
The Prevalence of Human Plasmodium Species during Peak Transmission Seasons from 2016 to 2021 in the Rural Commune of Ntjiba, Mali

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Methodology
2.1. Study Site and Population
2.2. Data Sources
2.3. Study Data and Statistical Methods
2.4. Ethical Considerations
3. Results
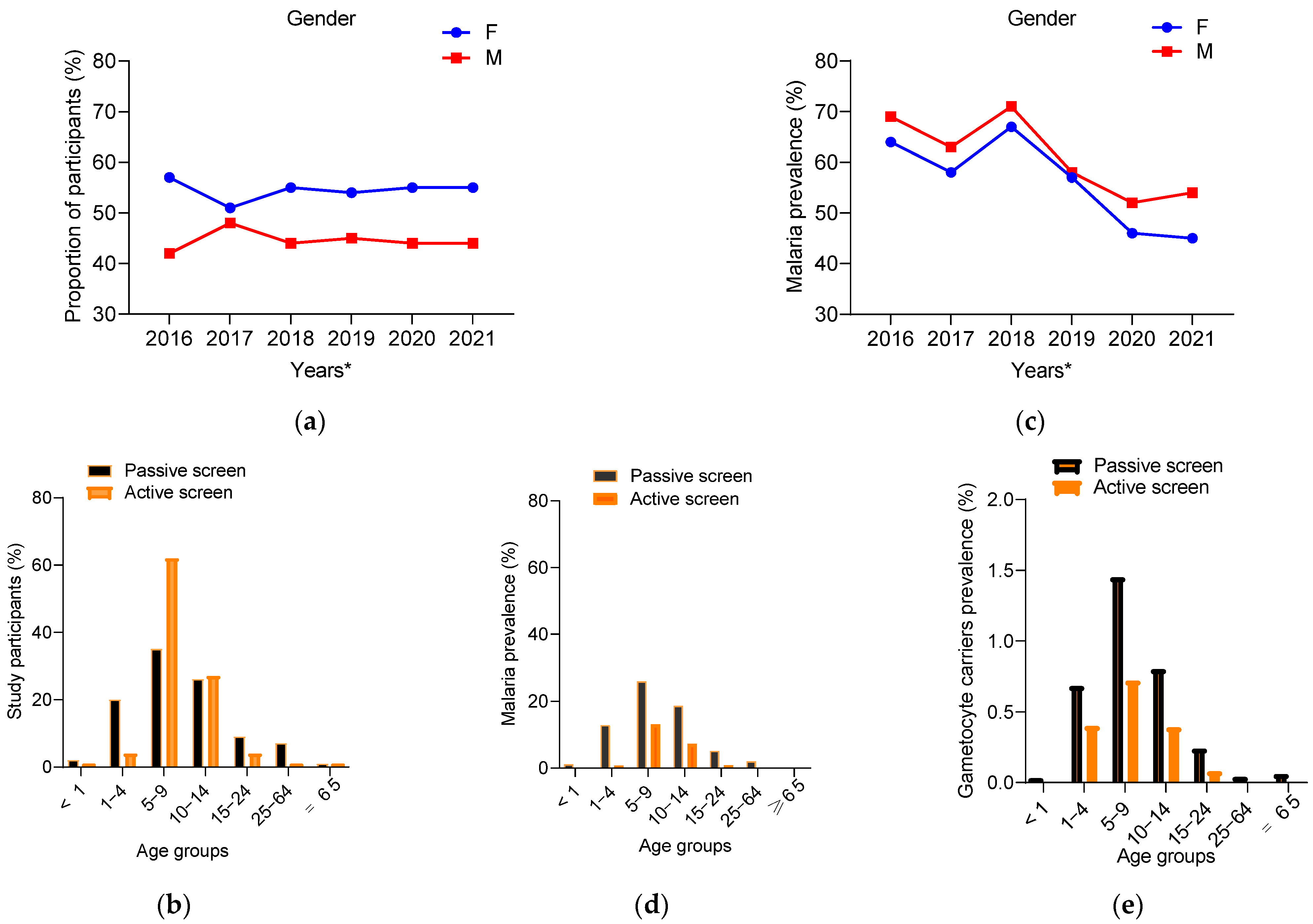
3.1. General Characteristics Observed over the Years in the Studies Participants
3.2. Distribution of Malaria Prevalence by Gender and Age Groups
3.3. Plasmodium Sexual Stage Prevalence
3.4. Plasmodium Species Prevalence and Frequency
3.5. Non-Falciparum Malaria Species Are Associated with the Burden of Malaria Anemia
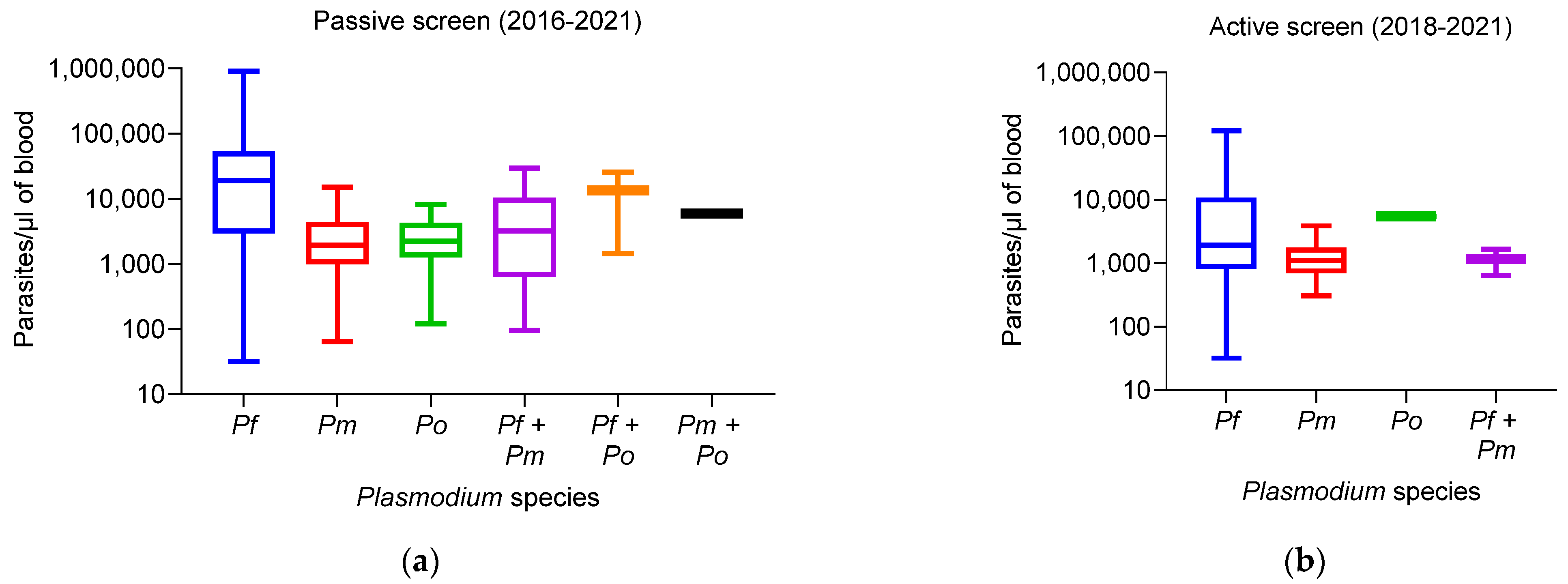
3.6. Plasmodium Species-Specific Characteristics
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Malaria Report 2022. Available online: https://www.who.int/teams/global-malaria-programme/reports/world-malaria-report-2022 (accessed on 16 July 2023).
- Paludisme: Situation Mondiale 2020 (Organisation Mondiale de la Santé). Available online: https://www.mesvaccins.net/web/news/16794-paludisme-situation-mondiale-2020-organisation-mondiale-de-la-sante (accessed on 16 July 2023).
- World Health Organization. World Malaria Report: 20 Years of Global Progress and Challenges. WHO/HTM/GM (December): 299. Available online: https://www.who.int/publications/i/item/9789240015791 (accessed on 16 July 2023).
- Rapport 2022 sur le Paludisme Dans le Monde. Available online: https://www.who.int/fr/teams/global-malaria-programme/reports/world-malaria-report-2022 (accessed on 16 July 2023).
- Yman, V.; Wandell, G.; Mutemi, D.D.; Miglar, A.; Asghar, M.; Hammar, U.; Karlsson, M.; Lind, I.; Nordfjell, C.; Rooth, I.; et al. Persistent transmission of Plasmodium malariae and Plasmodium ovale species in an area of declining Plasmodium falciparum transmission in eastern Tanzania. PLoS Negl. Trop. Dis. 2019, 13, e0007414. [Google Scholar] [CrossRef] [PubMed]
- Malaria. Available online: https://www.who.int/news-room/fact-sheets/detail/malaria (accessed on 31 July 2023).
- Camargo-Ayala, P.A.; Cubides, J.R.; Niño, C.H.; Camargo, M.; Rodríguez-Celis, C.A.; Quiñones, T.; Sánchez-Suárez, L.; Patarroyo, M.E.; Patarroyo, M.A. High Plasmodium malariae Prevalence in an Endemic Area of the Colombian Amazon Region. PLoS ONE 2016, 11, e0159968. [Google Scholar] [CrossRef] [PubMed]
- Noland, G.S.; Graves, P.M.; Sallau, A.; Eigege, A.; Emukah, E.; Patterson, A.E.; Ajiji, J.; Okorofor, I.; Oji, O.U.; Umar, M.; et al. Malaria prevalence, anemia and baseline intervention coverage prior to mass net distributions in Abia and Plateau States, Nigeria. BMC Infect. Dis. 2014, 14, 168. [Google Scholar] [CrossRef] [PubMed]
- Molineaux, L.; Gramiccia, G. The Garki Project Research on the Epidemiology and Control of Malaria in the Sudan Savanna of West Africa; World Health Organization: Geneva, Switzerland, 1980. [Google Scholar]
- Raja, T.N.; Hu, T.H.; Kadir, K.A.; Mohamad, D.S.A.; Rosli, N.; Wong, L.L.; Hii, K.C.; Divis, P.C.S.; Singh, B. Naturally Acquired Human Plasmodium cynomolgi and P. knowlesi Infections, Malaysian Borneo. Emerg. Infect. Dis. 2020, 26, 1801. [Google Scholar] [CrossRef] [PubMed]
- Galinski, M.R.; Barnwell, J.W. Nonhuman Primate Models for Human Malaria Research. Nonhum. Primates Biomed. Res. Dis. Second Ed. 2012, 2, 299–323. [Google Scholar] [CrossRef]
- World Malaria Report 2019. Available online: https://www.who.int/publications/i/item/9789241565721 (accessed on 16 July 2023).
- Enquête Démographique et de Santé 2018 Rapport de Synthèse Mali. Available online: www.DHSprogram.com (accessed on 28 October 2021).
- Dembele, L.; Diallo, N.; Sogore, F.; Diarra, B.; Ballo, F.I.; Daou, A.; Diakite, O.; Bare, Y.; Sangare, C.P.O.; Haidara, A.S.; et al. Ex Vivo Plasmodium malariae Culture Method for Antimalarial Drugs Screen in the Field. ACS Infect. Dis. 2021, 7, 3025–3033. [Google Scholar] [CrossRef] [PubMed]
- Niangaly, A.; Gunalan, K.; Ouattara, A.; Coulibaly, D.; Sá, J.M.; Adams, M.; Travassos, M.A.; Ferrero, J.; Laurens, M.B.; Kone, A.K.; et al. Plasmodium vivax Infections over 3 Years in Duffy Blood Group Negative Malians in Bandiagara, Mali. Am. J. Trop. Med. Hyg. 2017, 97, 744. [Google Scholar] [CrossRef] [PubMed]
- PNLP. Plan Strategique de Lutte Contre le Paludisme 2013–2017. Available online: https://www.severemalaria.org/sites/mmv-smo/files/content/attachments/2017-07-25/Mali malariaPlanStrategique2013-17PNLP_0.pdf (accessed on 16 July 2023).
- Bernabeu, M.; Gomez-Perez, G.P.; Sissoko, S.; Niambélé, M.B.; Haibala, A.A.; Sanz, A.; Théra, M.A.; Fernandez-Becerra, C.; Traoré, K.; Alonso, P.L.; et al. Plasmodium vivax malaria in Mali: A study from three different regions. Malar. J. 2012, 11, 405. [Google Scholar] [CrossRef] [PubMed]
- Greenwood, B.M.; Armstrong, J.R.M. Comparison of two simple methods for determining malaria parasite density. Trans. R. Soc. Trop. Med. Hyg. 1991, 85, 186–188. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Anaemia. Available online: https://www.who.int/data/nutrition/nlis/info/anaemia (accessed on 16 July 2023).
- Coulibaly, D.; Travassos, M.A.; Kone, A.K.; Tolo, Y.; Laurens, M.B.; Traore, K.; Diarra, I.; Niangaly, A.; Daou, M.; Dembele, A.; et al. Stable malaria incidence despite scaling up control strategies in a malaria vaccine-testing site in Mali. Malar. J. 2014, 13, 374. [Google Scholar] [CrossRef] [PubMed]
- Diouf, I.; Fonseca, B.R.; Caminade, C.; Thiaw, W.M.; Deme, A.; Morse, A.P.; Ndione, J.A.; Gaye, A.T.; Diaw, A.; Ndiaye, M.K.N. Climate Variability and Malaria over West Africa. Am. J. Trop. Med. Hyg. 2020, 102, 1037. [Google Scholar] [CrossRef]
- Gbalégba, C.G.N.; Ba, H.; Silué, K.D.; Ba, O.; Tia, E.; Chouaibou, M.; Tian-Bi, N.T.Y.; Yapi, G.Y.; Koné, B.; Utzinger, J.; et al. Distribution of Plasmodium spp. infection in asymptomatic carriers in perennial and low seasonal malaria transmission settings in West Africa. Infect. Dis. Poverty 2018, 7, 39. [Google Scholar] [CrossRef]
- Shaffer, J.G.; Touré, M.B.; Sogoba, N.; Doumbia, S.O.; Gomis, J.F.; Ndiaye, M.; Ndiaye, D.; Diarra, A.; Abubakar, I.; Ahmad, A.; et al. Clustering of asymptomatic Plasmodium falciparum infection and the effectiveness of targeted malaria control measures. Malar. J. 2020, 19, 33. [Google Scholar] [CrossRef]
- Adomako-Ankomah, Y.; Chenoweth, M.S.; Durfee, K.; Doumbia, S.; Konate, D.; Doumbouya, M.; Keita, A.S.; Nikolaeva, D.; Tullo, G.S.; Anderson, J.M.; et al. High Plasmodium falciparum longitudinal prevalence is associated with high multiclonality and reduced clinical malaria risk in a seasonal transmission area of Mali. PLoS ONE 2017, 12, e0170948. [Google Scholar] [CrossRef]
- The Importance of Gender in Malaria Data—MEASURE Evaluation. Available online: https://www.measureevaluation.org/resources/publications/fs-17-205d.html (accessed on 16 July 2023).
- WHO. Gender, Health and Malaria. May 2007. Available online: https://www.who.int/gender/documents/gender_health_malaria.pdf (accessed on 16 July 2023).
- Baba, E.; Hamade, P.; Kivumbi, H.; Marasciulo, M.; Maxwell, K.; Moroso, D.; Roca-Feltrer, A.; Sanogo, A.; Stenstrom Johansson, J.; Tibenderana, J.; et al. Effectiveness of seasonal malaria chemoprevention at scale in west and central Africa: An observational study. Lancet 2020, 396, 1829. [Google Scholar] [CrossRef]
- Cairns, M.; Ceesay, S.J.; Sagara, I.; Zongo, I.; Kessely, H.; Gamougam, K.; Diallo, A.; Ogboi, J.S.; Moroso, D.; van Hulle, S.; et al. Effectiveness of seasonal malaria chemoprevention (SMC) treatments when SMC is implemented at scale: Case–control studies in 5 countries. PLoS Med. 2021, 18, e1003727. [Google Scholar] [CrossRef]
- Konaté, D.; Diawara, S.I.; Touré, M.; Diakité, S.A.S.; Guindo, A.; Traoré, K.; Diarra, A.; Keita, B.; Thiam, S.; Keita, M.; et al. Effect of routine seasonal malaria chemoprevention on malaria trends in children under 5 years in Dangassa, Mali. Malar. J. 2020, 19, 137. [Google Scholar] [CrossRef]
- Diawara, F.; Steinhardt, L.C.; Mahamar, A.; Traore, T.; Kone, D.T.; Diawara, H.; Kamate, B.; Kone, D.; Diallo, M.; Sadou, A.; et al. Measuring the impact of seasonal malaria chemoprevention as part of routine malaria control in Kita, Mali. Malar. J. 2017, 16, 325. [Google Scholar] [CrossRef]
- Reynaldi, A.; Dent, A.E.; Schlub, T.E.; Ogolla, S.; Rochford, R.; Davenport, M.P. Interaction between maternally derived antibodies and heterogeneity in exposure combined to determine time-to-first Plasmodium falciparum infection in Kenyan infants. Malar. J. 2019, 18, 19. [Google Scholar] [CrossRef]
- Kone, M. Prévalence de L’infection Palustre et de L’anémie en Fin de Saison de Transmission Chez les Scolaires de 6 à 12 ans dans le District Sanitaire de Bougouni en 2015 et 2016 dans un Contexte de Mise en Œuvre de la Chimio-Prévention du Paludisme Saisonnier as; Université des sciences, des Techniques et des Technologies de Bamako (USTTB): Bamako, Republic of Mali, 2018. [Google Scholar]
- Dembele, L.; Aniweh, Y.; Diallo, N.; Sogore, F.; Sangare, C.P.O.; Haidara, A.S.; Traore, A.; Diakité, S.A.S.; Diakite, M.; Campo, B.; et al. Plasmodium malariae and Plasmodium falciparum comparative susceptibility to antimalarial drugs in Mali. J. Antimicrob. Chemother. 2021, 76, 2079–2087. [Google Scholar] [CrossRef]
- Feufack-Donfack, L.B.; Sarah-Matio, E.M.; Abate, L.M.; Bouopda Tuedom, A.G.; Ngano Bayibéki, A.; Maffo Ngou, C.; Toto, J.C.; Sandeu, M.M.; Eboumbou Moukoko, C.E.; Ayong, L.; et al. Epidemiological and entomological studies of malaria transmission in Tibati, Adamawa region of Cameroon 6 years following the introduction of long-lasting insecticide nets. Parasites and Vectors 2021, 14, 247. [Google Scholar] [CrossRef]
- CDC, USAID, President's Malaria Initiative (PMI): Mali Malaria Profile. Available online: https://reliefweb.int/report/mali/presidents-malaria-initiative-mali-country-profile (accessed on 3 August 2015).
- Mendes, C.; Dias, F.; Figueiredo, J.; Mora, V.G.; Cano, J.; de Sousa, B.; do Rosário, V.E.; Benito, A.; Berzosa, P.; Arez, A.P. Duffy Negative Antigen Is No Longer a Barrier to Plasmodium vivax—Molecular Evidences from the African West Coast (Angola and Equatorial Guinea). PLoS Negl Trop Dis. 2011, 5, e1192. [Google Scholar] [CrossRef] [PubMed]
- Wilairatana, P.; Tangpukdee, N.; Krudsood, S. Definition of hyperparasitemia in severe falciparum malaria should be updated. Asian Pac. J. Trop. Biomed. 2013, 3, 586. [Google Scholar] [CrossRef]
- Ayo, D.; Odongo, B.; Omara, J.; Andolina, C.; Mulder, O.; Staedke, S.G.; Bousema, T. Plasmodium malariae infections as a cause of febrile disease in an area of high Plasmodium falciparum transmission intensity in Eastern Uganda. Malar. J. 2021, 20, 586. [Google Scholar] [CrossRef]
- Trampuz, A.; Jereb, M.; Muzlovic, I.; Prabhu, R.M. Clinical review: Severe malaria. Crit. Care 2003, 7, 315. [Google Scholar] [CrossRef]
- Mukomena, S.E.; Philipe, C.M.; Désiré, M.K.; Pascal, L.T.; Ali, M.M.; Oscar, L.N. Asymptomatic Parasitemia in under five, school age children and households self-medication, Lubumbashi, Democratic Republic of Congo. Pan Afr. Med. J. 2016, 24, 94. [Google Scholar]
- Langhorne, J.; Ndungu, F.M.; Sponaas, A.M.; Marsh, K. Immunity to malaria: More questions than answers. Nat. Immunol. 2008, 9, 725–732. [Google Scholar] [CrossRef] [PubMed]
- Beeson, J.G.; Osier, F.H.A.; Engwerda, C.R. Recent insights into humoral and cellular immune responses against malaria. Trends Parasitol. 2008, 24, 578–584. [Google Scholar] [CrossRef] [PubMed]
- Crompton, P.D.; Moebius, J.; Portugal, S.; Waisberg, M.; Hart, G.; Garver, L.S.; Miller, L.H.; Barillas, C.; Pierce, S.K. Malaria immunity in man and mosquito: Insights into unsolved mysteries of a deadly infectious disease. Annu. Rev. Immunol. 2014, 32, 157–187. [Google Scholar] [CrossRef] [PubMed]
- Langford, S.; Douglas, N.M.; Lampah, D.A.; Simpson, J.A.; Kenangalem, E.; Sugiarto, P.; Anstey, N.M.; Poespoprodjo, J.R.; Price, R.N. Plasmodium malariae infection associated with a high burden of anemia: A hospital-based surveillance study. PLoS Negl. Trop. Dis. 2015, 9, e0004195. [Google Scholar] [CrossRef]
- Dao, F.; Djonor, S.K.; Ayin, C.T.M.; Adu, G.A.; Sarfo, B.; Nortey, P.; Akuffo, K.O.; Danso-Appiah, A. Burden of malaria in children under five and caregivers’ health-seeking behaviour for malaria-related symptoms in artisanal mining communities in Ghana. Parasit. Vectors 2021, 14, 418. [Google Scholar] [CrossRef] [PubMed]
- Knoblauch, A.M.; Winkler, M.S.; Archer, C.; Divall, M.J.; Owuor, M.; Yapo, R.M.; Yao, P.A.; Utzinger, J. The epidemiology of malaria and anaemia in the Bonikro mining area, central Côte d’Ivoire. Malar. J. 2014, 13, 194. [Google Scholar] [CrossRef] [PubMed]
- Assadou, M.H.; Sagara, I.; Healy, S.A.; Guindo, M.A.; Kone, M.; Sanogo, S.; Doucoure, M.; Keita, S.; Ellis, R.D.; Wu, Y.; et al. Malaria Infection and Gametocyte Carriage Rates in Preparation for Transmission Blocking Vaccine Trials in Bancoumana, Mali. Am. J. Trop. Med. Hyg. 2017, 97, 183. [Google Scholar] [CrossRef] [PubMed]
- Mobegi, V.A.; Herren, J.K.; Touray, A.O.; Wamunyokoli, F.; Butungi, H. Prevalence of asymptomatic P. falciparum gametocytecarriage among school children in Mbita, Western Kenya and assessment of the association between gametocyte density, multiplicity of infection and mosquito infection prevalence. Wellcome Open Res. 2020, 5, 259. [Google Scholar] [CrossRef]
- Les Aspects Parasitologiques de L’épidémiologie du Paludisme dans le Sahara Malien|GHDx. Available online: https://ghdx.healthdata.org/record/les-aspects-parasitologiques-de-lépidémiologie-du-paludisme-dans-le-sahara-malien (accessed on 16 July 2023).



{kind=link}
{kind=link}
| Plasmodial Species | |||||||
| Parameters | Pf | Pm | Po | Pf + Pm | Pf + Po | Pm + Po | |
| Screen | |||||||
| Passive | n1 | 4069 | 103 | 22 | 9 | 2 | 0 |
| (N1 = 6858) | Prev | 59.33 | 1.50 | 0.32 | 0.13 | 0.03 | 0.00 |
| Freq | 96.77 | 2.45 | 0.52 | 0.21 | 0.05 | 0.00 | |
| Active | n2 | 336 | 20 | 1 | 2 | 0 | 1 |
| (N2 = 1740) | Prev | 19.31 | 1.15 | 0.06 | 0.11 | 0.00 | 0.06 |
| Freq | 93.24 | 5.64 | 0.28 | 0.56 | 0.00 | 0.28 | |
| Age | Groups | ||||||
| <1 | 62 (1.40) | 0 | 0 | 0 | 0 | 0 | |
| 1–4 | 774 (17.72) | 7 (5.69) | 1 (4.35) | 1 (9.09) | 0 | 0 | |
| 5–9 | 1831 (41.91) | 34 (27.64) | 5 (21.74) | 2 (18.18) | 1 (50) | 0 | |
| 10–14 | 1254 (28.70) | 65 (52.85) | 13 (56.52) | 7 (63.64) | 1 (50) | 1 (100) | |
| 15–24 | 320 (7.30) | 13 (10.57) | 3 (13.04) | 1 (9.09) | 0 | 0 | |
| 25–64 | 122 (2.79) | 3 (2.44) | 1 (4.35) | 0 | 0 | 0 | |
| >65 | 8 (0.18) | 1 (0.81) | 0 | 0 | 0 | 0 | |
| Years | Months | ||||||
| 2016 | Oct. | 35 (97.22) | 1 (2.78) | 0 | 0 | 0 | 0 |
| Nov. | 379 (95.23) | 17 (4.27) | 1 (0.25) | 1 (0.25) | 0 | 0 | |
| Dec. | 104 (90.43) | 9 (7.83) | 2 (1.74) | 0 | 0 | 0 | |
| 2017 | Oct. | 107 (92.24) | 5 (4.31) | 1 (0.86) | 2 (1.72) | 1 (0.86) | 0 |
| Nov. | 35 (97.22) | 1 (2.78) | 0 | 0 | 0 | 0 | |
| Dec. | 15 (88.24) | 2 (11.76) | 0 | 0 | 0 | 0 | |
| 2018 | Oct. | 409 (97.61) | 6 (1.43) | 3 (0.72) | 1 (0.24) | 0 | 0 |
| Nov. | 322 (97.87) | 4 (1.22) | 3 (0.91) | 0 | 0 | 0 | |
| Dec. | 133 (95.68) | 6 (4.32) | 0 | 0 | 0 | 0 | |
| 2019 | Oct. | 362 (99.18) | 2 (0.55) | 0 | 1 (0.27) | 0 | 0 |
| Nov. | 571 (97.61) | 8 (1.37) | 6 | 0 | 0 | 0 | |
| Dec. | 184 (93.88) | 8 (4.08) | 4 (2.04) | 0 | 0 | 0 | |
| 2020 | Oct. | 689 (96.50) | 20 (2.80) | 2 (0.28) | 3 (0.42) | 0 | 0 |
| Nov. | 397 (96.13) | 13 (3.15) | 0 | 1 (0.24) | 1 (0.24) | 1 (0.24) | |
| Dec. | 110 (91.67) | 10 (8.33) | 0 | 0 | 0 | 0 | |
| 2021 | Nov. | 335 (98.24) | 5 (1.47) | 0 | 1 (0.29) | 0 | 0 |
| Dec. | 219 (96.48) | 6 (2.64) | 1 (0.44) | 1 (0.44) | 0 | 0 | |
| Total | 4406 (96.50) | 123 (2.69) | 23 (0.50) | 11 (0.24) | 2 (0.04) | 1 (0.02) | |
| Anaemic | Status | ||||||
| anemia | 6 (18.76) | 44 (41.51) | 5 (50.00) | 1 (20.00) | 0 | 0 | |
| Normal | 26 (81.24) | 62 (58.49) | 5 (50.00) | 4 (80.00) | 0 | 0 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dao, F.; Dembele, L.; Diarra, B.; Sogore, F.; Marin-Menendez, A.; Goita, S.; Haidara, A.S.; Barre, Y.N.; Sangare, C.P.O.; Kone, A.; et al. The Prevalence of Human Plasmodium Species during Peak Transmission Seasons from 2016 to 2021 in the Rural Commune of Ntjiba, Mali. Trop. Med. Infect. Dis. 2023, 8, 438. https://doi.org/10.3390/tropicalmed8090438
Dao F, Dembele L, Diarra B, Sogore F, Marin-Menendez A, Goita S, Haidara AS, Barre YN, Sangare CPO, Kone A, et al. The Prevalence of Human Plasmodium Species during Peak Transmission Seasons from 2016 to 2021 in the Rural Commune of Ntjiba, Mali. Tropical Medicine and Infectious Disease. 2023; 8(9):438. https://doi.org/10.3390/tropicalmed8090438
Chicago/Turabian StyleDao, Francois, Laurent Dembele, Bakoroba Diarra, Fanta Sogore, Alejandro Marin-Menendez, Siaka Goita, Aboubacrin S. Haidara, Yacouba N. Barre, Cheick P. O. Sangare, Aminatou Kone, and et al. 2023. "The Prevalence of Human Plasmodium Species during Peak Transmission Seasons from 2016 to 2021 in the Rural Commune of Ntjiba, Mali" Tropical Medicine and Infectious Disease 8, no. 9: 438. https://doi.org/10.3390/tropicalmed8090438