
The Effectiveness of Exergame Exercises to Improve Cognitive Function in Cases of Dementia: Literature Review †

Abstract
:1. Introduction
2. Research Methods
3. Results
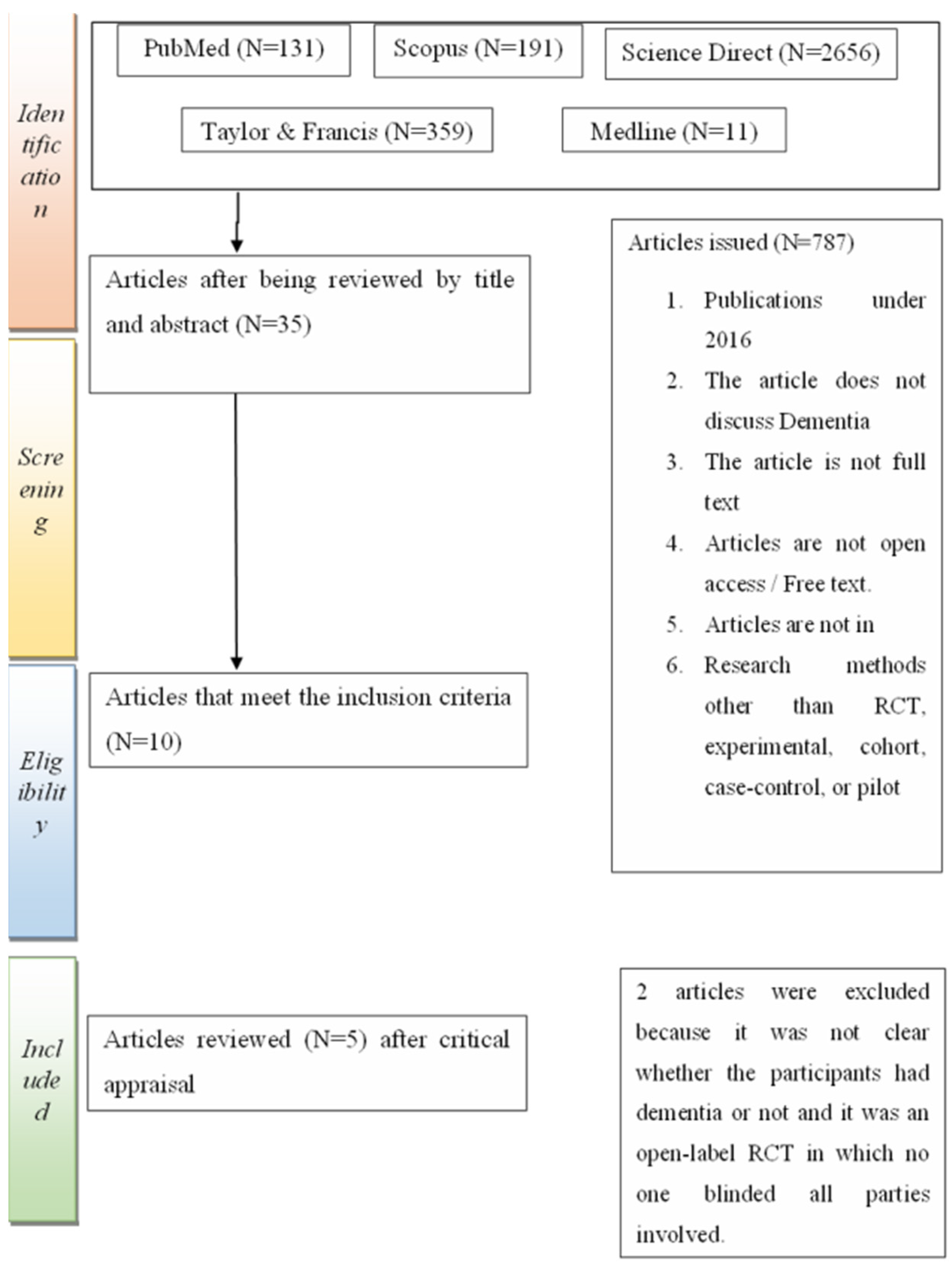
3.1. Study Selection
3.2. Study Design and Aims
4. Discussion
4.1. The Effect of Physical Exercise on Cognitive Improvement
4.2. Exergame Effectiveness and Dosage
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Duong, S.; Patel, T.; Chang, F. Dementia: What pharmacists need to know. Can. Pharm. J. 2017, 150, 118–129. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bansal, N.; Parle, M. Dementia: An Overview. J. Pharm. Technol. Res. Manag. 2014, 2, 29–45. [Google Scholar] [CrossRef]
- World Health Organization. Dementia. 2021. Available online: https://www.who.int/news-room/fact-sheets/detail/dementia (accessed on 18 May 2022).
- Prince, M. World Alzheimer Report 2015: The Global Impact of Dementia; Alzheimer’s Disease International (ADI): London, UK, 2015; pp. 1–87. Available online: https://www.alz.co.uk/research/worldalzheimerreport2015summary.pdf (accessed on 23 April 2022).
- Alzheimer’s Indonesia. Statistik Tentang Demensia—Alzheimer Indonesia. Available online: https://alzi.or.id/statistik-tentang-demensia/ (accessed on 18 May 2022).
- Johansson, M.M.; Marcusson, J.; Wressle, E. Cognitive impairment and its consequences in everyday life: Experiences of people with mild cognitive impairment or mild dementia and their relatives. Int. Psychogeriatr. 2015, 27, 949–958. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Infodatin. Situasi Lanjut Usia (Lansia) di Indonesia. Pusdatin, 12. Situasi Lanjut Usia (Lansia) di Indonesia. 2016. Available online: https://www.academia.edu/38158922/infodatin_lansia_2016_pdf/ (accessed on 24 April 2022).
- Rokom. Indonesia Masuki Periode Aging Population—Sehat Negeriku. Available online: https://sehatnege-riku.kemkes.go.id/baca/umum/20190704/4530734/indonesia-masuki-periode-aging-population/ (accessed on 18 May 2022).
- Tuomaala, J. Virtual Reality and Exergaming. 2020. Available online: https://core.ac.uk/download/pdf/323463204.pdf/ (accessed on 26 April 2022).
- Zheng, J.; Yu, P.; Chen, X. An Evaluation of the Effects of Active Game Play on Cognition, Quality of Life and Depression for Older People with Dementia. Clin. Gerontol. 2021, 45, 1034–1043. [Google Scholar] [CrossRef] [PubMed]
- Karssemeijer, E.G.A.; Aaronson, J.A.; Bossers, W.J.R.; Donders, R.; Olde Rikkert, M.G.M.; Kessels, R.P.C. The quest for synergy between physical exercise and cognitive stimulation via exergaming in people with dementia: A randomized controlled trial. Alzheimers Res. Ther. 2019, 11, 3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van Santen, J.; Dröes, R.M.; Twisk, J.W.R.; Blanson Henkemans, O.A.; van Straten, A.; Meiland, F.J.M. Effects of Exergaming on Cognitive and Social Functioning of People with Dementia: A Randomized Controlled Trial. J. Am. Med. Dir. Assoc. 2020, 21, 1958–1967.e5. [Google Scholar] [CrossRef] [PubMed]
- Swinnen, N.; Vandenbulcke, M.; de Bruin, E.D.; Akkerman, R.; Stubbs, B.; Firth, J.; Vancampfort, D. The efficacy of exergaming in people with major neurocognitive disorder residing in long-term care facilities: A pilot randomized controlled trial. Alzheimers Res. Ther. 2021, 13, 70. [Google Scholar] [CrossRef] [PubMed]
- Swinnen, N.; Vandenbulcke, M.; de Bruin, E.D.; Akkerman, R.; Stubbs, B.; Vancampfort, D. Exergaming for people with major neurocognitive disorder: A qualitative study. Disabil. Rehabil. 2020, 44, 2044–2052. [Google Scholar] [CrossRef] [PubMed]
- Mandolesi, L.; Polverino, A.; Montuori, S.; Foti, F.; Ferraioli, G.; Sorrentino, P.; Sorrentino, G. Effects of physical exercise on cognitive functioning and wellbeing: Biological and psychological benefits. Front. Psychol. 2018, 9, 509. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Skilleter, A.J.; Weickert, C.S.; Vercammen, A.; Lenroot, R.; Weickert, T.W. Peripheral BDNF: A candidate biomarker of healthy neural activity during learning is disrupted in schizophrenia. Psychol. Med. 2015, 45, 841–854. [Google Scholar] [CrossRef] [PubMed]
- Colucci-D’amato, L.; Speranza, L.; Volpicelli, F. Neurotrophic factor bdnf, physiological functions and therapeutic potential in depression, neurodegeneration and brain cancer. Int. J. Mol. Sci. 2020, 21, 7777. [Google Scholar] [CrossRef] [PubMed]
- Lorimer, A. The Cerebrum, its hemispheres and structures. Res. Rep. 2020, 9, 1–27. [Google Scholar] [CrossRef]
- Zoladz, J.A.; Pilc, A. The effect of physical activity on the brain derived neurotrophic factor: From animal to human studies. J. Physiol. Pharmacol. 2010, 61, 533–541. [Google Scholar] [PubMed]


{kind=link}
| Study | Method (Desain Sample, Variable, Instrument, and Analys) | Group Treatment | Group Control | Follow-Up | Results |
|---|---|---|---|---|---|
| Jiaying Zheng et al. [10] | D: Randomized controlled trial S: Convenience sampling V: Exergame group, I: MMSE A: Pre-post comparative design | For 8 weeks with a frequency of exercise 5 days/week with a duration of exercise 1 h/day. The exergame tool used is a Kinect system box, which has a Kinect sensor and a console (for game control). Participants were asked to sit in a chair 1–1.5 m away from the Kinect sensor so that their position and movement could be detected by the infrared camera on the sensor. The game played is The Kinect Fruit Ninja game, where participants are asked to cut the fruit to obtain points. If the participant cuts the bomb, there will be a point deduction. In addition, participants received treatment as usual (not explained what kind of special treatment) and received treatment as usual within 8 weeks. Eighth week after the initial intervention. | Receive the usual care within 8 weeks. | Eighth week after the initial intervention. | There was no significant between-group difference in MMSE scores (p = 0.252). There was an increase in the MMSE score in the intervention group, although it was not significant. |
| Esther et al. [11] | D: Controlled trial S: Convenience sampling V: Interactive cycling I: MMSE A: Intention to treat (ITT) analyses | Group Exergames: The intervention was given in 12 weeks with a frequency of 3x/week, with each session lasting 30–50 min. Participants were given an exergame exercise in the form of a combined cognitive–aerobic bicycle exercise developed by Bike Labyrinth. This exergame tool is a stationary bicycle connected to a video screen, and participants are asked to follow a bicycle route through a digital environment and jointly participate in cognitive tasks. The cognitive training task has seven levels of difficulty, so cognitive training becomes a permanent challenge for participants. Static Bike Group: Intervention was given in 12 weeks with a frequency of 3x/week. Participants were given cycling exercises on a stationary bicycle for 30 to 50 min. The intervention was given for 12 weeks with a frequency of 3x/week. Participants in this group were given exercises containing relaxation and flexibility exercises with an exercise time of 30 min in Week 12 (T2) and week 24 (F1) at the time of the initial intervention. | The intervention was given in 12 weeks with a frequency of 3x/week. Participants in this group were given an exercise containing relaxation and flexibility exercises with a 30 min exercise time. | Week 12 (T2) and week 24 (F1) after the initial intervention. | There was an increase in cognitive function in the exergame group on MMSE at T2 (r = 2.30, 95% CI: 0.65, 3.96, p = 0.007) and TMT-A at T2 (r = −28.98, 95% CI: −54.89, −3.08, p = 0.029). |
| Joeke van Santen et al. [12] | D: Randomized controlled trial S: Purposive sampling V: Combined cognitive aerobic bicycle I: TMT-B, the abbreviated 5-line Stroop color–word test interference score, letter fluency, the rule of shift cards, location learning test—revised, WAIS-III digit span, WMS-III spatial span A: Pre-test–post-test design | For 6 months with a frequency of 5 times/week. The interventions provided were a program of regular activities (music, arts and crafts, and physics exercises such as walking outside) and interactive cycling using a stationary bicycle linked to a screen. Carry out an activity program regularly within 6 months and exercise frequency 5x/week. Three (T1) and six (T2) months reward intervention. | Perform a regular activity program within 6 months and exercise frequency 5x/week. | Third (T1) and 6th (T2) months of initial intervention. | Participants who joined the exergame group had a better increase in cognitive function on MoCA (n2p = 0.385, p = <0.001). |
| Nathalie Swinnen et al. [13] | D: Pilot randomized controlled trial S: Purposive sampling V: Dividat Senso I: MoCA A: Pre-test–post-test comparative design | The intervention lasted for 8 weeks, and the intervention was in the form of exergame and care as usual, with exergame carried out 3x/week. Participants walked first to the practice room for about 10 min before using the exergame tool for 15 min. Dividat Senso tool has a platform with sensitive steps (left, right, up, and down) with changing pressure and a connected interface. If the game gives an order for the patient to step to the right or the left, then the participant must step with the same side foot. For the sequence of steps, forward or backward, participants can use the desired foot. Intervention lasting 8 weeks, the intervention is in the form of listening to love and affection music, as usual, carried out 3x/week with a duration of 15 min. Participants walk first to the practice room for about 10 min, then watch and listen to the desired music on the TV in the same room as the exergame room. The eighth week after the initial intervention. | The intervention lasted 8 weeks, the intervention was in the form of listening to favorite music, and treatment, as usual, was carried out 3x/week with a duration of 15 min. Participants walked first to the exercise room for about 10 min, then watched and listened to the desired music on the TV in the same room as the exergame room. | Eighth week after the initial intervention. | Participants who joined the exergame group had a better increase in cognitive function on MoCA (n2p = 0.385, p = <0.001). |
| Nathalie Swinnen et al. [14] | D: Qualitative study S: Purposive sampling V: Dividat Senso I: Semi-structured interviews A: Thematic analysis | The intervention lasts 8 weeks with a frequency of 3x/week (24 sessions in total exercise). Every session practice is filled with walking going to room practice, and coming back from room exercise, as well as using a tool exergame, namely ‘Dividat Senso’. To use this tool, a participant steps on footing shaped child arrow (to the direction right, left, up, and down). Participants first stand in the middle platform and then interact with the screen interface with the method step on footing child arrow by instruction from the screen. Practice every participant conducted in a room separated and each supervised one person to ensure comfort and safety. | Fourth (mid) and eighth (post) week after the initial intervention. | Some partici-pants reported increasing positive effects on their attention and concentration. Thirty-three participants indicated that the exergame stimulated attention and concentration required. | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Noviana, M.; Syahmansyur, M.A.F.; Pratama, A.D.; Pahlawi, R.; Abdullah, F. The Effectiveness of Exergame Exercises to Improve Cognitive Function in Cases of Dementia: Literature Review. Proceedings 2022, 83, 29. https://doi.org/10.3390/proceedings2022083029
Noviana M, Syahmansyur MAF, Pratama AD, Pahlawi R, Abdullah F. The Effectiveness of Exergame Exercises to Improve Cognitive Function in Cases of Dementia: Literature Review. Proceedings. 2022; 83(1):29. https://doi.org/10.3390/proceedings2022083029
Chicago/Turabian StyleNoviana, Mita, Muhammad Alif Faruq Syahmansyur, Aditya Denny Pratama, Riza Pahlawi, and Faizah Abdullah. 2022. "The Effectiveness of Exergame Exercises to Improve Cognitive Function in Cases of Dementia: Literature Review" Proceedings 83, no. 1: 29. https://doi.org/10.3390/proceedings2022083029