1. Introduction
The health of workers must begin to become a priority for every company. The health quality of human resources can affect the productivity of the company’s performance. Working more than 8 h every day in a static or non-ergonomic body position can cause many health problems [
1]. Musculoskeletal disorders are one of the most frequent complaints by every type of worker [
2]. Disorders of the musculoskeletal system, which includes muscles, tendons, ligaments, joints, peripheral nerves, and blood vessels, due to workload and unsupportive work environment conditions are called work-related musculoskeletal disorders (WMSDs) [
3]. The risk factors for WMSDs are static and non-ergonomic postures, repetitive movements, excessive use of body strength, vibration, mechanical compression, and temperature. In addition, psychosocial conditions also affect the occurrence of WMSDs, such as stress related to work assignments or problems adapting to the work environment [
2].
According to data released by the Indonesian Basic Health Research (2018), muscu-loskeletal complaints that occur in Indonesia reach 37.2% in productive age with a per-centage difference of 6.1% in men and 8.5% in women [
4]. Based on data from the Great Britain Labor Force Survey (2021), as many as 470,000 workers were recorded as suffering from work-related musculoskeletal disorders. The majority of the complaints felt by the workers were in the neck (45%), back (39%), and lower extremities (16%). Of the total cases, 85,000 cases were recorded to have worsened during the COVID-19 pandemic [
5].
Since December 2019, the whole world has experienced a pandemic due to the out-break of the COVID-19 virus. COVID-19 is an infectious disease caused by the SARS-CoV-2 virus. WHO has recorded 364,191,494 confirmed cases as of January 2022, including 5,631,457 deaths in the world [
6]. The presence of the COVID-19 pandemic in the midst of dense human activities has had a negative impact on the world, causing all human activ-ities to be limited to prevent higher transmission of the COVID-19 virus.
Telerehabilitation is a method of implementing remote rehabilitation carried out by health services using telecommunication devices such as computers, laptops, or smartphones. Telerehabilitation applied using videoconferencing as a medium of com-munication between patients and health services. The implementation of telerehabilita-tion in the rehabilitation of workers is expected to be a solution to prevent the spread of the virus from getting higher and to support the government’s program to limit the impact of the pandemic [
7]. Based on the above background, the authors raised the title of the re-search in the form of the application of telerehabilitation to reduce pain and increase qual-ity of life in workers with work-related musculoskeletal disorders.
2. Clinical Statements
The many problems caused by work-related musculoskeletal disorders make physiotherapy an important effort in solving these problems. In a pandemic situation, technology plays an important role in the sustainability of community activities. Virtual activities are the main alternative for individuals to stay active. One approach that can be applied to rehabilitation care in this pandemic situation is telerehabilitation. Based on the above, the formulation of the problem raised in this study is “How does the application of telerehabilitation affect pain reduction and increase quality of life in workers with work-related musculoskeletal disorders?”.
3. Material and Methods
The method used in this study is a systematic review with a search period from 2021 to 2022. The authors searched for articles using keywords and Boolean operators (AND, OR NOT, or AND NOT) in 5 databases (Google Scholar, Medline, Proquest, Pubmed, and Scopus). To filter the results of the articles, inclusion criteria and exclusion criteria were used as filters.
The inclusion criteria in this study were (1) workers; (2) never had or have experienced a work-related musculoskeletal disorder; (3) telerehabilitation; (4) measuring pain intensity and quality of life; (5) study design: mix methods study, experimental study, survey study, cross-sectional, comparative, or qualitative study; (6) published after 2017; (7) article in English or Indonesian. The exclusion criteria included (1) non-employees, (2) interventions other than telerehabilitation, (3) not measuring pain intensity and quality of life, (4) systematic review study design, (5) published before 2017, (6) articles in languages other than English and Indonesian. The keywords used to search for articles were mapped using the PICO framework, with the following details:
4. Results
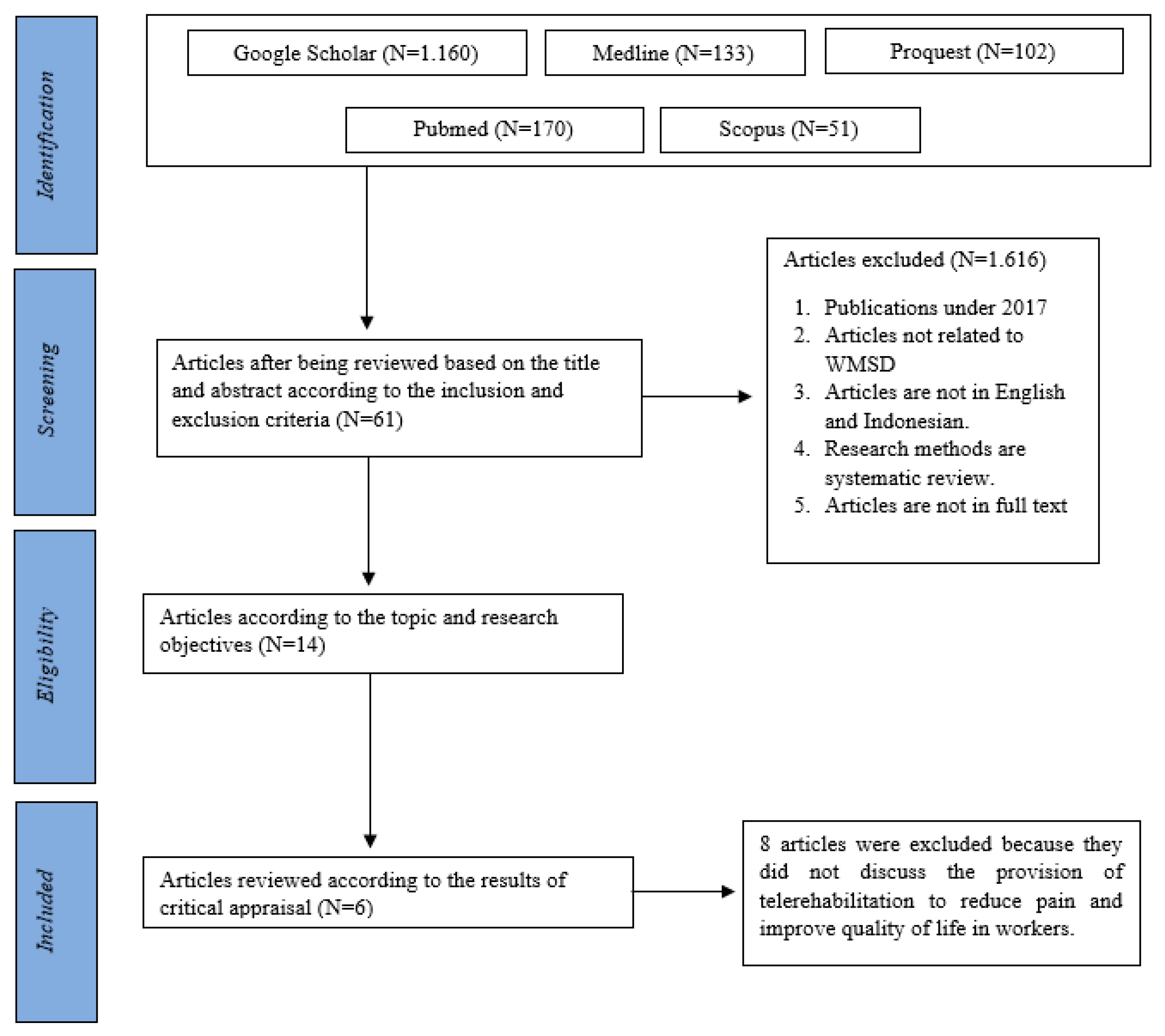
Based on the results of a literature search in Google Scholar, Medline, ProQuest, PUBMED, and Scopus databases using the keywords “Work-Related Musculoskeletal Disorder OR Musculoskeletal Disorder OR Worker AND Telerehabilitation OR Telecare OR Telehealth OR Videoconferencing OR Internet-based AND Pain OR Functional Ability OR Quality of life”, the researchers found 1.677 articles that matched these keywords. The research articles were then screened by title and abstract, and the researcher found 61 articles met the inclusion criteria, with 1.616 articles in the exclusion criteria. Then, a critical appraisal was carried out on 14 published articles, obtaining 6 articles for which data synthesis would be carried out. The data collection process used the PRISMA (Preferred Reporting Items for Systematic Review and Meta-Analysis) method. The PRISMA Chart can be seen in
Figure 1.
5. Outcome Measures
In assessing the quality of the intervention given to improve pain and quality of life, various parameters were used, such as the VAS, SF-12 HS, SF-36 HS, Work Ability Index, and EQ5D. The demographics and outcomes reported in each article can be seen in
Table 1.
The VAS is a pain measurement scale depicted by a 10 cm line that describes the conditions from “no pain” to “severe pain” at both ends of the line. Patients were in-structed to mark numbers on a line that describes the intensity of the pain felt. The ad-vantage of using the VAS is that this scale is more sensitive to see changes in pain, so it is easy to understand and is often used in various clinical conditions [
8]. While the weak-ness of this scale is that it is difficult to use in the elderly or individuals with cognitive deficits and children [
9].
The Short Form 36 Health Survey is one of the measurement instruments that assesses the quality of life of individuals [
10]. This questionnaire consists of 36 questions that have been classified into 8 domains in the form of physical aspects, social aspects, emotional aspects, physical health aspects, emotional health aspects, pain aspects, vital aspects, and general health aspects [
11]. Each question is given a score of 0–100. The higher the score for each domain, the better the quality-of-life score. The weakness of this parameter is that too many questions are asked so that it is more complicated and takes longer [
12].
The Short Form 12 Health Survey is a measurement parameter that assesses quality of life. The SF-12 contains 12 short questions drawn from all aspects of the SF-36. This pa-rameter is considered more effective and does not take much time because the number of questionnaire questions is only small. According to the research of Shou, et al. the param-eters SF-12 and SF-36 are considered valid and reliable in measuring quality of life status [
12].
The WAI is a measurement instrument used to assess workability. WAI contains seven items of questions related to job demands, health status of workers, and resources. The achievement score of this index ranges from 7–49 [
13].
The EQ-5D is the most frequently used parameter in assessing an individual’s quality of life. These parameters can be applied to patients with various diagnoses of different dis-eases. The EQ-5D consists of 5 domains which include aspects of mobility, aspects of self-care, aspects of daily activities, aspects of pain, and aspects of depression [
14].
Table 1.
Demographics and outcomes.
Table 1.
Demographics and outcomes.
| Study | Study Design | Level of Evidence | Age (Years) | Diagnosis | Outcomes |
|---|
| Pain | QoL |
|---|
| Maliaras, et al. [15] | RCT | 1c | 41–65 | Shoulder pain | VAS | EuroQol 5D-5L |
| Yaghoubitajani, et al. [16] | RCT | 1c | 21–42 | Neck pain and shoulder pain | VAS | Work ability |
| Moreira, et al. [17] | Quasi-experimental | 2d | 29–44 | Low back pain and neck pain | SF-36 HS | SF-36 HS |
| Blanquero, et al. [18] | RCT | 1c | 31–56 | Wrist, hand, or finger injuries | VAS | Return to work |
| Mbada, et al. [19] | RCT | 1c | 36–61 | Chronic low back pain | QVAS | SF-12 HS |
| Lee, et al. [20] | RCT | 1c | 25–35 | Chronic neck pain | VAS | SF-36 HS |
6. Intervention
Telerehabilitation is a remote health rehabilitation service provided through the medium of technology and communication. These services include assessment, diagnosis, prognosis, intervention, consultation, and counseling through patient and family education [
21]. The intervention was given through telerehabilitation in the form of physical exercise that was adapted to the patient’s condition and complaints. Physical exercise can reduce pain, which will indirectly increase work productivity [
22]. The forms of interventions carried out in the six studies in the intervention group and control group can be seen in
Table 2.
7. Discussion
7.1. Effect of Telerehabilitation on Reducing Pain
Based on the six articles reviewed, telerehabilitation can reduce pain in workers with work-related musculoskeletal disorders. In research by Maliaras et al., 36 participants were divided into 3 groups, namely, the advice group (N = 12), the recommended care group (internet-delivered exercise and education) (N = 12), and the recommended care and telerehabilitation group (N = 12), and the measurement parameter used to assess pain was the VAS. The intervention was carried out for 12 weeks. The results showed that there was a significant decrease in group 3, which was given an additional intervention with telerehabilitation, from 59.7 (21.1) to 28.1 (25.6) [
15]. This is similar to the results of research by Yaghoubitajani et al., where there was a decrease in pain felt by participants in the intervention group with the provision of online-supervised corrective exercise; participants in this group experienced a significant reduction in pain of 3.25 ± 1.95 [
16].
This study is in line with research conducted by Moreira et al. on 39 participants who were divided into two groups, namely, the intervention group (N = 13) and the control group (N = 26). The results showed that providing an exercise program to the intervention group in the form of mobility, flexibility, and strengthening exercises for 17 weeks with 3 meetings a week for 15 min had a major effect on pain, with an increase from 79 (17.1) to 87.4 (12.7), which means there was a decrease in the pain felt by the participants. Meanwhile, in the control group, the pain worsened from 79.2 (19) to 71.1 (20.1) [
17].
This study is comparable to research conducted by Lee et al., who provided a measuring tool for pain assessment. The results indicated that there was a significant change in pain reduction before and after the intervention was given, decreasing from 5.20 (2.19) to 2.73 (1.99) [
20].
Based on the six articles, it can be concluded that the application of telerehabilitation to workers is able to provide benefits that can significantly reduce the level of pain felt by workers during their daily work. Apart from the six articles above, this is supported by other studies conducted by Cottrell et al., who showed that telerehabilitation is able to provide an alternative for patients so that they can continue to receive proper care with limited environmental conditions that occur at the time [
23]. According to Chang et al., the application of telerehabilitation to workers with musculoskeletal disorders can significantly reduce pain that limits work productivity [
24]. Telerehabilitation helps patients to maintain an exercise program under the remote supervision of a physiotherapist so that the prescribed exercises can achieve significant results [
23].
In the study by Anan et al., it was shown that one of the benefits of telerehabilitation is the level of patient compliance with the given exercise program. Telerehabilitation facilitates exercise reminder services so that patients will be more obedient in implementing exercises at home and at work. In addition, telerehabilitation that is implemented through the application will make patients more motivated to complete the exercises so that patients are encouraged to be more diligent in following the exercise program that has been prescribed [
25]. In a study conducted by Smith et al., it was explained that exercise carried out regularly with the supervision of a physiotherapist will reduce pain significantly because physical exercise is able to stimulate the production of analgesics, which will contribute to pain reduction. Physical exercise performed at a certain dose is able to stimulate the release of endorphins, which will activate opioid receptors in the peripheral and central nervous systems, thereby triggering the endogenous opioid system to produce an analgesic effect that will reduce pain sensitivity [
26].
7.2. Effect of Telerehabilitation on Improving the Quality of Life and Work Productivity
According to the six studies above, the provision of telerehabilitation to workers is able to improve the quality of life and help improve work abilities. A decrease in the quality of life is caused by the discomfort felt by workers, such as pain. This decline in the quality of life will have an impact on the level of worker productivity, which will disrupt the company’s performance, as described in research by Maliaras et al., in which the intervention group that received recommended care and telerehabilitation showed an increase in quality of life using the EQ5D parameter. The parameter results in the intervention group showed a value of 0.74 (0.12) at the beginning and increased to 0.78 (0.07) [
15].
Similar results were shown in a study conducted by Yaghoubitajani et al. In the intervention group with online supervision, there was an increase in work ability, as measured using the Work Ability Index Questionnaire, to 8.00 ± 1.34, while in the control group, it was only 8.27 ± 90 [
16]. Another study conducted by Moreira et al. shows comparable results. In this study, there was an increase in physical function and physical performance, as measured using the SF-36 parameter. Although the increase from 93.8 (6.8) to 95.0 (7.4) was not significant, this result was better than the control group, which decreased from 94.4 to 88.1 [
17].
This study is in line with research conducted by Blanquero et al. on 74 participants who were divided into 2 groups, namely, the intervention group (N = 40) and the control group (N = 34). The results showed that the intervention group required an average return to work of 76 days in cases of wrist, hand, and finger injuries, and 94 days was the average time required by the control group (MD −18 days, 95% CI −33 to −3). With a fairly large difference in days, telerehabilitation can be said to be able to accelerate worker productivity [
18].
The same thing happened in the study by Mbada et al., who used the SF-12 HS parameter for the assessment of physical function. The results showed that the intervention group who exercised through telerehabilitation had a more significant improvement compared to the control group [
19]. The study also had comparable results to the study by Lee et al., in which 20 participants received a McKenzie exercise treatment and education through the application, and the control group was only given posture correction education. The results of the study by Lee et al. showed that there was a significant increase in the quality of life in the intervention group compared to the control group, as examined with the SF-36 HS parameter [
20].
The pain felt by workers with WMSDs is correlated with their quality of life, which will have an impact on job satisfaction and productivity. An MSD affects attendance and sick leave. Research conducted by Chhabra et al. suggested that physical exercise will improve physical abilities as well as psychological health, which usually occurs as a side effect in individuals with poor health [
27]. This is supported by research by Kim et al., who state that nurses who experience pain will have difficulty providing quality services to clients, so it has an impact on the level of client satisfaction [
28]. Another study by Nguyen et al. showed the same thing, namely, when physical exercise is carried out regularly, it will have an impact on psychosocial health, where there is an increase in mood and decreased levels of depression and anxiety, so it affects work productivity [
28]. Adhikari et al. reported that more than a third of workers experience back and neck pain after sitting for 2 h in front of the computer, which affects their work performance and productivity. With the implementation of telerehabilitation, there is an increase in the quality of life because physical exercise will help increase patient activation [
22]. Based on the six articles above, it can be concluded that the application of telerehabilitation to workers has a positive impact on improving the quality of life, which affects work productivity.
7.3. Effective Telerehabilitation Dose
The telerehabilitation dose applied in patients with musculoskeletal pain recommended by Alsobayel et al. was 2–3 times per week with a duration of 20–40 min for 6 weeks. It is proven that telerehabilitation has positive therapeutic impacts in the form of pain reduction and improvements in physical function [
29]. The telerehabilitation doses in the study by Blanquero et al., more than 3 days a week for 4 weeks, may be effective in reducing pain and increasing work productivity [
18]. This is supported by research conducted by Vega et al., who reported that the intervention carried out with application-based telerehabilitation 5 days a week for at least 4 weeks may be effective in reducing pain and improving the quality of life [
30].
8. Limitation
A limitation of this systematic review is that it does not discuss all complaints felt by workers with work-related musculoskeletal disorders; this study only discusses neck pain, low back pain, and upper extremity injuries.
9. Conclusions
Based on the six articles that have been reviewed, it can be concluded that the application of telerehabilitation to workers is able to provide benefits that can significantly reduce pain levels and have a positive impact on the quality of life, which affects work productivity and can be seen with the parameters VAS, QVAS, SF-12 HS, SF-36 HS, Work Ability Index, and EQ5D.
Author Contributions
Conceptualization, methodology, and writing (original draft preparation, review, and editing): A.D.F., A.D.P., T.K., R.P., M.N. and F.A. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Utami, U.; Karimuna, S.R.; Jufri, N. Hubungan Lama Kerja, Sikap Kerja Dan Beban Kerja Dengan Muskuloskeletal Disorders (Msds) Pada Petani Padi Di Desa Ahuhu Kecamatan Meluhu Kabu-Paten Konawe Tahun. 2017. Available online: https://www.neliti.com/publications/198186/hubungan-lama-kerja-sikap-kerja-dan-beban-kerja-dengan-muskuloskeletal-disorders (accessed on 23 April 2022).
- Govaerts, R.; Tassignon, B.; Ghillebert, J.; Serrien, B.; De Bock, S.; Ampe, T.; El Makrini, I.; Vanderborght, B.; Meeusen, R.; De Pauw, K. Prevalence and incidence of work-related musculoskeletal disorders in secondary industries of 21st century Europe: A systematic review and meta-analysis. BMC Musculoskelet. Disord. 2021, 22, 751. [Google Scholar] [CrossRef]
- Nunes, I.L.; Bush, P.M. Work-Related Musculoskeletal Disorders Assessment and Prevention. Available online: www.intechopen.com (accessed on 2 May 2022).
- Kementrian Kesehatan R.I. Laporan Provinsi DKI Jakarta Riskesdas 2018. 2018. Available online: http://repository.bkpk.kemkes.go.id/3881/ (accessed on 27 April 2022).
- Health, Safety, and Environment UK. Work-related musculoskeletal disorders statistics in Great Britain. 2021. Available online: https://www.hse.gov.uk/statistics/causdis/msd.pdf (accessed on 1 January 2022).
- World Health Organization (WHO). Coronavirus COVID-19 Dashboard. Available online: https://covid19.who.int (accessed on 8 December 2021).
- Silakarma, D.; Widnyana, M. Telerehabilitation as a physical therapy solution for the post-stroke patient in COVID-19 pandemic situations: A review I Made Yoga Prabawa. Intisari Sains Medis. Intisari Sains Medis 2021, 12, 1–5. [Google Scholar]
- Arifin, S.; Ferezagia, D.V.; Safitri, K.A. Effective Treatment in Reducing Pain in Patients With Musculoskeletal Pain Complaints. J. Vokasi Indones. 2018, 6. [Google Scholar] [CrossRef]
- Pathak, A.; Sharma, S.; Jensen, M.P. The utility and validity of pain intensity rating scales for use in developing countries. PAIN Rep. 2018, 3, e672. [Google Scholar] [CrossRef]
- Novitasari, L.; Perwitasari, D.A.; Khoirunisa, S. Validity of short form 36 (SF-36) Indonesian version on rheumatoid arthritis patients. J. Kedokt. dan Kesehat. Indones. 2016, 7, 80–86. [Google Scholar] [CrossRef] [Green Version]
- Keandalan, U.; Kuesioner, K.; Hidup, K.; Falah, N.M.; Putranto, R.; Setyohadi, B.; Rinaldi, I. Short Form 12 Ber-bahasa Indonesia pada Pasien Artritis Reumatoid Reliability and Validity Test Of Indonesian Version Short Form 12 Quality of Life Questionnaire in Rheumatoid Arthritis Patient. J. Penyakit Dalam Indonesia. 2017, 4. [Google Scholar] [CrossRef] [Green Version]
- Shou, J.; Ren, L.; Wang, H.; Yan, F.; Cao, X.; Wang, H.; Wang, Z.; Zhu, S.; Liu, Y. Reliability and validity of 12-item Short-Form health survey (SF-12) for the health status of Chinese community elderly population in Xujiahui district of Shanghai. Aging Clin. Exp. Res. 2015, 28, 339–346. [Google Scholar] [CrossRef]
- Ilmarinen, J. The Work Ability Index (WAI). Occup. Med. 2006, 57, 160. [Google Scholar] [CrossRef] [Green Version]
- Obradovic, M.; Lal, A.; Liedgens, H. Validity and responsiveness of EuroQol-5 dimension (EQ-5D) versus Short Form-6 dimension (SF-6D) questionnaire in chronic pain. Health Qual. Life Outcomes 2013, 11, 110–119. [Google Scholar] [CrossRef] [Green Version]
- Malliaras, P.; Cridland, K.; Hopmans, R.; Ashton, S.; Littlewood, C.; Page, R.; Harris, I.; Skouteris, H.; Haines, T. Internet and Telerehabilitation-Delivered Management of Rotator Cuff–Related Shoulder Pain (INTEL Trial): Randomized Controlled Pilot and Feasibility Trial. JMIR mHealth uHealth 2020, 8, e24311. [Google Scholar] [CrossRef]
- Yaghoubitajani, Z.; Gheitasi, M.; Bayattork, M.; Andersen, L.L. Corrective exercises administered online vs at the workplace for pain and function in the office workers with upper crossed syndrome: Randomized controlled trial. Int. Arch. Occup. Environ. Health 2022, 95, 1703–1718. [Google Scholar] [CrossRef] [PubMed]
- Moreira, S.; Criado, M.B.; Ferreira, M.S.; Machado, J.; Gonçalves, C.; Clemente, F.M.; Mesquita, C.; Lopes, S.; Santos, P.C. Positive Effects of an Online Workplace Exercise Intervention during the COVID-19 Pandemic on Quality of Life Perception in Computer Workers: A Quasi-Experimental Study Design. Int. J. Environ. Res. Public Health 2022, 19, 3142. [Google Scholar] [CrossRef] [PubMed]
- Blanquero, J.; Cortés-Vega, M.-D.; Rodríguez-Sánchez-Laulhé, P.; Corrales-Serra, B.-P.; Gómez-Patricio, E.; Díaz-Matas, N.; Suero-Pineda, A. Feedback-guided exercises performed on a tablet touchscreen improve return to work, function, strength and healthcare usage more than an exercise program prescribed on paper for people with wrist, hand or finger injuries: A randomised trial. J. Physiother. 2020, 66, 236–242. [Google Scholar] [CrossRef]
- Mbada, C.E.; Olaoye, M.I.; Dada, O.O.; Ayanniyi, O.; Johnson, O.E.; Odole, A.; Ishaya, G.P.; Omole, O.J.; Makinde, M.O. Comparative Efficacy of Clinic-Based and Telerehabilitation Application of Mckenzie Therapy in Chronic Low-Back Pain. Int. J. Telerehabil. 2019, 11, 41–58. [Google Scholar]
- Lee, J.; Lee, M.; Lim, T.; Kim, T.; Kim, S.; Suh, D.; Lee, S.; Yoon, B. Effectiveness of an application-based neck exercise as a pain management tool for office workers with chronic neck pain and functional disability: A pilot randomized trial. Eur. J. Integr. Med. 2017, 12, 87–92. [Google Scholar] [CrossRef]
- de Araújo Novaes, M. Telecare within Different Specialties. In Fundamentals of Telemedicine and Telehealth; Elsevier: Amsterdam, The Netherlands, 2019; pp. 185–254. [Google Scholar]
- Adhikari, S.P.; Shrestha, P.; Dev, R. Feasibility and Effectiveness of Telephone-Based Telephysiotherapy for Treatment of Pain in Low-Resource Setting: A Retrospective Pre-Post Design. Pain Res. Manag. 2020, 2020, 2741278. [Google Scholar] [CrossRef] [PubMed]
- Cottrell, M.A.; Galea, O.A.; O’Leary, S.P.; Hill, A.J.; Russell, T.G. Real-time telerehabilitation for the treatment of musculoskeletal conditions is effective and comparable to standard practice: A systematic review and meta-analysis. Clin. Rehabil. 2017, 31, 625–638. [Google Scholar] [CrossRef]
- Chang, Y.-F.; Yeh, C.-M.; Huang, S.-L.; Ho, C.-C.; Li, R.-H.; Wang, W.-H.; Tang, F.-C. Work Ability and Quality of Life in Patients with Work-Related Musculoskeletal Disorders. Int. J. Environ. Res. Public Health 2020, 17, 3310. [Google Scholar] [CrossRef]
- Anan, T.; Kajiki, S.; Oka, H.; Fujii, T.; Kawamata, K.; Mori, K.; Matsudaira, K. Effects of an Artificial Intelligence–Assisted Health Program on Workers With Neck/Shoulder Pain/Stiffness and Low Back Pain: Randomized Controlled Trial. JMIR mHealth uHealth 2021, 9, e27535. [Google Scholar] [CrossRef]
- E Smith, B.; Hendrick, P.; Bateman, M.; Holden, S.; Littlewood, C.; O Smith, T.; Logan, P. Musculoskeletal pain and exercise—Challenging existing paradigms and introducing new. Br. J. Sports Med. 2018, 53, 907–912. [Google Scholar]
- Chhabra, H.S.; Sharma, S.; Verma, S. Smartphone app in self-management of chronic low back pain: A randomized controlled trial. Eur. Spine J. 2018, 27, 2862–2874. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, T.; Nguyen, V.; Kim, J. Physical Exercise and Health-Related Quality of Life in Office Workers: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2021, 18, 3791. [Google Scholar] [CrossRef] [PubMed]
- Alsobayel, H.; Alodaibi, F.; Albarrati, A.; Alsalamah, N.; Alhawas, F.; Alhowimel, A. Does Telerehabilitation Help in Reducing Disability among People with Musculoskeletal Conditions? A Preliminary Study. Int. J. Environ. Res. Public Health 2021, 19, 72. [Google Scholar] [CrossRef] [PubMed]
- Kim, D. Effect of musculoskeletal pain of care workers on job satisfaction. J. Phys. Ther. Sci. 2018, 30, 164–168. [Google Scholar] [CrossRef]
| Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).


 ,
, 
{kind=link}
