
3D Printing of Dental Prostheses: Current and Emerging Applications

 , , ,
, , ,  ,
,  and
and
Abstract
:1. Introduction
2. General Overview of 3D Printing Techniques, Advantages, and Disadvantages
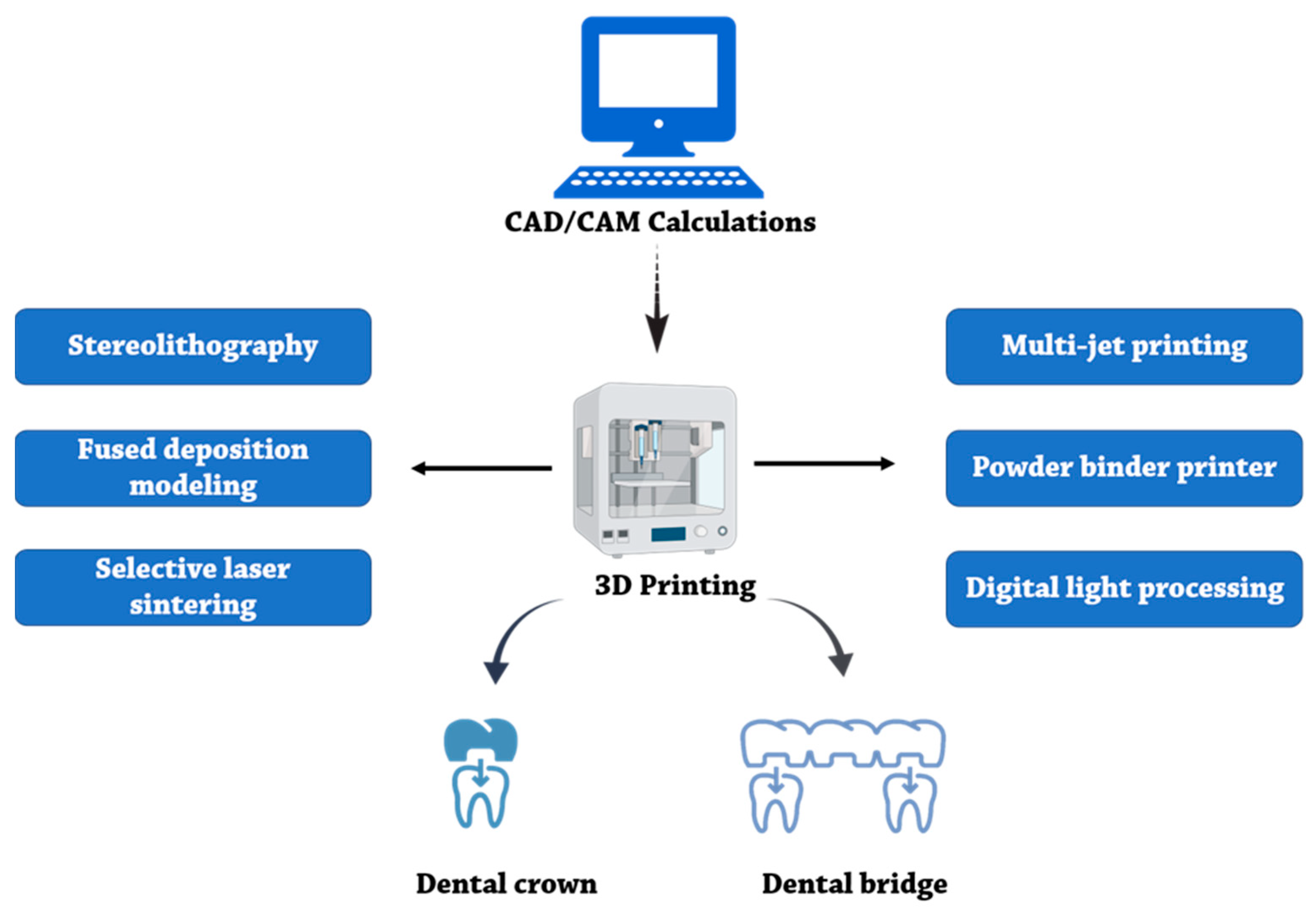
- Briefly, the extrusion-based methods employ a nozzle with a particular diameter to dispense the desired material in three axes, controlled by a computer. These methods rely on a continuous ejection of extruded material driven out of the nozzle, mechanically or pneumatically, to form a 3D structure at the centimeter scale [19]. In the FDM method, which is an extrusion-based technique, different materials, such as thermoplastic polymers, are melted and then driven out from the nozzle. The melting material deposition on the instrument support is concomitant with the cooling down of melted material, which is the main step for fabricating favorable 3D structures [20]. Extrusion-based techniques with low costs can quickly construct basic and less complex models. Recently, the use of microfluidics to develop the FDM method has been progressed. This gives them advantages, such as affordability and low cost. The application of microfluidic in the fabricating of dental prostheses development has attracted much attention [21].
- In the laser melting/sintering method, high-power pulsed laser light increases the temperature of specific areas to weld or sinter the added material on a three-axis moving stage. Using the SLS technique, a wide range of thermoplastic materials, including thermoplastic polymers, glass, ceramics, and metals, can be fused. Then, new surface layers can be created by refreshing the surfaces with a roller or blade. Finally, a powder form of material is applied to each sintered layer. One of the most important advantages of sintering techniques is that they lead to an autoclavable product that can be handled safely through common dental treatments [22]. The prostheses are easily duplicated at the dentistry office by applying computer-aided software and a desktop SLA 3D printer. This increases the rate and quality of manufacturing at a low moment [23].
- In the digital light processing (DLP) method, a projector light source cures the liquid resin layer-by-layer, and each layer is created upside down. To overcome problems during the DLP method, such as shrinkage or increasing the error when the size of the point out varies, the combination of DLP and FDM models has been proposed. The FDM accuracy for full-arched dental models and FDM inaccuracy for crown prostheses have been considered. So, a hybrid method of DLP (for special die) and FDM (for full dental model) is suggested [24].
- In the powder binder printers (PBP) method, the apparatus infiltrates pigmented liquid droplets layer-by-layer using an inkjet head [5]. However, utilizing biocompatible powders in tissue engineering is important. Calcium phosphate-based materials, as a reactive component, will be a good material (because of their similarity to dental sources) for implant applications [25].
- Lastly, lithography-based techniques employ photopolymers as the printing material. These photopolymers are directly exposed to the laser or a UV light beam or via the lithography-based ceramic manufacturing technique, while the stage moves in different directions to obtain the 3D structure. In these techniques, motorizing mirrors help concentrate the light beam on the surfaces containing the photoreactive liquid resin meant to be fused. Then, the curved surface is recoated by a wiper. This process is followed by another fusion step to infiltrate or stain the particular areas of the printed material [22]. These photopolymers have various properties, such as elemental composition microstructure and fracture mechanics. Ucar et al. compared these features in three products. The lithography ceramic-based technique was the most promising [26].
2.1. Three-Dimensional Printing and Modeling
2.2. Three-Dimensional Materials Characteristics
3. Application of 3D Printing in Dental Prostheses
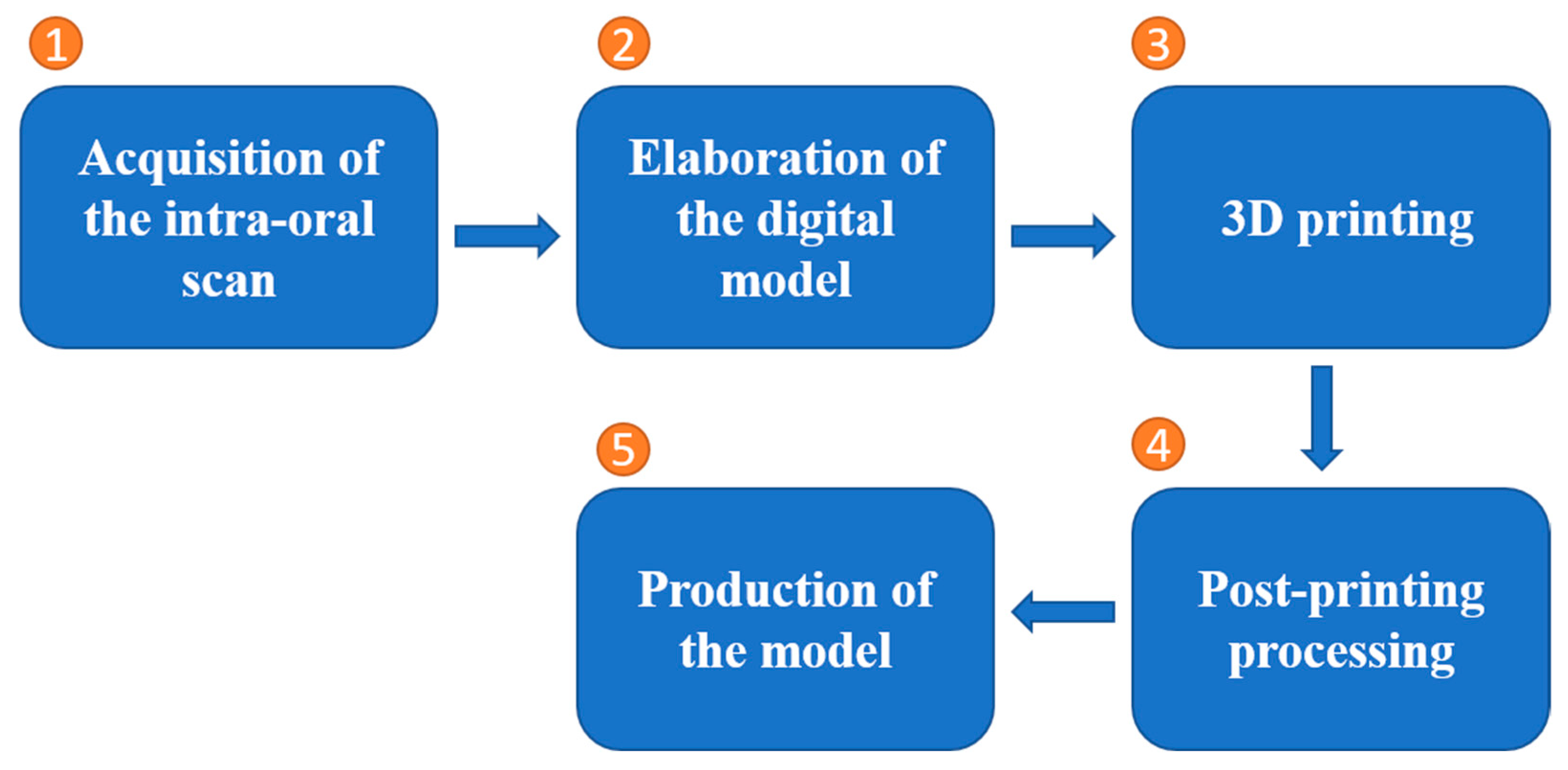
- Digital 3D scan of the patient’s jaw and teeth: The first step in fabricating a surgical guide using 3D printing is to obtain a digital 3D scan of the patient’s jaw and teeth. This can be achieved using a variety of technologies, including CBCT and intraoral scanners.
- Design of the surgical guide: Once a digital 3D scan has been obtained, the next step is to design the surgical guide using specialized software. This involves creating a virtual model of the patient’s jaw and teeth and then planning the placement of the dental implants based on the specific needs of the patient.
- Slicing the digital model: The next step is to slice the digital model of the surgical guide into layers, which can then be exported to the 3D printer. This process involves specifying the thickness of the layers and the type of 3D printing technology to be used.
- 3D printing: The slice data is then sent to the 3D printer, which creates a physical model of the surgical guide using a variety of materials, such as plastic or metal.
- Post-processing: Once the surgical guide has been printed, it may need to be post-processed, in order to smooth out any rough edges and ensure that it is accurate and ready for use. This may involve sanding, polishing, and sterilizing the guide.
- Use in surgery: The surgical guide is then used during the actual implant surgery to accurately position the implants in the jawbone. The guide helps the surgeon to place the implants in the correct location, ensuring that they are properly aligned and positioned for optimal function.
4. Dental 3D Printing Materials
4.1. Thermoplastic Polymers
4.2. Ceramics
4.3. Metals
4.4. Others
5. Prospects and Conclusions
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Abduo, J.; Lyons, K.; Bennamoun, M. Trends in computer-aided manufacturing in prosthodontics: A review of the available streams. Int. J. Dent. 2014, 2014, 783948. [Google Scholar] [CrossRef] [Green Version]
- Mainjot, A.; Dupont, N.; Oudkerk, J.; Dewael, T.; Sadoun, M. From artisanal to CAD-CAM blocks: State of the art of indirect composites. J. Dent. Res. 2016, 95, 487–495. [Google Scholar] [CrossRef]
- Cicciù, M.; Fiorillo, L.; Herford, A.S.; Crimi, S.; Bianchi, A.; D’Amico, C.; Laino, L.; Cervino, G. Bioactive Titanium Surfaces: Interactions of Eukaryotic and Prokaryotic Cells of Nano Devices Applied to Dental Practice. Biomedicines 2019, 7, 12. [Google Scholar] [CrossRef] [Green Version]
- Kim, J.-E.; Choi, W.-H.; Lee, D.; Shin, Y.; Park, S.-H.; Roh, B.-D.; Kim, D. Color and translucency stability of three-Dimensional printable dental materials for crown and bridge restorations. Materials 2021, 14, 650. [Google Scholar] [CrossRef]
- Dawood, A.; Marti, B.M.; Sauret-Jackson, V.; Darwood, A. 3D printing in dentistry. Br. Dent. J. 2015, 219, 521. [Google Scholar] [CrossRef]
- Stansbury, J.W.; Idacavage, M.J. 3D printing with polymers: Challenges among expanding options and opportunities. Dent. Mater. 2016, 32, 54–64. [Google Scholar] [CrossRef]
- Guilak, F.; Butler, D.L.; Goldstein, S.A.; Baaijens, F.P. Biomechanics and mechanobiology in functional tissue engineering. J. Biomech. 2014, 47, 1933–1940. [Google Scholar] [CrossRef] [Green Version]
- Nayar, S.; Bhuminathan, S.; Bhat, W.M. Rapid prototyping and stereolithography in dentistry. J. Pharm. Bioallied Sci. 2015, 7, S216. [Google Scholar] [CrossRef]
- Tasaka, A.; Shimizu, T.; Kato, Y.; Okano, H.; Ida, Y.; Higuchi, S.; Yamashita, S. Accuracy of removable partial denture framework fabricated by casting with a 3D printed pattern and selective laser sintering. J. Prosthodont. Res. 2019, 64, 224–230. [Google Scholar] [CrossRef]
- Salmi, M.; Paloheimo, K.-S.; Tuomi, J.; Ingman, T.; Mäkitie, A. A digital process for additive manufacturing of occlusal splints: A clinical pilot study. J. R. Soc. Interface 2013, 10, 20130203. [Google Scholar] [CrossRef]
- Kalberer, N.; Mehl, A.; Schimmel, M.; Müller, F.; Srinivasan, M. CAD-CAM milled versus rapidly prototyped (3D-printed) complete dentures: An in vitro evaluation of trueness. J. Prosthet. Dent. 2019, 121, 637–643. [Google Scholar] [CrossRef] [PubMed]
- Di Giacomo, G.d.A.; Cury, P.R.; da Silva, A.M.; da Silva, J.V.; Ajzen, S.A. A selective laser sintering prototype guide used to fabricate immediate interim fixed complete arch prostheses in flapless dental implant surgery: Technique description and clinical results. J. Prosthet. Dent. 2016, 116, 874–879. [Google Scholar] [CrossRef] [PubMed]
- Tserovski, S.; Georgieva, S.; Simeonov, R.; Bigdeli, A.; Röttinger, H.; Kinov, P. Advantages and disadvantages of 3D printing for pre-operative planning of revision hip surgery. J. Surg. Case Rep. 2019, 2019, rjz214. [Google Scholar] [CrossRef] [PubMed]
- Nakamura, K.; Harada, A.; Inagaki, R.; Kanno, T.; Niwano, Y.; Milleding, P.; Örtengren, U. Fracture resistance of monolithic zirconia molar crowns with reduced thickness. Acta Odontol. Scand. 2015, 73, 602–608. [Google Scholar] [CrossRef] [Green Version]
- Taira, Y.; Odatsu, T.; Sawase, T. Effects of a fluoride etchant and a phosphate primer on bonding of veneering composite to Ti–6Al–4V alloy for CAD/CAM restorations. J. Prosthodont. Res. 2013, 57, 30–35. [Google Scholar] [CrossRef] [Green Version]
- Lauvahutanon, S.; Takahashi, H.; Oki, M.; Arksornnukit, M.; Kanehira, M.; Finger, W.J. In vitro evaluation of the wear resistance of composite resin blocks for CAD/CAM. Dent. Mater. J. 2015, 34, 495–502. [Google Scholar] [CrossRef] [Green Version]
- Sachs, E.M.; Haggerty, J.S.; Cima, M.J.; Williams, P.A. Three-Dimensional Printing Techniques. Google Patents US5204055A, 20 April 1993. [Google Scholar]
- Etemad-Shahidi, Y.; Qallandar, O.B.; Evenden, J.; Alifui-Segbaya, F.; Ahmed, K.E. Accuracy of 3-Dimensionally Printed Full-Arch Dental Models: A Systematic Review. J. Clin. Med. 2020, 9, 3357. [Google Scholar] [CrossRef]
- Chameettachal, S.; Yeleswarapu, S.; Sasikumar, S.; Shukla, P.; Hibare, P.; Bera, A.K.; Bojedla, S.S.R.; Pati, F. 3D Bioprinting: Recent Trends and Challenges. J. Indian Inst. Sci. 2019, 99, 375–403. [Google Scholar] [CrossRef]
- Carneiro, O.S.; Silva, A.; Gomes, R. Fused deposition modeling with polypropylene. Mater. Des. 2015, 83, 768–776. [Google Scholar] [CrossRef]
- Tiboni, M.; Tiboni, M.; Pierro, A.; Del Papa, M.; Sparaventi, S.; Cespi, M.; Casettari, L. Microfluidics for nanomedicines manufacturing: An affordable and low-cost 3D printing approach. Int. J. Pharm. 2021, 599, 120464. [Google Scholar] [CrossRef]
- Shah, P.; Chong, B. 3D imaging, 3D printing and 3D virtual planning in endodontics. Clin. Oral Investig. 2018, 22, 641–654. [Google Scholar] [CrossRef] [PubMed]
- Lin, W.-S.; Harris, B.T.; Morton, D. Use of CBCT Imaging, Open-Source Modeling Software, and Desktop Stereolithography 3D Printing to Duplicate a Removable Dental Prosthesis-A Proof of Concept. Compend. Contin. Educ. Dent. 2017, 38, e5–e8. [Google Scholar] [PubMed]
- Lee, D.; Lee, S.Y.; Kim, H.; Park, C. A Hybrid Dental Model Concept Utilizing Fused Deposition Modeling and Digital Light Processing 3D Printing. Int. J. Prosthodont. 2020, 33, 229–231. [Google Scholar] [CrossRef] [PubMed]
- Khalyfa, A.; Vogt, S.; Weisser, J.; Grimm, G.; Rechtenbach, A.; Meyer, W.; Schnabelrauch, M. Development of a new calcium phosphate powder-binder system for the 3D printing of patient specific implants. J. Mater. Sci. Mater. Med. 2007, 18, 909–916. [Google Scholar] [CrossRef]
- Uçar, Y.; Aysan Meriç, İ.; Ekren, O. Layered manufacturing of dental ceramics: Fracture mechanics, microstructure, and elemental composition of lithography-sintered ceramic. J. Prosthodont. 2019, 28, e310–e318. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pillai, S.; Upadhyay, A.; Khayambashi, P.; Farooq, I.; Sabri, H.; Tarar, M.; Lee, K.T.; Harb, I.; Zhou, S.; Wang, Y. Dental 3D-printing: Transferring art from the laboratories to the clinics. Polymers 2021, 13, 157. [Google Scholar] [CrossRef]
- Ackerman, S.; Aguilera, F.C.; Buie, J.M.; Glickman, G.N.; Umorin, M.; Wang, Q.; Jalali, P. Accuracy of 3-dimensional–printed endodontic surgical guide: A human cadaver study. J. Endod. 2019, 45, 615–618. [Google Scholar] [CrossRef]
- Buda, M.; Bratos, M.; Sorensen, J.A. Accuracy of 3-dimensional computer-aided manufactured single-tooth implant definitive casts. J. Prosthet. Dent. 2018, 120, 913–918. [Google Scholar] [CrossRef]
- Zhang, Z.-c.; Li, P.-l.; Chu, F.-t.; Shen, G. Influence of the three-dimensional printing technique and printing layer thickness on model accuracy. J. Orofac. Orthop. 2019, 80, 194–204. [Google Scholar] [CrossRef]
- Yang, W.-f.; Choi, W.S.; Leung, Y.Y.; Curtin, J.P.; Du, R.; Zhang, C.-y.; Chen, X.-s.; Su, Y.-x. Three-dimensional printing of patient-specific surgical plates in head and neck reconstruction: A prospective pilot study. Oral Oncol. 2018, 78, 31–36. [Google Scholar] [CrossRef]
- Lavorgna, L.; Cervino, G.; Fiorillo, L.; Di Leo, G.; Troiano, G.; Ortensi, M.; Galantucci, L.; Cicciù, M. Reliability of a virtual prosthodontic project realized through a 2d and 3d photographic acquisition: An experimental study on the accuracy of different digital systems. Int. J. Environ. Res. Public Health 2019, 16, 5139. [Google Scholar] [CrossRef] [Green Version]
- Takeuchi, Y.; Koizumi, H.; Furuchi, M.; Sato, Y.; Ohkubo, C.; Matsumura, H. Use of digital impression systems with intraoral scanners for fabricating restorations and fixed dental prostheses. J. Oral Sci. 2018, 60, 1–7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Revilla-León, M.; Umorin, M.; Özcan, M.; Piedra-Cascón, W. Color dimensions of additive manufactured interim restorative dental material. J. Prosthet. Dent. 2020, 123, 754–760. [Google Scholar] [CrossRef] [PubMed]
- Lüchtenborg, J.; Burkhardt, F.; Nold, J.; Rothlauf, S.; Wesemann, C.; Pieralli, S.; Wemken, G.; Witkowski, S.; Spies, B.C. Implementation of Fused Filament Fabrication in Dentistry. Appl. Sci. 2021, 11, 6444. [Google Scholar] [CrossRef]
- Yoo, S.-Y.; Kim, S.-K.; Heo, S.-J.; Koak, J.-Y.; Kim, J.-G. Dimensional Accuracy of Dental Models for Three-Unit Prostheses Fabricated by Various 3D Printing Technologies. Materials 2021, 14, 1550. [Google Scholar] [CrossRef]
- Jeong, Y.-G.; Lee, W.-S.; Lee, K.-B. Accuracy evaluation of dental models manufactured by CAD/CAM milling method and 3D printing method. J. Adv. Prosthodont. 2018, 10, 245–251. [Google Scholar] [CrossRef] [Green Version]
- Xie, Z.; Gao, M.; Lobo, A.O.; Webster, T.J. 3D bioprinting in tissue engineering for medical applications: The classic and the hybrid. Polymers 2020, 12, 1717. [Google Scholar] [CrossRef]
- Mikolajczyk, T.; Malinowski, T.; Moldovan, L.; Fuwen, H.; Paczkowski, T.; Ciobanu, I. CAD CAM system for manufacturing innovative hybrid design using 3D printing. Procedia Manuf. 2019, 32, 22–28. [Google Scholar] [CrossRef]
- Harris, B.T.; Montero, D.; Grant, G.T.; Morton, D.; Llop, D.R.; Lin, W.-S. Creation of a 3-dimensional virtual dental patient for computer-guided surgery and CAD-CAM interim complete removable and fixed dental prostheses: A clinical report. J. Prosthet. Dent. 2017, 117, 197–204. [Google Scholar] [CrossRef]
- Joo, H.-S.; Park, S.-W.; Yun, K.-D.; Lim, H.-P. Complete-mouth rehabilitation using a 3D printing technique and the CAD/CAM double scanning method: A clinical report. J. Prosthet. Dent. 2016, 116, 3–7. [Google Scholar] [CrossRef]
- Oğuz, E.İ.; Kılıçarslan, M.A.; Ocak, M.; Bilecenoğlu, B.; Ekici, Z. Marginal and internal fit of feldspathic ceramic CAD/CAM crowns fabricated via different extraoral digitization methods: A micro-computed tomography analysis. Odontology 2021, 109, 440–447. [Google Scholar] [CrossRef] [PubMed]
- Abdullah, A.O.; Tsitrou, E.A.; Pollington, S. Comparative in vitro evaluation of CAD/CAM vs conventional provisional crowns. J. Appl. Oral Sci. 2016, 24, 258–263. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yao, J.; Li, J.; Wang, Y.; Huang, H. Comparison of the flexural strength and marginal accuracy of traditional and CAD/CAM interim materials before and after thermal cycling. J. Prosthet. Dent. 2014, 112, 649–657. [Google Scholar] [CrossRef]
- Cousley, R.R. Introducing 3D printing in your orthodontic practice. J. Orthod. 2020, 47, 265–272. [Google Scholar] [CrossRef] [PubMed]
- Straub, J. Initial work on the characterization of additive manufacturing (3D printing) using software image analysis. Machines 2015, 3, 55–71. [Google Scholar] [CrossRef] [Green Version]
- Sheela, U.B.; Usha, P.G.; Joseph, M.M.; Melo, J.S.; Nair, S.T.T.; Tripathi, A. 3D printing in dental implants. In 3D Printing in Medicine and Surgery; Elsevier: Amsterdam, The Netherlands, 2021; pp. 83–104. [Google Scholar]
- Londono, J.; Tadros, M.; Salgueiro, M.; Baker, P.S. Digital design and 3D printing of an implant-supported prosthetic stent for protecting complete arch soft tissue grafts around dental implants: A dental technique. J. Prosthet. Dent. 2018, 120, 801–804. [Google Scholar] [CrossRef]
- Ellakany, P.; Al-Harbi, F.; El Tantawi, M.; Mohsen, C. Evaluation of the accuracy of digital and 3D-printed casts compared with conventional stone casts. J. Prosthet. Dent. 2022, 127, 438–444. [Google Scholar] [CrossRef]
- Marei, H.F.; Alshaia, A.; Alarifi, S.; Almasoud, N.; Abdelhady, A. Effect of steam heat sterilization on the accuracy of 3D printed surgical guides. Implant. Dent. 2019, 28, 372–377. [Google Scholar] [CrossRef]
- Kalaivani, G.; Balaji, V.R.; Manikandan, D.; Rohini, G. Expectation and reality of guided implant surgery protocol using computer-assisted static and dynamic navigation system at present scenario: Evidence-based literature review. J. Indian Soc. Periodontol. 2020, 24, 398. [Google Scholar] [CrossRef]
- Bell, C.K.; Sahl, E.F.; Kim, Y.J.; Rice, D.D. Accuracy of Implants Placed with Surgical Guides: Thermoplastic Versus 3D Printed. Int. J. Periodontics Restor. Dent. 2018, 38, 113–119. [Google Scholar] [CrossRef]
- Block, M.S.; Emery, R.W.; Lank, K.; Ryan, J. Implant Placement Accuracy Using Dynamic Navigation. Int. J. Oral Maxillofac. Implant. 2017, 32. [Google Scholar] [CrossRef] [PubMed]
- Tartaglia, G.M.; Mapelli, A.; Maspero, C.; Santaniello, T.; Serafin, M.; Farronato, M.; Caprioglio, A. Direct 3D printing of clear orthodontic aligners: Current state and future possibilities. Materials 2021, 14, 1799. [Google Scholar] [CrossRef] [PubMed]
- Martorelli, M.; Gerbino, S.; Giudice, M.; Ausiello, P. A comparison between customized clear and removable orthodontic appliances manufactured using RP and CNC techniques. Dent. Mater. 2013, 29, e1–e10. [Google Scholar] [CrossRef] [PubMed]
- Schweiger, J.; Edelhoff, D.; Güth, J.-F. 3D printing in digital prosthetic dentistry: An overview of recent developments in additive manufacturing. J. Clin. Med. 2021, 10, 2010. [Google Scholar] [CrossRef]
- Mai, H.-N.; Lee, K.-B.; Lee, D.-H. Fit of interim crowns fabricated using photopolymer-jetting 3D printing. J. Prosthet. Dent. 2017, 118, 208–215. [Google Scholar] [CrossRef]
- Alharbi, N.; Alharbi, S.; Cuijpers, V.M.; Osman, R.B.; Wismeijer, D. Three-dimensional evaluation of marginal and internal fit of 3D-printed interim restorations fabricated on different finish line designs. J. Prosthodont. Res. 2018, 62, 218–226. [Google Scholar] [CrossRef]
- Papadiochou, S.; Pissiotis, A.L. Marginal adaptation and CAD-CAM technology: A systematic review of restorative material and fabrication techniques. J. Prosthet. Dent. 2018, 119, 545–551. [Google Scholar] [CrossRef]
- Joshi, N. Physical and Optical Properties of Provisional Crown and Bridge Materials Fabricated Using CAD/CAM Milling or 3D Printing Technology; Nova Southeastern University: Fort Lauderdale, FL, USA, 2019. [Google Scholar]
- Shin, J.-W.; Kim, J.-E.; Choi, Y.-J.; Shin, S.-H.; Nam, N.-E.; Shim, J.-S.; Lee, K.-W. Evaluation of the Color Stability of 3D-Printed Crown and Bridge Materials against Various Sources of Discoloration: An In Vitro Study. Materials 2020, 13, 5359. [Google Scholar] [CrossRef]
- De Oliveira, D.C.R.S.; Ayres, A.P.A.; Rocha, M.G.; Giannini, M.; Puppin Rontani, R.M.; Ferracane, J.L.; Sinhoreti, M.A.C. Effect of different in vitro aging methods on color stability of a dental resin-based composite using CIELAB and CIEDE 2000 color-difference formulas. J. Esthet. Dent. 2015, 27, 322–330. [Google Scholar] [CrossRef]
- Dozic, A.; Voit, N.F.; Zwartser, R.; Khashayar, G.; Aartman, I. Color coverage of a newly developed system for color determination and reproduction in dentistry. J. Dent. 2010, 38, e50–e56. [Google Scholar] [CrossRef]
- Karatas, O.; Gul, P.; Akgul, N.; Celik, N.; Gundogdu, M.; Duymus, Z.Y.; Seven, N. Effect of staining and bleaching on the microhardness, surface roughness and color of different composite resins. Dent. Med. Probl. 2021, 58, 369–376. [Google Scholar] [CrossRef] [PubMed]
- Schestatsky, R.; Zucuni, C.P.; Dapieve, K.S.; Burgo, T.A.L.; Spazzin, A.O.; Bacchi, A.; Valandro, L.F.; Pereira, G.K.R. Microstructure, topography, surface roughness, fractal dimension, internal and marginal adaptation of pressed and milled lithium-disilicate monolithic restorations. J. Prosthodont. Res. 2019, 64, 12–19. [Google Scholar] [CrossRef] [PubMed]
- Sabbah, A.; Romanos, G.; Delgado-Ruiz, R. Impact of Layer Thickness and Storage Time on the Properties of 3D-Printed Dental Dies. Materials 2021, 14, 509. [Google Scholar] [CrossRef] [PubMed]
- Arnold, C.; Monsees, D.; Hey, J.; Schweyen, R. Surface quality of 3D-printed models as a function of various printing parameters. Materials 2019, 12, 1970. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jain, S.; Sayed, M.; Ahmed, W.M.; Halawi, A.H.A.; Najmi, N.M.A.; Aggarwal, A.; Bhandi, S.; Patil, S. An In-Vitro Study to Evaluate the Effect of Denture Cleansing Agents on Color Stability of Denture Bases Fabricated Using CAD/CAM Milling, 3D-Printing and Conventional Techniques. Coatings 2021, 11, 962. [Google Scholar] [CrossRef]
- Warnecki, M.; Sarul, M.; Kozakiewicz, M.; Zięty, A.; Babiarczuk, B.; Kawala, B.; Jurczyszyn, K. Surface Evaluation of Aligners after Immersion in Coca-Cola and Orange Juice. Materials 2022, 15, 6341. [Google Scholar] [CrossRef]
- Kovacev, N.; Li, S.; Essa, K. Effect of the preparation techniques of photopolymerizable ceramic slurry and printing parameters on the accuracy of 3D printed lattice structures. J. Eur. Ceram. Soc. 2021, 41, 7734–7743. [Google Scholar] [CrossRef]
- Khosravani, M.R.; Berto, F.; Ayatollahi, M.R.; Reinicke, T. Characterization of 3D-printed PLA parts with different raster orientations and printing speeds. Sci. Rep. 2022, 12, 1016. [Google Scholar] [CrossRef]
- Huang, Z.; Zhang, L.; Zhu, J.; Zhao, Y.; Zhang, X. Clinical marginal and internal fit of crowns fabricated using different CAD/CAM technologies. J. Prosthodont. 2015, 24, 291–295. [Google Scholar] [CrossRef]
- Al Deeb, L.; Al Ahdal, K.; Alotaibi, G.; Alshehri, A.; Alotaibi, B.; Alabdulwahab, F.; Al Deeb, M.; AlFawaz, Y.F.; Vohra, F.; Abduljabbar, T. Marginal Integrity, Internal Adaptation and Compressive Strength of 3D Printed, Computer Aided Design and Computer Aided Manufacture and Conventional Interim Fixed Partial Dentures. J. Biomater. Tissue Eng. 2019, 9, 1745–1750. [Google Scholar] [CrossRef]
- Tian, Y.; Chen, C.; Xu, X.; Wang, J.; Hou, X.; Li, K.; Lu, X.; Shi, H.; Lee, E.-S.; Jiang, H.B. A review of 3D printing in dentistry: Technologies, affecting factors, and applications. Scanning 2021, 2021, 9950131. [Google Scholar] [CrossRef] [PubMed]
- Vasiliu, R.-D.; Porojan, S.D.; Porojan, L. In Vitro Study of Comparative Evaluation of Marginal and Internal Fit between Heat-Pressed and CAD-CAM Monolithic Glass-Ceramic Restorations after Thermal Aging. Materials 2020, 13, 4239. [Google Scholar] [CrossRef]
- Lee, W.-S.; Lee, D.-H.; Lee, K.-B. Evaluation of internal fit of interim crown fabricated with CAD/CAM milling and 3D printing system. J. Adv. Prosthodont. 2017, 9, 265. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tahayeri, A.; Morgan, M.; Fugolin, A.P.; Bompolaki, D.; Athirasala, A.; Pfeifer, C.S.; Ferracane, J.L.; Bertassoni, L.E. 3D printed versus conventionally cured provisional crown and bridge dental materials. Dent. Mater. 2018, 34, 192–200. [Google Scholar] [CrossRef] [PubMed]
- Yang, M.; Zeng, Q.; Vieira, M.P.; Olsson, B. Three-Dimensional Printing in Dentistry: An Advanced Technology for Craniofacial Regeneration. In Mesenchymal Stem Cells and Craniofacial Regeneration; Bentham Science Publishers: Sharjah, United Arab Emirates, 2016; pp. 33–59. [Google Scholar]
- Ashtiani, R.E.; Khanlar, L.N.; Mahshid, M.; Moshaverinia, A. Comparison of dimensional accuracy of conventionally and digitally manufactured intracoronal restorations. J. Prosthet. Dent. 2018, 119, 233–238. [Google Scholar] [CrossRef]
- Homsy, F.R.; Özcan, M.; Khoury, M.; Majzoub, Z.A. Marginal and internal fit of pressed lithium disilicate inlays fabricated with milling, 3D printing, and conventional technologies. J. Prosthet. Dent. 2018, 119, 783–790. [Google Scholar] [CrossRef]
- Chaturvedi, S.; Alqahtani, N.M.; Addas, M.K.; Alfarsi, M.A. Marginal and internal fit of provisional crowns fabricated using 3D printing technology. Technol. Health Care 2020, 28, 635–642. [Google Scholar] [CrossRef]
- Fathi, H.M.; Al-Masoody, A.H.; El-Ghezawi, N.; Johnson, A. The Accuracy of Fit of Crowns Made From Wax Patterns Produced Conventionally (Hand Formed) and Via CAD/CAM Technology. Eur. J. Prosthodont. Restor. Dent. 2016, 24, 10–17. [Google Scholar]
- Zimmermann, M.; Ender, A.; Egli, G.; Özcan, M.; Mehl, A. Fracture load of CAD/CAM-fabricated and 3D-printed composite crowns as a function of material thickness. Clin. Oral Investig. 2019, 23, 2777–2784. [Google Scholar] [CrossRef] [Green Version]
- Çakmak, G.; Cuellar, A.R.; Donmez, M.B.; Schimmel, M.; Abou-Ayash, S.; Lu, W.-E.; Yilmaz, B. Effect of Printing Layer Thickness on the Trueness and Margin Quality of 3D-Printed Interim Dental Crowns. Appl. Sci. 2021, 11, 9246. [Google Scholar] [CrossRef]
- Ebert, J.; Özkol, E.; Zeichner, A.; Uibel, K.; Weiss, Ö.; Koops, U.; Telle, R.; Fischer, H. Direct inkjet printing of dental prostheses made of zirconia. J. Dent. Res. 2009, 88, 673–676. [Google Scholar] [CrossRef] [PubMed]
- Zhao, M.; Geng, Y.; Fan, S.; Yao, X.; Zhu, M.; Zhang, Y. 3D-Printed Strong Hybrid Materials with Low Shrinkage for Dental Restoration. Compos. Sci. Technol. 2021, 213, 108902. [Google Scholar] [CrossRef]
- Wesemann, C.; Spies, B.C.; Sterzenbach, G.; Beuer, F.; Kohal, R.; Wemken, G.; Krügel, M.; Pieralli, S. Polymers for conventional, subtractive, and additive manufacturing of occlusal devices differ in hardness and flexural properties but not in wear resistance. Dent. Mater. 2021, 37, 432–442. [Google Scholar] [CrossRef] [PubMed]
- Firlej, M.; Pieniak, D.; Niewczas, A.M.; Walczak, A.; Domagała, I.; Borucka, A.; Przystupa, K.; Igielska-Kalwat, J.; Jarosz, W.; Biedziak, B. Effect of Artificial Aging on Mechanical and Tribological Properties of CAD/CAM Composite Materials Used in Dentistry. Materials 2021, 14, 4678. [Google Scholar] [CrossRef]
- Oliver, W.C.; Pharr, G.M. Measurement of hardness and elastic modulus by instrumented indentation: Advances in understanding and refinements to methodology. J. Mater. Res. 2004, 19, 3–20. [Google Scholar] [CrossRef]
- Hardiman, M.; Vaughan, T.J.; McCarthy, C.T. The effects of pile-up, viscoelasticity and hydrostatic stress on polymer matrix nanoindentation. Polym. Test. 2016, 52, 157–166. [Google Scholar] [CrossRef] [Green Version]
- Son, K.; Lee, J.-H.; Lee, K.-B. Comparison of intaglio surface trueness of interim dental crowns fabricated with SLA 3D printing, DLP 3D printing, and milling technologies. Healthcare 2021, 9, 983. [Google Scholar] [CrossRef]
- Moraru, E.; Besnea, D.; Dontu, O.; Gheorghe, G.I.; Constantin, V. Applications of additive technologies in realization of customized dental prosthesesr. Int. J. Mechatron. Appl. Mech. 2018, 3, 66–71. [Google Scholar]
- Galeva, H.; Uzunov, T.; Sofronov, Y.; Todorov, G. Accuracy evaluation of fixed prosthetic constructions made by milling and printing technologies and the influence of temperature changes. J. Phys. Conf. Ser. 2021, 1859, 012064. [Google Scholar] [CrossRef]
- Mohajeri, M.; Khazaei, S.; Vafaee, F.; Firouz, F.; Gholiabad, S.G.; Shisheian, A. Marginal Fit of Temporary Restorations Fabricated by the Conventional Chairside Method, 3D Printing, and Milling. Front. Dent. 2021, 18, 31. [Google Scholar] [CrossRef]
- Ryu, J.-E.; Kim, Y.-L.; Kong, H.-J.; Chang, H.-S.; Jung, J.-H. Marginal and internal fit of 3D printed provisional crowns according to build directions. J. Adv. Prosthodont. 2020, 12, 225. [Google Scholar] [CrossRef] [PubMed]
- Lee, B.-I.; You, S.-G.; You, S.-M.; Kim, D.-Y.; Kim, J.-H. Evaluating the accuracy (trueness and precision) of interim crowns manufactured using digital light processing according to post-curing time: An in vitro study. J. Adv. Prosthodont. 2021, 13, 89. [Google Scholar] [CrossRef] [PubMed]
- Yu, B.-Y.; Son, K.; Lee, K.-B. Evaluation of intaglio surface trueness and margin quality of interim crowns in accordance with the build angle of stereolithography apparatus 3-dimensional printing. J. Prosthet. Dent. 2021, 126, 231–237. [Google Scholar] [CrossRef]
- Galante, R.; Figueiredo-Pina, C.G.; Serro, A.P. Additive manufacturing of ceramics for dental applications: A review. Dent. Mater. 2019, 35, 825–846. [Google Scholar] [CrossRef] [PubMed]
- Alqahtani, A.S.; AlFadda, A.M.; Eldesouky, M.; Alnuwaiser, M.K.; Al-Saleh, S.; Alresayes, S.; Alshahrani, A.; Vohra, F.; Abduljabbar, T. Comparison of Marginal Integrity and Surface Roughness of Selective Laser Melting, CAD-CAM and Digital Light Processing Manufactured Co-Cr Alloy Copings. Appl. Sci. 2021, 11, 8328. [Google Scholar] [CrossRef]
- Veeman, D.; Sai, M.S.; Sureshkumar, P.; Jagadeesha, T.; Natrayan, L.; Ravichandran, M.; Mammo, W.D. Additive manufacturing of biopolymers for tissue engineering and regenerative medicine: An overview, potential applications, advancements, and trends. Int. J. Polym. Sci. 2021, 2021, 4907027. [Google Scholar] [CrossRef]
- Karamifar, K.; Tondari, A.; Saghiri, M.A. Endodontic periapical lesion: An overview on the etiology, diagnosis and current treatment Modalities. Eur. Endod. J. 2020, 5, 54. [Google Scholar] [CrossRef]
- Kowsari, K.; Akbari, S.; Wang, D.; Fang, N.X.; Ge, Q. High-efficiency high-resolution multimaterial fabrication for digital light processing-based three-dimensional printing. 3D Print. Addit. Manuf. 2018, 5, 185–193. [Google Scholar] [CrossRef]
- Javaid, M.; Haleem, A. Current status and applications of additive manufacturing in dentistry: A literature-based review. J. Oral Biol. Craniofac. Res. 2019, 9, 179–185. [Google Scholar] [CrossRef]
- Jin, M.-C.; Yoon, H.-I.; Yeo, I.-S.; Kim, S.-H.; Han, J.-S. The effect of build angle on the tissue surface adaptation of maxillary and mandibular complete denture bases manufactured by digital light processing. J. Prosthet. Dent. 2020, 123, 473–482. [Google Scholar] [CrossRef]
- D’Souza, K.M.; Aras, M.A. Types of implant surgical guides in dentistry: A review. J. Oral Implantol. 2012, 38, 643–652. [Google Scholar] [CrossRef] [PubMed]
- Kim, T.; Lee, S.; Kim, G.B.; Hong, D.; Kwon, J.; Park, J.-w.; Kim, N. Accuracy of a simplified 3D-printed implant surgical guide. J. Prosthet. Dent. 2020, 124, 195–201.e2. [Google Scholar] [CrossRef] [PubMed]
- Miljanovic, D.; Seyedmahmoudian, M.; Horan, B.; Stojcevski, A. Novel and accurate 3D-Printed surgical guide for mandibular reconstruction with integrated dental implants. Comput. Biol. Med. 2022, 151, 106327. [Google Scholar] [CrossRef] [PubMed]
- Yeung, M.; Abdulmajeed, A.; Carrico, C.K.; Deeb, G.R.; Bencharit, S. Accuracy and precision of 3D-printed implant surgical guides with different implant systems: An in vitro study. J. Prosthet. Dent. 2020, 123, 821–828. [Google Scholar] [CrossRef] [PubMed]
- Jindal, P.; Juneja, M.; Siena, F.L.; Bajaj, D.; Breedon, P. Mechanical and geometric properties of thermoformed and 3D printed clear dental aligners. Am. J. Orthod. Dentofac. Orthop. 2019, 156, 694–701. [Google Scholar] [CrossRef] [Green Version]
- Venezia, P.; Ronsivalle, V.; Rustico, L.; Barbato, E.; Leonardi, R.; Giudice, A.L. Accuracy of orthodontic models prototyped for clear aligners therapy: A 3D imaging analysis comparing different market segments 3D printing protocols. J. Dent. 2022, 124, 104212. [Google Scholar] [CrossRef]
- Zinelis, S.; Panayi, N.; Polychronis, G.; Papageorgiou, S.N.; Eliades, T. Comparative analysis of mechanical properties of orthodontic aligners produced by different contemporary 3D printers. Orthod. Craniofacial Res. 2022, 25, 336–341. [Google Scholar] [CrossRef]
- Mukai, S.; Mukai, E.; Santos-Junior, J.A.; Shibli, J.A.; Faveri, M.; Giro, G. Assessment of the reproducibility and precision of milling and 3D printing surgical guides. BMC Oral Health 2021, 21, 1. [Google Scholar] [CrossRef]
- Oh, K.C.; Park, J.-M.; Shim, J.-S.; Kim, J.-H.; Kim, J.-E.; Kim, J.-H. Assessment of metal sleeve-free 3D-printed implant surgical guides. Dent. Mater. 2019, 35, 468–476. [Google Scholar] [CrossRef]
- Kohal, R.J.; Klaus, G. A zirconia implant-crown system: A case report. Int. J. Periodontics Restor. Dent. 2004, 24, 147–153. [Google Scholar]
- Srinivasan, M.; Kalberer, N.; Fankhauser, N.; Naharro, M.; Maniewicz, S.; Müller, F. CAD-CAM complete removable dental prostheses: A double-blind, randomized, crossover clinical trial evaluating milled and 3D-printed dentures. J. Dent. 2021, 115, 103842. [Google Scholar] [CrossRef] [PubMed]
- Vlahović, Z.; Mikić, M. 3D printing guide implant placement: A case report. Balk. J. Dent. Med. 2017, 21, 65–68. [Google Scholar] [CrossRef] [Green Version]
- Park, J.-H.; Odkhuu, M.; Cho, S.; Li, J.; Park, B.-Y.; Kim, J.-W. 3D-printed titanium implant with pre-mounted dental implants for mandible reconstruction: A case report. Maxillofac. Plast. Reconstr. Surg. 2020, 42, 28. [Google Scholar] [CrossRef] [PubMed]
- Tsioukas, V.; Pikridas, C.; Karolos, I.-A. Challenges, opportunities, and limitations in 3D printing. 3d Print. Appl. Med. Surg. 2020, 1, 151–155. [Google Scholar]
- Martelli, N.; Serrano, C.; van den Brink, H.; Pineau, J.; Prognon, P.; Borget, I.; El Batti, S. Advantages and disadvantages of 3-dimensional printing in surgery: A systematic review. Surgery 2016, 159, 1485–1500. [Google Scholar] [CrossRef]
- Son, K.; Lee, K.-B. A novel method for precise guided hole fabrication of dental implant surgical guide fabricated with 3d printing technology. Appl. Sci. 2020, 11, 49. [Google Scholar] [CrossRef]
- Li, C.-H.; Wu, C.-H.; Lin, C.-L. Design of a patient-specific mandible reconstruction implant with dental prosthesis for metal 3D printing using integrated weighted topology optimization and finite element analysis. J. Mech. Behav. Biomed. Mater. 2020, 105, 103700. [Google Scholar] [CrossRef]
- Tamimi, F.; Torres, J.; Al-Abedalla, K.; Lopez-Cabarcos, E.; Alkhraisat, M.H.; Bassett, D.C.; Gbureck, U.; Barralet, J.E. Osseointegration of dental implants in 3D-printed synthetic onlay grafts customized according to bone metabolic activity in recipient site. Biomaterials 2014, 35, 5436–5445. [Google Scholar] [CrossRef]
- Zhang, F.; Spies, B.C.; Willems, E.; Inokoshi, M.; Wesemann, C.; Cokic, S.M.; Hache, B.; Kohal, R.J.; Altmann, B.; Vleugels, J.; et al. 3D printed zirconia dental implants with integrated directional surface pores combine mechanical strength with favorable osteoblast response. Acta Biomater. 2022, 150, 427–441. [Google Scholar] [CrossRef]
- Zandinejad, A.; Revilla-León, M.; Methani, M.M.; Nasiry Khanlar, L.; Morton, D. The Fracture Resistance of Additively Manufactured Monolithic Zirconia vs. Bi-Layered Alumina Toughened Zirconia Crowns When Cemented to Zirconia Abutments. Evaluating the Potential of 3D Printing of Ceramic Crowns: An In Vitro Study. Dent. J. 2021, 9, 115. [Google Scholar] [CrossRef]
- Zhang, L.; Liu, H.; Yao, H.; Zeng, Y.; Chen, J. Preparation, microstructure, and properties of ZrO2 (3Y)/Al2O3 bioceramics for 3D printing of all-ceramic dental implants by vat photopolymerization. Chin. J. Mech. Eng. Addit. Manuf. Front. 2022, 1, 100023. [Google Scholar] [CrossRef]
- Sampaio, C.S.; Niemann, K.D.; Schweitzer, D.D.; Hirata, R.; Atria, P.J. Microcomputed tomography evaluation of cement film thickness of veneers and crowns made with conventional and 3D printed provisional materials. J. Esthet. Restor. Dent. 2021, 33, 487–495. [Google Scholar] [CrossRef] [PubMed]
- Pugliese, R.; Beltrami, B.; Regondi, S.; Lunetta, C. Polymeric biomaterials for 3D printing in medicine: An overview. Ann. 3d Print. Med. 2021, 2, 100011. [Google Scholar] [CrossRef]
- Van Noort, R. The future of dental devices is digital. Dent. Mater. 2012, 28, 3–12. [Google Scholar] [CrossRef]
- Barazanchi, A.; Li, K.C.; Al-Amleh, B.; Lyons, K.; Waddell, J.N. Additive technology: Update on current materials and applications in dentistry. J. Prosthodont. 2017, 26, 156–163. [Google Scholar] [CrossRef]
- Pal, A.K.; Mohanty, A.K.; Misra, M. Additive manufacturing technology of polymeric materials for customized products: Recent developments and future prospective. RSC Adv. 2021, 11, 36398–36438. [Google Scholar] [CrossRef]
- Turner, B.N.; Strong, R.; Gold, S.A. A review of melt extrusion additive manufacturing processes: I. Process design and modeling. Rapid Prototyp. J. 2014, 20, 192–204. [Google Scholar] [CrossRef]
- Schönhoff, L.M.; Mayinger, F.; Eichberger, M.; Reznikova, E.; Stawarczyk, B. 3D printing of dental restorations: Mechanical properties of thermoplastic polymer materials. J. Mech. Behav. Biomed. Mater. 2021, 119, 104544. [Google Scholar] [CrossRef]
- Wieckiewicz, M.; Opitz, V.; Richter, G.; Boening, K.W. Physical properties of polyamide-12 versus PMMA denture base material. BioMed Res. Int. 2014, 2014, 150298. [Google Scholar] [CrossRef] [Green Version]
- Chen, Z.; Li, Z.; Li, J.; Liu, C.; Lao, C.; Fu, Y.; Liu, C.; Li, Y.; Wang, P.; He, Y. 3D printing of ceramics: A review. J. Eur. Ceram. Soc. 2019, 39, 661–687. [Google Scholar] [CrossRef]
- Malik, H.H.; Darwood, A.R.; Shaunak, S.; Kulatilake, P.; Abdulrahman, A.; Mulki, O.; Baskaradas, A. Three-dimensional printing in surgery: A review of current surgical applications. J. Surg. Res. 2015, 199, 512–522. [Google Scholar] [CrossRef] [PubMed]
- Bukhari, S.; Goodacre, B.J.; AlHelal, A.; Kattadiyil, M.T.; Richardson, P.M. Three-dimensional printing in contemporary fixed prosthodontics: A technique article. J. Prosthet. Dent. 2018, 119, 530–534. [Google Scholar] [CrossRef]
- Tang, Z.; Li, X.; Tan, Y.; Fan, H.; Zhang, X. The material and biological characteristics of osteoinductive calcium phosphate ceramics. Regen. Biomater. 2018, 5, 43–59. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Michna, S.; Wu, W.; Lewis, J.A. Concentrated hydroxyapatite inks for direct-write assembly of 3-D periodic scaffolds. Biomaterials 2005, 26, 5632–5639. [Google Scholar] [CrossRef] [PubMed]
- Tarafder, S.; Dernell, W.S.; Bandyopadhyay, A.; Bose, S. SrO-and MgO-doped microwave sintered 3D printed tricalcium phosphate scaffolds: Mechanical properties and in vivo osteogenesis in a rabbit model. J. Biomed. Mater. Res. Part B Appl. Biomater. 2015, 103, 679–690. [Google Scholar] [CrossRef] [PubMed]
- Obregon, F.; Vaquette, C.; Ivanovski, S.; Hutmacher, D.; Bertassoni, L. Three-dimensional bioprinting for regenerative dentistry and craniofacial tissue engineering. J. Dent. Res. 2015, 94, 143S–152S. [Google Scholar] [CrossRef] [PubMed]
- Miyazaki, T.; Nakamura, T.; Matsumura, H.; Ban, S.; Kobayashi, T. Current status of zirconia restoration. J. Prosthodont. Res. 2013, 57, 236–261. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hong, M.-H.; Min, B.K.; Kwon, T.-Y. Fabricating high-quality 3D-printed alloys for dental applications. Appl. Sci. 2017, 7, 710. [Google Scholar] [CrossRef] [Green Version]
- Vaicelyte, A.; Janssen, C.; Le Borgne, M.; Grosgogeat, B. Cobalt–Chromium Dental Alloys: Metal Exposures, Toxicological Risks, CMR Classification, and EU Regulatory Framework. Crystals 2020, 10, 1151. [Google Scholar] [CrossRef]
- Zhang, X.; Wei, L.C.; Wu, B.; Yu, L.Y.; Wang, X.P.; Liu, Y. A comparative analysis of metal allergens associated with dental alloy prostheses and the expression of HLA-DR in gingival tissue. Mol. Med. Rep. 2016, 13, 91–98. [Google Scholar] [CrossRef] [Green Version]
- Chua, K.; Khan, I.; Malhotra, R.; Zhu, D. Additive manufacturing and 3D printing of metallic biomaterials. Eng. Regen. 2022, 2, 288–299. [Google Scholar] [CrossRef]
- Osakada, K.; Shiomi, M. Flexible manufacturing of metallic products by selective laser melting of powder. Int. J. Mach. Tools Manuf. 2006, 46, 1188–1193. [Google Scholar] [CrossRef]
- Kathuria, Y. Microstructuring by selective laser sintering of metallic powder. Surf. Coat. Technol. 1999, 116, 643–647. [Google Scholar] [CrossRef]
- Konieczny, B.; Szczesio-Wlodarczyk, A.; Sokolowski, J.; Bociong, K. Challenges of Co–Cr alloy additive manufacturing methods in dentistry—The current state of knowledge (systematic review). Materials 2020, 13, 3524. [Google Scholar] [CrossRef] [PubMed]
- Frazier, W.E. Metal additive manufacturing: A review. J. Mater. Eng. Perform. 2014, 23, 1917–1928. [Google Scholar] [CrossRef]
- Sing, S.L.; Yeong, W.Y.; Wiria, F.E.; Tay, B.Y.; Zhao, Z.; Zhao, L.; Tian, Z.; Yang, S. Direct selective laser sintering and melting of ceramics: A review. Rapid Prototyp. J. 2017, 23, 611–623. [Google Scholar] [CrossRef]
- Moniz, L.; Chen, Q.; Guillemot, G.; Bellet, M.; Gandin, C.-A.; Colin, C.; Bartout, J.-D.; Berger, M.-H. Additive manufacturing of an oxide ceramic by laser beam melting—Comparison between finite element simulation and experimental results. J. Mater. Process. Technol. 2019, 270, 106–117. [Google Scholar] [CrossRef]
- Carrillo, M.H.; Lee, G.; Maniere, C.; Olevsky, E.A. Additive manufacturing of powder components based on subtractive sintering approach. Rapid Prototyp. J. 2021, 27, 1731–1736. [Google Scholar] [CrossRef]
- Thurzo, A.; Kočiš, F.; Novák, B.; Czako, L.; Varga, I. Three-dimensional modeling and 3D printing of biocompatible orthodontic power-arm design with clinical application. Appl. Sci. 2021, 11, 9693. [Google Scholar] [CrossRef]
- Revilla-León, M.; Besné-Torre, A.; Sánchez-Rubio, J.L.; Fábrega, J.J.; Özcan, M. Digital tools and 3D printing technologies integrated into the workflow of restorative treatment: A clinical report. J. Prosthet. Dent. 2019, 121, 3–8. [Google Scholar] [CrossRef] [Green Version]
- Jawahar, A.; Maragathavalli, G. Applications of 3D Printing in Dentistry–A Review. Int. J. Pharm. Sci. Res. 2019, 11, 1670–1675. [Google Scholar]
- Park, J.-Y.; Kim, H.-Y.; Kim, J.-H.; Kim, J.-H.; Kim, W.-C. Comparison of prosthetic models produced by traditional and additive manufacturing methods. J. Adv. Prosthodont. 2015, 7, 294–302. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Revilla-León, M.; Meyer, M.; Özcan, M. Metal additive manufacturing technologies: Literature review of current status and prosthodontic applications. Int. J. Comput. Dent. 2019, 22, 55–67. [Google Scholar] [PubMed]
- Bae, S.; Hong, M.-H.; Lee, H.; Lee, C.-H.; Hong, M.; Lee, J.; Lee, D.-H. Reliability of metal 3D printing with respect to the marginal fit of fixed dental prostheses: A systematic review and meta-analysis. Materials 2020, 13, 4781. [Google Scholar] [CrossRef]
- Balamurugan, P.; Selvakumar, N. Development of patient specific dental implant using 3D printing. J. Ambient. Intell. Humaniz. Comput. 2021, 12, 3549–3558. [Google Scholar] [CrossRef]
- Anadioti, E.; Musharbash, L.; Blatz, M.B.; Papavasiliou, G.; Kamposiora, P. 3D printed complete removable dental prostheses: A narrative review. BMC Oral Health 2020, 20, 343. [Google Scholar] [CrossRef]
- Jang, Y.; Sim, J.-Y.; Park, J.-K.; Kim, W.-C.; Kim, H.-Y.; Kim, J.-H. Accuracy of 3-unit fixed dental prostheses fabricated on 3D-printed casts. J. Prosthet. Dent. 2020, 123, 135–142. [Google Scholar] [CrossRef] [Green Version]
- Park, S.-M.; Park, J.-M.; Kim, S.-K.; Heo, S.-J.; Koak, J.-Y. Flexural strength of 3D-printing resin materials for provisional fixed dental prostheses. Materials 2020, 13, 3970. [Google Scholar] [CrossRef]
- Alageel, O. Three-dimensional printing technologies for dental prosthesis: A review. Rapid Prototyp. J. 2022, 28, 1764–1778. [Google Scholar] [CrossRef]
- Oliveira, T.T.; Reis, A.C. Fabrication of dental implants by the additive manufacturing method: A systematic review. J. Prosthet. Dent. 2019, 122, 270–274. [Google Scholar] [CrossRef]
- Yao, Q.; Morton, D.; Eckert, G.J.; Lin, W.-S. The effect of surface treatments on the color stability of CAD-CAM interim fixed dental prostheses. J. Prosthet. Dent. 2021, 126, 248–253. [Google Scholar] [CrossRef] [PubMed]
- Choonara, Y.E.; du Toit, L.C.; Kumar, P.; Kondiah, P.P.; Pillay, V. 3D-printing and the effect on medical costs: A new era? Expert Rev. Pharm. Outcomes Res. 2016, 16, 23–32. [Google Scholar] [CrossRef]
- Sun, J.; Zhang, F.Q. The application of rapid prototyping in prosthodontics. J. Prosthodont. Implant. Esthet. Reconstr. Dent. 2012, 21, 641–644. [Google Scholar] [CrossRef] [PubMed]
- Vasamsetty, P.; Pss, T.; Kukkala, D.; Singamshetty, M.; Gajula, S. 3D printing in dentistry–Exploring the new horizons. Mater. Today Proc. 2020, 26, 838–841. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Technique | Advantages | Disadvantages |
|---|---|---|
| FDM or FFF |
|
|
| DLP |
|
|
| SLA |
|
|
| MJP |
|
|
| SLS |
|
|
| SLM |
|
|
| Specimen | Fabrication Method | Resin | Mean Marginal Fit (µm) | Mean Internal Fit (µm) | Mechanical Properties | Ref./Authors/Year |
|---|---|---|---|---|---|---|
| Dental crown | 3D printing (Dentis) | ZMD-1000B | 91.1 | - | - | [76]/Lee et al./2017 |
| Dental crown and bridge | 3D printing | Dental crown and bridge | - | Elastic modulus = 1600 MPa (50 µm thickness), peak stress = 100 MPa (25 µm thickness) | [77]/Tahayeri et al./2018 | |
| Interim restorations | 3D printing (DW028D, DWS) | Temporis® composite | 28 (RSB) | 66 (KE) | - | [78]/Yang et al./2016 |
| Intracoronal restorations | 3D printing (Envision TEC) | WIC 300A envision | 10 | - | Intracoronal restorations | [79]/Ashtiani et al./2018 |
| Dental inlays | 3D printing (ProJet 1200) | Lithium disilicate | 39.7 | 88.8 | - | [80]/Homsy et al./2018 |
| Interim restorations | Stereolithography-based 3D printer (DW028D) | hybrid composite resin material (Temporis) | - | - | - | [58]/Alharbi et al./2018 |
| Dental crown | 3D printing | - | - | - | - | [81]/Chaturvedi et al./2020 |
| Interim crown | 3D polymer jetting (Object Eden 260VS; Stratasys) | VeroGlaze MED620 | 99 | 139 | - | [57]/Mai et al./2017 |
| Dental crown | 3D wax printing (3Z Lab, Solidscape) | Bego Crown Wax | 60 | 115 | - | [82]/Fathi et al./2016 |
| Dental crown | 3D printing (Freeform Pro 2, ASIGA) | Els-3D Harz | - | - | Mean fracture loading force = 1478.7 N | [83]/Zimmermann et al./2019 |
| Dental interim crown | DLP 3D printing (MoonRay S100) | Nextdent Crown and Bridge Micro Filled Hybrid-MFH | 100 | - | - | [84]/Çakmak et al./2021 |
| Dental Prostheses | Direct inkjet 3D printing | the ceramic suspension (zirconia powder, TZ-3YS-E) | - | - | - | [85]/Ebert et al./2009 |
| Dental crown | Stereolithographic 3D printing | Resin matrix Bis-GMA/ TEGDMA mixture with CQ and 4- EDMAB | - | - | - | [86]/Zhao et al./2021 |
| Dental crown | ASIGA UV MAX | Gr-17.1 temporary | - | - | - | [87,88]/Wesemann et al./2021 and Firlej et al./2021 |
| Dental crown | ASIGA UV MAX | GR-17 temporary | - | - | - | [88,89]/Firlej et al./2021 and Oliver et al./2004 |
| Dental crown | Phrozen Shuffle Lite 3D | NextDent SG Orange | - | - | - | [88,90]/Firlej et al./2021 and Hardiman. et al./2016 |
| Dental crown | Phrozen Shuffle Lite 3D | NextDent C&B MFH | - | - | - | [88]/Firlej et al./2021 |
| Dental Crowns | SLA 3D printing (ZENITH U) | Photopolymer resin ZMD-1000B | - | - | Intaglio surface trueness = 26.7 µm | [91]/Son et al./2021 |
| Dental Crowns | DLP 3D printing (RAYDENT Studio) | Photopolymer resin (RAYDENT C&B) | - | - | Intaglio surface trueness = 27.0 µm | [91]/Son et al./2021 |
| Dental prostheses | 3D DLP digital printing | Photopolymers | - | - | - | [92]/Moraru et al./2018 |
| Removable dental prostheses | Direct light processing (DLP) 3D printer (NextDent 5100) | Dimethacrylate-based | - | - | - | [68]/Jain et al./2021 |
| Dental pros-theses | 3D printing machine (STM 125) | Acrylic resin | 60 | - | - | [93]/Galeva et al.,/2021 |
| Dental crowns | Digital light processing printer (Prodent Labx, Product Bonyan Mecatronic, Tabriz, Iran) | UV resin (Freeprint Temp UV, Detax, Germany) | 91.40 | - | - | [94]/Mohajeri et al./2021 |
| Dental crowns | DLP-based 3D printer (Hunter, Flashforge Corp., Jinhua, China) | A5AN-500, Nissin Dental Products Inc., Kyoto, Japan | Because of different fabrication angles, there is more than one mean marginal/internal fit | [95]/Ryu et al./2020 | ||
| Dental crowns | DLP-type 3D printer (NextDent 5100, NextDent, Soesterberg, Netherlands) | PMMA resin liquid (NextDent C&B, NextDent, Soesterberg, Netherlands) | - | - | External surface; mean Trueness; 87.8 µm Intaglio surface; mean Trueness; 78.2 µm | [96]/Lee et al./2021 |
| Dental crowns | Dental SLA 3D printer (ZENITH U; ZENITH | ZMD-1000B Temporary; Dentis | - | - | - | [97]/Yu et al./2021 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rezaie, F.; Farshbaf, M.; Dahri, M.; Masjedi, M.; Maleki, R.; Amini, F.; Wirth, J.; Moharamzadeh, K.; Weber, F.E.; Tayebi, L. 3D Printing of Dental Prostheses: Current and Emerging Applications. J. Compos. Sci. 2023, 7, 80. https://doi.org/10.3390/jcs7020080
Rezaie F, Farshbaf M, Dahri M, Masjedi M, Maleki R, Amini F, Wirth J, Moharamzadeh K, Weber FE, Tayebi L. 3D Printing of Dental Prostheses: Current and Emerging Applications. Journal of Composites Science. 2023; 7(2):80. https://doi.org/10.3390/jcs7020080
Chicago/Turabian StyleRezaie, Fereshte, Masoud Farshbaf, Mohammad Dahri, Moein Masjedi, Reza Maleki, Fatemeh Amini, Jonathan Wirth, Keyvan Moharamzadeh, Franz E. Weber, and Lobat Tayebi. 2023. "3D Printing of Dental Prostheses: Current and Emerging Applications" Journal of Composites Science 7, no. 2: 80. https://doi.org/10.3390/jcs7020080