
Evaluation of the Methods for Nonlinear Analysis of Heart Rate Variability





Abstract
:1. Introduction
2. Materials and Methods
- Fractal and multifractal methods: Rescaled Range (R/S), Detrended Fluctuation Analysis (DFA) and Multifractal Detrended Fluctuation Analysis (MFDFA;
- Visual methods: Poincaré plot;
- Information methods: Approximate Entropy (AppEn) and Sample Entropy (SampEn).
2.1. Fractal and Multifractal Methods
2.1.1. R/S Method
- Step 1:
- The investigated process is divided into segments of different lengths.
- Step 2:
- For each segment, the parameters are calculated: Range R(n) and standard deviation S(n) with the following formulas:
- Range R(n):where:
- Standard deviation S(n):
- Step 3:
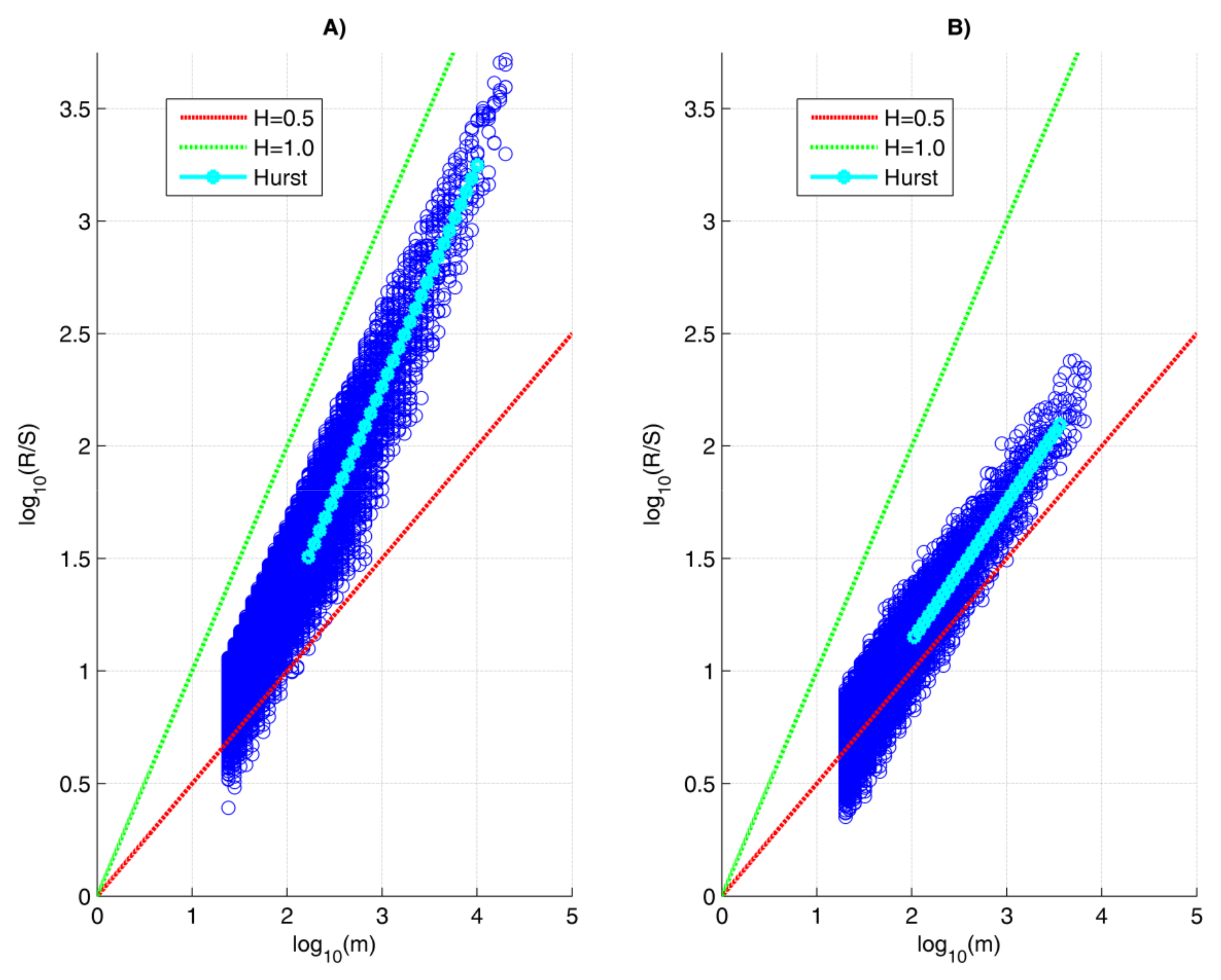
- The relationship between R(n) and S(n) is determined. A regression model between Log10(R/S) and Log10(segment size) is created. For fractal processes, the relationship between these two variables is linear.
- Step 4:
- Using the method of least squares, the slope of the regression line is determined.
- Step 5:
- The value of the Hurst exponent is determined, which is equal to the slope of the regression line.
2.1.2. Detrended Fluctuation Analysis Method
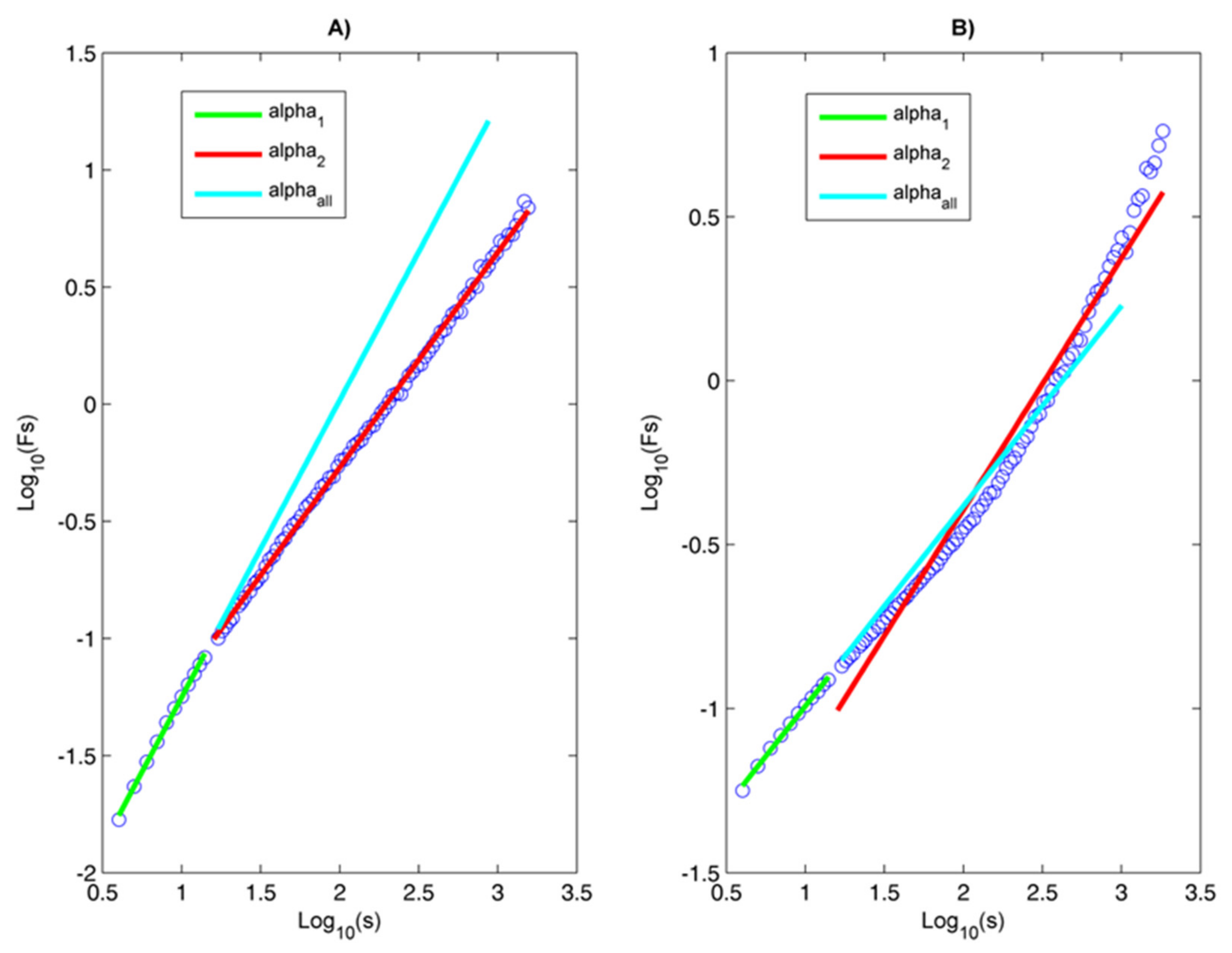
- α1 to detect short-term correlations;
- α2 to detect long-term correlations;
- αall to detect the self-similarity in the signal. If it has a value of 0.5, it is an indicator of an uncorrelated process resembling white noise, while if the value of αall is between 0.5 and 1, it is evidence of positive correlations and self-similarity (fractality) in the process. Conversely, if the process has a value for αall that is between 0 and 0.5, this is an indication of negative correlations. Using the DFA method, the coefficient of fluctuations of the process can be determined, which is related to the Hurst exponent. When the value of the parameter αall is less than or equal to 1, the resulting value of αall coincides with the value of the Hurst exponent.
- Step 1:
- For the analyzed time series X(i), i = 1, 2, …, N, a fluctuation profile with an average value is determined:
- Step 2:
- The resulting time series Y(i) is divided into Ns = int(N/s) non-overlapping segments containing an equal number of points s. In case the length of the time series N is not a multiple of s, the division procedure is repeated starting from the opposite end of the series. This results in 2N segments of length s.
- Step 3:
- The local trend for each segment is calculated using the method of least squares and the sums for the segments v = 1, N and v = Ns + 1, …, 2N are determined:
- Step 4:
- A summation is performed for all segments, resulting in the following fluctuation function:
- Step 5:
- Steps 2 to 4 are repeated for different values of the parameter s. The fluctuation function is determined:
2.1.3. Multifractal Detrended Fluctuation Analysis Method
- Step 4:
- The Fq(s) function is determined for the following two cases: q ≠ 0; q → 0.
- Step 5:
- For a fixed value of q, the graphical dependence of log Fq(s) vs. log(s) is plotted. If the studied time series has a fractal behavior, then Fq(s) changes according to the power law:where h(q) is called the generalized Hurst exponent.
- Step 6:
- For different values of the parameter q, steps 1 to 5 are repeated.
- The fluctuation function Fq(s) is the same for all segments v into which the studied process is divided;
- The generalized Hurst exponent h(q) = H does not depend on the parameter q and is a constant quantity;
- They are characterized by a linear increase of the function τ(q);
- They have a narrow multifractal spectrum F(α).
- The fluctuation function Fq(s) is different for the different segments v into which the process is divided;
- The generalized Hurst exponent is not a constant quantity, but depends on the change of the parameter q;
- The function τ(q) increases nonlinearly;
- The multifractal spectrum F(α) is wide.
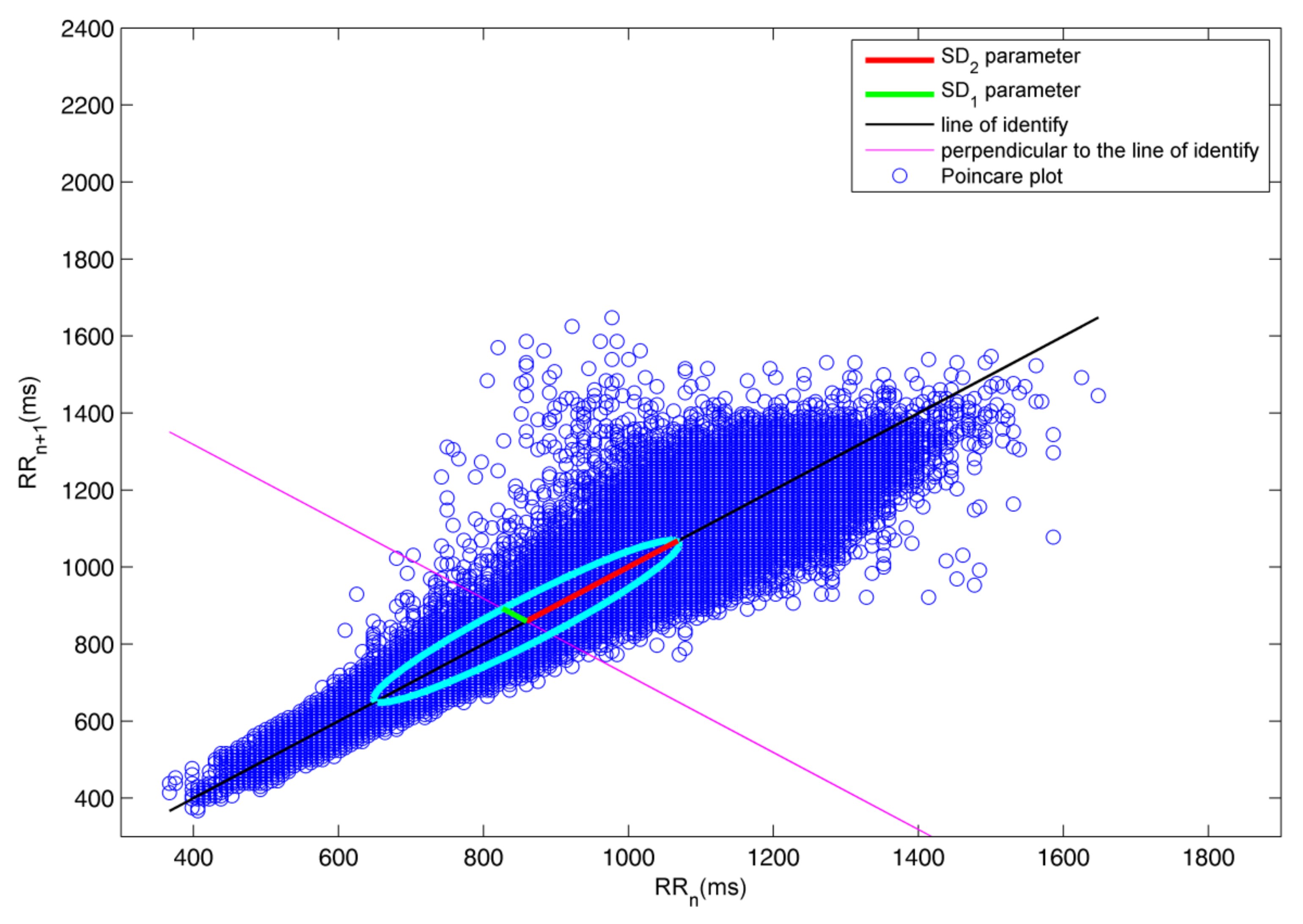
2.2. Poincaré Plot
- SD2 [ms] parameter, which corresponds to the semimajor axis of the ellipse and lies on a line that is perpendicular to the line of identity. This parameter corresponds to the long-term variability of the RR intervals;
- SD1 [ms] parameter, which corresponds to the semiminor axis of the ellipse and lies on the line of identity. This parameter is related to the rapid variations between heartbeats;
- The SD1/SD2 ratio, which shows the relationship between the short- and long-term HRV.
- n are the number of points in the graph;
- var(d) is the variance of d;
- ; .
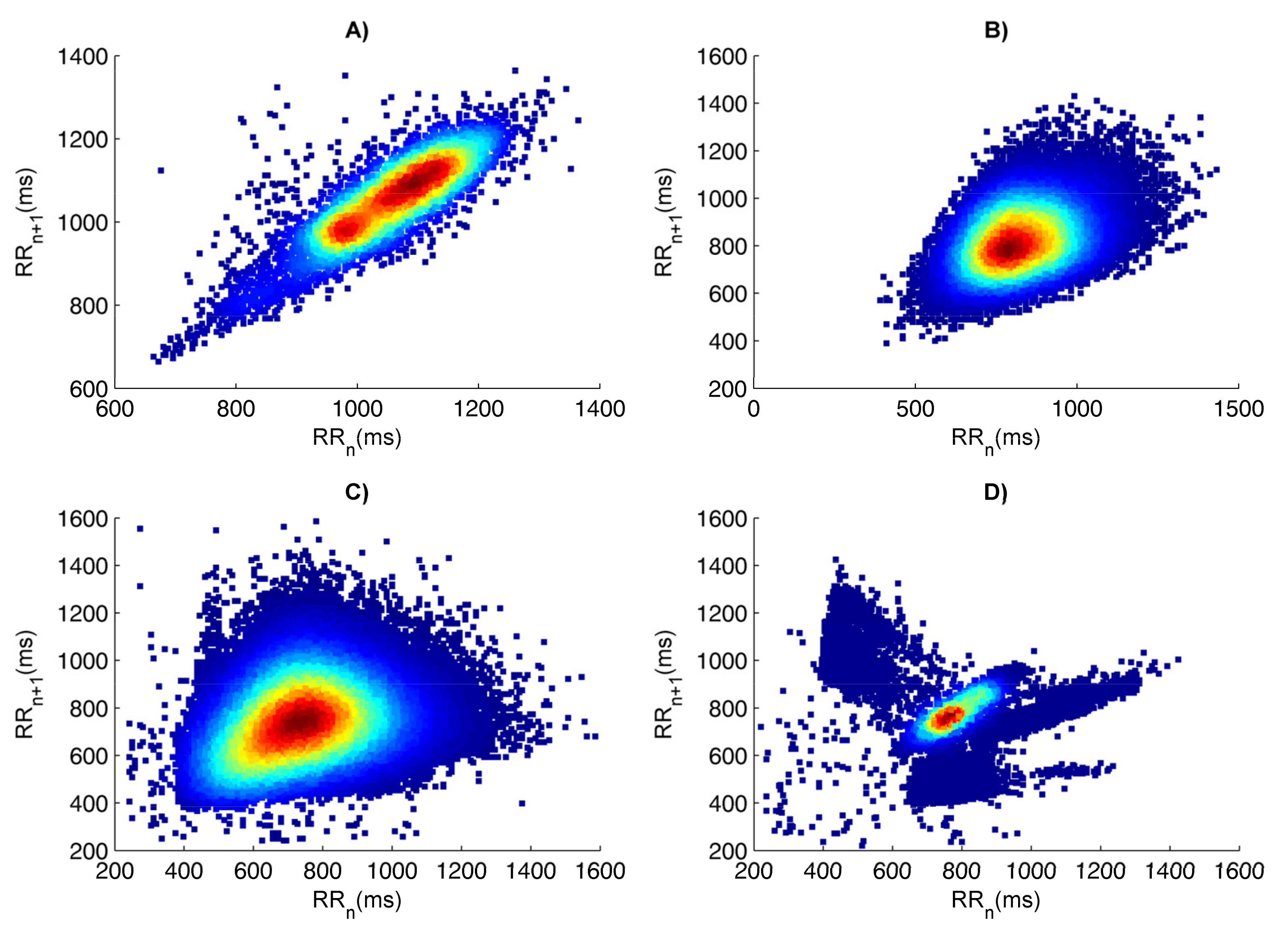
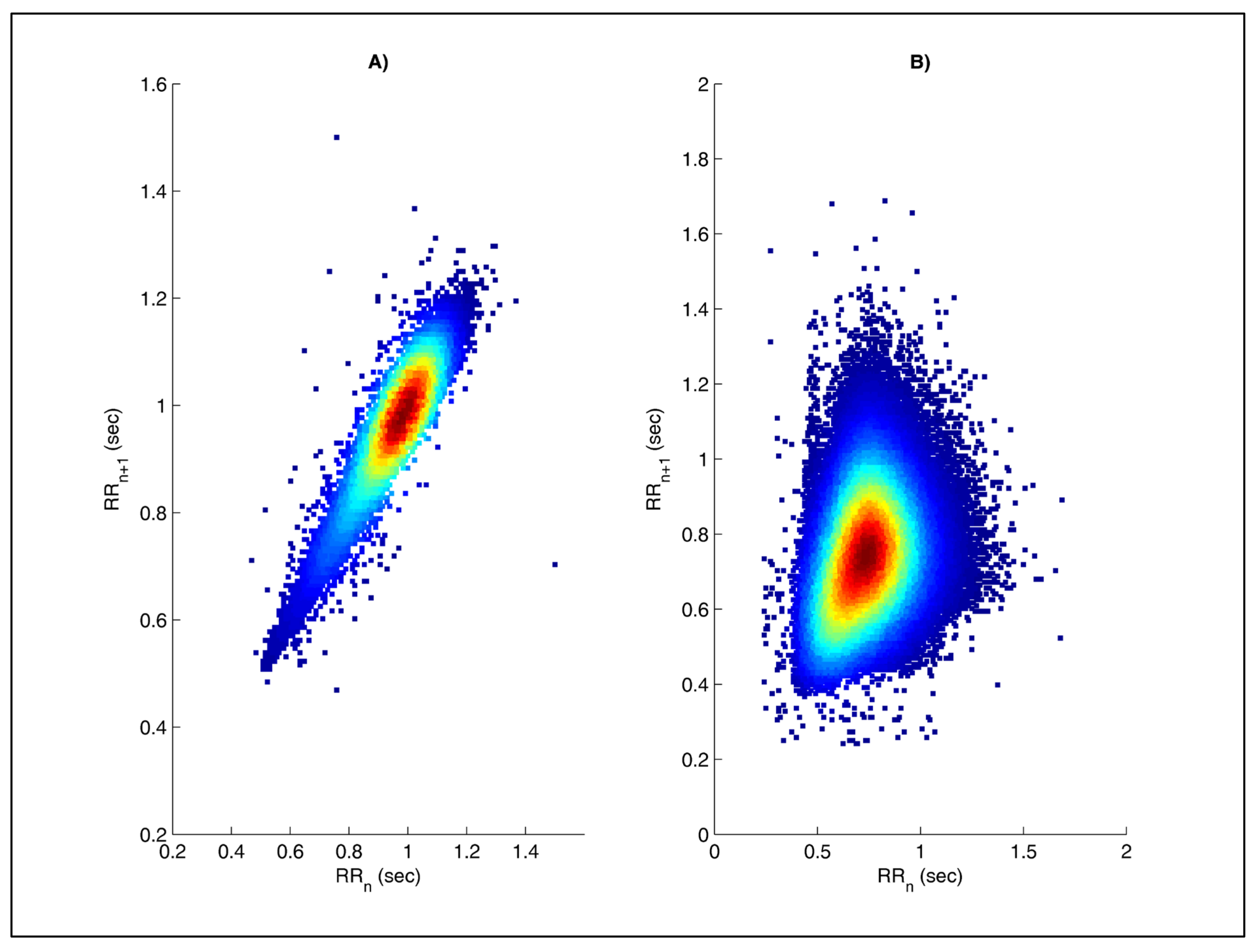
- The graph of the healthy subject has one main segment of points to which more points may be evenly scattered. The main segment is comet-shaped with a narrow lower part and gradually widening towards the apex (Figure 2A);
2.3. Approximate Entropy and Sample Entropy
- Subseries length (m);
- Tolerance (r);
- Data length (N).
- d is the distance between the vectors.
2.4. Data
- Group 1 (healthy subjects) consisted of 25 subjects, of which 15 were male and 10 were female. The average age for this group is 56.3 years.
- Group 2 (arrhythmia patients) consisted of 25 patients, of which 13 were men and 12 were women. The average age of the group is 58.7 years.
2.5. Receiver Operating Characteristics Analysis
- If the AUC is in the interval 0.9–1.0, the quality of the parameter used is excellent;
- If the AUC is in the interval 0.8–0.9, the quality of the parameter used is very good;
- If the AUC is in the interval 0.7–0.8, the quality of the parameter used is good;
- If the AUC is in the interval 0.5–0.6, the quality of the method used is unsatisfactory.
3. Results and Discussion
3.1. Evaluation of the Fractal and Multifractal Methods for the Analysis of HRV
3.1.1. Evaluation of the R/S Method
3.1.2. Evaluation of the DFA Method
- The values of α1, α2 and αall are higher in healthy people;
- The value of the parameter αall in healthy and diseased subjects varies between 0.5 and 1.0, which is close to the value of the Hurst exponent determined by the R/S method;
- The parameters α1, α2 and αall have statistical significance determined by t-test; therefore, with this method, the two groups can be distinguished;
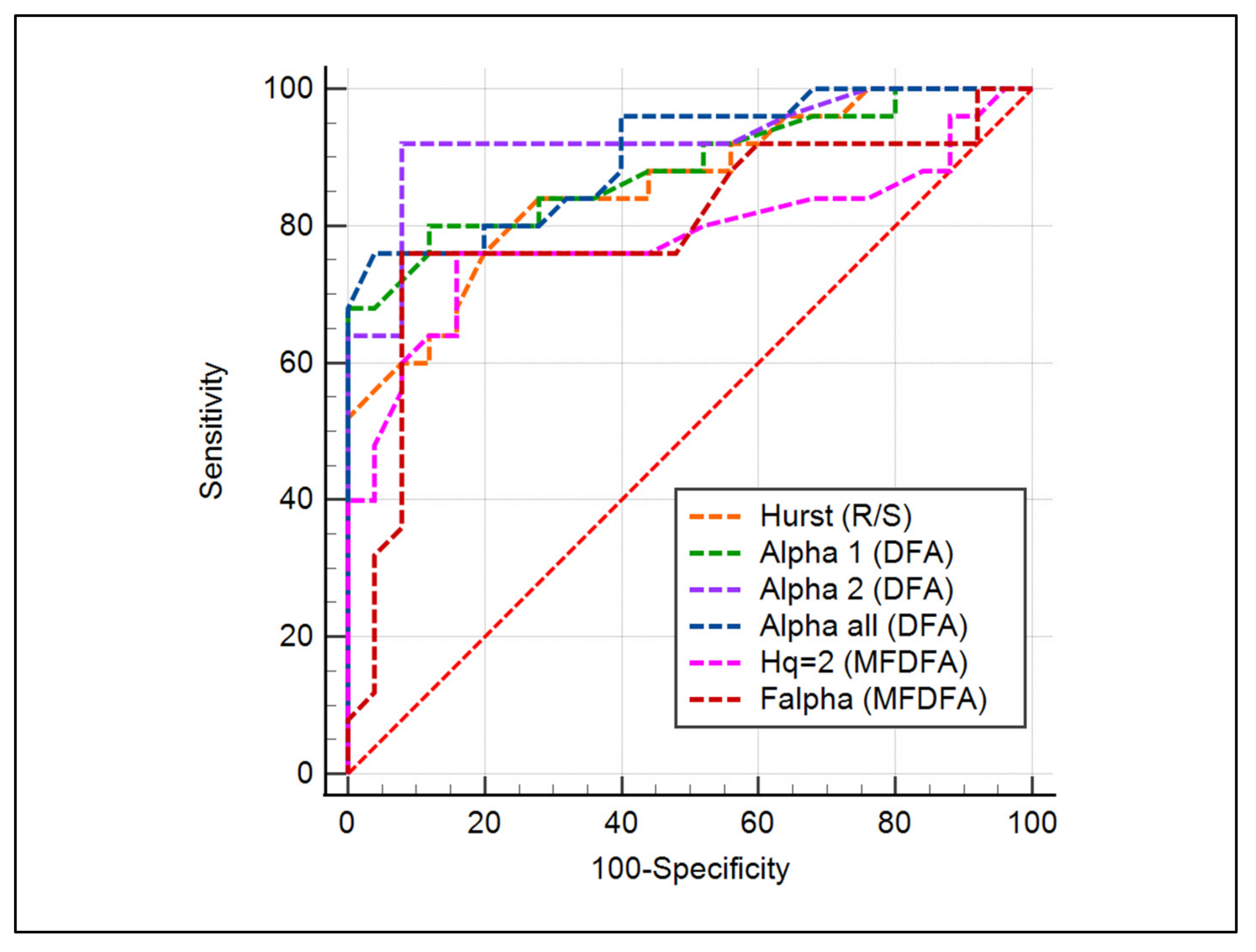
- Quantitative AUC evaluation shows that one of the parameters (α1) has a very good diagnostic score and the other two (α2 and αall) have an excellent score. Quantitative AUC evaluation shows that one of the parameters (α1) has a very good diagnostic score, and the other two (α2 and αall) have an excellent score; the graphs for the three parameters obtained by the ROC analysis are shown in Figure 5.
3.1.3. Evaluation of the MFDFA Method
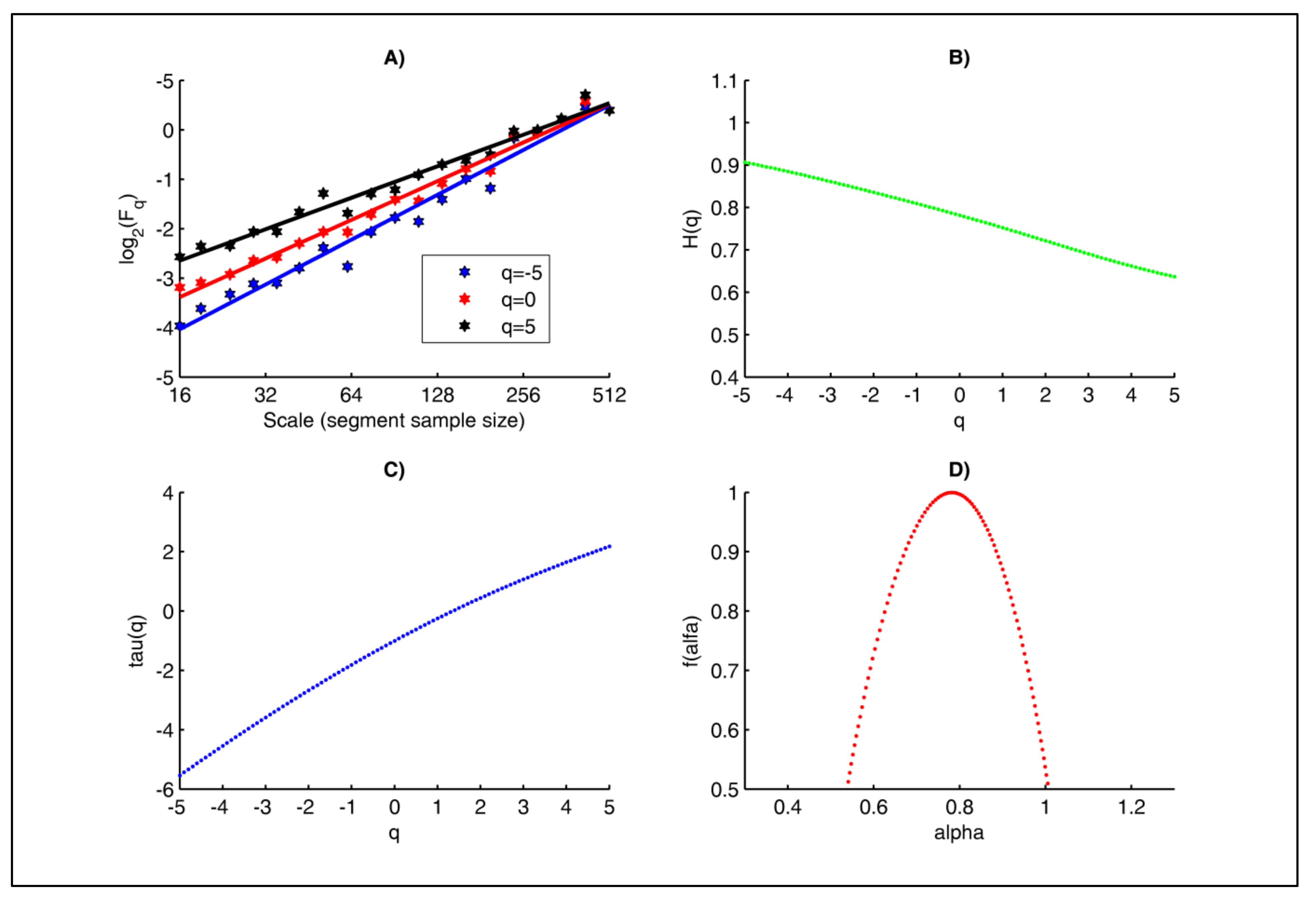
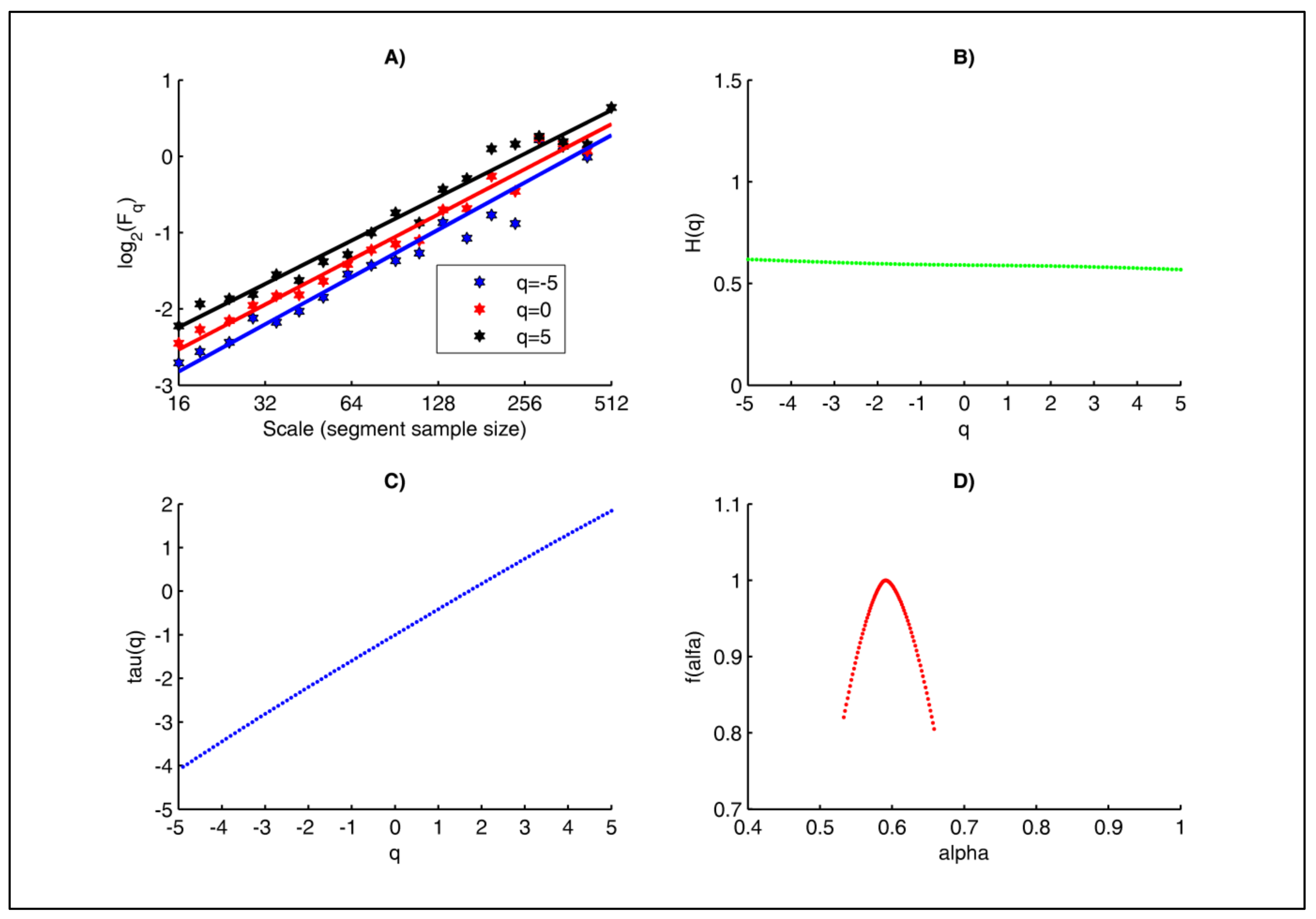
- The graphs of the Fq(scale) function for different values of the parameter q shown in Figure 6A and Figure 7A are for a healthy subject and an unhealthy subject (arrhythmia patient). The graphs for both subjects are straight lines, i.e., the studied RR time series are scale-invariant and therefore exhibit fractal behavior. The slopes of the Fq vs. q corresponding to a healthy individual are different, which is evidence of multifractal behavior of the studied cardiac signal. The graphs for the unhealthy subject are parallel, i.e., the slope of the oscillation functions is constant, and this observation can be interpreted as monofractal behavior;
- Figure 6B and Figure 7B show the dependence of the generalized Hurst exponent H(q) versus q for the RR time intervals of healthy and unhealthy subjects. The range of values of the Hurst exponent for a healthy subject varies from 0.9 to 0.6 in the case of different values of the q parameter. Therefore, the RR intervals for healthy subjects have a multifractal behavior. In the case of an unhealthy subject (arrhythmia patient), the Hurst exponent is a constant at different values of the q parameters; therefore, the investigated signal has a monofractal behavior. From the graph in Figure 6B, for the healthy patient it can be seen that H(q = 2) = 0.7848, and for the diseased patient (Figure 6B) H(q = 2) = 0.5912. In Table 1 are shown the values of this parameter for the two studied groups. This parameter has statistical significance (p < 0.05), and the determined AUC value is 0.789;
- Figure 6C and Figure 7C show the tau(q) curves of healthy and unhealthy subjects. When the function tau(q) is a convex curve, this is evidence that the studied signal has a multifractal behavior. In the case where tau(q) is a straight line, this is evidence that the signal is monofractal. Therefore, the RR time intervals of the healthy subjects have a multifractal behavior, while the signals of the patients with arrhythmia are monofractals;
- The graphs on Figure 6D and Figure 7D illustrate the multifractal spectrum of RR intervals for healthy and unhealthy individuals. The multifractal spectrum of the RR intervals of the healthy subject (Figure 6D) is Δα = αmax − αmin = 1.0077 − 0.5224 = 0.4853, while for the unhealthy subject (Figure 6D) it is Δα = αmax − αmin =0.6580 − 0.5329 = 0.1251. The signal of the healthy subject has a broad multifractal spectrum, while the signal of the unhealthy subject (arrhythmia patient) has a narrow multifractal spectrum that is about 4 times smaller than that of the healthy subject. The graph in Figure 7D corresponding to the arrhythmia patient is an example of a monofractal process. In Table 1 are shown the values of the multifractal spectrum of the two studied groups. The value of this parameter is higher in healthy individuals, which is due to the higher HRV. This parameter has statistical significance (p < 0.05), and the determined value of AUC (Figure 8) is 0.798.
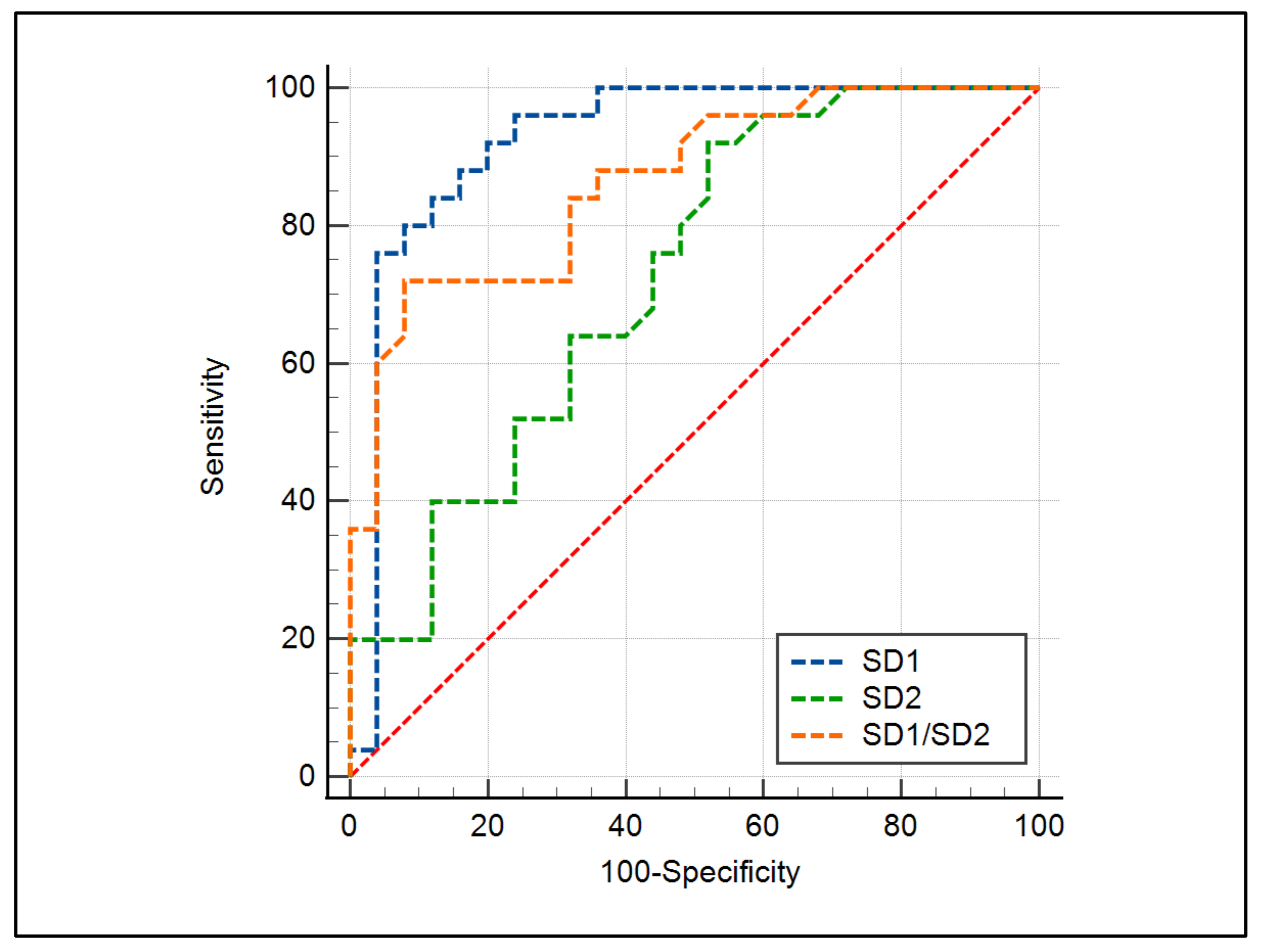
3.2. Evaluation of the Poincaré Plot
- SD1 = 0.925—the parameter has an excellent diagnostic value;
- SD2 = 0.725—the parameter has a good diagnostic value;
- SD1/SD2 = 0.863—the parameter has a very good diagnostic value.
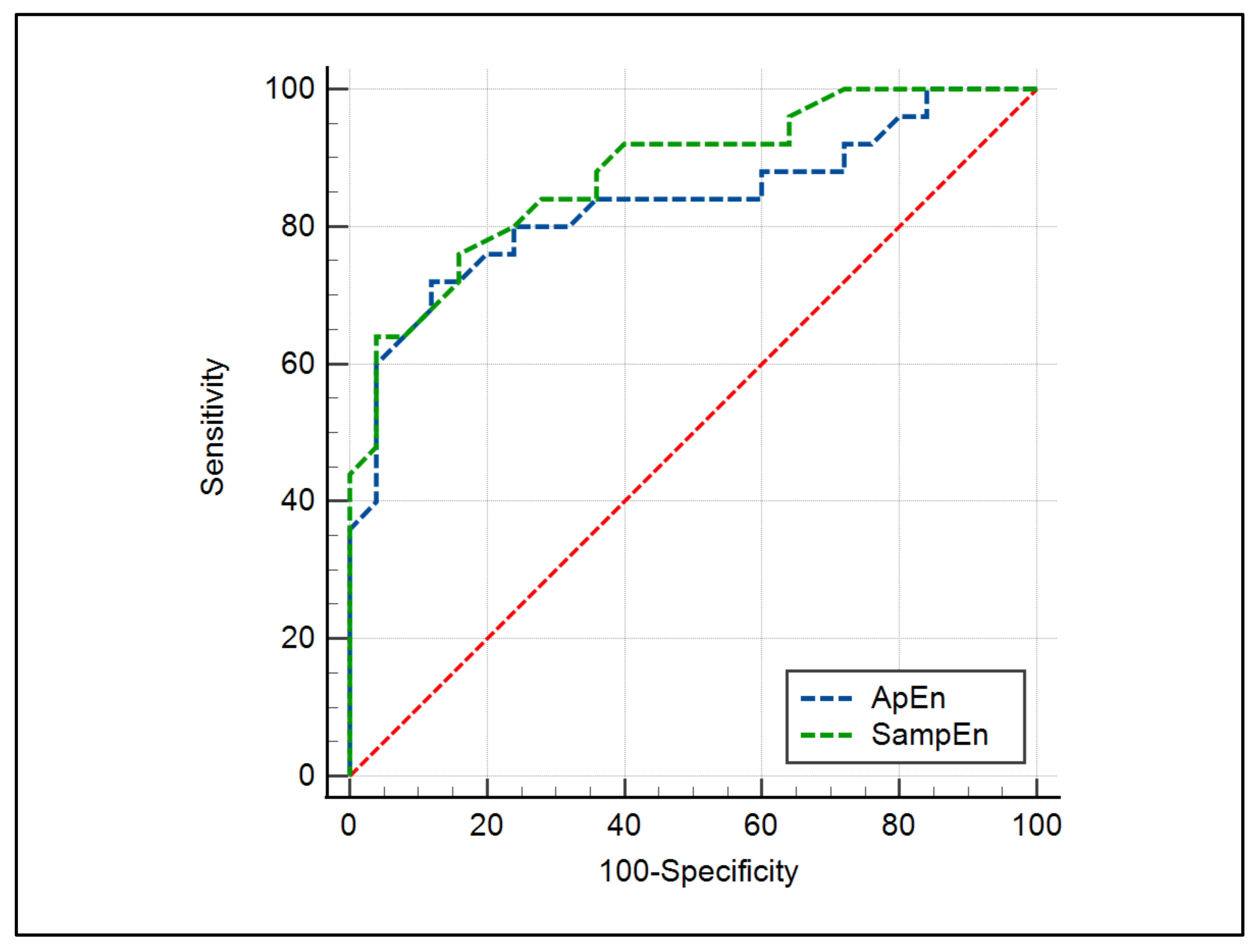
3.3. Evaluation of the ApEn and SampEn Methods
- The values of ApEn and SampEn were higher for the healthy subjects compared to those of the diseased subjects; therefore, the RR intervals of healthy subjects had greater complexity;
- For the two studied parameters ApEn and SampEn, the p-value is less than 0.05; therefore, these parameters have statistical significance, which makes it possible to distinguish between the two investigated groups;
- From the determined AUC values for ApEn and SampEn, it follows that a very good diagnostic score is obtained with these two methods.
4. Conclusions
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Haque, M.; Tariq, M.; Hussain, T. Presence of Multifractality in High-Energy Nuclear Collisions. J. Mod. Phys. 2014, 5, 1889–1895. [Google Scholar] [CrossRef]
- Rafique, M.; Javid, I.; Javed, L.K.; Jane, K.K.; Saeed, U.R.; Lal, H. Multifractal detrended fluctuation analysis of soil radon (222Rn) and thoron (220Rn) time series. J. Radioanal. Nucl. Chem. Vol. 2021, 328, 425–434. [Google Scholar] [CrossRef]
- Miloş, L.R.; Haţiegan, C.; Miloş, M.C.; Barna, F.M.; Boțoc, C. Multifractal Detrended Fluctuation Analysis (MF-DFA) of Stock Market Indexes Empirical Evidence from Seven Central and Eastern European Markets. Sustainability 2020, 12, 535. [Google Scholar] [CrossRef]
- Goldberger, A.L. Fractal variability versus pathologic periodicity: Complexity loss and stereotypy in disease. Perspect. Biol. Med. 1996, 4, 543–561. [Google Scholar] [CrossRef]
- Das, N.; Chatterjee, S.; Kumar, S.; Pradhan, A.; Panigrahi, P.; Vitkin, I.A.; Ghosh, N. Tissue multifractality and Born approximation in analysis of light scattering: A novel approach for precancers detection. Sci. Rep. 2014, 20, 6129. [Google Scholar] [CrossRef]
- Das, N.; Alexandrov, S.; Gilligan, K.E.; Dwyer, R.M.; Saager, R.B.; Ghosh, N.; Leahy, M. Characterization of nanosensitive multifractality in submicron scale tissue morphology and its alteration in tumor progression. J. Biomed. Opt. 2021, 26, 016003. [Google Scholar] [CrossRef]
- Owis, M.I.; Abou-Zied, A.H.; Youssef, A.-B.M.; Kadah, Y.M. Study of features based on nonlinear dynamical modeling in ECG arrhythmia detection and classification. IEEE Trans. Biomed. Eng. 2002, 49, 733–736. [Google Scholar] [CrossRef]
- Kumar, P.; Das, A.K.; Halder, S. Time-domain HRV Analysis of ECG Signal under Different Body Postures. Procedia Comput. Sci. 2020, 167, 1705–1710. [Google Scholar] [CrossRef]
- Kumar, D.M.; Prasannakumar, S.C.; Sudarshan, B.G.; Jayadevappa, D. Heart Rate Variability Analysis: A Review. Int. J. Adv. Technol. Eng. Sci. 2013, 1, 9–24. [Google Scholar]
- Costa, M.D.; Davis, R.B.; Goldberger, A.L. Heart rate fragmentation: A new approach to the analysis or cardiac interbeat internal dynamics. Front. Psychol 2017, 8, 255. [Google Scholar] [CrossRef]
- Malik, M. Task Force of the European Society of Cardiology and the North American Society of Pacing and Electrophysiology, Heart rate variability—Standards of measurement, physiological interpretation, and clinical use. Circulation 1996, 93, 1043–1065. [Google Scholar] [CrossRef]
- Eke, A.; Herman, P.; Kocsis, L.; Kozak, L.R. Fractal characterization of complexity in temporal physiological signals. Physiol. Meas. 2002, 23, R1–R38. [Google Scholar] [CrossRef] [PubMed]
- Ivanov, P.; Amaral, L.; Goldberger, A.; Halvin, S.; Rosenblum, M.; Stanley, H.; Struzik, Z. From 1/f noise to multifractal cascades in heartbeat dynamics. Chaos 2001, 11, 641–652. [Google Scholar] [CrossRef] [PubMed]
- Ivanov, P.; Chen, Z.; Hu, K.; Stanley, H. Multiscale aspects of cardiac control. Phys. A 2004, 344, 685–704. [Google Scholar] [CrossRef]
- Ivanov, P.; Amaral, L.; Goldberger, A.; Halvin, S.; Rosenblum, M.; Stanley, H.; Struzik, Z. Multifractality in human heartbeat dynamics. Nature 1999, 399, 461–465. [Google Scholar] [CrossRef]
- Acharya, U.R.; Suri, J.S.; Spaan, J.A.E.; Krishnan, A.M. Advances in Cardiac Signal Processing; Springer: Berlin/Heidelberg, Germany, 2007. [Google Scholar] [CrossRef]
- Kleiger, R.; Miller, J.; Bigger, J.; Moss, A.J. Decreased Heart Rate Variability and It‘s Association with Increased Mortality After Acute Myocardial Infarction. Am. J. Cardiol. 1987, 59, 256–262. [Google Scholar] [CrossRef]
- Glenny, R.W.; Robertson, H.T.; Yamashiro, S.; Bassingthwaighte, J.B. Applications of fractal analysis to physiology. J. Appl. Physiol. 1985, 70, 2351–2367. [Google Scholar] [CrossRef]
- Haykin, S.; Li, X.B. Detection of signals in chaos. Proc. IEEE 1995, 83, 95–122. [Google Scholar] [CrossRef]
- Kale, M.; Butar, F.B. Fractal analysis of Time Series and Distribution Properties of Hurst Exponent. J. Math. Sci. Math. Educ. 2011, 5, 8–19. [Google Scholar]
- Kalisky, T.; Ashkenazy, Y.; Havlin, S. Volatility of fractal and multifractal time series. Isr. J. Earth Sci. 2007, 65, 47–56. [Google Scholar] [CrossRef]
- Wang, J.; Ning, Y.; Chen, Y. Multifractal analysis of electronic cardiogram taken from healthy and unhealthy adult subjects. Phys. A 2003, 323, 561–568. [Google Scholar] [CrossRef]
- Martinis, M.; Knežević, A.; Krstačić, G.; Vargović, E. Changes in the Hurst exponent of heart beat intervals during physical activities. Phys. Rev. E 2004, 70, 012903. [Google Scholar] [CrossRef] [PubMed]
- Sheluhin, O.I.; Smolskiy, S.M.; Osin, A.V. Self-Similar Processes in Telecommunications; John Wiley & Sons, Ltd.: England, UK, 2006. [Google Scholar]
- Biswas, A.; Zeleke, T.B.; Si, B.C. Multifractal detrended fluctuation analysis in examining scaling properties of the spatial patterns of soil water storage. Nonlinear Process Geophys. 2012, 19, 227–238. [Google Scholar] [CrossRef]
- Delgado-Bonal, A.; Marshak, A. Approximate Entropy and Sample Entropy: A Comprehensive Tutorial. Entropy. Entropy 2019, 21, 541. [Google Scholar] [CrossRef]
- Yentes, J.M.; Hunt, N.; Schmid, K.K.; Kaipust, J.P.; McGrath, D.; Stergiou, N. The Appropriate Use of Approximate Entropy and Sample Entropy with Short Data Sets. J. Artic. 2013, 44, e21060541. [Google Scholar] [CrossRef]
- Tarvainen, M.P.; Lipponen, J.; Niskanen, J.P.; Ranta-Aho, P. Kubios HRV Version 3—User’s Guide. Kuopio: University of Eastern Finland 2016–2021. Available online: www.kubios.com (accessed on 3 November 2021).
- Hurst, H.E.; Black, R.P.; Sinaika, Y.M. Long-Term Storage in Reservoirs: An Experimental Study; Constable: London, UK, 1965. [Google Scholar]
- Nikolopoulos, D.; Moustris, K.; Petraki, E.; Koulougliotis, D.; Cantzos, D. Fractal and Long-Memory Traces in PM10 Time Series in Athens, Greece. Environments 2019, 6, 29. [Google Scholar] [CrossRef]
- Brătian, V.; Acu, A.-M.; Oprean-Stan, C.; Dinga, E.; Ionescu, G.-M. Efficient or Fractal Market Hypothesis? A Stock Indexes Modelling Using Geometric Brownian Motion and Geometric Fractional Brownian Motion. Mathematics 2021, 9, 2983. [Google Scholar] [CrossRef]
- Mielniczuk, J.; Wojdyllo, P. Estimation of Hurst exponent revisited. Comput. Stat. Data Anal. 2007, 51, 4510–4525. [Google Scholar] [CrossRef]
- Naiman, E. The Hurst Index Calculation to Identify Persistence of the Financial Markets and Macroeconomic Indicators. Ukr. J. Ekon. 2009, 10, 18–28. [Google Scholar]
- Peng, C.-K.; Buldyrev, S.V.; Havlin, S.; Simons, M.; Stanley, H.E.; Goldberger, A.L. Mosaic organization of dna nucleotides. Phys. Rev. E. Stat. Phys. Plasmas Fluids Relat. Interdiscip. Top. 1994, 49, 1685–1689. [Google Scholar] [CrossRef]
- Peng, C.-K.; Havlin, S.; Stanley, H.E.; Goldberger, A.L. Quantification of scaling exponents and crossover phenomena in nonstationary heartbeat time series. Chaos 1995, 5, 82–87. [Google Scholar] [CrossRef] [PubMed]
- Costa, N.; Silva, C.; Ferreira, P. Long-range behaviour and correlation in detrended fluctuation analysis and DCCA analysis of cryptocurrencies. Int. J. Financ. Stud. 2019, 7, 51. [Google Scholar] [CrossRef]
- Golińska, A.K. Detrended Fluctuation Analysis (DFA) in Biomedical Signal Processing: Selected Examples. Stud. Log. Gramm. Rhetor. 2012, 29, 107–115. [Google Scholar]
- Hardstone, R.; Poil, S.-S.; Schiavone, G.; Jansen, R.; Nikulin, V.V.; Mansvelder, H.D.; Linkenkaer-Hansen, K. Detrended Fluctuation Analysis: A Scale-Free View on Neuronal Oscillations. Front. Physiol. 2012, 3, 450. [Google Scholar] [CrossRef]
- Maraun, D.; Rust, H.W.; Timmer, J. Tempting long-memory—On the interpretation of DFA results. Nonlinear Process. Geophys. Eur. Geosci. Union 2004, 11, 495–503. [Google Scholar] [CrossRef]
- Kantelhardt, J.W.; Zschiegner, S.A.; Koscielny-Bunde, E.; Havlin, S.; Bunde, A.; Stanley, H.E. Multifractal detrended fluctuation analysis of nonstationary time series. Phys. A: Stat. Mech. Its Appl. 2002, 316, 87–114. [Google Scholar] [CrossRef]
- Sassi, R.; Gabriella, M.S.; Cerutti, S. Multifractality and heart rate variability. Chaos 2009, 19, 028507. [Google Scholar] [CrossRef]
- Li, E.; Mu, X.; Zhao, G.; Gao, P. Multifractal Detrended Fluctuation Analysis of Streamflow in the Yellow River Bain, China. Water 2015, 7, 1670–1686. [Google Scholar] [CrossRef]
- Salat, H.; Murcio, R.; Arcaute, E. Multifractal methodology. Phys. A Stat. Mech. 2017, 473, 467–487. [Google Scholar] [CrossRef]
- Ernst, G. Heart Rate Variability; Springer: London, UK, 2014. [Google Scholar] [CrossRef]
- Byun, S.; Kim, A.Y.; Jang, E.H.; Kim, S.; Choi, K.W.; Yu, H.Y.; Jeon, H.J. Entropy analysis of heart rate variability and its application to recognize major depressive disorder: A pilot study. Technol. Health Care 2019, 27, 407–424. [Google Scholar] [CrossRef]
- Montesinos, L.; Castaldo, R.; Pecchia, L. On the use of approximate entropy and sample entropy with centre of pressure time-series. J. Neuroeng. Rehabil 2018, 15, 116. [Google Scholar] [CrossRef] [PubMed]
- Pincus, S.M. Approximate entropy as a measure of system complexity. Proc. Nati. Acad. Sci. USA 1991, 88, 2297–2301. [Google Scholar] [CrossRef] [PubMed]
- Krupinski, E.A. Receiver Operating Characteristic (ROC) Analysis. Frontline Learn. Res. 2017, 5, 31–42. [Google Scholar] [CrossRef]
- Salcedo-Martínez, A.; Zamora-Justo, J.A.; Muñoz-Diosdado, A. Analysis of the Hurst exponent in RR series of healthy subjects and congestive patients in a state of sleep and wakefulness and in healthy subjects in physical activity. AIP Conf. Proc. 2021, 2348, 040009. [Google Scholar] [CrossRef]
- Gospodinova, E. Fractal time series analysis by using entropy and hurst exponent. In Proceedings of the 23rd International Conference on Computer Systems and Technologies, Ruse, Bulgaria, 17–18 June 2022; pp. 69–75. [Google Scholar] [CrossRef]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameters | Group 1 (Mean ± Std) | Group 2 (Mean ± Std) | AUC | 95% Confidence Interval | p-Value |
|---|---|---|---|---|---|
| Fractal and Multifractal Methods | |||||
| H (R/S) | 0.981 ± 0.01 | 0.701 ± 0.07 | 0.852 | 0.721 to 0.937 | <0.0001 |
| α1 (DFA) | 1.106 ± 0.21 | 0.723 ± 0.18 | 0.879 | 0.754 to 0.955 | <0.0001 |
| α2 (DFA) | 1.042 ± 0.08 | 0.805 ± 0.07 | 0.926 | 0.814 to 0.981 | <0.0001 |
| αall (DFA) | 0.973 ± 0.02 | 0.745 ± 0.03 | 0.918 | 0.791 to 0.972 | <0.0001 |
| Hq=2 (MFDFA) | 0.978 ± 0.04 | 0.699 ± 0.06 | 0.789 | 0.638 to 0.886 | <0.0001 |
| F(α) (MFDFA) | 0.550 ± 0.18 | 0.201 ± 0.05 | 0.798 | 0.660 to 0.898 | <0.0001 |
| Poincaré plot | |||||
| SD1 [ms] | 29.12 ± 10.19 | 145.46 ± 31.01 | 0.925 | 0.814 to 0.980 | <0.0001 |
| SD2 [ms] | 175.15 ± 41.22 | 210.70 ± 25.12 | 0.725 | 0.580 to 0.842 | 0.0006 |
| SD1/SD2 | 0.141 ± 0.11 | 0.723 ± 0.13 | 0.863 | 0.736 to 0.944 | <0.0001 |
| Entropy Methods | |||||
| ApEn | 1.592 ± 0.15 | 1.212 ± 0.19 | 0.832 | 0.700 to 0.923 | <0.0001 |
| SampEn | 1.697 ± 0.21 | 1.351 ± 0.20 | 0.876 | 0.752 to 0.952 | <0.0001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gospodinova, E.; Lebamovski, P.; Georgieva-Tsaneva, G.; Negreva, M. Evaluation of the Methods for Nonlinear Analysis of Heart Rate Variability. Fractal Fract. 2023, 7, 388. https://doi.org/10.3390/fractalfract7050388
Gospodinova E, Lebamovski P, Georgieva-Tsaneva G, Negreva M. Evaluation of the Methods for Nonlinear Analysis of Heart Rate Variability. Fractal and Fractional. 2023; 7(5):388. https://doi.org/10.3390/fractalfract7050388
Chicago/Turabian StyleGospodinova, Evgeniya, Penio Lebamovski, Galya Georgieva-Tsaneva, and Mariya Negreva. 2023. "Evaluation of the Methods for Nonlinear Analysis of Heart Rate Variability" Fractal and Fractional 7, no. 5: 388. https://doi.org/10.3390/fractalfract7050388