
Spatial and Temporal Data Visualisation for Mass Dissemination: Advances in the Era of COVID-19

Abstract
:1. Introduction
2. Platforms for Information Display
3. Sources of Data
4. Access Control for Data Visualisation Platforms
5. Types of Data Representation
6. Data and Visualisation Platform Quality
7. Discussion and Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Franch-Pardo, I.; Napoletano, B.M.; Rosete-Verges, F.; Billa, L. Spatial analysis and GIS in the study of COVID-19. A review. Sci. Total Environ. 2020, 739, 140033. [Google Scholar] [CrossRef]
- Koch, T. Welcome to the revolution: COVID-19 and the democratization of spatial-temporal data. Patterns 2021, 2, 100272. [Google Scholar] [CrossRef]
- Komenda, M.; Bulhart, V.; Karolyi, M.; Jarkovsky, J.; Muzik, J.; Majek, O.; Šnajdrová, L.; Růžičková, P.; Rážová, J.; Prymula, R.; et al. Complex Reporting of the COVID-19 Epidemic in the Czech Republic: Use of an Interactive Web-Based App in Practice. J. Med. Internet Res. 2020, 22, e19367. [Google Scholar] [CrossRef] [PubMed]
- Onemocnění Aktuálně. COVID-19: Overview of Current Situation in the Czech Republic. Available online: https://onemocneni-aktualne.mzcr.cz/covid-19 (accessed on 11 April 2023).
- Kolak, M.; Li, X.; Lin, Q.; Wang, R.; Menghaney, M.; Yang, S.; Anguiano, V., Jr. The US COVID Atlas: A dynamic cyberinfrastructure surveillance system for interactive exploration of the pandemic. Trans. GIS 2021, 25, 1741–1765. [Google Scholar] [CrossRef] [PubMed]
- WHO Coronavirus (COVID-19) Dashboard. Available online: https://covid19.who.int/ (accessed on 11 April 2023).
- Worldometer COVID-19 Coronavirus Pandemic. Available online: https://www.worldometers.info/coronavirus/ (accessed on 11 April 2023).
- COVID-19 Information Centre. Available online: https://www2.deloitte.com/ca/en/pages/about-deloitte/articles/covid-dashboard.html (accessed on 11 April 2023).
- Our World in Data Coronavirus Pandemic (COVID-19): Our World in Data. Available online: https://ourworldindata.org/coronavirus (accessed on 11 April 2023).
- Wissel, B.D.; Van Camp, P.J.; Kouril, M.; Weis, C.; Glauser, T.A.; White, P.S.; Kohane, I.; Dexheimer, J.W. An interactive online dashboard for tracking COVID-19 in U.S. counties, cities, and states in real time. J. Am. Med. Inf. Assoc. 2020, 27, 1121–1125. [Google Scholar] [CrossRef] [PubMed]
- Ivanković, D.; Barbazza, E.; Bos, V.; Brito Fernandes, O.; Jamieson Gilmore, K.; Jansen, T.; Kara, P.; Larrain, N.; Lu, S.; Meza-Torres, B.; et al. Features Constituting Actionable COVID-19 Dashboards: Descriptive Assessment and Expert Appraisal of 158 Public Web-Based COVID-19 Dashboards. J. Med. Internet Res. 2021, 23, e25682. [Google Scholar] [CrossRef]
- Naqvi, A. COVID-19 European regional tracker. Sci. Data. 2021, 8, 181. [Google Scholar] [CrossRef]
- Martinez Beltran, E.T.; Quiles Perez, M.; Pastor-Galindo, J.; Nespoli, P.; Garcia Clemente, F.J.; Gomez Marmol, F. COnVIDa: COVID-19 multidisciplinary data collection and dashboard. J. Biomed. Inform. 2021, 117, 103760. [Google Scholar] [CrossRef] [PubMed]
- Field, E.; Dyda, A.; Hewett, M.; Weng, H.; Shi, J.; Curtis, S.; Law, C.; McHugh, L.; Sheel, M.; Moore, J.; et al. Development of the COVID-19 Real-Time Information System for Preparedness and Epidemic Response (CRISPER), Australia. Front. Public Health 2021, 9, 753493. [Google Scholar] [CrossRef]
- Ponce-de-Leon, M.; Del Valle, J.; Fernandez, J.M.; Bernardo, M.; Cirillo, D.; Sanchez-Valle, J.; Smith, M.; Capella-Gutierrez, S.; Gullón, T. COVID-19 Flow-Maps an open geographic information system on COVID-19 and human mobility for Spain. Sci. Data 2021, 8, 310. [Google Scholar] [CrossRef]
- Kaul, S.; Coleman, C.; Gotz, D. A rapidly deployed, interactive, online visualization system to support fatality management during the coronavirus disease 2019 (COVID-19) pandemic. J. Am. Med. Inform. Assoc. 2020, 27, 1943–1948. [Google Scholar] [CrossRef] [PubMed]
- Chande, A.; Lee, S.; Harris, M.; Nguyen, Q.; Beckett, S.J.; Hilley, T.; Andris, C.; Weitz, J.S. Real-time, interactive website for US-county-level COVID-19 event risk assessment. Nat. Hum. Behav. 2020, 4, 1313–1319. [Google Scholar] [CrossRef] [PubMed]
- Ghimire, B.R.; Parajuli, R.R.; Khatiwada, B.; Poudel, S.; Sharma, K.; Mishra, B. Covira: A COVID-19 risk assessment, visualization and communication tool. SoftwareX 2021, 16, 100873. [Google Scholar] [CrossRef] [PubMed]
- Bos, V.; Jansen, T.; Klazinga, N.S.; Kringos, D.S. Development and Actionability of the Dutch COVID-19 Dashboard: Descriptive Assessment and Expert Appraisal Study. JMIR Public Health Surveill. 2021, 7, e31161. [Google Scholar] [CrossRef]
- Dong, E.; Du, H.; Gardner, L. An interactive web-based dashboard to track COVID-19 in real time. Lancet Infect. Dis. 2020, 20, 533–534. [Google Scholar] [CrossRef]
- Lan, H.; Sha, D.; Malarvizhi, A.S.; Liu, Y.; Li, Y.; Meister, N.; Liu, Q.; Wang, Z.; Yang, J. COVID-Scraper: An Open-Source Toolset for Automatically Scraping and Processing Global Multi-Scale Spatiotemporal COVID-19 Records. IEEE Access 2021, 9, 84783–84798. [Google Scholar] [CrossRef]
- Kamel Boulos, M.N.; Geraghty, E.M. Geographical tracking and mapping of coronavirus disease COVID-19/severe acute res-piratory syndrome coronavirus 2 (SARS-CoV-2) epidemic and associated events around the world: How 21st century GIS technol-ogies are supporting the global fight against outbreaks and epidemics. Int. J. Health Geogr. 2020, 19, 8. [Google Scholar]
- Shaheen, A.W.; Ciesco, E.; Johnson, K.; Kuhnen, G.; Paolini, C.; Gartner, G. Interactive, on-line visualization tools to measure and drive equity in COVID-19 vaccine administrations. J. Am. Med. Inf. Assoc. 2021, 28, 2451–2455. [Google Scholar] [CrossRef]
- Su, W.; Fu, W.; Kato, K.; Wong, Z.S. “Japan LIVE Dashboard” for COVID-19: A Scalable Solution to Monitor Real-Time and Re-gional-Level Epidemic Case Data. Stud. Health Technol. Inform. 2021, 286, 21–25. [Google Scholar]
- Pfeiffer, D.; Robinson, T.; Stevenson, M.; Stevens, K.; Rogers, D.; Clements, A.C.A. (Eds.) Spatial visualization. In Spatial Analysis in Epidemiology; Oxford University Press: Oxford, UK, 2008; pp. 17–31. [Google Scholar]
- Juergens, C. Trustworthy COVID-19 Mapping: Geo-spatial Data Literacy Aspects of Choropleth Maps. KN J. Cart. Geogr. Inf. 2020, 70, 155–161. [Google Scholar] [CrossRef]
- Rosenkrantz, L.; Schuurman, N.; Bell, N.; Amram, O. The need for GIScience in mapping COVID-19. Health Place 2021, 67, 102389. [Google Scholar] [CrossRef] [PubMed]
- Badker, R.; Miller, K.; Pardee, C.; Oppenheim, B.; Stephenson, N.; Ash, B.; Philippsen, T.; Ngoon, C.; Savage, P.; Lam, C.; et al. Challenges in reported COVID-19 data: Best practices and recommendations for future epidemics. BMJ Glob. Health 2021, 6, e005542. [Google Scholar] [CrossRef] [PubMed]
- Zhao, B.; Kim, M.; Nam, E.W. Information Disclosure Contents of the COVID-19 Data Dashboard Websites for South Korea, China, and Japan: A Comparative Study. Healthcare 2021, 9, 1487. [Google Scholar] [CrossRef]
- Monkman, H.; Martin, S.Z.; Minshall, S.; Kushniruk, A.W.; Lesselroth, B.J. Opportunities to Improve COVID-19 Dashboard Designs for the Public. Stud. Health Technol. Inform. 2021, 286, 16–20. [Google Scholar] [PubMed]
- Dowding, D.; Merrill, J.A. The Development of Heuristics for Evaluation of Dashboard Visualizations. Appl. Clin. Inform. 2018, 9, 511–518. [Google Scholar] [CrossRef] [Green Version]
- Anwar, A.; Malik, M.; Raees, V.; Anwar, A. Role of Mass Media and Public Health Communications in the COVID-19 Pandemic. Cureus 2020, 12, e10453. [Google Scholar] [CrossRef]
- Flaherty, E.; Sturm, T.; Farries, E. The conspiracy of COVID-19 and 5G: Spatial analysis fallacies in the age of data democratization. Soc. Sci. Med. 2022, 293, 114546. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Name | Website | Organization |
|---|---|---|
| Dashboards * | ||
| WHO Coronavirus (COVID-19) Dashboard | https://covid19.who.int/ (accessed 11 April 2023) | World Health Organization |
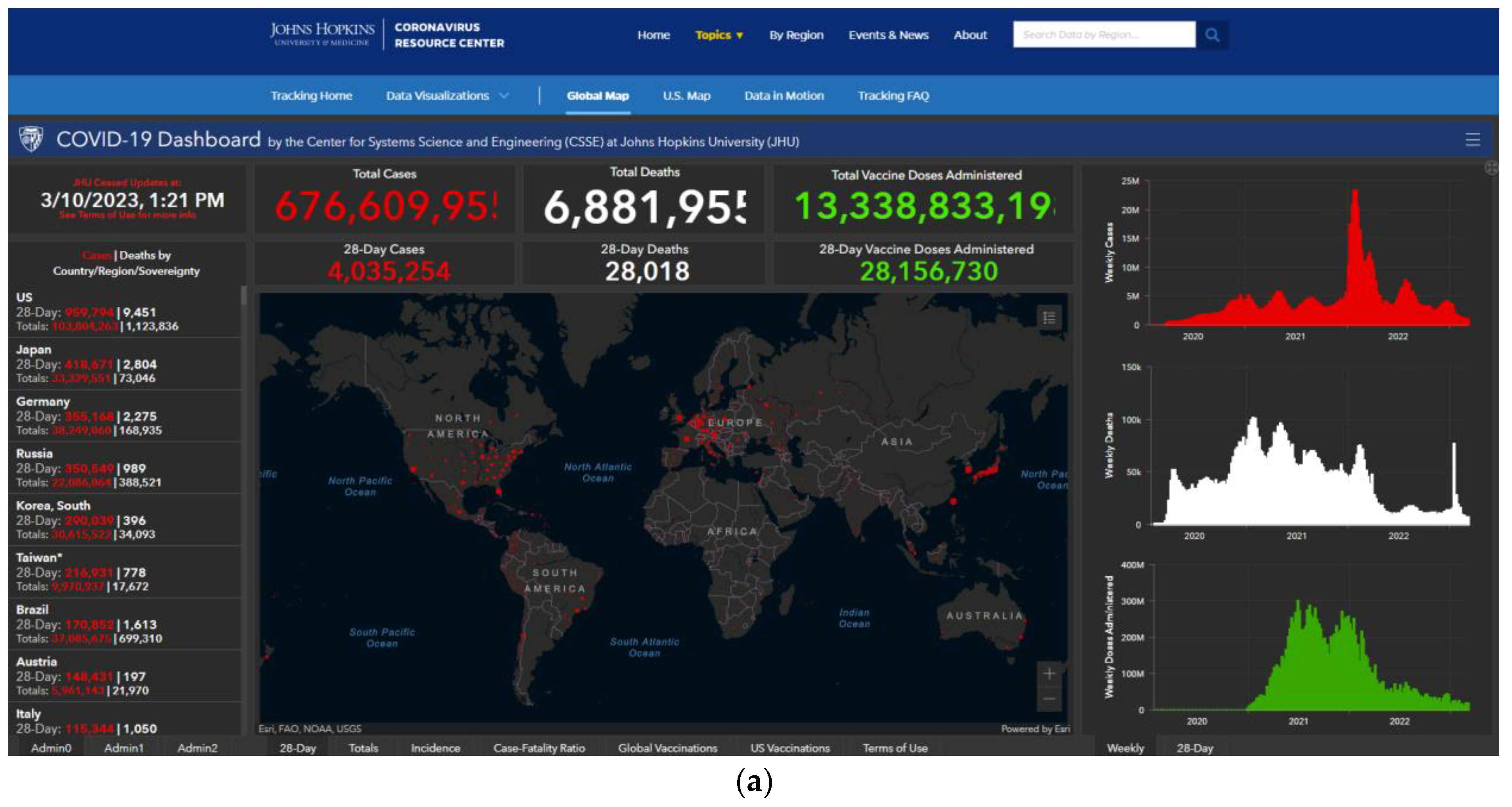
| COVID-19 Dashboard by the Center for Systems Science and Engineering (CSSE) at Johns Hopkins University (JHU) | https://coronavirus.jhu.edu/map.html (accessed on 11 April 2023) | Johns Hopkins University |
| How’s My Flattening | https://howsmyflattening.ca/#/home (accessed on 4 April 2023) | University of Toronto and partners |
| COVID Act Now | https://covidactnow.org/?s=1710634 (accessed on 4 April 2023) | Georgetown, Stanford and Harvard Universities |
| 1Point3Acres | https://coronavirus.1point3acres.com/en (accessed on 6 April 2023) | |
| COVID-19 Info Switzerland | https://corona-data.ch/ (accessed on 4 April 2023) | Swiss National COVID-19 Science Taskforce |
| Japan LIVE Dashboard | http://COVID-2019.live/en/ (accessed on 4 April 2023) | Yahoo Japan, Keio University and St Luke’s International University |
| US COVID Atlas | https://theuscovidatlas.org/ (accessed on 6 April 2023) | University of Chicago and partners. |
| COnVIDa | https://convida.inf.um.es/(no longer live) (accessed on 4 April 2023) | University of Murcia |
| Track COVID-19 in the U.S. | https://www.nytimes.com/interactive/2023/us/covid-cases.html (accessed on 4 April 2023) | The New York Times |
| COVID-19 Coronavirus Pandemic | https://www.worldometers.info/coronavirus/ (accessed on 4 April 2023) | Worldometer |
| Coronavirus Pandemic (COVID-19) | https://ourworldindata.org/coronavirus (accessed on 4 April 2023) | Our World in Data |
| Global COVID-19 Tracker | https://www.kff.org/coronavirus-covid-19/issue-brief/global-covid-19-tracker/ (accessed on 4 April 2023) | Kaiser Family Foundation |
| Coronavirus (COVID-19) in the UK | https://coronavirus.data.gov.uk/details/interactive-map/cases (accessed on 4 April 2023) | UK Government |
| COVID map: Coronavirus cases, deaths, vaccinations by country | https://www.bbc.co.uk/news/world-51235105 (accessed on 4 April 2023) | British Broadcasting Corporation |
| Web scraping tools ** | ||
| COVID-scraper | George Mason University and partners. | |
| COVID-19 European Regional Tracker | https://asjadnaqvi.github.io/COVID19-European-Regional-Tracker/ (accessed on 25 March 2023) | European Union |
| CRISPER | https://crisper.net.au/ (accessed on 25 March 2023) | Australian National University and partners. |
| Static data representations | ||
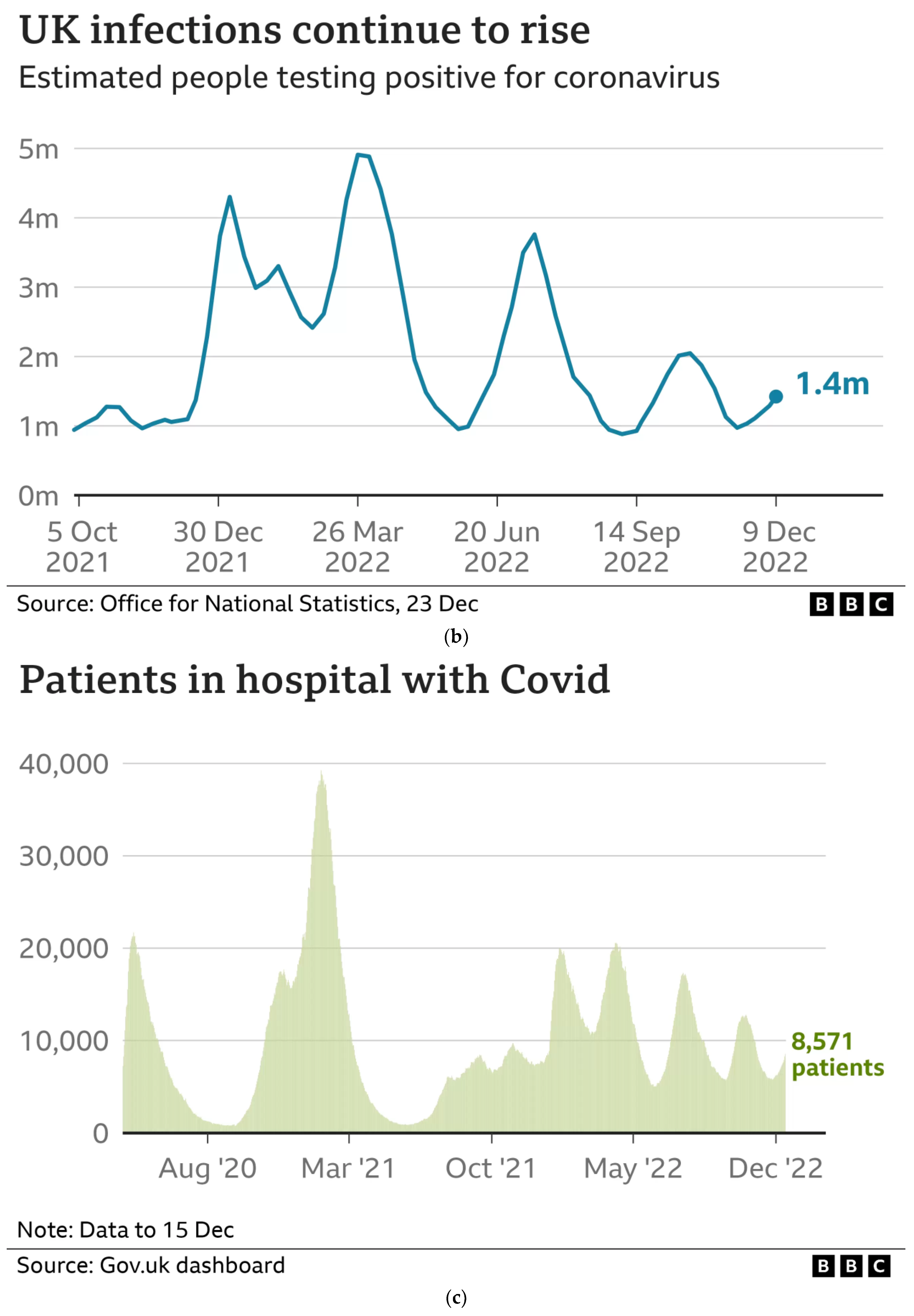
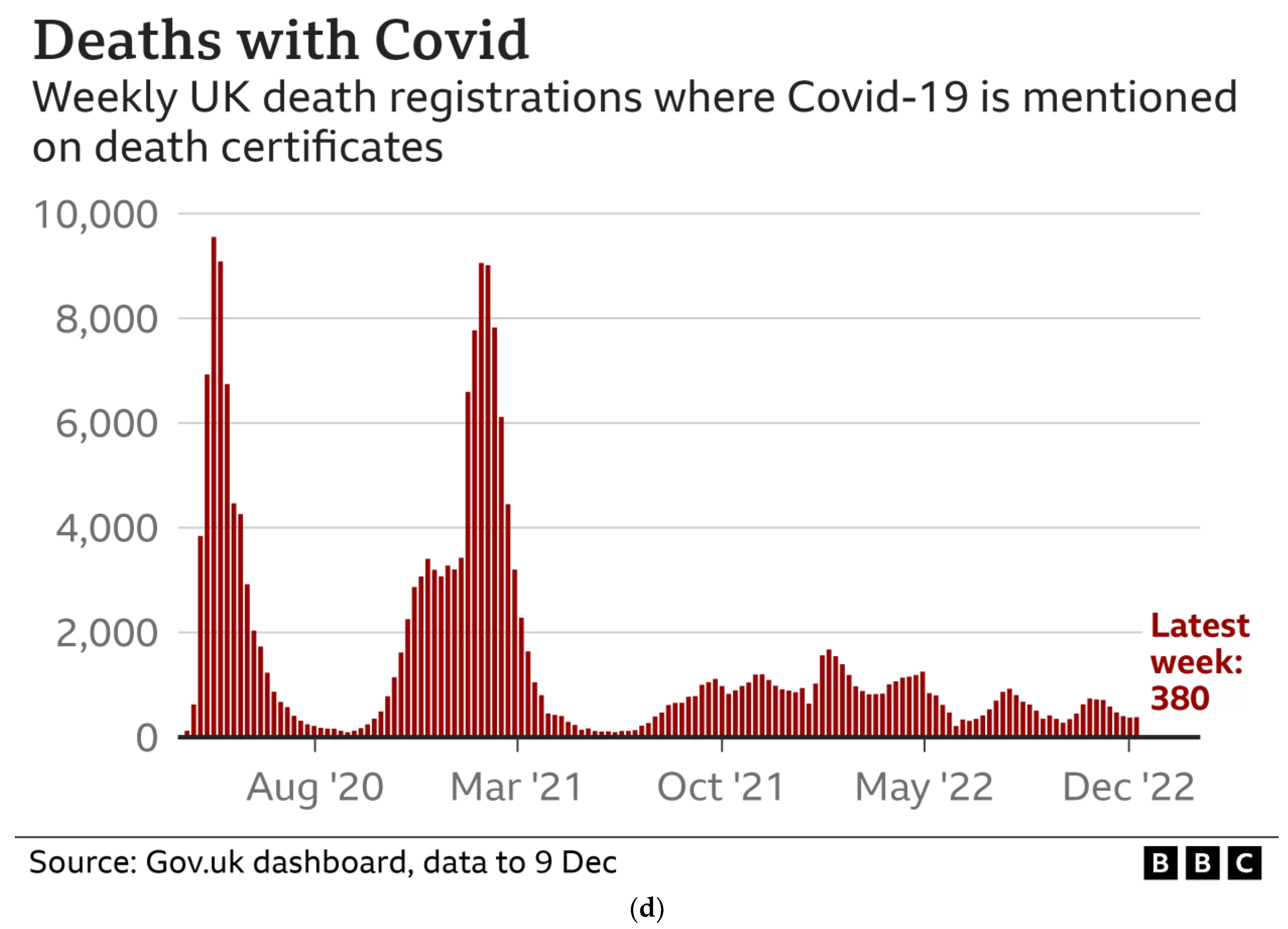
| COVID-19 in the UK | https://www.bbc.co.uk/news/uk-51768274 (accessed on 11 April 2023) | British Broadcasting Corporation |
| COVID hospitalisations: see the latest trend and current count | https://www.nbcnews.com/data-graphics/covid-hospitalizations-see-latest-trend-current-count-rcna61053 (accessed on 11 April 2023) | CNBC News |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Clements, A.C.A. Spatial and Temporal Data Visualisation for Mass Dissemination: Advances in the Era of COVID-19. Trop. Med. Infect. Dis. 2023, 8, 314. https://doi.org/10.3390/tropicalmed8060314
Clements ACA. Spatial and Temporal Data Visualisation for Mass Dissemination: Advances in the Era of COVID-19. Tropical Medicine and Infectious Disease. 2023; 8(6):314. https://doi.org/10.3390/tropicalmed8060314
Chicago/Turabian StyleClements, Archie C. A. 2023. "Spatial and Temporal Data Visualisation for Mass Dissemination: Advances in the Era of COVID-19" Tropical Medicine and Infectious Disease 8, no. 6: 314. https://doi.org/10.3390/tropicalmed8060314