

Additive In-Time Manufacturing of Customised Orthoses

Abstract
:1. Introduction
2. Materials and Methods
3. Results
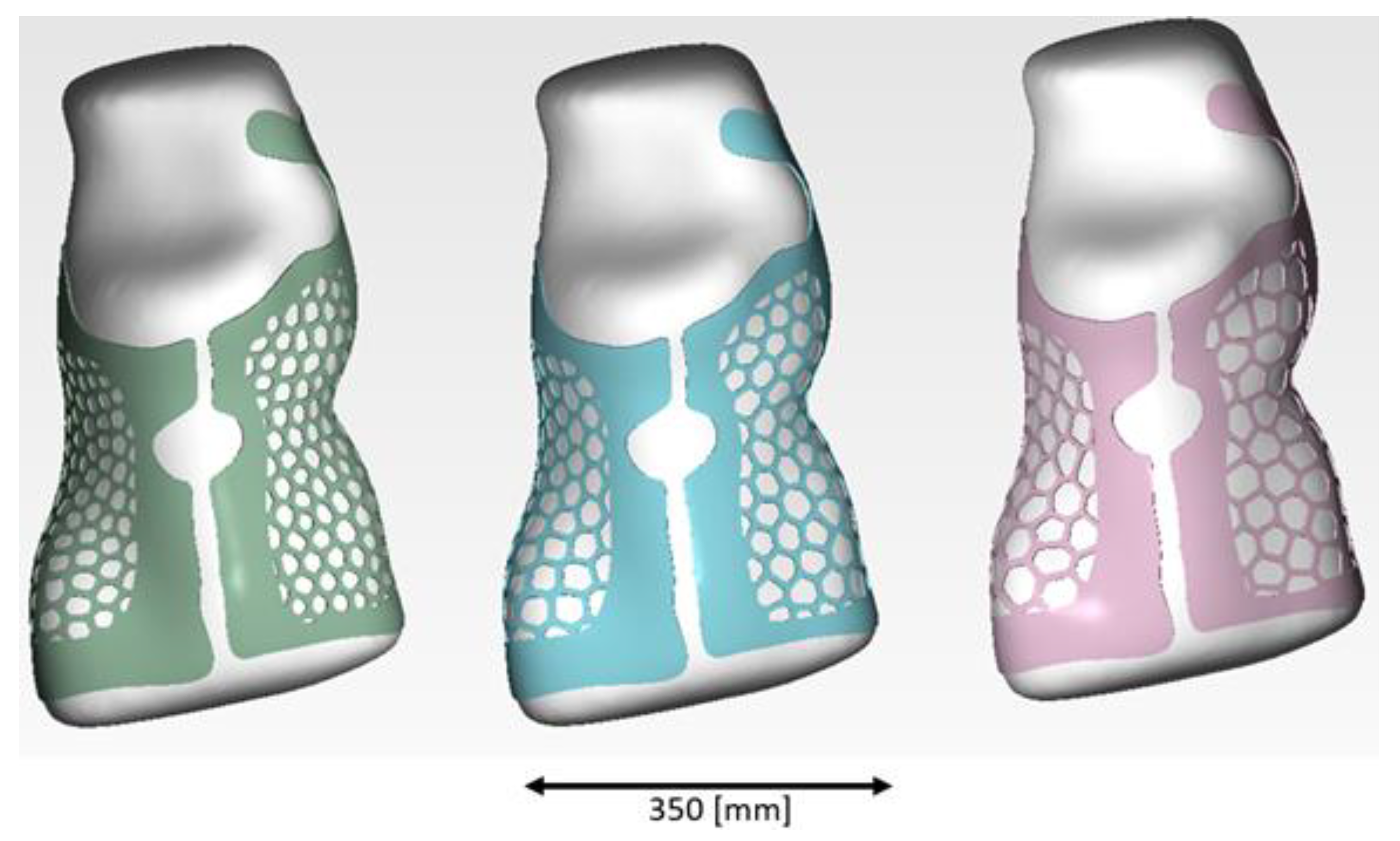
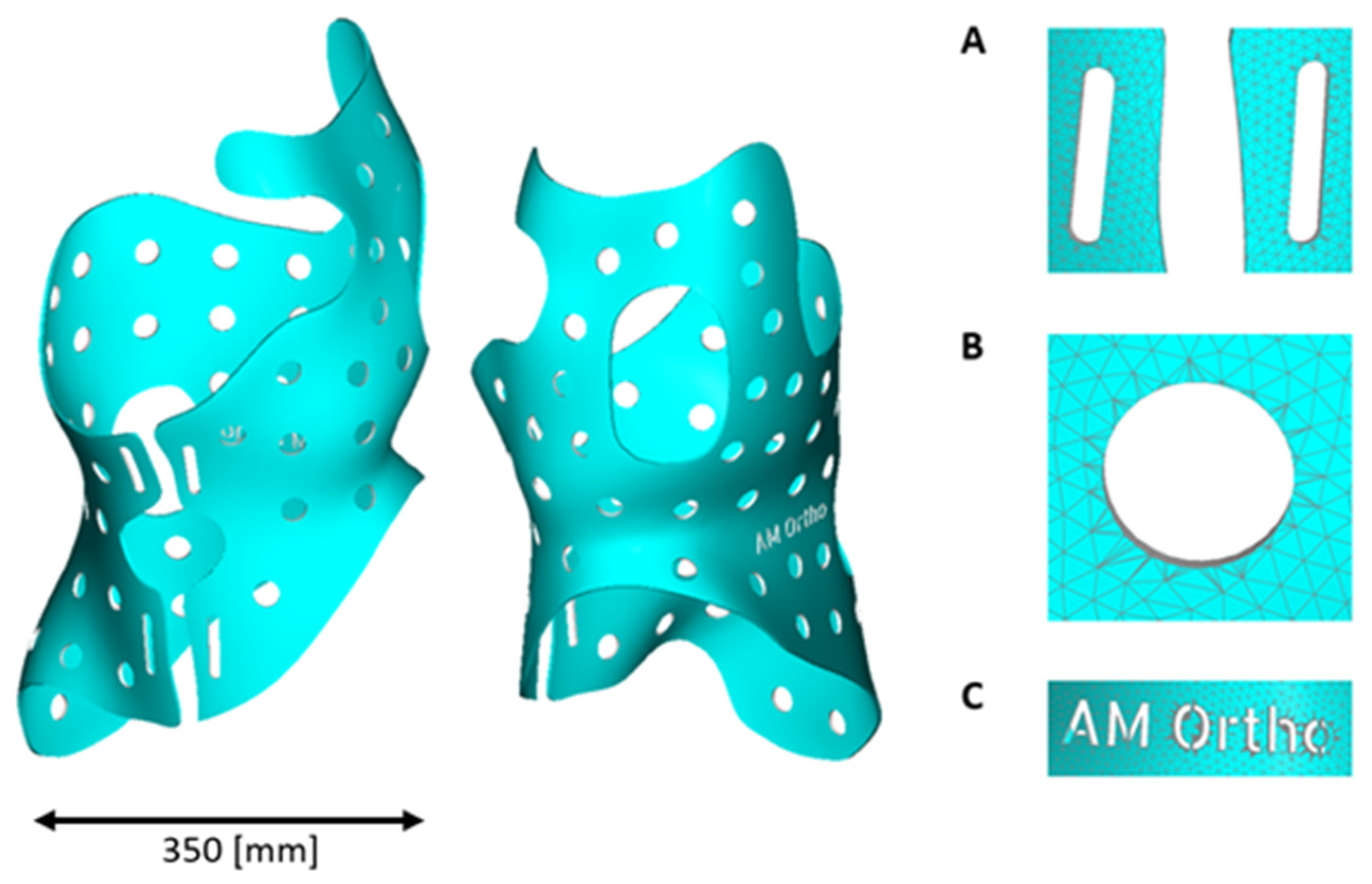
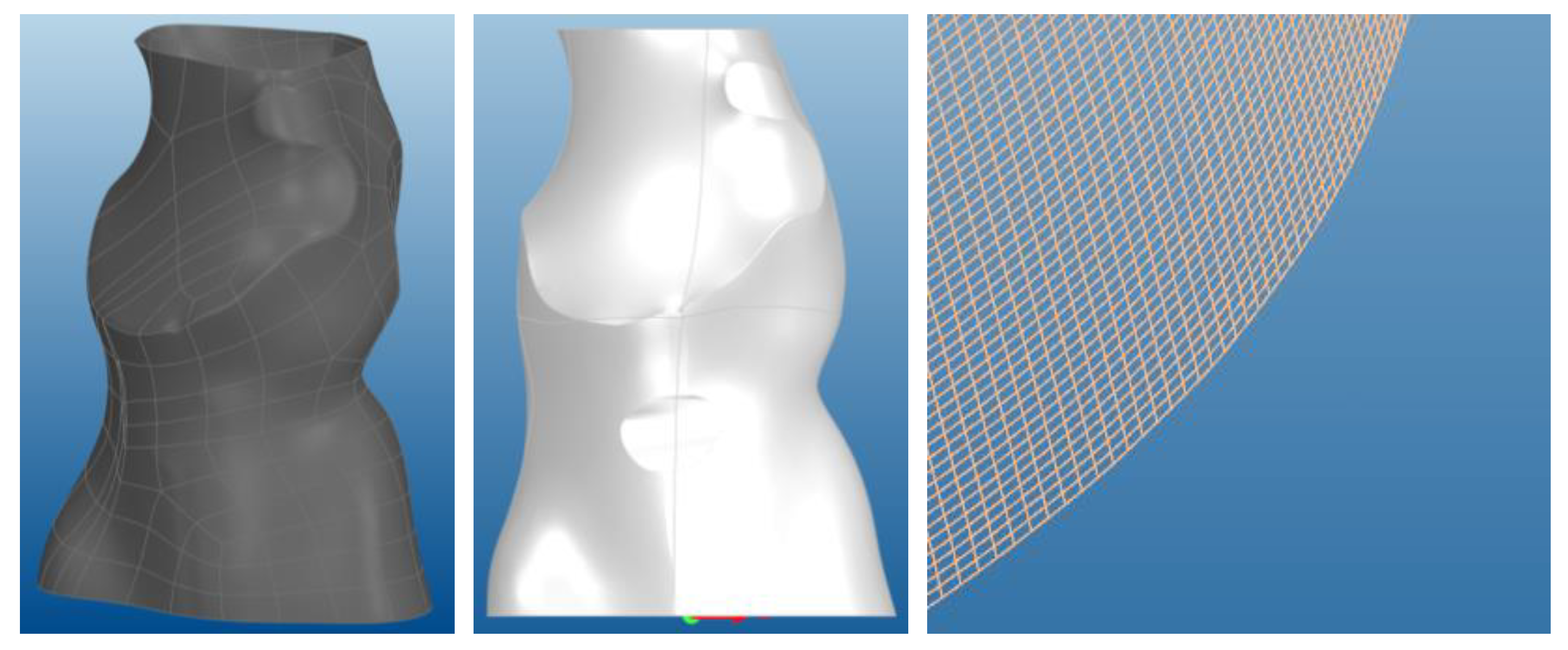
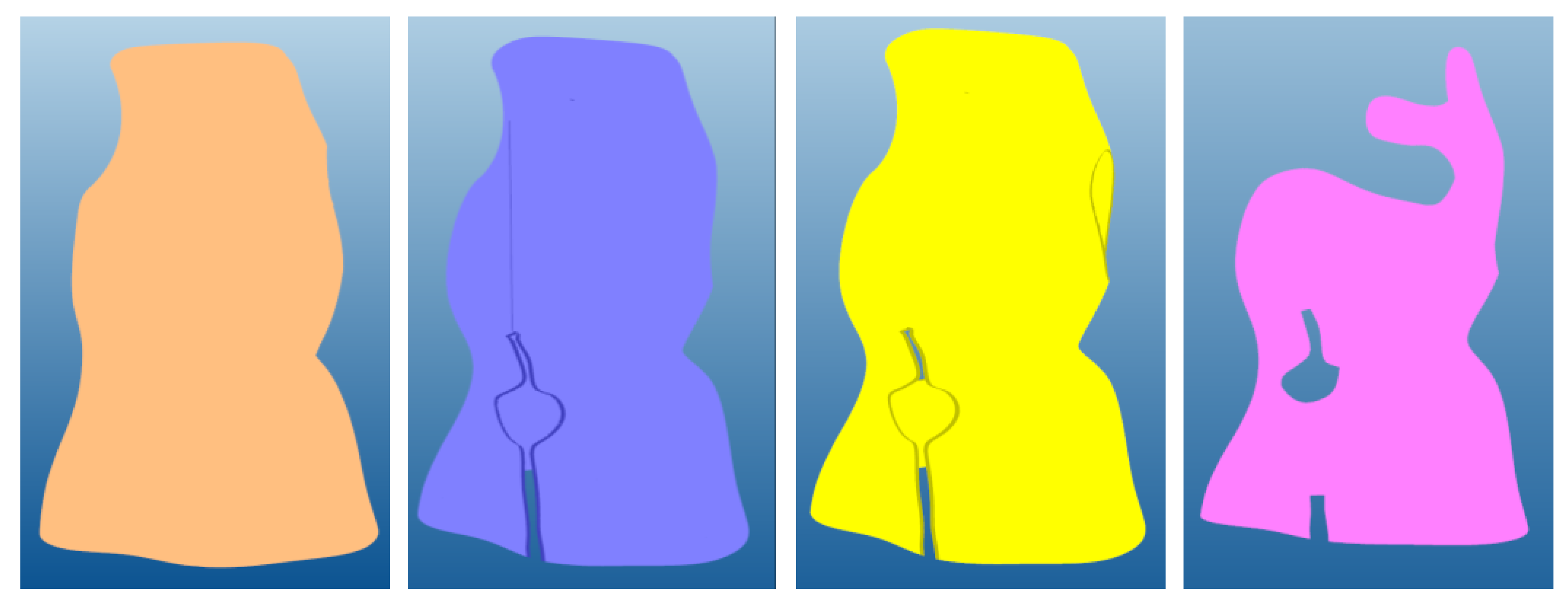
3.1. Model Generation
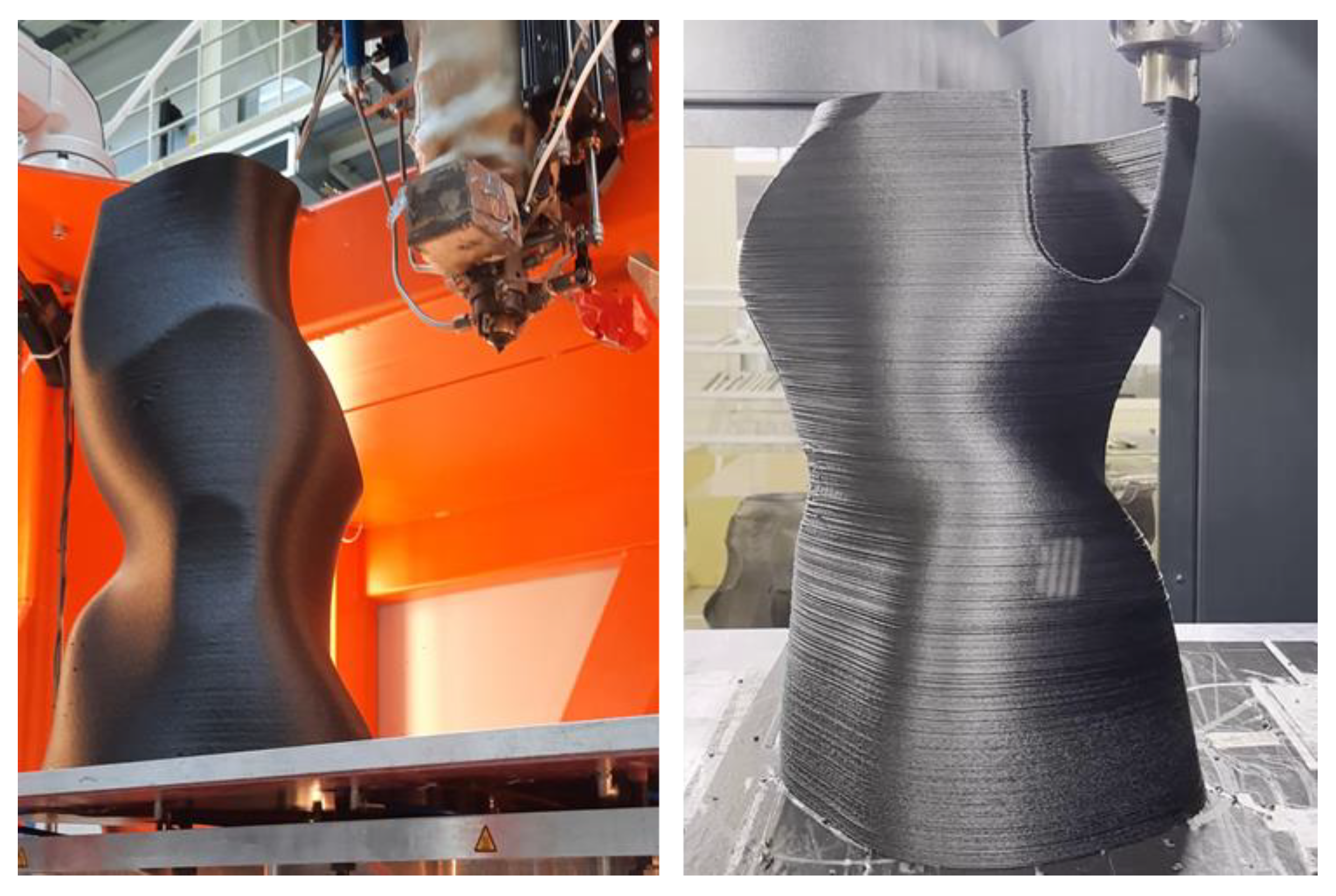
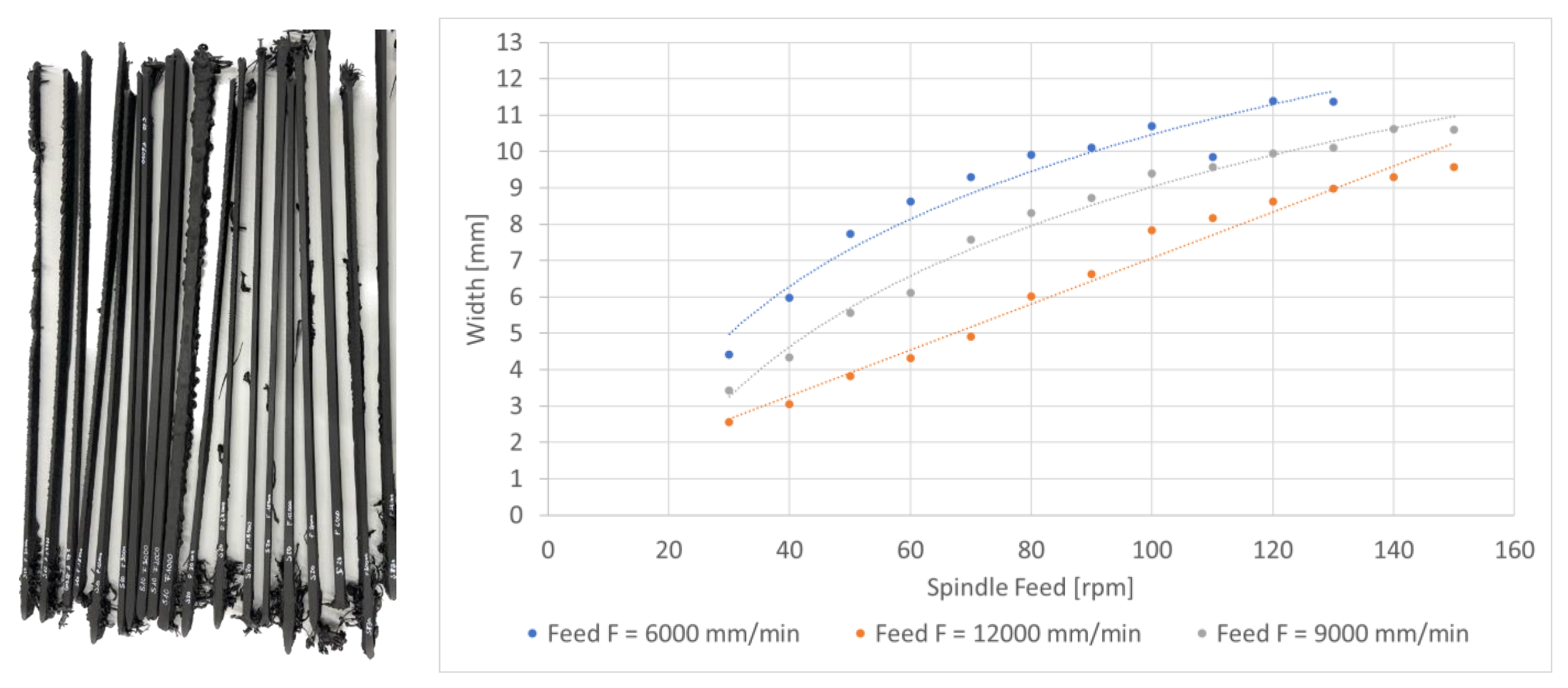
3.2. Manufacturing
4. Conclusions and Outlook
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Asher, M.A.; Burton, D.C. Adolescent idiopathic scoliosis: Natural history and long term treatment effects. Scoliosis 2006, 1, 2. [Google Scholar] [CrossRef] [PubMed]
- Goldberg, C.J.; Moore, D.P.; Fogarty, E.E.; Dowling, F.E. Adolescent idiopathic scoliosis: Natural history and prognosis. In Research into Spinal Deformities 4; IOS Press: Amsterdam, The Netherlands, 2002; pp. 59–63. [Google Scholar]
- Weiss, H.-R.; Lehnert-Schroth, C.; Moramarco, M.; Moramarco, K. Schroth Therapy Advancements in Conservative Scoliosis Treatment, 3rd ed.; Book Publisher International (a part of SCIENCEDOMAIN International): New York, NY, USA, 2022; ISBN 9789355473219. [Google Scholar]
- Weiss, H.-R.; Tournavitis, N.; Nan, X.; Borysov, M.; Paul, L. Workflow of CAD/CAM Scoliosis Brace Adjustment in Preparation Using 3D Printing. Open Med. Inform. J. 2017, 11, 44–51. [Google Scholar] [CrossRef] [PubMed]
- Kaushik, A.; Gahletia, S.; Garg, R.K.; Sharma, P.; Chhabra, D.; Yadav, M. Advanced 3D body scanning techniques and its clinical applications. In Proceedings of the 2022 International Conference on Computational Modelling, Simulation and Optimization (ICCMSO), Pathum Thani, Thailand, 23–25 December 2022; IEEE: Piscataway, NJ, USA, 2022; pp. 352–358, ISBN 979-8-3503-3288-9. [Google Scholar]
- Creaform. HandySCAN 3D Series Metrology-Grade 3D Scanner Optimized for Large Parts. Available online: https://www.creaform3d.com/en (accessed on 20 November 2023).
- Artec3D. Eva Fast Structured Light 3D Scanner for Professionals. Available online: https://www.artec3d.com/de/portable-3d-scanners/artec-eva (accessed on 20 November 2023).
- SMARTTECH 3D. 3D Scanning Technology to Digitizing the Human Body. Available online: https://smarttech3dscanner.com/3d-scanners/smarttech3d-med/ (accessed on 20 November 2023).
- 3D SYSTEMS. Geomagic. Available online: https://de.3dsystems.com/software (accessed on 20 November 2023).
- Helle, R.H.; Lemu, H.G. A case study on use of 3D scanning for reverse engineering and quality control. Mater. Today Proc. 2021, 45, 5255–5262. [Google Scholar] [CrossRef]
- Weiss, H.R.; Seibel, S.; Moramarco, M.; Kleban, A. Bracing scoliosis: The evolution to CAD/CAM for improved in-brace corrections. Hard Tissue 2013, 2, 43. [Google Scholar] [CrossRef]
- Rothstock, S.; Weiss, H.-R.; Krueger, D.; Kleban, V.; Paul, L. Innovative Decision Support for Scoliosis Brace Therapy Based on Statistical Modelling of Markerless 3d Trunk Surface Data. Comput. Methods Biomech. Biomed. Eng. 2020, 23, 923–933. [Google Scholar] [CrossRef] [PubMed]
- Rigo, M.; Chêneau, J. Praxis der Chêneau-Korsettversorgung in der Skoliosetherapie; Thieme: Stuttgart, Germany, 2000; ISBN 9783131185419. [Google Scholar]
- Desbiens-Blais, F.; Clin, J.; Parent, S.; Labelle, H.; Aubin, C.-E. New brace design combining CAD/CAM and biomechanical simulation for the treatment of adolescent idiopathic scoliosis. Clin. Biomech. 2012, 27, 999–1005. [Google Scholar] [CrossRef] [PubMed]
- Sankar, W.N.; Albrektson, J.; Lerman, L.; Tolo, V.T.; Skaggs, D.L. Scoliosis in-brace curve correction and patient preference of CAD/CAM versus plaster molded TLSOs. J. Child. Orthop. 2007, 1, 345–349. [Google Scholar] [CrossRef] [PubMed]
- Vorum. CAD/CAM and 3D Printing Solutions for Orthotics and Prosthetics Providers. Available online: https://vorum.com/op-solution-overview/ (accessed on 18 December 2023).
- Rodin 4D. Software and Applications CAD/CAM. Available online: https://www.rodin4d.com/en/logiciel-cfao/ (accessed on 17 March 2024).
- Nathan, P.; Chou, S.M.; Liu, G. A review on different methods of scoliosis brace fabrication. Prosthet. Orthot. Int. 2023, 47, 424–433. [Google Scholar] [CrossRef] [PubMed]
- Lalegani Dezaki, M.; Mohd Ariffin, M.K.A.; Hatami, S. An overview of fused deposition modelling (FDM): Research, development and process optimisation. RPJ 2021, 27, 562–582. [Google Scholar] [CrossRef]
- Rothstock, S.; González-Ruiz, J.M.; Weiss, H.-R.; Turnbull, D.; Krueger, D. Severity and Cobb angle of scoliosis patients quantified with markerless trunk surface topography using k-NN search and multivariate regression analysis. Comput. Methods Biomech. Biomed. Eng. Imaging Vis. 2023, 11, 2433–2439. [Google Scholar] [CrossRef]
- Gefertec GmbH. Die 3DMP®-Prozesskette. Available online: https://www.gefertec.de/3dmp-verfahren/#prozesskette (accessed on 20 November 2023).
- Invet Medical. Company Invet Medical. Available online: https://www.inventmedical.com/de/start/ (accessed on 10 March 2024).
- 3Faktur. Available online: https://3faktur.com/3d-druck-in-der-orthopaedie/ (accessed on 12 March 2024).
- Ahrendt, D.; Schmitt, F.; Krzywinski, S.; Krzywinski, J. Bend-It—Rethinking Customized Orthopaedic Devices Using Additive Manufacturing; CONVERGE Europe: Essen, Germany, 2017. [Google Scholar]
- Hopmann, C.; Hellmich, C.; Lammert, N. Schichtweise vom Granulat zum Bauteil—Additive Fertigung von faserverstärkten PA6-Strukturbauteilen in hoher Geschwindigkeit. Kunststoffe 2018, 11, 22–25. [Google Scholar]
- IceSL. Product page IceSL. Available online: https://icesl.loria.fr/#header (accessed on 20 November 2023).
- Product Page OctoPrint. Available online: https://octoprint.org/ (accessed on 20 November 2023).
- Product Page Slic3r. Available online: http://slic3r.org/ (accessed on 20 November 2023).
- UltiMaker. Product Page Ultimaker Cura. Available online: https://ultimaker.com/software/ultimaker-cura/ (accessed on 20 November 2023).
- Blase, J.; John, C.; Kausch, M.; Witt, M. Ultrafast 3D printing. Kunststoffe Int. 2019, 11, 32–34. [Google Scholar]
- Ihlenfeldt, S.; Drossel, W.-G.; Kausch, M.; Friedrich, C.; Wiese, T.; Jankowsky, L. SEAMHex—Fast 6D Additive Manufacturing using an innovative Screw Extruder applied on a Hexapod Parallel Kinematic. TLS 2022, 5, 1–14. [Google Scholar] [CrossRef]
- Werner Pluta. Fraunhofer-Forscher Entwickeln Sehr Schnellen 3D-Drucker. Available online: https://www.golem.de/news/seam-fraunhofer-forscher-entwickeln-sehr-schnellen-3d-drucker-1904-140472.html (accessed on 20 November 2023).
- Friedrich, C.; Kauschinger, B.; Ihlenfeldt, S. Stiffness evaluation of a hexapod machine tool with integrated force sensors. J. Mach. Eng. 2020, 20, 58–69. [Google Scholar] [CrossRef]
- Wiese, T.; Abicht, J.; Friedrich, C.; Hellmich, A.; Ihlenfeldt, S. Flexible skill-based control for robot cells in manufacturing. Front. Robot. AI 2022, 9, 1014476. [Google Scholar] [CrossRef] [PubMed]
- Kauschinger, B.; Friedrich, C.; Zhou, R.; Ihlenfeldt, S. Fast Evaluation of the Volumetric Motion Accuracy of Multi-Axis Machine Tools using a Double-Ball-Bar. J. Mach. Eng. 2020, 20, 44–62. [Google Scholar] [CrossRef]
- GFaI e., V. Final Surface: 3D-Software zur Professionellen Erfassung, Visualisierung, Bearbeitung und Analyse von Komplexen 3D-Messdaten. Available online: https://www.final-surface.de (accessed on 12 March 2024).













{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Property | Part | Conventional Forming | SEAM 5 Axis Additive | Conventional 2.5D Additive |
|---|---|---|---|---|
| Technology | Mould | Milling | - | - |
| Brace | Thermoforming | 3D Printing SEAM | 3D Printing FFF | |
| Material | Mould | Polyurethane | - | - |
| Brace | Polyethylene | PA/PP/PET Granulate | PA/PP Filament | |
| Manual work | Mould | No | - | - |
| Brace | Yes | No | No | |
| Waste | Mould | ca. 50% | - | - |
| Brace | ca. 50% | ca. 1–2% | ca. 1–2% | |
| Warehousing | Mould | Necessary | - | - |
| Wall thickness | Brace | 3 mm | 2.5 mm | 2.5 mm |
| Manufacturing Time | Mould | 30 min | - | - |
| Brace | 2 h | 2.5 h | 12 h | |
| Total | 2.5 h | 2.5 h | 12 h | |
| Costs | Mould | EUR 200 | - | - |
| Brace Machining Brace Material | EUR 500 | 2.5 h × 100 EUR/h = EUR 250 0.9 kg × 7 EUR/kg = EUR 6 | 12 h × 60 EUR/h = EUR 720 0.9 kg × 80 EUR/kg = EUR 72 | |
| Total | EUR 700 | 256 | EUR 792 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Friedrich, C.; Rothstock, S.; Slabon, L.; Ihlenfeldt, S. Additive In-Time Manufacturing of Customised Orthoses. J. Manuf. Mater. Process. 2024, 8, 63. https://doi.org/10.3390/jmmp8020063
Friedrich C, Rothstock S, Slabon L, Ihlenfeldt S. Additive In-Time Manufacturing of Customised Orthoses. Journal of Manufacturing and Materials Processing. 2024; 8(2):63. https://doi.org/10.3390/jmmp8020063
Chicago/Turabian StyleFriedrich, Christian, Stephan Rothstock, Laura Slabon, and Steffen Ihlenfeldt. 2024. "Additive In-Time Manufacturing of Customised Orthoses" Journal of Manufacturing and Materials Processing 8, no. 2: 63. https://doi.org/10.3390/jmmp8020063