spine damage on disability worsening in multiple sclerosis. J. Neurol. 2021, 268, 4698–4706. [Google Scholar] [CrossRef] [PubMed]
- Meyer-Moock, S.; Feng, Y.S.; Maeurer, M.; Dippel, F.W.; Kohlmann, T. Systematic literature review and validity evaluation of the Expanded Disability Status Scale (EDSS) and the Multiple Sclerosis Functional Composite (MSFC) in patients with multiple sclerosis. BMC Neurol. 2014, 14, 58. [Google Scholar] [CrossRef]
- Ochoa-Morales, A.; Hernández-Mojica, T.; Paz-Rodríguez, F.; Jara-Prado, A.; Trujillo-De Los Santos, Z.; Sánchez-Guzmán, M.A.; Guerrero-Camacho, J.L.; Corona-Vázquez, T.; Flores, J.; Camacho-Molina, A.; et al. Quality of life in patients with multiple sclerosis and its association with depressive symptoms and physical disability. Mult. Scler. Relat. Disord. 2019, 36, 101386. [Google Scholar] [CrossRef]
- Walton, C.; King, R.; Rechtman, L.; Kaye, W.; Leray, E.; Marrie, R.A.; Robertson, N.; La Rocca, N.; Uitdehaag, B.; Van Der Mei, I.; et al. Rising prevalence of multiple sclerosis worldwide: Insights from the Atlas of MS, third edition. Mult. Scler. J. 2020, 26, 1816–1820. [Google Scholar] [CrossRef]
- Paz-Zulueta, M.; Parás-Bravo, P.; Cantarero-Prieto, D.; Blázquez-Fernández, C.; Oterino-Durán, A. A literature review of cost-of-illness studies on the economic burden of multiple sclerosis. Mult. Scler. Relat. Disord. 2020, 43, 102162. [Google Scholar] [CrossRef]
- Solari, A.; Filippini, G.; Mendozzi, L.; Ghezzi, A.; Cifani, S.; Barbieri, E.; Baldini, S.; Salmaggi, A.; La Mantia, L.; Farinotti, M.; et al. Validation of Italian multiple sclerosis quality of life 54 questionnaire. J. Neurol. Neurosurg. Psychiatry 1999, 67, 158–162. [Google Scholar] [CrossRef]
- Vickrey, B.G.; Hays, R.D.; Harooni, R.; Myers, L.W.; Ellison, G.W. A health-related quality of life measure for multiple sclerosis. Qual. Life Res. 1995, 4, 187–206. [Google Scholar] [CrossRef]
- Dymecka, J.; Gerymski, R.; Tataruch, R.; Bidzan, M. Fatigue, Physical Disability and Self-Efficacy as Predictors of the Acceptance of Illness and Health-Related Quality of Life in Patients with Multiple Sclerosis. Int. J. Environ. Res. Public Health 2021, 18, 13237. [Google Scholar] [CrossRef]
- Torres-Costoso, A.; Martínez-Vizcaíno, V.; Reina-Gutiérrez, S.; Álvarez-Bueno, C.; Guzmán-Pavón, M.J.; Pozuelo-Carrascosa, D.P.; Fernández-Rodríguez, R.; Sanchez-López, M.; Cavero-Redondo, I. Effect of Exercise on Fatigue in Multiple Sclerosis: A Network Meta-analysis Comparing Different Types of Exercise. Arch. Phys. Med. Rehabil. 2021, 103, 970–987.e18. [Google Scholar] [CrossRef] [PubMed]
- Sellitto, G.; Morelli, A.; Bassano, S.; Conte, A.; Baione, V.; Galeoto, G.; Berardi, A. Outcome measures for physical fatigue in individuals with multiple sclerosis: A systematic review. Expert Rev. Pharmacoecon. Outcomes Res. 2021, 21, 625–646. [Google Scholar] [CrossRef] [PubMed]
- Induruwa, I.; Constantinescu, C.S.; Gran, B. Fatigue in multiple sclerosis—A brief review. J. Neurol. Sci. 2012, 323, 9–15. [Google Scholar] [CrossRef] [PubMed]
- Schwid, S.R.; Covington, M.; Segal, B.M.; Goodman, A.D. Fatigue in multiple sclerosis: Current understanding and future directions. J. Rehabil. Res. Dev. 2002, 39, 211–224. [Google Scholar]
- Krupp, L.B.; LaRocca, N.G.; Muir-Nash, J.; Steinberg, A.D. The fatigue severity scale. Application to patients with multiple sclerosis and systemic lupus erythematosus. Arch. Neurol. 1989, 46, 1121–1123. [Google Scholar] [CrossRef]
- Rosti-Otajärvi, E.; Hämäläinen, P.; Wiksten, A.; Hakkarainen, T.; Ruutiainen, J. Validity and reliability of the Fatigue Severity Scale in Finnish multiple sclerosis patients. Brain Behav. 2017, 7, e00743. [Google Scholar] [CrossRef]
- Krupp, L.B.; Coyle, P.K.; Doscher, C.; Miller, A.; Cross, A.H.; Jandorf, L.; Halper, J.; Johnson, B.; Morgante, L.; Grimson, R. Fatigue therapy in multiple sclerosis: Results of a double-blind, randomized, parallel trial of amantadine, pemoline, and placebo. Neurology 1995, 45, 1956–1961. [Google Scholar] [CrossRef]
- Valko, P.O.; Bassetti, C.L.; Bloch, K.E.; Held, U.; Baumann, C.R. Validation of the Fatigue Severity Scale in a Swiss Cohort. Sleep 2008, 31, 1601–1607. [Google Scholar] [CrossRef]
- Ghasemi, N.; Razavi, S.; Nikzad, E. Multiple Sclerosis: Pathogenesis, Symptoms, Diagnoses and Cell-Based Therapy. Cell J. 2017, 19, 1–10. [Google Scholar]
- de Angelis, F.; John, N.A.; Brownlee, W.J. Disease-modifying therapies for multiple sclerosis. BMJ 2018, 363, k4674. [Google Scholar] [CrossRef]
- Comi, G.; Radaelli, M.; Soelberg Sørensen, P. Evolving concepts in the treatment of relapsing multiple sclerosis. Lancet 2017, 389, 1347–1356. [Google Scholar] [CrossRef] [PubMed]
- Henze, T.; Rieckmann, P.; Toyka, K.V. Symptomatic Treatment of Multiple Sclerosis. Eur. Neurol. 2006, 56, 78–105. [Google Scholar] [CrossRef] [PubMed]
- Toosy, A.; Ciccarelli, O.; Thompson, A. Symptomatic treatment and management of multiple sclerosis. Handb. Clin. Neurol. 2014, 122, 513–562. [Google Scholar] [PubMed]
- Olsson, T.; Barcellos, L.F.; Alfredsson, L. Interactions between genetic, lifestyle and environmental risk factors for multiple sclerosis. Nat. Rev. Neurol. 2017, 13, 25–36. [Google Scholar] [CrossRef] [PubMed]
- Bjornevik, K.; Cortese, M.; Healy, B.C.; Kuhle, J.; Mina, M.J.; Leng, Y.; Elledge, S.J.; Niebuhr, D.W.; Scher, A.I.; Munger, K.L.; et al. Longitudinal analysis reveals high prevalence of Epstein-Barr virus associated with multiple sclerosis. Science 2022, 375, 296–301. [Google Scholar] [CrossRef] [PubMed]
- Munger, K.L.; Levin, L.I.; Hollis, B.W.; Howard, N.S.; Ascherio, A. Serum 25-Hydroxyvitamin D Levels and Risk of Multiple Sclerosis. JAMA 2006, 296, 2832. [Google Scholar] [CrossRef]
- McKay, K.A.; Jahanfar, S.; Duggan, T.; Tkachuk, S.; Tremlett, H. Factors associated with onset, relapses or progression in multiple sclerosis: A systematic review. Neurotoxicology 2017, 61, 189–212. [Google Scholar] [CrossRef]
- Ascherio, A.; Munger, K.L.; White, R.; Köchert, K.; Simon, K.C.; Polman, C.H.; Freedman, M.S.; Hartung, H.-P.; Miller, D.H.; Montalban, X.; et al. Vitamin D as an Early Predictor of Multiple Sclerosis Activity and Progression. JAMA Neurol. 2014, 71, 306–314. [Google Scholar] [CrossRef]
- Simpson-Yap, S.; Jelinek, P.; Weiland, T.; Nag, N.; Neate, S.; Jelinek, G. Self-reported use of vitamin D supplements is associated with higher physical quality of life scores in multiple sclerosis. Mult. Scler. Relat. Disord. 2021, 49, 102760. [Google Scholar] [CrossRef]
- Ashtari, F.; Toghianifar, N.; Zarkesh-Esfahani, S.H.; Mansourian, M. High dose Vitamin D intake and quality of life in relapsing-remitting multiple sclerosis: A randomized, double-blind, placebo-controlled clinical trial. Neurol. Res. 2016, 38, 888–892. [Google Scholar] [CrossRef]
- Fattizzo, B.; Zaninoni, A.; Giannotta, J.A.; Binda, F.; Cortelezzi, A.; Barcellini, W. Reduced 25-OH vitamin D in patients with autoimmune cytopenias, clinical correlations and literature review. Autoimmun. Rev. 2016, 15, 770–775. [Google Scholar] [CrossRef] [PubMed]
- Goischke, H.K. Vitamin D supplementation for the prevention or depletion of side effects of therapy with alemtuzumab in multiple sclerosis. Ther. Clin. Risk Manag. 2019, 15, 891–904. [Google Scholar] [CrossRef] [PubMed]
- Sintzel, M.B.; Rametta, M.; Reder, A.T. Vitamin D and Multiple Sclerosis: A Comprehensive Review. Neurol. Ther. 2018, 7, 59–85. [Google Scholar] [CrossRef]
- Holick, M.F.; Binkley, N.C.; Bischoff-Ferrari, H.A.; Gordon, C.M.; Hanley, D.A.; Heaney, R.P.; Murad, M.H.; Weaver, C.M. Evaluation, Treatment, and Prevention of Vitamin D Deficiency: An Endocrine Society Clinical Practice Guideline. J. Clin. Endocrinol. Metab. 2011, 96, 1911–1930. [Google Scholar] [CrossRef]
- Lemke, D.; Klement, R.J.; Schweiger, F.; Schweiger, B.; Spitz, J. Vitamin D Resistance as a Possible Cause of Autoimmune Diseases: A Hypothesis Confirmed by a Therapeutic High-Dose Vitamin D Protocol. Front. Immunol. 2021, 12, 655739. [Google Scholar] [CrossRef] [PubMed]
- Scazzone, C.; Agnello, L.; Bivona, G.; Lo Sasso, B.; Ciaccio, M. Vitamin D and Genetic Susceptibility to Multiple Sclerosis. Biochem. Genet. 2021, 59, 1–30. [Google Scholar] [CrossRef]
- Smolders, J.; Peelen, E.; Thewissen, M.; Cohen Tervaert, J.W.; Menheere, P.; Hupperts, R.; Damoiseaux, J. Safety and T Cell Modulating Effects of High Dose Vitamin D3 Supplementation in Multiple Sclerosis. PLoS ONE 2010, 5, e15235. [Google Scholar] [CrossRef] [PubMed]
- Kimball, S.M.; Ursell, M.R.; O’Connor, P.; Vieth, R. Safety of vitamin D3 in adults with multiple sclerosis. Am. J. Clin. Nutr. 2007, 86, 645–651. [Google Scholar] [CrossRef] [PubMed]
- Burton, J.M.; Kimball, S.; Vieth, R.; Bar-Or, A.; Dosch, H.M.; Cheung, R.; Gagne, D.; D’Souza, C.; Ursell, M.; O’Connor, P. A phase I/II dose-escalation trial of vitamin D3 and calcium in multiple sclerosis. Neurology 2010, 74, 1852–1859. [Google Scholar] [CrossRef]
- Thompson, A.J.; Banwell, B.L.; Barkhof, F.; Carroll, W.M.; Coetzee, T.; Comi, G.; Correale, J.; Fazekas, F.; Filippi, M.; Freedman, M.S.; et al. Diagnosis of multiple sclerosis: 2017 revisions of the McDonald criteria. Lancet Neurol. 2018, 17, 162–173. [Google Scholar] [CrossRef]
- Efron, B.; Tibshirani, R.J. Regression Models. In An Introduction to the Bootstrap; Champan & Hall CRC: Boca Raton, FL, USA, 1994; pp. 105–121. [Google Scholar]
- Azzalini, A.; Scarpa, B. Data Analysis and Data Mining: An Introduction—Chapter 3; OUP: New York, NY, USA, 2012. [Google Scholar]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing [Internet]: Vienna, Austria, 2021; Available online: https://www.R-project.org/ (accessed on 20 December 2022).
- Beckmann, Y.; Türe, S.; Duman, S.U. Vitamin D deficiency and its association with fatigue and quality of life in multiple sclerosis patients. EPMA J. 2020, 11, 65–72. [Google Scholar] [CrossRef] [PubMed]
- Głąbska, D.; Kołota, A.; Lachowicz, K.; Skolmowska, D.; Stachoń, M.; Guzek, D. Vitamin D Supplementation and Mental Health in Multiple Sclerosis Patients: A Systematic Review. Nutrients 2021, 13, 4207. [Google Scholar] [CrossRef] [PubMed]
- Boltjes, R.; Knippenberg, S.; Gerlach, O.; Hupperts, R.; Damoiseaux, J. Vitamin D supplementation in multiple sclerosis: An expert opinion based on the review of current evidence. Expert Rev. Neurother. 2021, 21, 715–725. [Google Scholar] [CrossRef]
- Bhargava, P.; Steele, S.U.; Waubant, E.; Revirajan, N.R.; Marcus, J.; Dembele, M.; Cassard, S.D.; Hollis, B.W.; Crainiceanu, C.; Mowry, E.M. Multiple sclerosis patients have a diminished serologic response to vitamin D supplementation compared to healthy controls. Mult. Scler. J. 2016, 22, 753–760. [Google Scholar] [CrossRef] [PubMed]
- Graves, J.S.; Barcellos, L.F.; Krupp, L.; Belman, A.; Shao, X.; Quach, H.; Hart, J.; Chitnis, T.; Weinstock-Guttman, B.; Aaen, G.; et al. Vitamin D genes influence MS relapses in children. Mult. Scler. J. 2020, 26, 894–901. [Google Scholar] [CrossRef] [PubMed]
- Mimpen, M.; Rolf, L.; Poelmans, G.; van den Ouweland, J.; Hupperts, R.; Damoiseaux, J.; Smolders, J. Vitamin D related genetic polymorphisms affect serological response to high-dose vitamin D supplementation in multiple sclerosis. PLoS ONE 2021, 16, e0261097. [Google Scholar] [CrossRef]
- Mahtani, R.; Nair, P.M.K. Daily oral vitamin D3 without concomitant therapy in the management of psoriasis: A case series. Clin. Immunol. Commun. 2022, 2, 17–22. [Google Scholar] [CrossRef]
- Etemadifar, M.; Janghorbani, M. Efficacy of high-dose vitamin D3 supplementation in vitamin D deficient pregnant women with multiple sclerosis: Preliminary findings of a randomized-controlled trial. Iran. J. Neurol. 2015, 14, 67–73. [Google Scholar] [PubMed]
- Hupperts, R.; Smolders, J.; Vieth, R.; Holmøy, T.; Marhardt, K.; Schluep, M.; Killestein, J.; Barkhof, F.; Beelke, M.; Grimaldi, L.M.; et al. Randomized trial of daily high-dose vitamin D 3 in patients with RRMS receiving subcutaneous interferon β-1a. Neurology 2019, 93, e1906–e1916. [Google Scholar] [CrossRef]
- Toghianifar, N.; Ashtari, F.; Zarkesh-Esfahani, S.H.; Mansourian, M. Effect of high dose vitamin D intake on interleukin-17 levels in multiple sclerosis: A randomized, double-blind, placebo-controlled clinical trial. J. Neuroimmunol. 2015, 285, 125–128. [Google Scholar] [CrossRef]
- Milovanovic, J.; Arsenijevic, A.; Stojanovic, B.; Kanjevac, T.; Arsenijevic, D.; Radosavljevic, G.; Milovanovic, M.; Arsenijevic, N. Interleukin-17 in Chronic Inflammatory Neurological Diseases. Front. Immunol. 2020, 11, 947. [Google Scholar] [CrossRef] [PubMed]
- Berrigan, L.I.; Fisk, J.D.; Patten, S.B.; Tremlett, H.; Wolfson, C.; Warren, S.; Fiest, K.M.; McKay, K.A.; Marrie, R.A.; For the CIHR Team in the Epidemiology and Impact of Comorbidity on Multiple Sclerosis (ECoMS). Health-related quality of life in multiple sclerosis. Neurology 2016, 86, 1417–1424. [Google Scholar] [CrossRef] [PubMed]
- Motl, R.W.; McAuley, E.; Snook, E.M.; Gliottoni, R.C. Physical activity and quality of life in multiple sclerosis: Intermediary roles of disability, fatigue, mood, pain, self-efficacy and social support. Psychol. Health Med. 2009, 14, 111–124. [Google Scholar] [CrossRef] [PubMed]
- Sakkas, G.K.; Giannaki, C.D.; Karatzaferi, C.; Manconi, M. Sleep Abnormalities in Multiple Sclerosis. Curr. Treat. Options Neurol. 2019, 21, 4. [Google Scholar] [CrossRef] [PubMed]
- Dauwan, M.; Begemann, M.J.H.; Slot, M.I.E.; Lee, E.H.M.; Scheltens, P.; Sommer, I.E.C. Physical exercise improves quality of life, depressive symptoms, and cognition across chronic brain disorders: A transdiagnostic systematic review and meta-analysis of randomized controlled trials. J. Neurol. 2021, 268, 1222–1246. [Google Scholar] [CrossRef]
- Sotirchos, E.S.; Bhargava, P.; Eckstein, C.; van Haren, K.; Baynes, M.; Ntranos, A.; Gocke, A.; Steinman, L.; Mowry, E.M.; Calabresi, P.A. Safety and immunologic effects of high-vs low-dose cholecalciferol in multiple sclerosis. Neurology 2016, 86, 382–390. [Google Scholar] [CrossRef] [PubMed]
- Amon, U.; Yaguboglu, R.; Ennis, M.; Holick, M.F.; Amon, J. Safety Data in Patients with Autoimmune Diseases during Treatment with High Doses of Vitamin D3 According to the “Coimbra Protocol”. Nutrients 2022, 14, 1575. [Google Scholar] [CrossRef]





| Variable | Groups | DMT Only | VD Only | DMT+VD | No Treatment | Total VD Patients Per Class (%) | p-Value | p-Value (VD Only and DMT Only) |
|---|---|---|---|---|---|---|---|---|
| Age | 18–30 | 8 | 22 | 3 | 1 | 25 (73.5) | 0.01 | 0.014 |
| 31–45 | 48 | 63 | 20 | 27 | 83 (52.5) | |||
| 46–70 | 51 | 40 | 13 | 28 | 53 (40.2) | |||
| Sex | Male | 16 | 31 | 14 | 12 | 45 (61.6) | 0.024 | 0.09 |
| Female | 91 | 94 | 22 | 44 | 116 (46.2) | |||
| Weight | 40–60 kg | 51 | 58 | 12 | 22 | 70 (49) | 0.369 | 0.184 |
| 61–80 kg | 38 | 55 | 17 | 26 | 72 (52.9) | |||
| >80 kg | 18 | 12 | 7 | 8 | 19 (42.2) | |||
| Years since diagnosis | 0–10 | 60 | 64 | 24 | 19 | 88 (52.7) | 0.041 | 0.463 |
| 11–20 | 28 | 42 | 6 | 22 | 48 (49) | |||
| >20 | 19 | 19 | 6 | 15 | 25 (42.4) | |||
| Marital status | Single | 18 | 30 | 15 | 11 | 45 (60.8) | <0.001 | 0.016 |
| Married/Cohabitant | 71 | 88 | 17 | 44 | 105 (47.7) | |||
| Separated/Divorced/Widow | 18 | 7 | 4 | 1 | 11 (36.7) | |||
| Employment status | Active worker/unemployed/inactive worker (for reasons not related to the health status) | 93 | 118 | 33 | 41 | 151 (53.0) | <0.001 | 0.08 |
| Inactive worker (for health reasons) | 14 | 7 | 3 | 15 | 10 (25.6) | |||
| Disease phenotype | Relapsing–remitting | 92 | 106 | 25 | 33 | 131 (51.1) | <0.001 | 0.946 |
| Progressive | 15 | 19 | 11 | 23 | 30 (44.1) | |||
| EDSS | 0–3.5 | 73 | 101 | 24 | 29 | 125 (55.1) | 0.001 | 0.04 |
| ≥4.0 | 34 | 24 | 12 | 27 | 36 (37.1) |
| Mean TPH (Diff. from Reference) | Standard Error | p-Value | |
|---|---|---|---|
| Reference group | 76.53 | 3.80 | <0.001 |
| EDSS single point increase | (−4.70) * | 0.46 | <0.001 |
| Age 31–45 years | 71.80 (−4.73) | 3.04 | 0.120 |
| Age 46–70 years | 69.51 (−7.02) | 3.22 | 0.030 |
| Weight 61–80 kg | 79.53 (3.00) | 1.91 | 0.117 |
| Weight > 80 kg | 72.13 (−4.41) | 2.71 | 0.105 |
| DMT group | 70.58 (−5.95) | 2.62 | 0.024 |
| VD group | 86.46 (9.92) | 2.65 | <0.001 |
| DMT+VD group | 77.03 (0.50) | 3.38 | 0.883 |
| Inactive worker (for health reasons) | 64.03 (−12.50) | 3.02 | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ianniello, A.; Sottosanti, A.; Borriello, G.; Vincenti, M. Perception of Quality of Life and Fatigue in Multiple Sclerosis Patients Treated with High-Dose Vitamin D. Clin. Transl. Neurosci. 2023, 7, 12. https://doi.org/10.3390/ctn7020012
Ianniello A, Sottosanti A, Borriello G, Vincenti M. Perception of Quality of Life and Fatigue in Multiple Sclerosis Patients Treated with High-Dose Vitamin D. Clinical and Translational Neuroscience. 2023; 7(2):12. https://doi.org/10.3390/ctn7020012
Chicago/Turabian StyleIanniello, Antonio, Andrea Sottosanti, Giovanna Borriello, and Massimo Vincenti. 2023. "Perception of Quality of Life and Fatigue in Multiple Sclerosis Patients Treated with High-Dose Vitamin D" Clinical and Translational Neuroscience 7, no. 2: 12. https://doi.org/10.3390/ctn7020012