


Image Segmentation for Mitral Regurgitation with Convolutional Neural Network Based on UNet, Resnet, Vnet, FractalNet and SegNet: A Preliminary Study


Abstract
:1. Introduction
- Designing a CNN model for segmentation of Mitral Regurgitation heart valve disease with high Accuracy
- Developed CNN-based U-Net3 architecture for segmentation of Mitral Valve disease and normal valve condition
- Validating U-Net3 model with six other architectures using pixel accuracy, intersection over union, mean accuracy, precision, recall, and dice coefficient
2. Materials and Methods
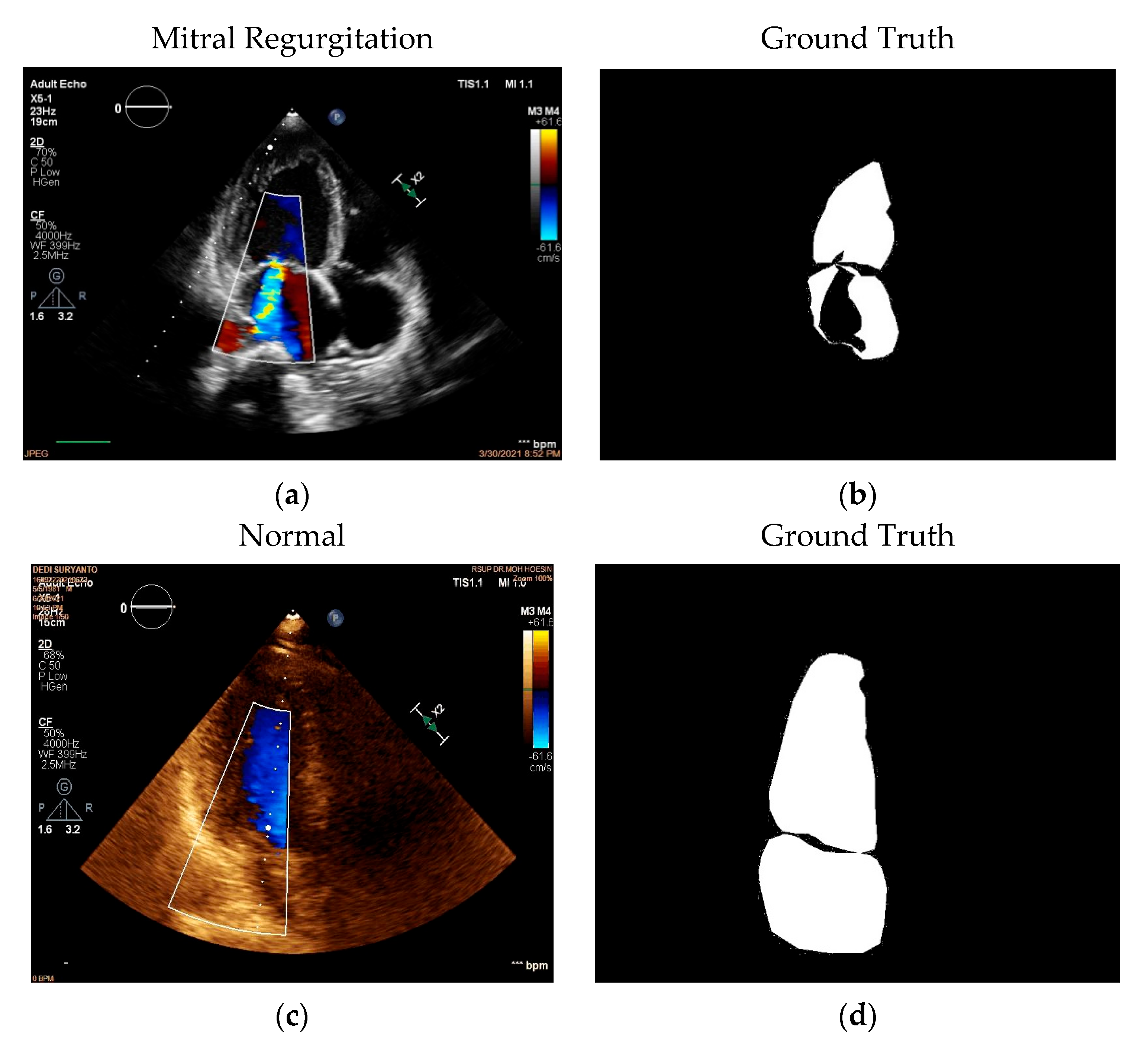
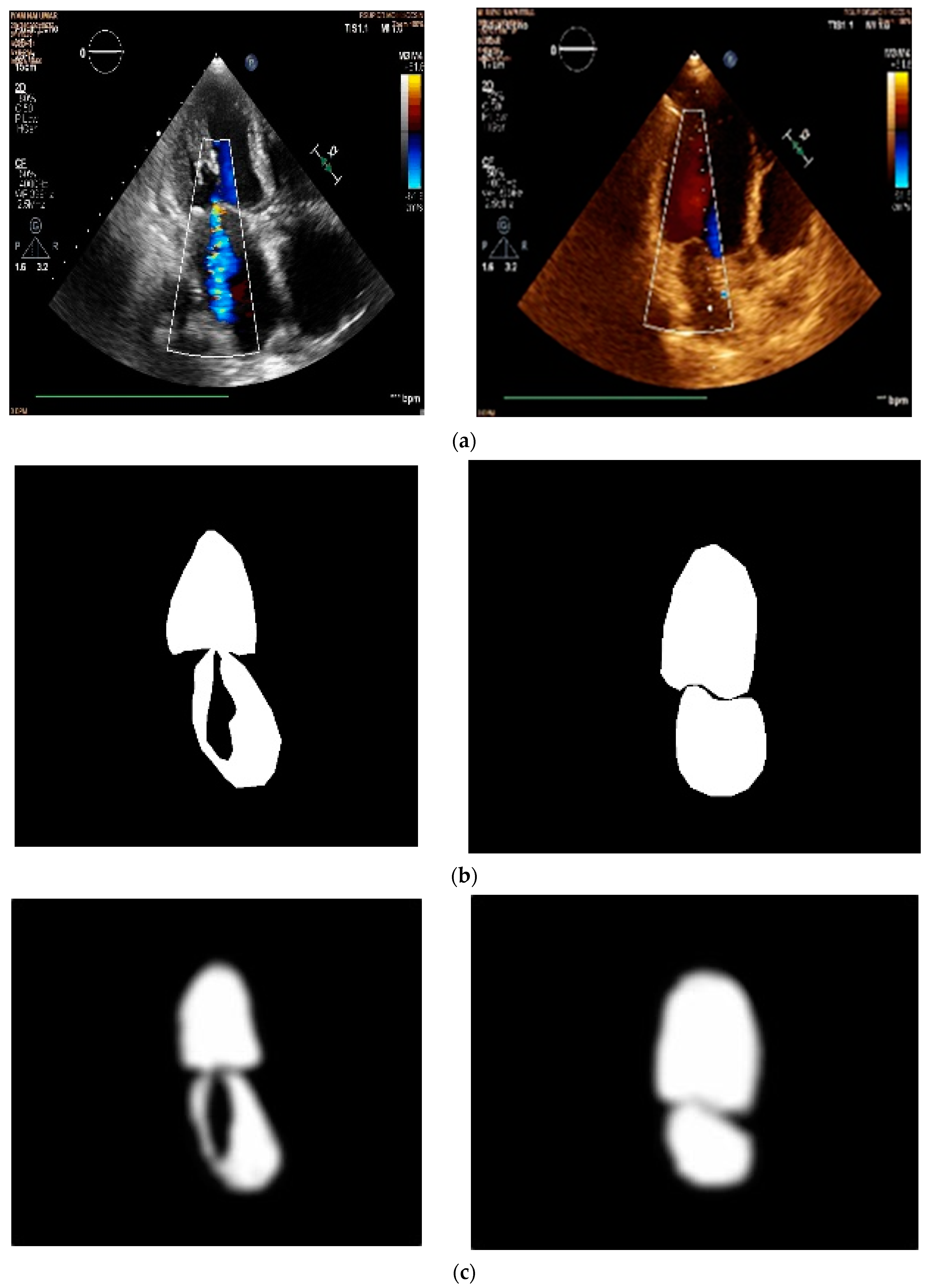
2.1. Data Acquisition
2.2. Data Pre-Processing
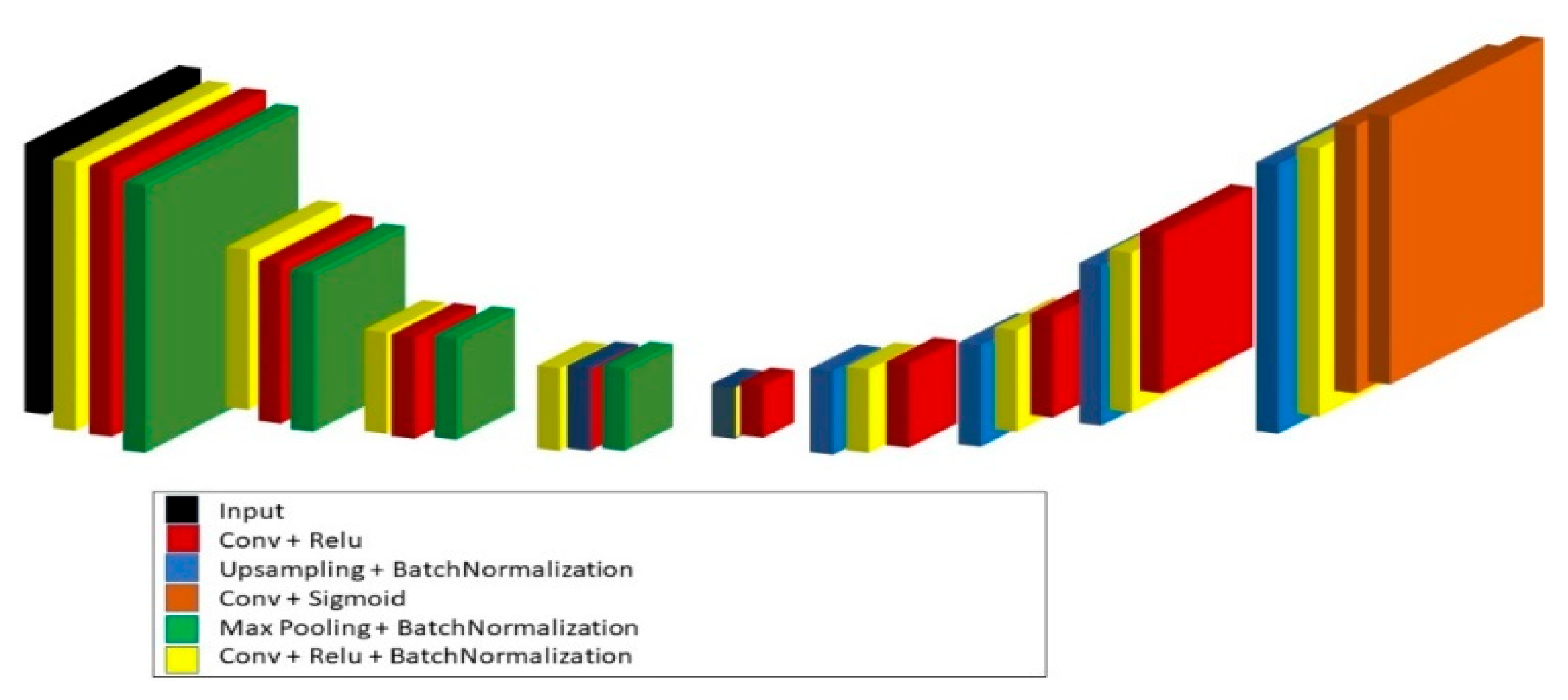
2.3. Model Architecture
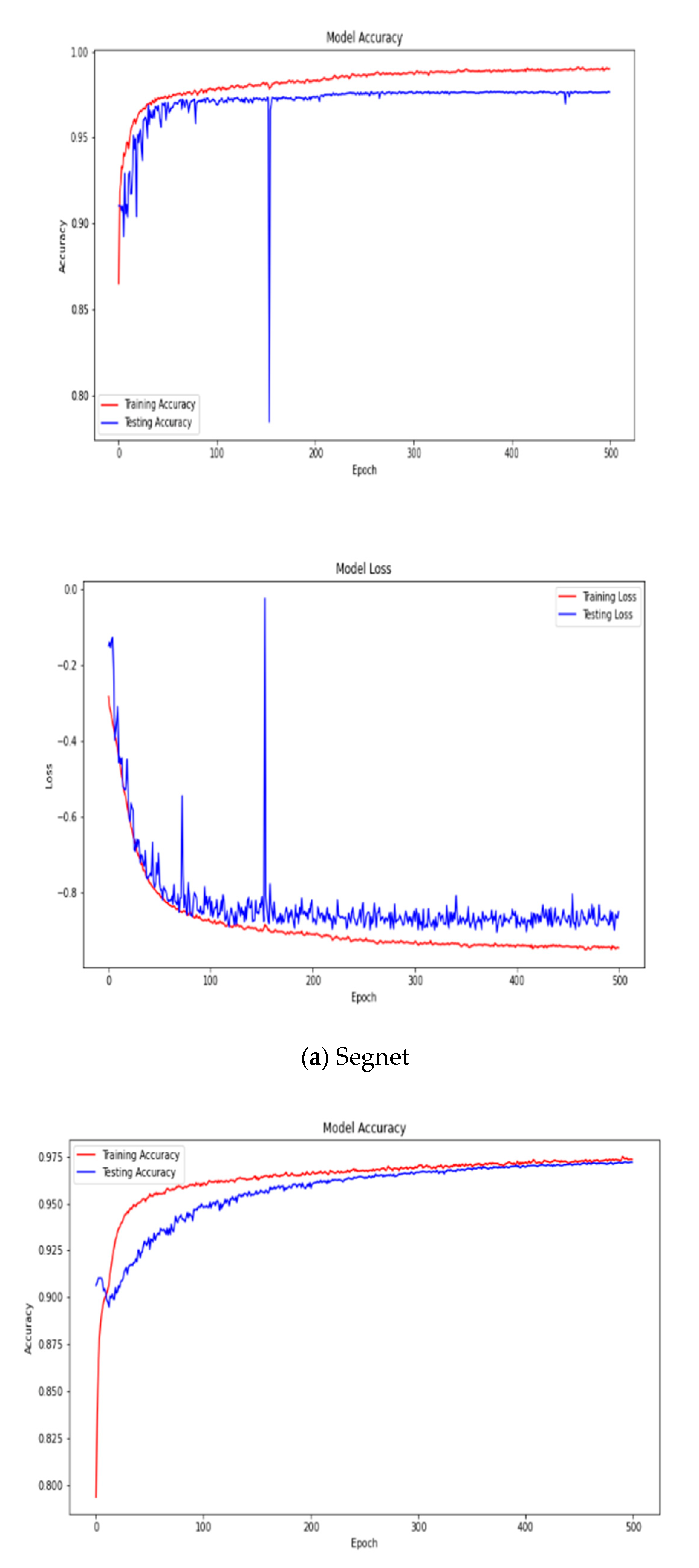
2.3.1. SegNet
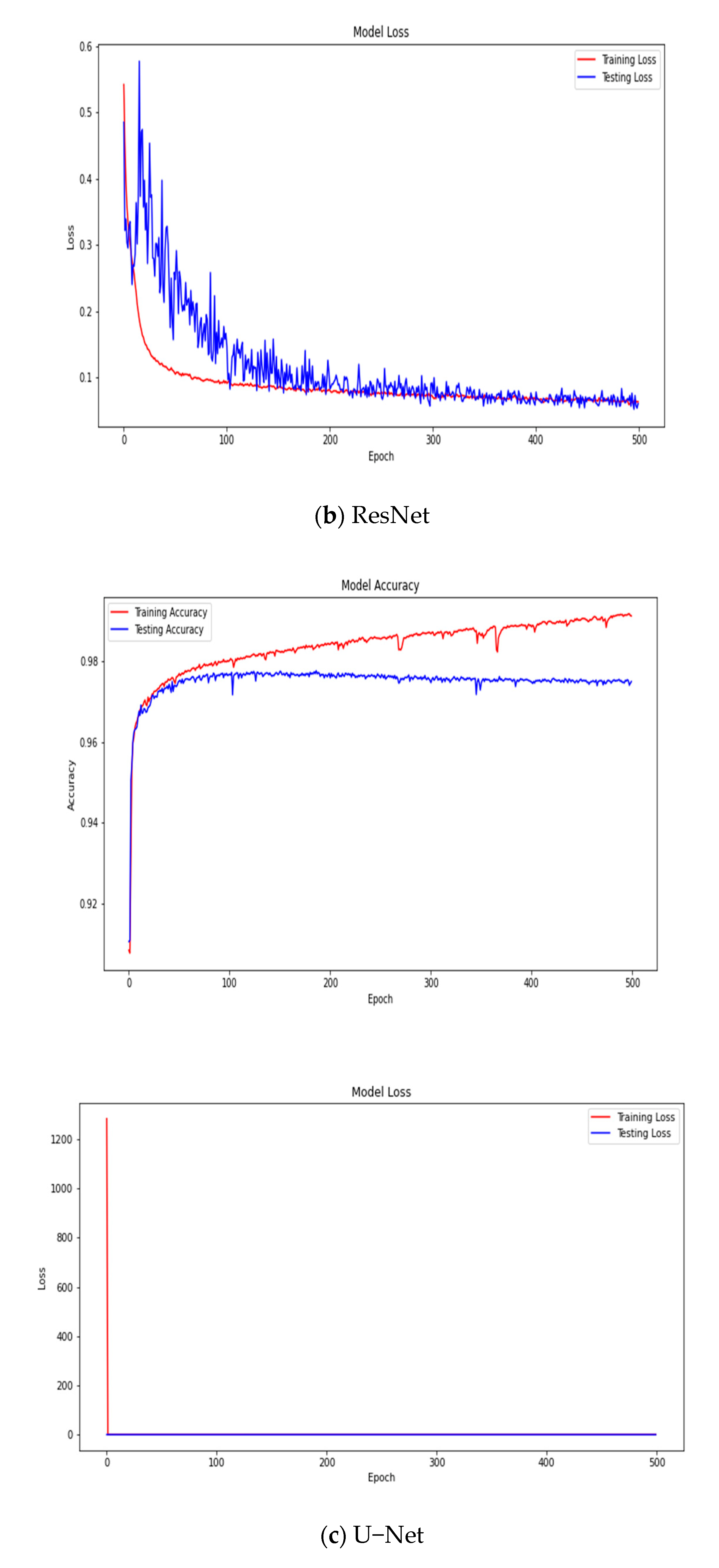
2.3.2. ResNet
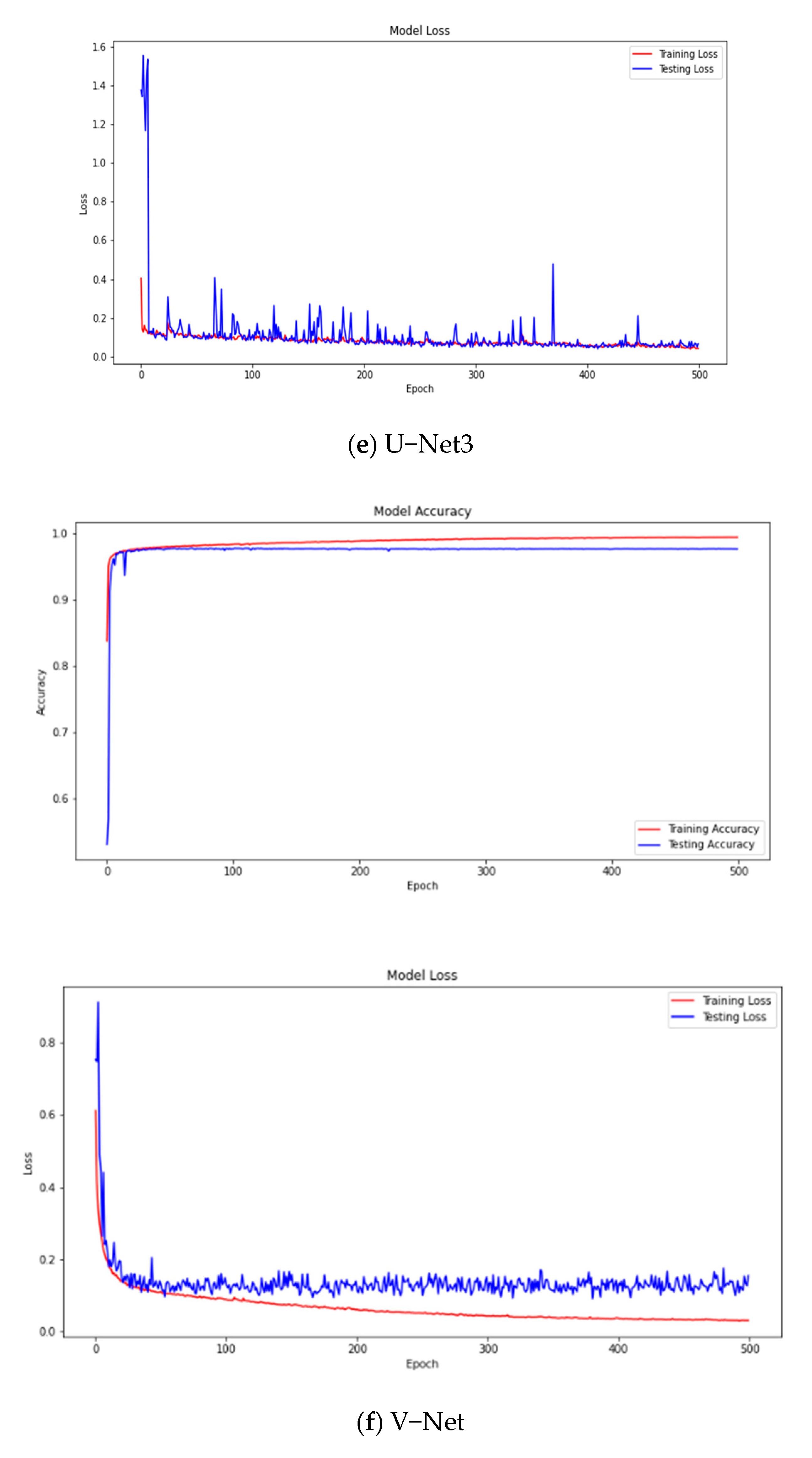
2.3.3. V-Net
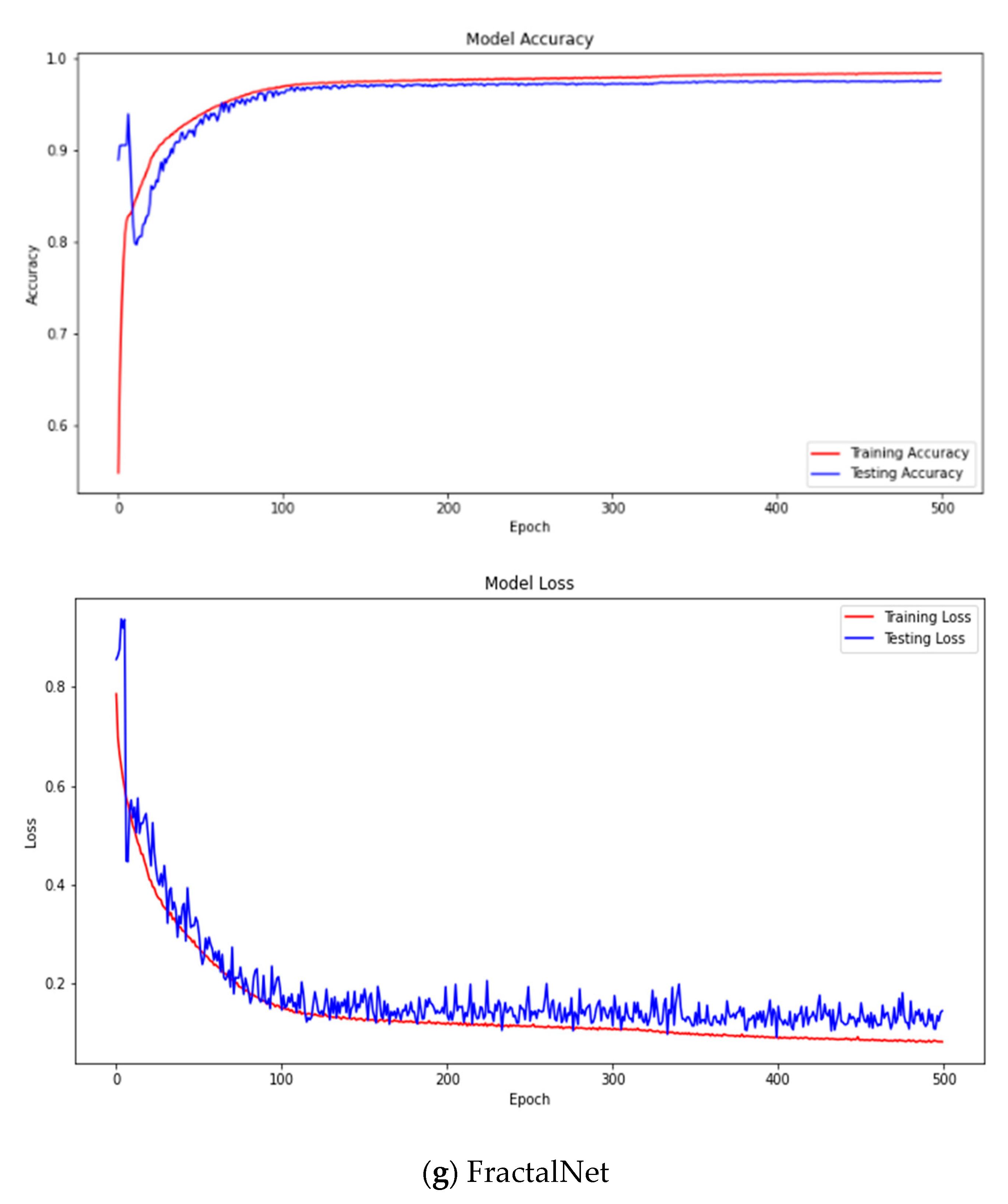
2.3.4. Fractal-Net
2.3.5. U-Net
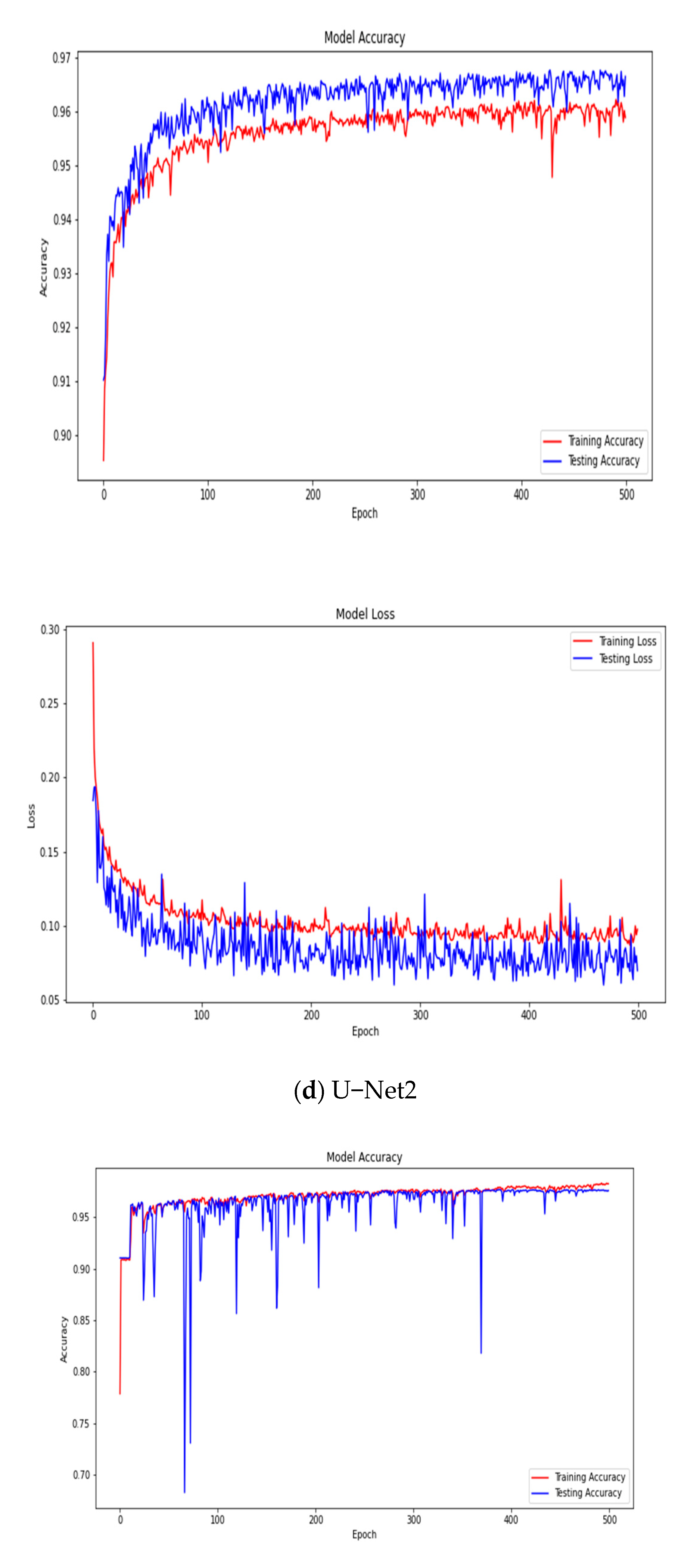
2.3.6. U-Net3
2.4. Performance Metric
3. Results and Discussion
3.1. Results
3.2. Discussion

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| No | Author | Year | Study | Architecture | Dice Coefficient |
|---|---|---|---|---|---|
| 1 | Nova et al. [14] | 2021 | Fetal Heart Echocardiography | U-Net | 94.88% |
| 2 | Rahmatullah et al. [21] | 2021 | Fetal Heart Echocardiography | U-Net and Otsu threshold | 87.95% |
| 3 | Diniz et al. [22] | 2021 | CT Scan heart | U-Net with Concat U-Net | 96.71% |
| 4 | Proposed | 2022 | Mitral Valve Echocardiography | U-Net3 | 86.58% |
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Callow, A.D. Cardiovascular disease 2005—The global picture. Vasc. Pharmacol. 2006, 45, 302–307. [Google Scholar] [CrossRef] [PubMed]
- Mozaffarian, D.; Benjamin, E.J.; Go, A.S.; Arnett, D.K.; Blaha, M.J.; Cushman, M.; Das, S.R.; de Ferranti, S.; Després, J.-P.; Fullerton, H.J.; et al. Heart Disease and Stroke Statistics-2016 Update: A Report From the American Heart Association. Circulation 2016, 133, e38–e360. [Google Scholar] [CrossRef] [PubMed]
- Gumireddy, S.R.; Katayama, M.; Chaliki, H.P. A Case of Severe Mitral Valve Regurgitation in a Patient with Leadless Pacemaker. Case Rep. Cardiol. 2020, 2020, 5389279. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Q.; Liu, Y.; Mi, J.; Wang, X.; Liu, X.; Zhao, F.; Xie, C.; Cui, P.; Zhang, Q.; Zhu, X. Automatic Assessment of Mitral Regurgitation Severity Using the Mask R-CNN Algorithm with Color Doppler Echocardiography Images. Comput. Math. Methods Med. 2021, 2021, 2602688. [Google Scholar] [CrossRef] [PubMed]
- Mayasari, N.M.; Anggrahini, D.W.; Mumpuni, H.; Krisdinarti, L. Incidence of Mitral Valve Prolapse and Mitral Valve Regurgitation in Patient with Secundum Atrial Septal Defect. Acta Cardiol. Indones. 2015, 1, 5–7. [Google Scholar]
- Esteva, A.; Robicquet, A.; Ramsundar, B.; Kuleshov, V.; Depristo, M.; Chou, K.; Cui, C.; Corrado, G.; Thrun, S.; Dean, J. A guide to deep learning in healthcare. Nat. Med. 2019, 25, 24–29. [Google Scholar] [CrossRef] [PubMed]
- Popescu, D.; El-Khatib, M.; El-Khatib, H.; Ichim, L. New Trends in Melanoma Detection Using Neural Networks: A Systematic Review. Sensors 2022, 22, 496. [Google Scholar] [CrossRef] [PubMed]
- Minaee, S.; Boykov, Y.Y.; Porikli, F.; Plaza, A.J.; Kehtarnavaz, N.; Terzopoulos, D. Image Segmentation Using Deep Learning: A Survey. IEEE Trans. Pattern Anal. Mach. Intell. 2021, 44, 3523–3542. [Google Scholar] [CrossRef] [PubMed]
- Skourt, B.A.; El Hassani, A.; Majda, A. Lung CT image segmentation using deep neural networks. Procedia Comput. Sci. 2018, 127, 109–113. [Google Scholar] [CrossRef]
- Ronneberger, O.; Fischer, P.; Brox, T. U-net: Convolutional networks for biomedical image segmentation. In International Conference on Medical image Computing and Computer-Assisted Intervention; Lect. Notes Comput. Sci. (including Subser. Lect. Notes Artif. Intell. Lect. Notes Bioinformatics); Springer: Cham, Switzerland, 2015; Volume 9351, pp. 234–241. [Google Scholar] [CrossRef] [Green Version]
- Siddique, N.; Paheding, S.; Elkin, C.P.; Devabhaktuni, V. U-net and its variants for medical image segmentation: A review of theory and applications. IEEE Access 2021, 9, 82031–82057. [Google Scholar] [CrossRef]
- Zhang, Q.; Cui, Z.; Niu, X.; Geng, S.; Qiao, Y. Image Segmentation with Pyramid Dilated Convolution Based on ResNet and U-Net. In International Conference on Neural Information Processing; Lect. Notes Comput. Sci. (including Subser. Lect. Notes Artif. Intell. Lect. Notes Bioinformatics); Springer: Cham, Switzerland, 2017; Volume 10635, pp. 364–372. [Google Scholar] [CrossRef]
- Liciotti, D.; Paolanti, M.; Pietrini, R.; Frontoni, E.; Zingaretti, P. Convolutional Networks for Semantic Heads Segmentation using Top-View Depth Data in Crowded Environment. In Proceedings of the 2018 24th International Conference on Pattern Recognition (ICPR), Beijing, China, 20–24 August 2018; pp. 1384–1389. [Google Scholar] [CrossRef]
- Nova, R.; Nurmaini, S.; Partan, R.U.; Putra, S.T. Automated image segmentation for cardiac septal defects based on contour region with convolutional neural networks: A preliminary study. Inform. Med. Unlocked 2021, 24, 100601. [Google Scholar] [CrossRef]
- Kalane, P.; Patil, S.; Patil, B.; Sharma, D.P. Automatic detection of COVID-19 disease using U-Net architecture based fully convolutional network. Biomed. Signal Process. Control 2021, 67, 102518. [Google Scholar] [CrossRef] [PubMed]
- Milletari, F.; Navab, N.; Ahmadi, S.-A. V-Net: Fully convolutional neural networks for volumetric medical image segmentation. In Proceedings of the 2016 Fourth International Conference on 3D Vision (3DV), Stanford, CA, USA, 25–28 October 2016; pp. 565–571. [Google Scholar] [CrossRef] [Green Version]
- Badrinarayanan, V.; Kendall, A.; Cipolla, R. Segnet: A deep convolutional encoder-decoder architecture for image segmentation. IEEE Trans. Pattern Anal. Mach. Intell. 2017, 39, 2481–2495. [Google Scholar] [CrossRef] [PubMed]
- Larsson, G.; Maire, M.; Shakhnarovich, G. FractalNet: Ultra-Deep Neural Networks without Residuals. arXiv 2016, arXiv:1605.07648. [Google Scholar]
- Zhuang, J. LadderNet: Multi-path networks based on U-Net for medical image segmentation. arXiv 2018, arXiv:1810.07810. [Google Scholar]
- Benjdira, B.; Ammar, A.; Koubaa, A.; Ouni, K. Data-efficient domain adaptation for semantic segmentation of aerial imagery using generative adversarial networks. Appl. Sci. 2020, 10, 1092. [Google Scholar] [CrossRef] [Green Version]
- Rachmatullah, M.N.; Nurmaini, S.; Sapitri, A.I.; Darmawahyuni, A.; Tutuko, B.; Firdaus, F. Convolutional neural network for semantic segmentation of fetal echocardiography based on four-chamber view. Bull. Electr. Eng. Informatics 2021, 10, 1987–1996. [Google Scholar] [CrossRef]
- Diniz, J.O.B.; Ferreira, J.L.; Cortes, O.A.C.; Silva, A.C.; de Paiva, A.C. An automatic approach for heart segmentation in CT scans through image processing techniques and Concat-U-Net. Expert Syst. Appl. 2022, 196, 116632. [Google Scholar] [CrossRef]









| Video | No. of Videos | Total Duration (second) | Frame Rate (fps) | Filter Frames |
|---|---|---|---|---|
| Normal 1 | 1 Video | 02: 00 | 25 | 28 |
| Normal 2 | 1 Video | 02: 00 | 25 | 28 |
| Normal 3 | 2 Videos | 04: 00 | 25 | 41 |
| Normal 4 | 2 Videos | 04: 00 | 25 | 38 |
| Normal 5 | 1 Video | 02: 00 | 25 | 22 |
| Normal 6 | 1 Video | 02: 00 | 25 | 12 |
| Normal 7 | 1 Video | 02: 00 | 25 | 7 |
| Normal 8 | 1 Video | 02: 00 | 25 | 13 |
| Normal 9 | 1 Video | 02: 00 | 25 | 25 |
| Normal 10 | 1 Video | 02: 00 | 25 | 15 |
| Normal 11 | 1 Video | 02: 00 | 25 | 11 |
| Normal 12 | 2 Videos | 04: 00 | 25 | 41 |
| Normal 13 | 1 Video | 02: 00 | 25 | 13 |
| Normal 14 | 1 Video | 02: 00 | 25 | 11 |
| Normal 15 | 1 Video | 02: 00 | 25 | 17 |
| Normal 16 | 2 Videos | 02: 00 | 25 | 41 |
| Normal 17 | 1 Video | 02: 00 | 25 | 16 |
| Normal 18 | 1 Video | 02: 00 | 25 | 7 |
| Normal 19 | 1 Video | 02: 00 | 25 | 30 |
| Normal 20 | 1 Video | 02: 00 | 25 | 22 |
| Normal 21 | 1 Video | 02: 00 | 25 | 31 |
| Mitral Regurgitation 1 | 1 Video | 02: 00 | 25 | 16 |
| Mitral Regurgitation 2 | 1 Video | 02: 00 | 25 | 6 |
| Mitral Regurgitation 3 | 1 Video | 02: 00 | 25 | 5 |
| Mitral Regurgitation 4 | 1 Video | 02: 00 | 25 | 11 |
| Mitral Regurgitation 5 | 1 Video | 02: 00 | 25 | 22 |
| Mitral Regurgitation 6 | 1 Video | 02: 00 | 25 | 4 |
| Mitral Regurgitation 7 | 1 Video | 02: 00 | 25 | 28 |
| Mitral Regurgitation 8 | 1 Video | 02: 00 | 25 | 18 |
| Mitral Regurgitation 9 | 3 videos | 06: 00 | 25 | 52 |
| Mitral Regurgitation 10 | 1 Video | 02: 00 | 25 | 12 |
| Mitral Regurgitation 11 | 1 Video | 02: 00 | 25 | 23 |
| Mitral Regurgitation 12 | 1 Video | 02: 00 | 25 | 30 |
| Mitral Regurgitation 13 | 1 Video | 02: 00 | 25 | 41 |
| Mitral Regurgitation 14 | 1 Video | 02: 00 | 25 | 31 |
| Mitral Regurgitation 15 | 1 Video | 02: 00 | 25 | 36 |
| Mitral Regurgitation 16 | 1 Video | 02: 00 | 25 | 14 |
| Mitral Regurgitation 17 | 1 Video | 02: 00 | 25 | 7 |
| Mitral Regurgitation 18 | 1 Video | 02: 00 | 25 | 32 |
| Mitral Regurgitation 19 | 1 Video | 02: 00 | 25 | 26 |
| Mitral Regurgitation 20 | 1 Video | 02: 00 | 25 | 21 |
| Mitral Regurgitation 21 | 1 Video | 02: 00 | 25 | 19 |
| Total Frames | 923 |
| No | No. of Patients | Total Frames | Training | Testing | Unseen |
|---|---|---|---|---|---|
| Normal | 21 | 469 | 334 | 79 | 56 |
| Mitral Regurgitation | 21 | 454 | 287 | 77 | 90 |
| Total | 42 | 923 | 621 | 156 | 146 |
| Architecture | Batch Size | Learning Rate | Epoch |
|---|---|---|---|
| SegNet | 64 | 0.00001 | 500 |
| ResNet | 64 | 0.00001 | 500 |
| U-Net | 64 | 0.00001 | 500 |
| U-Net 2 | 64 | 0.00001 | 500 |
| U-Net 3 | 64 | 0.00001 | 500 |
| V-Net | 64 | 0.00001 | 500 |
| Fractal-Net | 64 | 0.00001 | 500 |
| Layer | Kernel Size | Stride | Activation Function | Output |
|---|---|---|---|---|
| Input Layer | - | - | - | 256 256 1 |
| Convolution Layer 1 | 64 64 1 | 1 | ReLU | 128 128 3 |
| Batch Normalization | ||||
| Convolution Layer 2 | 64 64 1 | 1 | ReLU | 128 128 3 |
| Max Pooling 1 | 2 2 | 2 | 128 128 3 | |
| Batch Normalization | ||||
| Convolution Layer 3 | 128 128 3 | 1 | ReLU | 256 256 3 |
| Batch Normalization | ||||
| Convolution Layer 4 | 128 128 3 | 1 | ReLU | 256 256 3 |
| Max Pooling 2 | 2 2 | 2 | 256 256 3 | |
| Batch Normalization | ||||
| Convolution Layer 5 Batch Normalization | 256 256 3 | 1 | ReLU | 512 512 3 |
| Convolution Layer 6 | 256 256 3 | 1 | ReLU | 512 512 3 |
| Max Pooling 3 | 2 2 | 2 | - | 512 512 3 |
| Batch Normalization | ||||
| Convolution Layer 7 | 512 512 3 | 1 | ReLU | 1024 1024 3 |
| Batch Normalization | ||||
| Convolution Layer 8 | 512 512 3 | 1 | ReLU | 1024 1024 3 |
| Max Pooling 4 Batch Normalization | 2 2 | 2 | - | 1024 1024 3 |
| Convolution Layer 9 | 1024 1024 3 | 1 | ReLU | 512 512 3 |
| Batch Normalization | ||||
| Convolution Layer 10 | 1024 1024 3 | 1 | ReLU | 512 512 3 |
| Up 1 | 512 512 3 | 3 (axis) | ReLU | 512 512 3 |
| Batch Normalization | ||||
| Convolution Layer 11 | 512 512 3 | 1 | ReLU | 256 256 3 |
| Batch Normalization | ||||
| Covolutional Layer 12 | 512 512 3 | 1 | ReLU | 256 256 3 |
| Up 2 | 256 256 3 | 3 (axis) | ReLU | 256 256 3 |
| Batch Normalization | ||||
| Covolutional Layer 13 | 256 256 3 | 1 | ReLU | 128 128 3 |
| Batch Normalization | ||||
| Covolutional Layer 14 | 256 256 3 | 1 | ReLU | 128 128 3 |
| Up 3 | 128 128 3 | 3 (axis) | ReLU | 128 128 3 |
| Batch Normalization | ||||
| Convolutional Layer 15 | 128 128 3 | 1 | ReLU | 64 64 3 |
| Batch Normalization | ||||
| Covolutional Layer 16 | 128 128 3 | 1 | ReLU | 64 64 3 |
| Up 4 | 64 64 3 | 1 | ReLU | 64 64 3 |
| Batch Normalization | ||||
| Covolutional Layer 17 | 64 64 3 | 1 | ReLU | |
| Convolution Layer 18 | 64 64 3 | 1 | Hard_ Sigmoid | 2 2 3 |
| Batch Normalization | ||||
| Output Layer | - | - | Hard_ Sigmoid | 1 |
| Evaluation Metrics | Performance (%) | ||||||
|---|---|---|---|---|---|---|---|
| Segnet | ResNet | U-Net | U-Net2 | U-Net3 | FractalNet | VNet | |
| Pixel Accuracy | 97.62 | 97.40 | 97.58 | 96.09 | 97.59 | 97.63 | 97.67 |
| IoU | 87.20 | 86.04 | 86.78 | 78.50 | 86.98 | 87.03 | 87.23 |
| Mean Accuracy | 93.73 | 92.73 | 92.59 | 83.73 | 93.46 | 92.91 | 93.05 |
| Precision | 85.49 | 84.69 | 86.92 | 85.76 | 85.60 | 85.49 | 87.01 |
| Recall | 88.95 | 86.99 | 86.46 | 68.57 | 88.39 | 88.95 | 87.38 |
| Dice Coefficient | 86.85 | 85.48 | 86.34 | 75.36 | 86.58 | 86.85 | 86.87 |
| Evaluation Metrics | Performance (%) | ||||||
|---|---|---|---|---|---|---|---|
| Segnet | ResNet | U-Net | U-Net2 | U-Net3 | FractalNet | VNet | |
| Pixel Accuracy | 97.05 | 96.39 | 96.79 | 95.69 | 97.24 | 96.61 | 94.53 |
| IoU | 85.26 | 82.58 | 84.45 | 78.33 | 86.44 | 82.97 | 74.18 |
| Mean Accuracy | 88.69 | 88.91 | 90.87 | 83.12 | 86.92 | 87.90 | 81.61 |
| Precision | 87.24 | 84.16 | 84.82 | 87.37 | 80.44 | 88.64 | 74.40 |
| Recall | 82.62 | 79.46 | 83.38 | 67.29 | 86.16 | 76.89 | 65.52 |
| Dice Coefficient | 84.89 | 81.29 | 83.72 | 75.44 | 86.14 | 81.91 | 67.73 |
| Architecture | Training Time (s) |
|---|---|
| Segnet | 270.81 |
| ResNet | 196.77 |
| U-Net | 231.02 |
| U-Net 2 | 224.53 |
| U-Net 3 | 194.32 |
| V-Net | 357.84 |
| Fractal-Net | 295.26 |
| Ground Truth | Arsitektur | Predict Ground Truth |
|---|---|---|
 | Segnet |  |
| ResNet |  | |
| U-Net |  | |
| U-Net 2 |  | |
| U-Net 3 |  | |
| V-Net | ||
| Fractal-Net |   |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Atika, L.; Nurmaini, S.; Partan, R.U.; Sukandi, E. Image Segmentation for Mitral Regurgitation with Convolutional Neural Network Based on UNet, Resnet, Vnet, FractalNet and SegNet: A Preliminary Study. Big Data Cogn. Comput. 2022, 6, 141. https://doi.org/10.3390/bdcc6040141
Atika L, Nurmaini S, Partan RU, Sukandi E. Image Segmentation for Mitral Regurgitation with Convolutional Neural Network Based on UNet, Resnet, Vnet, FractalNet and SegNet: A Preliminary Study. Big Data and Cognitive Computing. 2022; 6(4):141. https://doi.org/10.3390/bdcc6040141
Chicago/Turabian StyleAtika, Linda, Siti Nurmaini, Radiyati Umi Partan, and Erwin Sukandi. 2022. "Image Segmentation for Mitral Regurgitation with Convolutional Neural Network Based on UNet, Resnet, Vnet, FractalNet and SegNet: A Preliminary Study" Big Data and Cognitive Computing 6, no. 4: 141. https://doi.org/10.3390/bdcc6040141