
Evaluating COVID-19-Related Disruptions to Effective Malaria Case Management in 2020–2021 and Its Potential Effects on Malaria Burden in Sub-Saharan Africa
 , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Overview
2.2. Geographic Scope
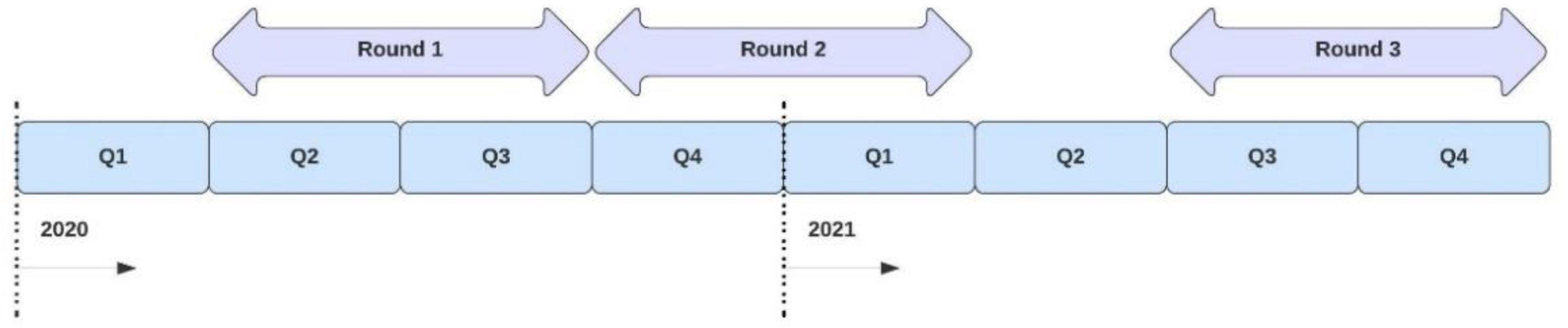
2.3. WHO Pulse Surveys
2.4. Calculating Upper and Lower Disruption Thresholds—WHO Pulse Survey
2.5. Estimating Malaria Case Incidence and Mortality
3. Results
3.1. Estimating Malaria Case Incidence and Mortality
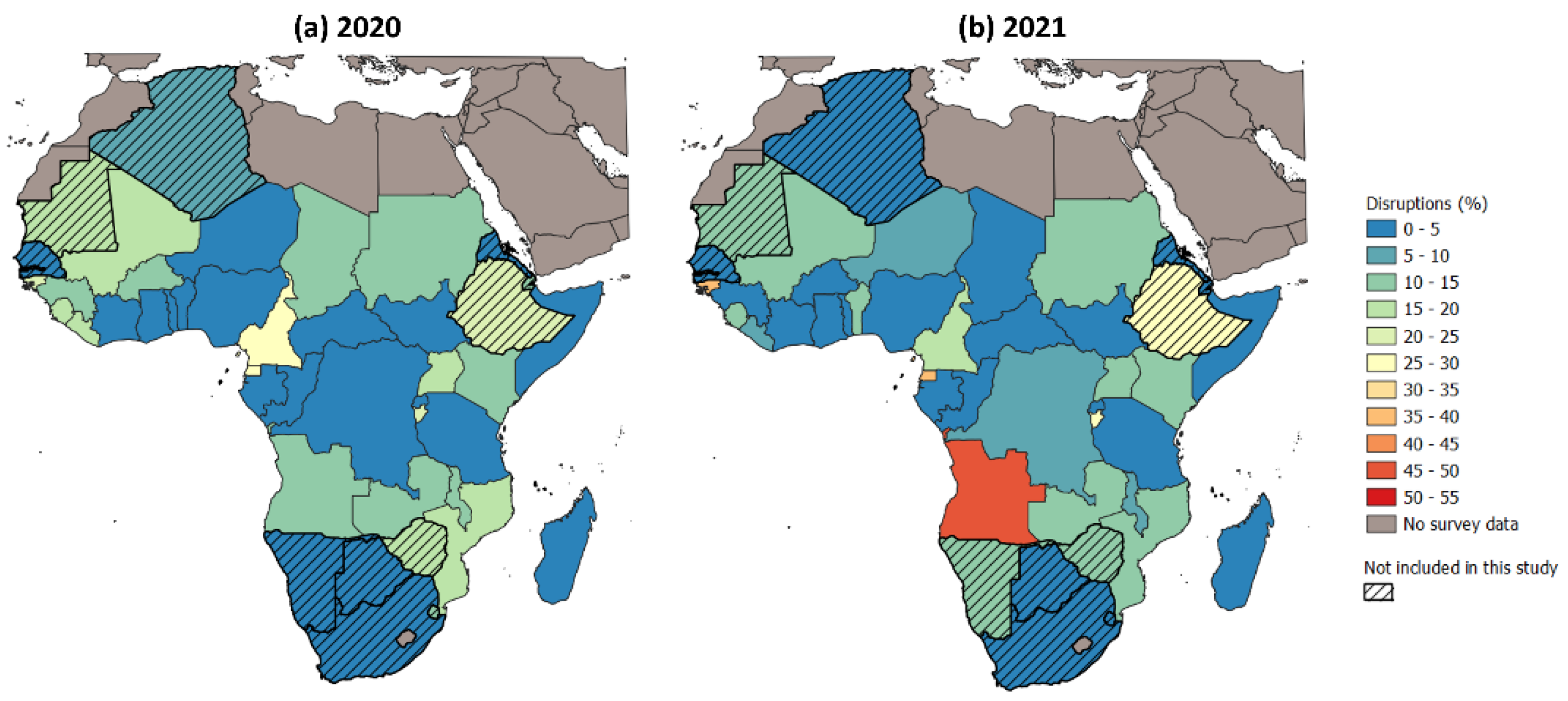
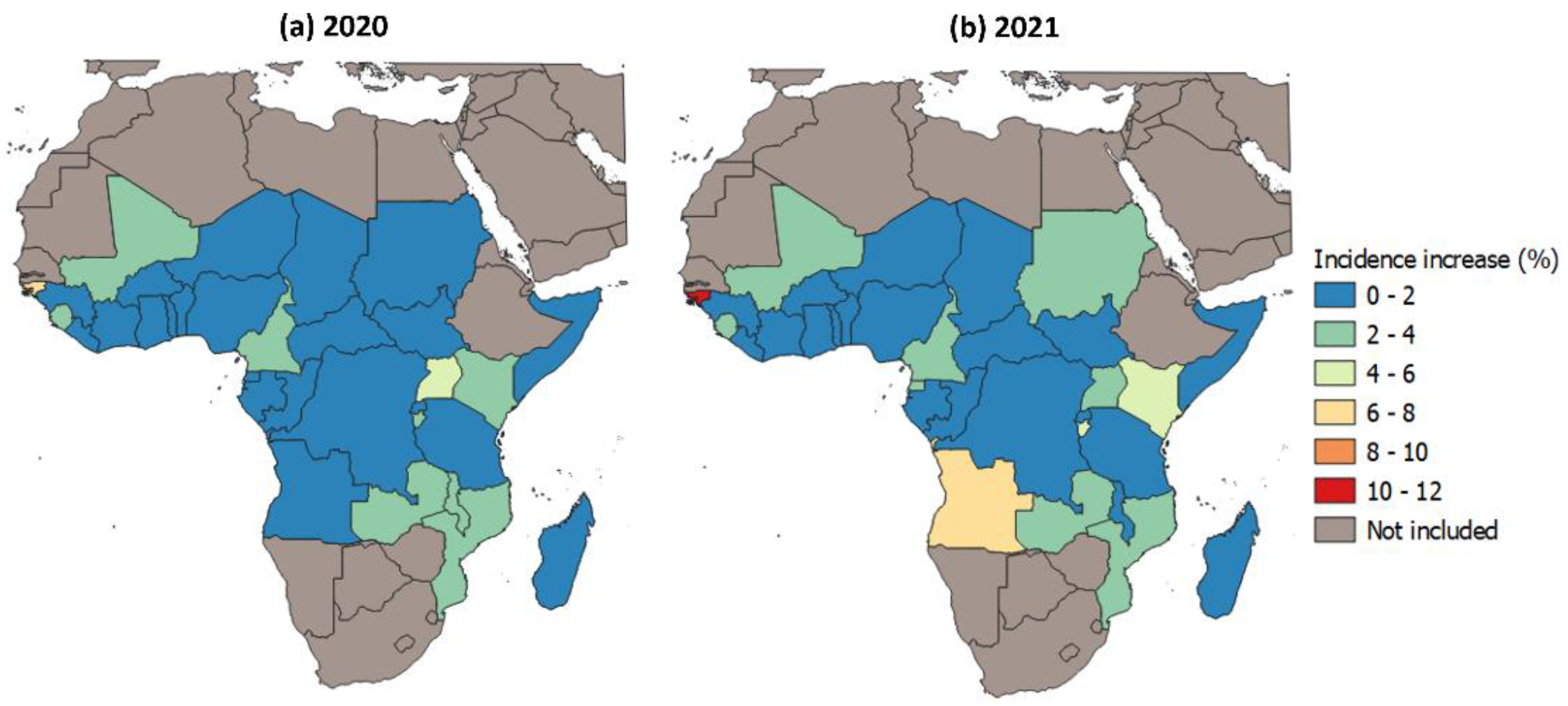
3.2. Effect of Disruptions to Malaria Case Management on Malaria Case Incidence in 2020–2021
3.3. Effect of Disruptions to Malaria Case Management on Malaria Mortality in 2020–2021
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. World Malaria Report 2022. 2022. Available online: https://www.who.int/teams/global-malaria-programme/reports/world-malaria-report-2022 (accessed on 9 January 2023).
- Weiss, D.J.; Bertozzi-Villa, A.; Rumisha, S.F.; Amratia, P.; Arambepola, R.; Battle, K.E.; Cameron, E.; Chestnutt, E.; Gibson, H.S.; Harris, J.; et al. Indirect effects of the COVID-19 pandemic on malaria intervention coverage, morbidity, and mortality in Africa: A geospatial modelling analysis. Lancet Infect. Dis. 2021, 21, 59–69. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. WHO Urges Countries to Move Quickly to Save Lives from Malaria in Sub-Saharan Africa. Available online: https://www.who.int/news/item/23-04-2020-who-urges-countries-to-move-quickly-to-save-lives-from-malaria-in-sub-saharan-africa (accessed on 14 September 2022).
- World Health Organization. World Malaria Report 2021. 2021. Available online: https://www.who.int/teams/global-malaria-programme/reports/world-malaria-report-2021 (accessed on 15 December 2021).
- World Health Organization. Global Malaria Programme. Available online: https://www.who.int/teams/global-malaria-programme/reports (accessed on 9 January 2023).
- Battle, K.E.; Lucas, T.C.D.; Nguyen, M.; Howes, R.E.; Nandi, A.K.; Twohig, K.A.; Pfeffer, D.A.; Cameron, E.; Rao, P.C.; Casey, D.; et al. Mapping the global endemicity and clinical burden of Plasmodium vivax, 2000–2017: A spatial and temporal modelling study. Lancet 2019, 394, 332–343. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bhatt, S.; Weiss, D.J.; Cameron, E.; Bisanzio, D.; Mappin, B.; Dalrymple, U.; Battle, K.E.; Moyes, C.L.; Henry, A.; Eckhoff, P.A.; et al. The effect of malaria control on Plasmodium falciparum in Africa between 2000 and 2015. Nature 2015, 526, 207–211. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- ICF. Demographic and Health Surveys. Funded by USAID. 2022. Available online: http://www.dhsprogram.com (accessed on 2 December 2022).
- USAID. The DHS Program-COVID-19 Update: Some DHS Surveys Return to the Field; Others Postponed Until 2021. Available online: https://www.dhsprogram.com/Who-We-Are/News-Room/COVID-19-Update-Some-DHS-surveys-return-to-the-field-others-postponed-until-2021.cfm (accessed on 15 July 2021).
- World Health Organization. Pulse Survey on Continuity of Essential Health Services during the COVID-19 Pandemic: Interim Report, 27 August 2020. 2020. Available online: https://www.who.int/publications/i/item/WHO-2019-nCoV-EHS_continuity-survey-2020.1 (accessed on 3 March 2021).
- World Health Organization. Second Round of the National Pulse Survey on Continuity of Essential Health Services during the COVID-19 Pandemic. 2021. Available online: https://www.who.int/publications/i/item/WHO-2019-nCoV-EHS-continuity-survey-2021.1 (accessed on 27 July 2021).
- World Health Organization. Third Round of the Global Pulse Survey on Continuity of Essential Health Services during the COVID-19 Pandemic. 2022. Available online: https://www.who.int/publications/i/item/WHO-2019-nCoV-EHS_continuity-survey-2022.1 (accessed on 12 April 2022).
- Weiss, D.J.; Lucas, T.C.D.; Nguyen, M.; Nandi, A.K.; Bisanzio, D.; Battle, K.E.; Cameron, E.; Twohig, K.A.; Pfeffer, D.A.; Rozier, J.A.; et al. Mapping the global prevalence, incidence, and mortality of Plasmodium falciparum, 2000–2017: A spatial and temporal modelling study. Lancet 2019, 394, 322–331. [Google Scholar] [CrossRef] [Green Version]
- Bhatt, S.; Cameron, E.; Flaxman, S.R.; Weiss, D.J.; Smith, D.L.; Gething, P.W. Improved prediction accuracy for disease risk mapping using Gaussian process stacked generalization. J. R. Soc. Interface 2017, 14, 20170520. [Google Scholar] [CrossRef] [Green Version]
- Cameron, E.; Battle, K.E.; Bhatt, S.; Weiss, D.J.; Bisanzio, D.; Mappin, B.; Dalrymple, U.; Hay, S.I.; Smith, D.L.; Griffin, J.T.; et al. Defining the relationship between infection prevalence and clinical incidence of Plasmodium falciparum malaria. Nat. Commun. 2015, 6, 8170. [Google Scholar] [CrossRef] [Green Version]
- Gething, P.W.; Casey, D.C.; Weiss, D.J.; Bisanzio, D.; Bhatt, S.; Cameron, E.; Battle, K.E.; Dalrymple, U.; Rozier, J.; Rao, P.C.; et al. Mapping Plasmodium falciparum Mortality in Africa between 1990 and 2015. N. Engl. J. Med. 2016, 375, 2435–2445. [Google Scholar] [CrossRef] [Green Version]
- Zezza, A.; Martuscelli, A.; Wollburg, P.; Gourlay, S.; Kilic, T. Viewpoint: High-frequency phone surveys on COVID-19: Good practices, open questions. Food Policy 2021, 105, 102153. [Google Scholar] [CrossRef]
- Amouzou, A.; Maïga, A.; Faye, C.M.; Chakwera, S.; Melesse, D.Y.; Mutua, M.K.; Thiam, S.; Abdoulaye, I.B.; Afagbedzi, S.K.; Iknane, A.A.; et al. Health service utilisation during the COVID-19 pandemic in sub-Saharan Africa in 2020: A multicountry empirical assessment with a focus on maternal, newborn and child health services. BMJ Glob. Health 2022, 7, e008069. [Google Scholar] [CrossRef]
- Shapira, G.; Ahmed, T.; Drouard, S.H.P.; Amor Fernandez, P.; Kandpal, E.; Nzelu, C.; Wesseh, C.S.; Mohamud, N.A.; Smart, F.; Mwansambo, C.; et al. Disruptions in maternal and child health service utilization during COVID-19: Analysis from eight sub-Saharan African countries. Health Policy Plan. 2021, 36, 1140–1151. [Google Scholar] [CrossRef]
- World Health Organization. World Malaria Report: 20 Years of Global Progress and Challenges. 2020. Available online: https://www.who.int/publications/i/item/9789240015791 (accessed on 20 January 2021).
- Bertozzi-Villa, A.; Bever, C.A.; Koenker, H.; Weiss, D.J.; Vargas-Ruiz, C.; Nandi, A.K.; Gibson, H.S.; Harris, J.; Battle, K.E.; Rumisha, S.F.; et al. Maps and metrics of insecticide-treated net access, use, and nets-per-capita in Africa from 2000–2020. Nat. Commun. 2021, 12, 3589. [Google Scholar] [CrossRef]
- Institute For Health Metrics and Evaluation. Global Burden of Disease. Available online: https://www.healthdata.org/gbd/2019 (accessed on 4 March 2022).
- Balogun, M.; Banke-Thomas, A.; Sekoni, A.; Boateng, G.O.; Yesufu, V.; Wright, O.; Ubani, O.; Abayomi, A.; Afolabi, B.B.; Ogunsola, F. Challenges in access and satisfaction with reproductive, maternal, newborn and child health services in Nigeria during the COVID-19 pandemic: A cross-sectional survey. PLoS ONE 2021, 16, e0251382. [Google Scholar] [CrossRef]
- Buonsenso, D.; Iodice, F.; Sorba Biala, J.; Goletti, D. COVID-19 effects on tuberculosis care in Sierra Leone. Pulmonology 2021, 27, 67–69. [Google Scholar] [CrossRef]
- Hailemariam, S.; Agegnehu, W.; Derese, M. Exploring COVID-19 Related Factors Influencing Antenatal Care Services Uptake: A Qualitative Study among Women in a Rural Community in Southwest Ethiopia. J. Prim. Care Community Health 2021, 12, 2150132721996892. [Google Scholar] [CrossRef]
- Abdela, S.G.; Berhanu, A.B.; Ferede, L.M.; van Griensven, J. Essential Healthcare Services in the Face of COVID-19 Prevention: Experiences from a Referral Hospital in Ethiopia. Am. J. Trop. Med. Hyg. 2020, 103, 1198–1200. [Google Scholar] [CrossRef]
- Chilot, D.; Woldeamanuel, Y.; Manyazewal, T. Real-Time Impact of COVID-19 on Clinical Care and Treatment of Patients with Tuberculosis: A Multicenter Cross-Sectional Study in Addis Ababa, Ethiopia. Ann. Glob. Health 2021, 87, 109. [Google Scholar] [CrossRef]
- Giebel, C.; Ivan, B.; Burger, P.; Ddumba, I. Impact of COVID-19 public health restrictions on older people in Uganda: “hunger is really one of those problems brought by this COVID”. Int. Psychogeriatr. 2020, 34, 805–812. [Google Scholar] [CrossRef]
- Abdoulaye, M.B.; Oumarou, B.; Moussa, H.; Anya, B.M.; Didier, T.; Nsiari-Muzeyi, B.J.; Katoto, P.; Wiysonge, C.S. The impact of the COVID-19 pandemic on health service utilisation in the City of Niamey: A study conducted in 17 health care facilities from January to June 2020. Pan. Afr. Med. J. 2021, 39, 159. [Google Scholar] [CrossRef]
- Abebe, W.; Worku, A.; Moges, T.; Tekle, N.; Amogne, W.; Haile, T.; Mekonen, D.; Habtamu, A.; Deressa, W. Trends of follow-up clinic visits and admissions three-months before and during COVID-19 pandemic at Tikur Anbessa specialized hospital, Addis Ababa, Ethiopia: An interrupted time series analysis. BMC Health Serv. Res. 2021, 21, 731. [Google Scholar] [CrossRef]
- Atim, M.G.; Kajogoo, V.D.; Amare, D.; Said, B.; Geleta, M.; Muchie, Y.; Tesfahunei, H.A.; Assefa, D.G.; Manyazewal, T. COVID-19 and Health Sector Development Plans in Africa: The Impact on Maternal and Child Health Outcomes in Uganda. Risk Manag. Health Policy 2021, 14, 4353–4360. [Google Scholar] [CrossRef]
- Banke-Thomas, A.; Semaan, A.; Amongin, D.; Babah, O.; Dioubate, N.; Kikula, A.; Nakubulwa, S.; Ogein, O.; Adroma, M.; Adiga, W.A.; et al. A mixed-methods study of maternal health care utilisation in six referral hospitals in four sub-Saharan African countries before and during the COVID-19 pandemic. BMJ Glob. Health 2022, 7, e008064. [Google Scholar] [CrossRef]
- Arthur-Holmes, F.; Akaadom, M.K.A.; Agyemang-Duah, W.; Abrefa Busia, K.; Peprah, P. Healthcare Concerns of Older Adults during the COVID-19 Outbreak in Low- and Middle-Income Countries: Lessons for Health Policy and Social Work. J. Gerontol. Soc. Work 2020, 63, 717–723. [Google Scholar] [CrossRef]
- Gitau, T.; Kamita, M.; Muli, E.; Mweni, S.; Waithanji, R.; Mutisya, F.; Kirira, P.; Nzioka, A.; Figueroa, J.; Makokha, F. The impact of measures to curb COVID-19 on patient attendance at 10 hospitals in Machakos County, Kenya. J. Glob. Health 2021, 11, 5016. [Google Scholar] [CrossRef] [PubMed]
- Kassaman, D.; Kimani, R.W.; Lusambili, A. Challenges for cancer care during COVID-19 pandemic in Kenya: Policy implications. J. Cancer Policy 2020, 25, 100247. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, S.; Ajisola, M.; Azeem, K.; Bakibinga, P.; Chen, Y.F.; Choudhury, N.N.; Fayehun, O.; Griffiths, F.; Harris, B.; Kibe, P.; et al. Impact of the societal response to COVID-19 on access to healthcare for non-COVID-19 health issues in slum communities of Bangladesh, Kenya, Nigeria and Pakistan: Results of pre-COVID and COVID-19 lockdown stakeholder engagements. BMJ Glob. Health 2020, 5, e003042. [Google Scholar] [CrossRef] [PubMed]
- das Neves Martins Pires, P.H.; Macaringue, C.; Abdirazak, A.; Mucufo, J.R.; Mupueleque, M.A.; Zakus, D.; Siemens, R.; Belo, C.F. COVID-19 pandemic impact on maternal and child health services access in Nampula, Mozambique: A mixed methods research. BMC Health Serv. Res. 2021, 21, 860. [Google Scholar] [CrossRef]
- Burt, J.F.; Ouma, J.; Lubyayi, L.; Amone, A.; Aol, L.; Sekikubo, M.; Nakimuli, A.; Nakabembe, E.; Mboizi, R.; Musoke, P.; et al. Indirect effects of COVID-19 on maternal, neonatal, child, sexual and reproductive health services in Kampala, Uganda. BMJ Glob. Health 2021, 6, e006102. [Google Scholar] [CrossRef]
- Chu, K.M.; Smith, M.; Steyn, E.; Goldberg, P.; Bougard, H.; Buccimazza, I. Changes in surgical practice in 85 South African hospitals during COVID-19 hard lockdown. S. Afr. Med. J. 2020, 110, 916–919. [Google Scholar]
- Habtamu, E. COVID-19 and Eye Care Services in Ethiopia. Community Eye Health 2020, 33, 19. [Google Scholar]
- Emmanuel Awucha, N.; Chinelo Janefrances, O.; Chima Meshach, A.; Chiamaka Henrietta, J.; Ibilolia Daniel, A.; Esther Chidiebere, N. Impact of the COVID-19 Pandemic on Consumers’ Access to Essential Medicines in Nigeria. Am. J. Trop. Med. Hyg. 2020, 103, 1630–1634. [Google Scholar] [CrossRef]
- Asante, D.; Twumasi, M.A.; Sakyi, A.S.K.; Gyamerah, S.; Asante, B. A socio-geographic perspective of health and economic impacts of COVID-19 on poor households in Ghana. GeoJournal 2021, 87, 4113–4125. [Google Scholar] [CrossRef]
- Desta, A.A.; Woldearegay, T.W.; Gebremeskel, E.; Alemayehu, M.; Getachew, T.; Gebregzabiher, G.; Ghebremedhin, K.D.; Zgita, D.N.; Aregawi, A.B.; Redae, G. Impacts of COVID-19 on essential health services in Tigray, Northern Ethiopia: A pre-post study. PLoS ONE 2021, 16, e0256330. [Google Scholar] [CrossRef]
- Ahmed, T.; Rahman, A.E.; Amole, T.G.; Galadanci, H.; Matjila, M.; Soma-Pillay, P.; Gillespie, B.M.; El Arifeen, S.; Anumba, D.O.C. The effect of COVID-19 on maternal newborn and child health (MNCH) services in Bangladesh, Nigeria and South Africa: Call for a contextualised pandemic response in LMICs. Int. J. Equity Health 2021, 20, 77. [Google Scholar] [CrossRef]
- Heuschen, A.K.; Lu, G.; Razum, O.; Abdul-Mumin, A.; Sankoh, O.; von Seidlein, L.; D’Alessandro, U.; Müller, O. Public health-relevant consequences of the COVID-19 pandemic on malaria in sub-Saharan Africa: A scoping review. Malar. J. 2021, 20, 339. [Google Scholar] [CrossRef]
- Bimpong, K.A.; Nuertey, B.D.; Seidu, A.S.; Ajinkpang, S.; Abdul-Mumin, A. Decline in Uptake of Childhood Vaccinations in a Tertiary Hospital in Northern Ghana during the COVID-19 Pandemic. Biomed. Res. Int. 2021, 2021, 6995096. [Google Scholar] [CrossRef]
- Linnemayr, S.; Jennings Mayo-Wilson, L.; Saya, U.; Wagner, Z.; MacCarthy, S.; Walukaga, S.; Nakubulwa, S.; Karamagi, Y. HIV Care Experiences During the COVID-19 Pandemic: Mixed-Methods Telephone Interviews with Clinic-Enrolled HIV-Infected Adults in Uganda. AIDS Behav. 2021, 25, 28–39. [Google Scholar] [CrossRef]
- Abdela, S.G.; van Griensven, J.; Seife, F.; Enbiale, W. Neglecting the effect of COVID-19 on neglected tropical diseases: The Ethiopian perspective. Trans. R. Soc. Trop. Med. Hyg. 2020, 114, 730–732. [Google Scholar] [CrossRef]
- Arsenault, C.; Gage, A.; Kim, M.K.; Kapoor, N.R.; Akweongo, P.; Amponsah, F.; Aryal, A.; Asai, D.; Awoonor-Williams, J.K.; Ayele, W.; et al. COVID-19 and resilience of healthcare systems in ten countries. Nat. Med. 2022, 28, 1314–1324. [Google Scholar] [CrossRef]
- Crowley, T.; Kitshoff, D.; De Lange-Cloete, F.; Baron, J.; De Lange, S.; Young, C.; Esterhuizen, T.; Couper, I. Reorganisation of primary care services during COVID-19 in the Western Cape, South Africa: Perspectives of primary care nurses. S. Afr. Fam. Pr. 2021, 63, e1–e10. [Google Scholar] [CrossRef]
- Adelekan, B.; Goldson, E.; Abubakar, Z.; Mueller, U.; Alayande, A.; Ojogun, T.; Ntoimo, L.; Williams, B.; Muhammed, I.; Okonofua, F. Effect of COVID-19 pandemic on provision of sexual and reproductive health services in primary health facilities in Nigeria: A cross-sectional study. Reprod. Health 2021, 18, 166. [Google Scholar] [CrossRef]
- Gizaw, T.; Jemal, A.; Gudeta, T. Tracer Pharmaceuticals Availability and Distribution Trends Prior to and During the COVID-19 Pandemic: A Comparative Study. J. Multidiscip. Heal. 2022, 15, 93–102. [Google Scholar] [CrossRef] [PubMed]
- Boyd, A.T.; Jahun, I.; Dirlikov, E.; Greby, S.; Odafe, S.; Abdulkadir, A.; Odeyemi, O.; Dalhatu, I.; Ogbanufe, O.; Abutu, A.; et al. Expanding access to HIV services during the COVID-19 pandemic-Nigeria, 2020. AIDS Res. Ther. 2021, 18, 62. [Google Scholar] [CrossRef] [PubMed]
- Harris, T.G.; Jaszi, E.; Lamb, M.R.; Laudari, C.A.; Furtado, M.L.M.; Nijirazana, B.; Aimé, N.; Ekali, G.L.; Lifanda, L.E.; Brou, H.; et al. Effects of the COVID-19 Pandemic on HIV Services: Findings from 11 Sub-Saharan African Countries. Clin. Infect. Dis. 2021, 75, e1046–e1053. [Google Scholar] [CrossRef]
- Tran, D.N.; Were, P.M.; Kangogo, K.; Amisi, J.A.; Manji, I.; Pastakia, S.D.; Vedanthan, R. Supply-chain strategies for essential medicines in rural western Kenya during COVID-19. Bull. World Health Organ. 2021, 99, 388–392. [Google Scholar] [CrossRef] [PubMed]
- Haque, M.; Abubakar, A.R.; Ogunleye, O.O.; Sani, I.H.; Sefah, I.; Kurdi, A.; Islam, S. Changes in Availability, Utilization, and Prices of Medicines and Protection Equipment for COVID-19 in an Urban Population of Northern Nigeria. J. Res. Pharm. Pr. 2021, 10, 17–22. [Google Scholar] [CrossRef]
- Hakizimana, D.; Ntizimira, C.; Mbituyumuremyi, A.; Hakizimana, E.; Mahmoud, H.; Birindabagabo, P.; Musanabaganwa, C.; Gashumba, D. The impact of COVID-19 on malaria services in three high endemic districts in Rwanda: A mixed-method study. Malar. J. 2022, 21, 48. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| <5% | 5–50% | >50% | |
|---|---|---|---|
| Round one | 9 | 12 | 0 |
| Round two | 12 | 7 | 2 |
| Round three | 19 | 4 | 0 |
| Indirect impacts of COVID-19 on healthcare services | Inhibited movement | Increased cost of transport [23,24,25] |
| Suspension of public transport [26,27,28] | ||
| Government-imposed movement restrictions [29,30,31] | ||
| Scaling down operations by health facilities | Temporarily closing down [32,33,34] | |
| Shortening opening hours [35,36,37] | ||
| Limiting operations to essential services [38,39,40] | ||
| Increased cost of care | Direct increase in costs due to additional cost of PPE and increased price of medicine [27,32,41] | |
| Perceived increase in the costs due to loss of income [42,43,44] | ||
| Other | Avoiding health facilities due to fear of COVID-19 [45,46,47] | |
| Repurposing resources to manage COVID-19 [48,49,50] | ||
| Supply shortages (PPE equipment and medicine) [36,51,52] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dzianach, P.A.; Rumisha, S.F.; Lubinda, J.; Saddler, A.; van den Berg, M.; Gelaw, Y.A.; Harris, J.R.; Browne, A.J.; Sanna, F.; Rozier, J.A.; et al. Evaluating COVID-19-Related Disruptions to Effective Malaria Case Management in 2020–2021 and Its Potential Effects on Malaria Burden in Sub-Saharan Africa. Trop. Med. Infect. Dis. 2023, 8, 216. https://doi.org/10.3390/tropicalmed8040216
Dzianach PA, Rumisha SF, Lubinda J, Saddler A, van den Berg M, Gelaw YA, Harris JR, Browne AJ, Sanna F, Rozier JA, et al. Evaluating COVID-19-Related Disruptions to Effective Malaria Case Management in 2020–2021 and Its Potential Effects on Malaria Burden in Sub-Saharan Africa. Tropical Medicine and Infectious Disease. 2023; 8(4):216. https://doi.org/10.3390/tropicalmed8040216
Chicago/Turabian StyleDzianach, Paulina A., Susan F. Rumisha, Jailos Lubinda, Adam Saddler, Mauricio van den Berg, Yalemzewod A. Gelaw, Joseph R. Harris, Annie J. Browne, Francesca Sanna, Jennifer A. Rozier, and et al. 2023. "Evaluating COVID-19-Related Disruptions to Effective Malaria Case Management in 2020–2021 and Its Potential Effects on Malaria Burden in Sub-Saharan Africa" Tropical Medicine and Infectious Disease 8, no. 4: 216. https://doi.org/10.3390/tropicalmed8040216